WO2008013492A1 - Embryonic stem cell markers for cancer diagnosis and prognosis - Google Patents
Embryonic stem cell markers for cancer diagnosis and prognosis Download PDFInfo
- Publication number
- WO2008013492A1 WO2008013492A1 PCT/SE2007/000689 SE2007000689W WO2008013492A1 WO 2008013492 A1 WO2008013492 A1 WO 2008013492A1 SE 2007000689 W SE2007000689 W SE 2007000689W WO 2008013492 A1 WO2008013492 A1 WO 2008013492A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- cancer
- genes
- tumor
- expression
- group
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Classifications
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/68—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving nucleic acids
- C12Q1/6876—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes
- C12Q1/6883—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for diseases caused by alterations of genetic material
- C12Q1/6886—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for diseases caused by alterations of genetic material for cancer
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/106—Pharmacogenomics, i.e. genetic variability in individual responses to drugs and drug metabolism
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/112—Disease subtyping, staging or classification
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/118—Prognosis of disease development
Definitions
- the present invention relates to embryonic stem cell (ES) gene markers for use in diagnosis and prognosis of cancer, in particular prostate cancer.
- ES embryonic stem cell
- Bioinformatic analyses based on published or unpublished high throughput proteomic data have not yet reached robust and high resolution as compared with high throughput DNA and RNA analyses.
- Bioinformatic analyses based on published and unpublished high throughput genome-scale DNA analyses provide a list of DNA markers in the form gene copy number changes (deletions, gains and amplifications), mutations and polymorphisms, and methylations. DNA is comparatively stable and easy to be handled in analytical process. However, these DNA changes have to be detected by different methods. It is still an open question why cancer originating from the same kind of tissue progresses slowly in one person and rapidly in another.
- Prostate cancer is a major cause of death worldwide in male adults. Accurately predicting the outcome of prostate cancer at an early stage of tumor development is crucial for providing the proper kind of treatment, and is still an unresolved question. The correct choice of treatment is most important in younger patients (11). It is estimated that of 232,090 American men with newly diagnosed prostate cancer in 2005, roughly 210,000 or approximately 90% will be diagnosed at an early stage with 100% survival for 5 years. In contrast, the estimated deaths from prostate cancer are much less, about 30,350 (12). Online data from the Swedish National Board of Health and Welfare have shown that 7,702 out of 4,427,107 Swedish men in 2001 had newly diagnosed prostate cancer.
- Humphrey PA has given a comprehensive review of Gleason grading and current status of clinical methods in diagnosis and prognosis of prostate cancer (15-16).
- Gleason score of needle core biopsy is currently the key method for confirming the diagnosis of prostate cancer, and has demonstrated strong association with cancer specific survival.
- Gleason grading is not satisfactory for predicting cancer outcome when tumors are small, in particular when tumors are moderately differentiated with a biopsy Gleason score 6, the most common Gleason sum in clinical biopsy cases (15).
- a diagnosis of prostate cancer is uncertain due to insufficient, or lack of, malignant structures, rendering further prediction of cancer outcome impossible (15).
- genomic changes involved include DNA sequence changes, such as base change, deletion, copy number gain, amplification and translocation, as well as DNA modification such as promoter methylation.
- DNA sequence changes such as base change, deletion, copy number gain, amplification and translocation
- DNA modification such as promoter methylation.
- genomic changes cause gene expression alterations that further cause biological alterations in the cell, such as accelerated cell cycle, alteration of cell-cell contact and signalling, increase of genomic instability, escape from apoptosis, increase of cell mobility, activation of angiogenesis and escape from immune surveillance.
- a highly relevant problem is how to predict the outcome of a tumor in a patient.
- Predictive methods available today are based on the concept that all tumor cells in a specific tumor are of the same functional importance. New data has shown that the total tumor cell population can be divided into two populations, i.e., a small tumor stem cell population and a large partially differentiated tumor cell population.
- Tumor stem cells are malignant cells that can proliferate, invade and metastasize, whereas differentiated tumor cells do not possess these properties.
- the present invention is based on the concept that a method for predicting the development of cancer should be based on the genetic profile of tumor stem cells, notwithstanding that they do comprise only a small portion of the total tumor cell population.
- Embryonic stem cell (ES) gene markers of the invention are herein referred to as ES tumor predictor genes (ESTP genes).
- EST expressed sequence tag
- the IMAGE clone ID or the UniGene cluster ID is given.
- the present invention is further based on the concept that embryonic stem cells are the origin of all tissue cells including so called progenitor cells of various specific cell lineages or cell types.
- Tumor cells may be derived from a few tissue stem cells whose regulatory system to guide time- and space-specific differentiation is disabled due to incorrectly repaired DNA damage. Despite impaired differentiation, other stem cell functional properties are more or less maintained or even enhanced, such as proliferation and metastasis. Thus, the more stem cell properties are conserved in the tumor cells, the more aggressive they will be biologically and clinically.
- the datasets are derived from gene expression profiling studies in embryonic cell lines and cancers of the prostate, breast, lung, brain, stomach, kidney, ovary and blood.
- the expression profile of ESTP genes that is, genes strongly regulated in ES tumor cells, allows to predict histological as well as biological subtypes with different clinical outcomes.
- strongly regulated applies to ESTP genes with a specific high expression level but also to ESTP genes with a specific low expression level.
- the present invention is additionally based on the hypothesis that strongly regulated ESTP genes in ES tumor cells, play a crucial role in tumor development and that, more specifically, different patterns of expression alterations of these ESTP genes determine tumor aggressiveness. According to the present invention this hypothesis is validated by using a large series of published datasets of genome-wide gene expression profiling in ES cells and in normal and tumor tissues for identifying ES genes of high prognostic power, that is, ESTP genes:
- arrays can be used to predict pathological and clinical characteristics of a tumor in a patient by applying a simple hierarchical cluster method to a corresponding dataset obtained for the respective tumor.
- high prognostic accuracy was obtained for all tumor types investigated, in particular prostate cancer but also gastric cancer, lung cancer, and leukaemia.
- prognostic accuracy was also obtained for breast cancer, ovary cancer, brain tumor, soft tissue tumor, and kidney cander.
- prognostic analysis is based on the genes with highest and lowest level of expression, that is, genes within ranges of expression which are near or comprise the level of maximal expression and of minimal expression.
- the present invention provides a prognostic method of predicting tumor pathological and clinical characteristics in a patient based on a restricted number of ES genes, such as less than 2,500 ES genes, more preferred less than 1,000, even more preferred from 500 to 750 ES genes, in particular from 600 to 680 ES genes, most preferred about 641 ES genes.
- ES genes used for prediction such as about 641 ES genes
- their specific functionality in stem cell biology allows errors due to biological and methodological background noise to be reduced or even eliminated.
- Virtual experimental methods based on such a restricted number of ES genes can be used for the diagnosis and prognosis of a broad spectrum of tumors. In contrast methods known in the art usually rely on few markers restricted to different tumor types.
- ESTP genes of the invention Based on the ESTP genes of the invention, a variety of robust analytical methods can be designed and applied in tumor diagnosis and prognosis using trace amounts of RNA derived from small tumor samples. For most tumors, such as prostate cancer, there is no method known in the art capable of predicting with good accuracy clinical outcome at an early stage of tumor development. It is in particular here that the prognostic method of the invention solves an important clinical problem.
- a first preferred aspect comprises selecting ES genes of predictive significance, that is, ESTP genes that constitute a minor proportion of all ES genes, in a cancer;
- genes with weak prediction power are eliminated from the list of ES genes identified by the method of the invention and thus from consideration, thereby reducing the number of ESTP genes and improving prediction accuracy;
- ESTP genes with high specificity are selected from the ES gene list obtained by the method of the invention for application to a specific type of tumor, such as prostate cancer or breast cancer;
- a specific type of tumor such as prostate cancer or breast cancer;
- methods known in the art used in diagnosis and prognosis of tumors are based on one or several ESTP genes identified by the method of the invention, such as multiplex or high throughput RT-PCR (reverse transcriptase polymerase chain reaction) using small amounts of tumor samples, a specific DNA microarray platform, and other low or high throughput RNA analytical methods.
- FNA biopsy for clinical diagnosis and prognosis allows sampling multiple areas to cover a large volume of a tumor due to its minimal morbidity, thus being superior in overcoming tumor heterogeneity.
- FNA biopsy is a preferred method for obtaining pure tumor samples for molecular diagnosis and prognosis from small tumors, in particular from early stage prostate tumors.
- Conventional cDNA array experiments require approximately 40 ⁇ g total RNA.
- FNA biopsy yields 100-2,000 ng total RNA (57-59). This small amount of RNA is sufficient for analyses by using a small array platform as well as by multiplex or other high throughput RT-PCR methods.
- a method of predicting the development of a cancer in a patient comprising:
- a method of predicting the development of a cancer in a patient comprising:
- genes in the first group and/or the second group are consecutive, that is, ranked consecutively, in respect of their expression levels.
- the total number of genes in the first and second groups is substantially smaller than the number of the genes in the third group, in particular less than a fifth of the number of the genes in the third group.
- the total number of genes in the first and second groups is preferably from 500 to 750, more preferred from 600 to 680, most preferred about 641.
- the genes pertaining to the first and second groups are preferably identified by employing a q value of from 0.01 to 0.1, more preferred of from 0.025 to 0.075, most preferred of about 0.05, in a one class significant analysis of microarrays (SAM) on a centered embryonic stem cell gene dataset by which all genes are ranked according to their expression levels
- SAM microarrays
- the method of the invention is applicable to cancer of any kind, in particular to prostate cancer, gastric cancer, lung cancer, and leukaemia.
- a second preferred aspect of the invention is disclosed the use of an embryonic stem cell gene DNA or RNA microarray for predicting the development of a cancer tumor in a patient.
- the microarray comprises DNA or RNA of a first group of embryonic stem cell genes with high level of expression in the tumor and of a second group of embryonic stem cell genes with a low level of expression in the tumor but not comprising DNA or RNA, respectively, of embryonic stem cell genes with an intermediate level of expression in the tumor.
- the genes in the first and second groups to be those ranked according to their expression levels, in particular in a consecutive manner.
- a preferred method of ranking is a one class significant analysis of microarray s (SAM) on a centered embryonic tumor stem cell gene dataset by employing a q value of from 0.01 to 0.1, more preferred of from 0.025 to 0.075, most preferred of about 0.05.
- the embryonic stem cell gene DNA or RNA microarray can be used for the predictions of the development of any cancer, in particular of prostate cancer, gastric cancer, lung cancer, and leukaemia and, furthermore, of breast cancer, ovary cancer, brain tumor, soft tissue tumor, and kidney tumour.
- a microarray comprising a fragment of embryonic stem cell gene DNA or RNA derived from a first group of embryonic stem cell genes with high level of expression in a cancer tumor and from a second group of embryonic stem cell genes with a low level of expression in said cancer tumor but not comprising a fragment of embryonic stem cell gene DNA/RNA with an intermediate level of expression in the tumor. It is particularly preferred for the genes in the first group and/or the second group to be ranked consecutively in respect of their expression levels.
- the genes in the first and second groups are those ranked according to their expression levels by a one class significant analysis of microarrays (SAM) on a centered embryonic tumor stem cell gene dataset by employing a q value of from 0.01 to 0.1, more preferred of from 0.025 to 0.075, most preferred of about 0.05.
- the cancer can be any cancer, in particular prostate cancer, gastric cancer, lung cancer, and leukaemia but also breast cancer, ovary cancer, brain tumor, soft tissue tumour, and kidney tumor.
- a probe comprising any of DNA, DNA fragment, DNA oligomer, DNA primer, RNA, RNA fragment, RNA oligomer of a first group of embryonic stem cell genes with high level of expression in a cancer tumor and of a second group of embryonic stem cell genes with a low level of expression in said cancer tumor but not comprising DNA, DNA fragment, DNA oligomer, DNA primer, RNA, RNA fragment, RNA oligomer, respectively, of embryonic stem cell genes with an intermediate level of expression in said cancer tumor.
- the genes in the first and second groups are those ranked, preferably consecutively, according to their expression levels by a one class significant analysis of microarrays (SAM) on a centered embryonic tumor stem cell gene dataset by employing a q value of from 0.01 to 0.1, more preferred of from 0.025 to 0.075, most preferred of about 0.05.
- the cancer can be any cancer, in particular prostate cancer, gastric cancer, lung cancer, and leukaemia but also breast cancer, ovary cancer, brain tumor, soft tissue tumor, and kidney cancer.
- a fifth preferred aspect of the invention is disclosed the use of a multitude of embryonic stem cell genes in a method of assessing the prognosis of a cancer tumor, wherein said multitude comprises a first group of embryonic stem cell genes with high level of expression in the tumor and of a second group of embryonic stem cell genes with a low level of expression in the tumor but does not comprise embryonic stem cell genes with an intermediate level of expression. It is preferred for the genes in the first and second groups to be ranked consecutively according to their expression levels and to constitute a fraction of the embryonic stem cell genes expressed in the tumor, in particular a fraction of 20 per cent or less of the embryonic stem cell genes expressed in the tumor.
- SAM microarrays
- the use relates to any type of cancer, preferably prostate cancer, gastric cancer, lung cancer, and leukaemia but also breast cancer, ovary cancer, brain tumor, soft tissue tumor, and kidney cancer.
- the ESTP genes in the first group and the second group can be for analysis of clinical tumor tissue biopsies or tumor cell aspirate samples using high throughput DNA microarrays for clinical diagnosis and prognosis.
- a gene microarray for probing the 641 or, less preferred, the aforementioned 1,000 or from 500 to 750 or, in particular, from 600 to 680 ESTP genes by spotting a DNA fragment (PCR products or oligos) of each of them on a glass or other suitable support.
- RNA isolated from tumor tissue biopsies or tumor cell aspirates can be labelled and hybridized with the ESTP gene microarray.
- the expression changes of all the 641 ES genes can be determined and compared with a group of standard reference cases with well defined data of clinical parameters such as histology, pathology and outcomes. The clinical outcomes of the new cases can thus be predicted.
- a second preferred use relies on a gene solution array, for instance one based on the xMAP technology (http://www.luminexcorp.com).
- Probes that specifically bind to RNA of the ESTP genes can be designed, synthesized and immobilized on the surface of of a microsphere or microbead support. RNA isolated from clinical tumor tissue biopsies or tumor cell aspirates can be bound to the support. Upon illuminating the beads/spheres with light of varying wavelength under laser beam activation the expression levels of the various ESTP genes in the tumor samples can be simultaneously and accurately measured. This method is simple, sensitive, and accurate and of high throughput; the expression levels of up to 100 genes can be in one experiment.
- a third preferred use comprises the design of probes for assembling an ESTP gene microarray or chip of any kinds, for the purpose of application in clinical diagnosis and prognosis of common cancers.
- high throughput PT-PCR can be used for analysis of clinical tumor tissue biopsies or tumor cell aspirate samples.
- design primers for each gene can be designed to carry out multiplex RT-PCR for determining the expression level of each gene in a tumor tissue or aspirate sample. Since the common RT-PCR platform can analyze 96 or multiple sets of 96 samples simultaneously, a small number of multiplex RT-PCR suffice to achieve high throughput measurement of the expression levels of the most preferred 641 ESTP genes or the less preferred 1000 or from 500 to 750 or, in particular, from 600 to 680 ESTP genes in a large set of clinical tumor tissue biopsies or aspirates.
- clinical tumor tissue biopsy samples and tumor cell aspirate samples can be analyzed using high throughput protein/antibody microarrays or an ELISA method.
- the protein sequence or a portion thereof can be retrieved from publicly available human genome sequence resources and used to produce specific monoclonal antibodies for targeting the proteins encoded by the respective ESTP genes.
- the specific antibodies can be assembled into an ES protein array or incorporated into a high throughput ELISA system to measure the protein expression levels of the most preferred 641 ESTP genes and the less preferred 1000 or from 500 to 750 or, in particular, from 600 to 680 ESTP genes in clinical tumor tissue biopsies and tumor cell aspirates.
- Fig. 1 is a graph illustrating the identification of ES predictor genes by a one-class SAM ranking test
- Fig. 2 is a gene expression profile obtained from biopsies of healthy and cancerous prostate tissue, and from embryonic stem cell lines, with a hierarchial clustering of the biopsies;
- Fig. 3 is a gene expression profile obtained from biopsies of healthy and cancerous lung tissue biopsies, and from embryonic stem cell lines, with a hierarchial clustering of the biopsies;
- Fig. 4 is a graph illustrating survival for the patients related to major cancerous lung tissue clusters of Fig. 3;
- Fig. 5 is a gene expression profile obtained from biopsies of healthy and cancerous stomach tissue biopsies, and from embryonic stem cell lines, with a hierarchial clustering of the biopsies;
- Fig. 6 is a graph illustrating survival for the patients related to major cancerous gastric tissue clusters of Fig. 5;
- Fig. 7 is a gene expression profile obtained from leukocytes of acute myeloid leukaemia patients, and from embryonic stem cell lines, with a hierarchial clustering of the leukocyte samples;
- Fig. 8 is a graph illustrating survival for the patients pertaining to the major acute myeloid leukaemia subtype clusters of Fig. 7.
- the method of the invention is based on published gene data such as the data sets published and deposited in the Stanford Microarray Database (SMD) (http://genome-www5.stanford.edu/). All array experiments used the same two-dye cDNA array platform with a common RNA reference, which enables reliable combination of or comparison with data from different experiments.
- SMD Stanford Microarray Database
- All array experiments used the same two-dye cDNA array platform with a common RNA reference, which enables reliable combination of or comparison with data from different experiments.
- These datasets include genome- wide expression data for embryonic stem cells (60), normal tissues from most of the human organs (61), and tumors from the prostate (62), breast, lung (63), stomach (64), liver (65), blood (66), brain (67), kidney (68), soft tissue (69), ovary (70; 71) and pancreas (72). In total about 1000 arrays were included in the analysis.
- Each array (tissue) in these datasets is denoted with corresponding basic clinical
- Data Collapse /Retrieval Raw data are retrieved and averaged by SUID; UID column contains NAME; Retrieved Log(base2) of R/G Normalized Ratio (Mean).
- Data filtering options Selected Data Filters: Spot is not flagged by experimenter.
- Data filters for GENEPIX result sets: Channel 1 Mean Intensity / Median Background Intensity > 1.5 AND Channel 2 Normalized (Mean Intensity / Median Background Intensity) > 1.5.
- the ES cell data set was combined with each of a number of other data sets. Genes and array batches were centered separately in each combined dataset as previously described (61 ; 62).
- ES predictor genes After centering a data set containing ES cells and normal tissues from most human organs, the ES data set was separated from the normal tissue data set. A one-class SAM (significant analysis of microarrays) was carried out using the centered ES dataset, by which all genes were ranked according to their expression levels in the ES cells (73). Using a q value equal to or less than 0.05 as cut-off, top 328 genes with highest level and top 313 genes with lowest level of expression in the ES cells were identified (Table 1). These 641 ES genes are named ES tumor predictor genes (ESTP genes).
- ESTP genes ES tumor predictor genes
- Prediction of clinical and pathological tumor types After centering each combined data set, a sub-dataset containing only the 641 ESTP genes was isolated from the original dataset. A simple hierarchical clustering was carried out based on this sub-dataset using genes with 70% qualified data in all samples (78). The sample grouping was directly correlated with the clinical and pathological information of each individual tissue sample. Prediction examples for a number of tumor types are given below. Prediction in other datasets is carried out in essentially the same manner. In the one class SAM analysis, numbers of genes selected is in correlation with q value. There were 201 genes selected when q value at 0.01, 641 genes selected when q value at 0.05, and 1368 genes selected when q value at 0.1.
- an increased q value would result in increased number of selected genes as well as increased number of genes that would not be associated with the transcriptional regulation in the ES cells.
- the 641 genes selected by q value at 0.05 had best classification (prediction) results, as shown in the prostate cancer (Table 2) and lung cancer (Table 3) materials. The difference was particularly obvious in respect of lung cancer (Table 3).
- the 641 genes selected by q value at 0.05 was the best choice of gene selection when both stem cell association and tumor classification are taken into consideration.
- the ESTP genes were derived from the ES cell dataset. The power of this set of genes in the classification of a broad spectrum of tumors was then validated in each independent tumor dataset.
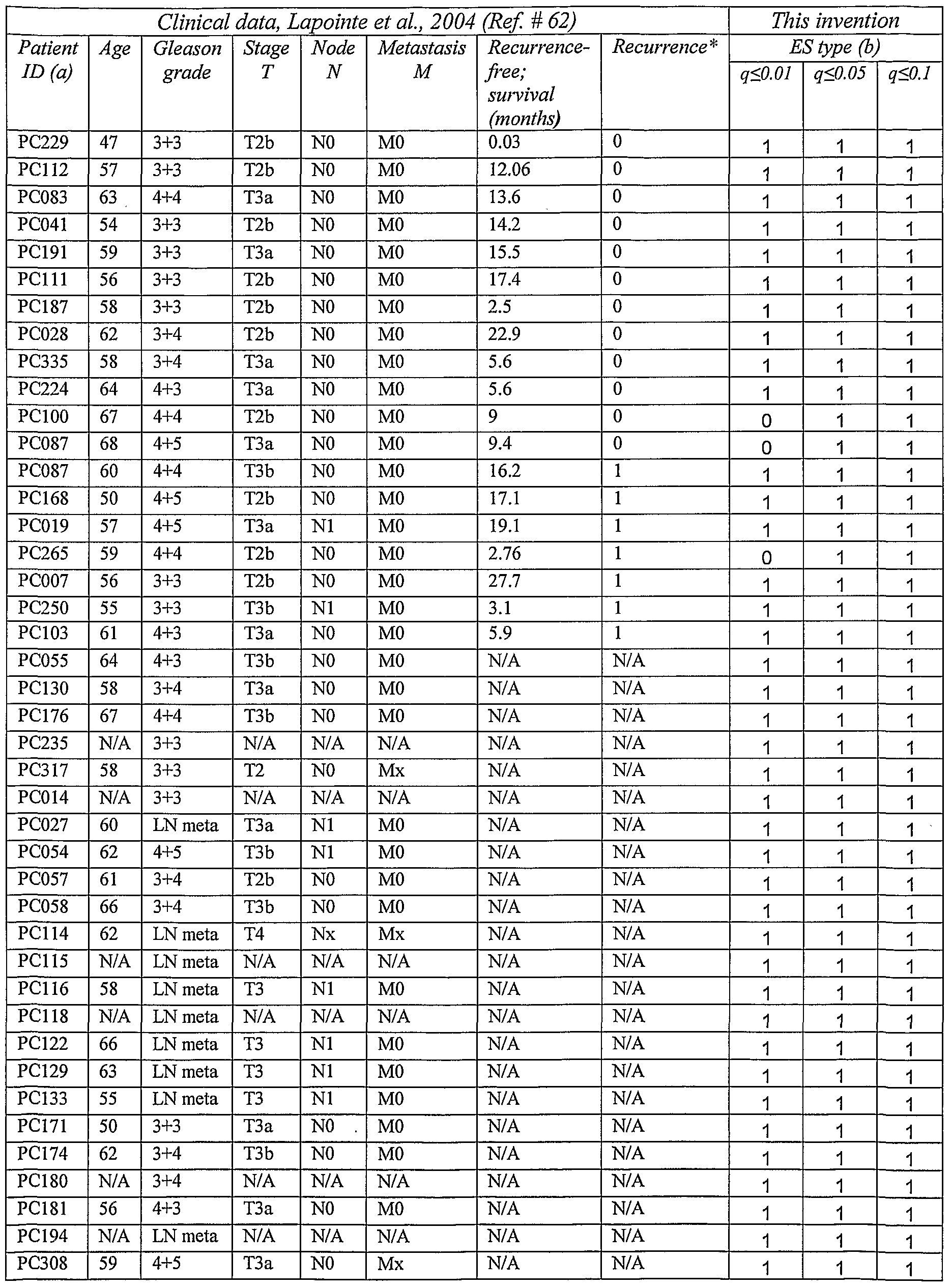
- Prostate cancer Published clinical data and predicted tumor subtype by ESTP genes of the invention for prostate cancer are listed in Table 2: Gleason grade, stage, biological subtype and short term recurrence (prostate specific antigen (PSA) survival) after radical surgery. Of the 641 ESTP genes, 505 had good data in 70% of all samples. In the gene expression profile of Fig. 2, the expression level (range in log ratio between -5.06 and 6.15) was transformed into a transitional color presentation, with red indicating above 0, black equal to 0 and green for less than 0; in Fig. 2 and the other figures illustrating gene expression profiles the colors are rendered in white, black, and grey (see, DESCRIPTION OF THE FIGURES).
- Prediction value for choice of treatment Patients with a tumor predicted to be of a recurrent type (pertaining to the recurrent group) should be treated by radical surgery at a very early stage even in case of a moderate or low Gleason score. Patients with a very early stage tumor predicted to be of a non-recurrent type (pertaining to the non-recurrent group) should be kept under regular PSA and other examination control, because most of the tumors in this group are in fact indolent or very slow-progressive.
- Lung cancer Lung cancer. Published clinical data and predicted tumor subtype by ESTP genes of the invention are shown in Table 3. Prediction of histological type and survival in lung cancer is illustrated in Fig. 3, tissue clustering by ESTP genes. Of the 641 ES predictor genes, 316 had qualified data in 70% or more of the samples.
- Lung cancer tissue samples were predictively sorted into two major groups, an adenocarcinoma group (a) that mainly contained adenocarcinomas, some normal lung tissues, ES cells and a few non- adenocarcinomas, and a (b) non-adenocarcinoma group that contained most non- adenocarcinomas including squamous cell carcinoma, large cell lung cancer and small cell lung cancer, together with a fraction of adenocarcinomas.
- adenocarcinoma has a better prognosis than other types of lung cancer. Survival analysis based on lung adenocarcinoma subtypes is illustrated in Fig. 4.
- adenocarcinoma cases in the non-adenocarcinoma group (b) further showed shorter survival than adenocarcinoma cases in the adenocarcinoma group (a) as shown in Fig. 3, adenocarcinoma subtypes by ES predictor genes associated with survival.
- tumors predicted to pertain to the adenocarcinoma group seem to have a generally favorable outcome after radical surgery at a very early stage; whereas tumors in the non-adenocarcinoma group may respond relatively better to chemotherapy such as to Iressa or radiation.
- Gastric cancer Gastric cancer. Published clinical data and tumor subtype predicted by ESTP genes of the invention are illustrated in Table 4. The prediction of histological types and survival in gastric cancer is illustrated in Figure 5: (a) tissue clustering by ES predictor genes; (b) issue subtypes by ES predictor genes associated with survival.
- Prediction of subtypes of gastric cancer by ESTP genes of the 641 ESTP genes 613 had qualified data in 70% of all samples.
- Gastric tumors were classified into two major subtypes, type 1 enriched in tumors with diffuse and mix histological types generally with poor prognosis, type 0 together with most normal gastric tissue samples.
- the survival time for gastric cancer patients pertaining to these groups is compared in Fig. 6.
- the subtype 0 tumors can be further divided into two sub-subtypes, one with the A subtype enriched in EB virus positive tumors, the other not.
- Predictive value a) EBV infection is linked to gastric cancer via stem cell biology.
- Preventing an EBV infection by vaccination may have preventive effect on gastric cancer; b) Diffused type of gastric cancer has very strong hereditary tendency.
- Fig. 7 illustrates the prediction of subtypes of acute mononucleocyte leukemia associated with chromosome aberration and survival: (a) classification by ESTP genes; (b) AML subtypes associated with survival. Prediction of acute myeloid leukemia (AML) by ESTP genes: of the 641 ES predictor genes, 324 had qualified data in 70% of all samples.
- AML acute myeloid leukemia
- AML cases were classified into two major subtypes, type 1 enriched in cases with t(8;21) and del7q chromosomal aberrations, and type 0, which was further divided into two sub-subtypes A and B the first with a subtype enriched with inv(16), the second enriched with t(15;17).
- Type 1 cases showed shorter overall survival than type 0 as presented in Figure 8. Survival analysis was based on AML subtypes predicted in Fig. 4a and the published clinical data in Table 5.
- Predictive value for treatment choices AML with different chromosomal aberrations responds to different chemotherapies; in particular all-trans retinoic acid can induce differentiation of AML with t(l 5; 17) translocation. It is suggested that AML in the group enriched with t(15;17) but without the translocation detected by cytogenetic diagnostic method may show good response to all-trans retinoic acid due to the same stem cell biological alteration.
- ES typing according to the present invention is significantly better than conventional histological grading in the prognosis of lung adenocarcinoma.
- cases # 222-97 and # 226-97 were of grade 3 that would be poorly differentiated with poor outcome according to conventional clinical prognostic methods.
- the cases are classified as being of ES type 0 that would have a relatively good outcome.
- the patients were recurrence-free more than 48 months after radical surgery.
- ES typing by the method of the invention is more accurate than by conventional histological grading.
- FIG. 1 Identification of ESTP genes by a one-class SAM ranking test. There were 24361 genes with qualified expression data in 75% of the 6 embryonic stem (ES) cell lines. These 24361 genes were ranked according to their homogenous expression levels in the ES cells by a one-class SAM (significant analysis of microarrays) method as shown in this figure. At delta 0.23, q value ⁇ 0.05, 328 genes with highest expression levels and 313 genes with lowest expression levels were identified. The expression changes of these 641 genes in different tumor samples showed also strongest classification power as compared to genes located within the cut-off lines.
- ES embryonic stem
- the expression level (range in log ratio between -5.06 and 6.15) was transformed into a transitional gray-black scale presentation, with black indicating above 1, median gray indicate equal to 1 and green for less than 1.
- all samples were classified by hierarchical clustering into distinct groups as normal prostate, prostate cancer aggressive group type 1 that contained all cases with recurrence, prostate cancer non-aggressive group type 0 that contained only cases without recurrence.
- a healthy tissue sample was provided from an unaffected prostate area.
- These normal samples formed the "normal” cluster in Fig. 1.
- ES embryonic stem
- EC embryonic carcinoma
- patients whose tumor is predicted in the aggressive group type 1 should be treated by radical surgery at very early stage even if the tumor Gleason score is not high; whereas patients whose tumor is predicted in the non-aggressive group type 0 should be under regular PSA and other examination control if the tumor is at very early stage, because most of the tumors in this group are in fact indolent or progress very slowly.
- FIG. 3 Prediction of lung cancer tissue type. Of the 641 ESTP genes, 316 had qualified data in 70% or more of the samples. Lung cancer tissue samples were predicted into two major groups, adenocarcinoma group type 0 that mainly contained adenocarcinomas, some normal lung tissues, ES cells and a few non-adenocarcinomas, and non-adenocarcinoma group type 1 that contained most non-adenocarcinomas including squamous cell carcinoma, large cell lung cancer and small cell lung cancer, together with a fraction of adenocarcinomas. In general, adenocarcinoma has relatively better prognosis than other types of lung cancer.
- the adenocarcinoma cases in the non- adenocarcinoma group type 1 further showed shorter survival than adenocarcinoma cases in the adenocarcinoma group type 0 as shown in Fig. 4.
- ES embryonic stem
- EC embryonic carcinoma
- FIG. 5 Prediction of subtypes of gastric cancer by ESTP genes. Of the 641 ESTP genes, 613 had qualified measuring in 70% of all samples. Gastric tumors were classified into two major subtypes, type 1 enriched with diffuse type and mix type tumors generally with poor prognosis, type 0 together with most normal gastric tissue samples. Type 0 tumors was further divided into two subtypes with the a subtype enriched with tumors with EB virus-positive. One tumor sample was provided from each gastric cancer patient. From some of the patients also a normal sample was taken from an unaffected stomach area. These "normal" samples formed the normal cluster in Fig. 5. There were 6 embryonic stem (ES) cell lines from non-prostate cancer subjects. In addition 10 embryonic carcinoma (EC) cell lines from patients with embryonic carcinoma were also included. These ES and EC cell lines were used as reference to indicate different patterns of gene expression.
- ES embryonic stem
- EC embryonic carcinoma
- EBV infection is linked to gastric cancer via stem cell biology. Preventing EBV infection by vaccination may have preventing effect on gastric cancer; b) diffused type of gastric cancer has a very strong hereditary tendency.
- FIG. 6 Gastric cancer survival analysis. The analysis was based on gastric cancer subtypes predicted in Fig. 5 and on the published clinical data reproduced in Table 4. Time unit: months.
- FIG. 7 Prediction of acute myeloid leukemia (AML) by ESTP genes.
- AML cases were classified into two major subtypes, type 1 enriched in cases with t(8;21) and del7q chromosomal aberrations, type 0 that was further divided into two subtypes a and b with a subtype enriched inv(16) and b subtype enriched with t(15;17).
- Type 1 cases showed shorter overall survival than type 0 as presented in Fig. 5. From each patient one leukocyte sample was harvested. There were 6 embryonic stem (ES) cell lines from non-prostate cancer subjects.
- ES embryonic stem
- embryonic carcinoma (EC) cell lines from patients with embryonic carcinoma were also included. These ES and EC cell lines were used as reference to indicate different patterns of gene expression. Importance of the prediction for treatment choices: AML with different chromosomal aberrations respond to different chemotherapies, in particular all-trans retinoic acid can induce differentiation of AML with t(15;17) translocation. It is highly possible that AML in the group enriched with t(15;17) but without the translocation detected by cytogenetic diagnostic method can show good response to all-trans retinoic acid due to the same stem cell biological alteration.
- Figure 8 Leukemia survival analysis. The analysis was based on AML subtypes predicted in Fig. 7 and on the published clinical data reproduced in Table 5. Time unit: months.
- van de Vijver MJ et al. A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med, 2002; 347(25): 1999-2009. 6. van 't Veer LJ et al., Gene expression profiling predicts clinical outcome of breast cancer. Nature, 2002; 415(6871): 530-536.
- Johansson JE et al. Natural history of early, localized prostate cancer. Jama, 2004; 291(22): 2713-2719.
- Partin AW et al. Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer. A multi-institutional update. Jama, 1997; 277(18): 1445-1451. 18. Partin AW et al, The use of prostate specific antigen, clinical stage and
- Chetcuti A et al. Identification of differentially expressed genes in organ- confined prostate cancer by gene expression array. Prostate, 2001; 47(2): 132- 140.
- LN meta lymph node metastasis.
- N/A non available.
- Table 3 presents clinical data from lung adenocarcinoma cases only.
- cases with non-adenocarcinoma are included, comprising large cell lung cancer, small cell lung cancer, and squamous cell lung cancer.
- the non-adenocarcinoma cases were analyzed by gene expression profiling in the original publication but lacked clinical follow-up data.
- (b) By choosing different q value cut-off at 0.01, 0.05 and 0.1, 201, 641, and 1386, respectively, significant ES genes were selected. Using the expression profile of the corresponding gene lists for tumor aggressiveness prediction provided slightly different results as shown Table 3. The q ⁇ 0.05 gene list gave the best prediction.
- the ES type was determined by using the gene list of 641 ES predictor genes selected at q ⁇ 0.05 in the one-class SAM.
- the ES type was determined by using the gene list of 641 ES predictor genes selected at q ⁇ 0.05 in the one-class SAM.
- RNASEL ribonuclease L (2',5'-oligoisoadenylate synthetase-dependent)/hereditary prostate
- AML acute myeloid leukemia AML acute myeloid leukemia
- AML acute myeloid leukemia AML acute myeloid leukemia.
Landscapes
- Chemical & Material Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Health & Medical Sciences (AREA)
- Organic Chemistry (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Engineering & Computer Science (AREA)
- Immunology (AREA)
- Pathology (AREA)
- Analytical Chemistry (AREA)
- Zoology (AREA)
- Genetics & Genomics (AREA)
- Wood Science & Technology (AREA)
- Physics & Mathematics (AREA)
- Biotechnology (AREA)
- Microbiology (AREA)
- Molecular Biology (AREA)
- Hospice & Palliative Care (AREA)
- Biophysics (AREA)
- Oncology (AREA)
- Biochemistry (AREA)
- Bioinformatics & Cheminformatics (AREA)
- General Engineering & Computer Science (AREA)
- General Health & Medical Sciences (AREA)
- Measuring Or Testing Involving Enzymes Or Micro-Organisms (AREA)
Abstract
Description







Claims
Priority Applications (5)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US12/375,177 US20100009858A1 (en) | 2006-07-28 | 2007-07-16 | Embryonic stem cell markers for cancer diagnosis and prognosis |
| EP07769001A EP2052089A4 (en) | 2006-07-28 | 2007-07-16 | EMBRYONIC STEM CELL MARKERS FOR ESTABLISHING DIAGNOSIS OR PROGNOSIS OF CANCER |
| AU2007277508A AU2007277508A1 (en) | 2006-07-28 | 2007-07-16 | Embryonic stem cell markers for cancer diagnosis and prognosis |
| CA 2659231 CA2659231A1 (en) | 2006-07-28 | 2007-07-16 | Embryonic stem cell markers for cancer diagnosis and prognosis |
| IL196774A IL196774A0 (en) | 2006-07-28 | 2009-01-28 | Embryonic stem cell markers for a cancer diagnosis and prognosis |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| SE0601615-8 | 2006-07-28 | ||
| SE0601615 | 2006-07-28 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2008013492A1 true WO2008013492A1 (en) | 2008-01-31 |
Family
ID=38981730
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/SE2007/000689 Ceased WO2008013492A1 (en) | 2006-07-28 | 2007-07-16 | Embryonic stem cell markers for cancer diagnosis and prognosis |
Country Status (6)
| Country | Link |
|---|---|
| US (1) | US20100009858A1 (en) |
| EP (1) | EP2052089A4 (en) |
| AU (1) | AU2007277508A1 (en) |
| CA (1) | CA2659231A1 (en) |
| IL (1) | IL196774A0 (en) |
| WO (1) | WO2008013492A1 (en) |
Cited By (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2011025542A1 (en) * | 2009-08-31 | 2011-03-03 | Ludwig Institute For Cancer Research Ltd. | Seromic analysis of ovarian cancer |
| WO2013060739A1 (en) | 2011-10-24 | 2013-05-02 | Chundsell Medicals Ab | Marker genes for prostate cancer classification |
| EP2356446A4 (en) * | 2008-11-14 | 2014-03-19 | Brigham & Womens Hospital | DIAGNOSTIC AND THERAPEUTIC METHODS RELATING TO CANCER STEM CELLS |
| US8906864B2 (en) | 2005-09-30 | 2014-12-09 | AbbVie Deutschland GmbH & Co. KG | Binding domains of proteins of the repulsive guidance molecule (RGM) protein family and functional fragments thereof, and their use |
| US8962803B2 (en) | 2008-02-29 | 2015-02-24 | AbbVie Deutschland GmbH & Co. KG | Antibodies against the RGM A protein and uses thereof |
| US9102722B2 (en) | 2012-01-27 | 2015-08-11 | AbbVie Deutschland GmbH & Co. KG | Composition and method for the diagnosis and treatment of diseases associated with neurite degeneration |
| US9175075B2 (en) | 2009-12-08 | 2015-11-03 | AbbVie Deutschland GmbH & Co. KG | Methods of treating retinal nerve fiber layer degeneration with monoclonal antibodies against a retinal guidance molecule (RGM) protein |
| US11542328B2 (en) | 2008-11-14 | 2023-01-03 | The Brigham And Women's Hospital, Inc. | Therapeutic and diagnostic methods relating to cancer stem cells |
| US12448461B2 (en) | 2018-04-25 | 2025-10-21 | Children's Medical Center Corporation | ABCB5 ligands and substrates |
| US12460260B2 (en) | 2019-05-23 | 2025-11-04 | The Board Of Trustees Of Leland Stanford Junior University | Methods utilizing single cell genetic data for cell population analysis and applications thereof |
Families Citing this family (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10648035B2 (en) | 2012-11-26 | 2020-05-12 | The Johns Hopkins University | Methods and compositions for diagnosing and treating gastric cancer |
| US9804162B2 (en) * | 2015-08-31 | 2017-10-31 | The University Of Hong Kong | Pleural fluid markers for malignant pleural effusions |
| WO2018174861A1 (en) * | 2017-03-21 | 2018-09-27 | Mprobe Inc. | Methods and compositions for detecting early stage breast cancer with rna-seq expression profiling |
Citations (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US6090559A (en) * | 1996-03-29 | 2000-07-18 | Urocor, Inc. | Biomarkers for the detection of prostate cancer |
Family Cites Families (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US6984522B2 (en) * | 2000-08-03 | 2006-01-10 | Regents Of The University Of Michigan | Isolation and use of solid tumor stem cells |
| WO2006135886A2 (en) * | 2005-06-13 | 2006-12-21 | The Regents Of The University Of Michigan | Compositions and methods for treating and diagnosing cancer |
-
2007
- 2007-07-16 WO PCT/SE2007/000689 patent/WO2008013492A1/en not_active Ceased
- 2007-07-16 US US12/375,177 patent/US20100009858A1/en not_active Abandoned
- 2007-07-16 AU AU2007277508A patent/AU2007277508A1/en not_active Abandoned
- 2007-07-16 EP EP07769001A patent/EP2052089A4/en not_active Withdrawn
- 2007-07-16 CA CA 2659231 patent/CA2659231A1/en not_active Abandoned
-
2009
- 2009-01-28 IL IL196774A patent/IL196774A0/en unknown
Patent Citations (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US6090559A (en) * | 1996-03-29 | 2000-07-18 | Urocor, Inc. | Biomarkers for the detection of prostate cancer |
Non-Patent Citations (18)
| Title |
|---|
| EISEN MB ET AL.: "Cluster analysis and display of genome-wide expression patterns", PROC NATL ACAD SCI USA, vol. 95, no. 25, 1998, pages 14863 - 14868, XP002939285, DOI: doi:10.1073/pnas.95.25.14863 |
| GLINSKY G.V. ET AL.: "Microarray analysis identifies a death-from-cancer signature predicting therapy failure in patients with multiple types of cancer", THE JOURNAL OF CLINICAL INVESTIGATION, vol. 115, no. 6, June 2005 (2005-06-01), pages 1503 - 1521, XP002460132 * |
| HOLMBERG L ET AL.: "A randomized trial comparing radical prostatectomy with watchful waiting in early prostate cancer", N ENGL J MED, vol. 347, no. 11, 2002, pages 781 - 789 |
| ISAACS W ET AL.: "Focus on prostate cancer", CANCER CELL, vol. 2, no. 2, 2002, pages 113 - 116 |
| JEMAL A ET AL.: "Cancer Statistics, 2005.", CA CANCER J CLIN, vol. 55, no. 1, 2005, pages 10 - 30 |
| JOHANSSON JE ET AL.: "Natural history of early, localized prostate cancer", JAMA |
| LAHAD J.P. ET AL.: "Stem cell-ness: a "magic marker" for cancer", THE JOURNAL OF CLINICAL INVESTIGATION, vol. 115, no. 6, June 2005 (2005-06-01), pages 1463 - 1467, XP003018693 * |
| LAPOINTE J ET AL.: "Gene expression profiling identifies clinically relevant subtypes of prostate cancer", PROC NATL ACAD SCI USA, vol. 101, no. 3, 2004, pages 811 - 816, XP002395334, DOI: doi:10.1073/pnas.0304146101 |
| PEROU CM ET AL.: "Molecular portraits of human breast tumours", NATURE, vol. 406, no. 6797, 2000, pages 747 - 752, XP008138703, DOI: doi:10.1038/35021093 |
| See also references of EP2052089A4 |
| SHERLOCK G; OF FISH, NAT METHODS, vol. 2, no. 5, 2005, pages 329 - 330 |
| SINGH R ET AL.: "Microarray based comparison of three amplification methods for nanogram amounts of total RNA", AM J PHYSIOL CELL PHYSIOL, 2004 |
| SORLIE T ET AL.: "Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications", PROC NATL ACAD SCI USA, vol. 98, no. 19, 2001, pages 10869 - 10874, XP002215483, DOI: doi:10.1073/pnas.191367098 |
| SPERGER J.M. ET AL.: "Gene expression patterns in human embryonic stem cells and human pluripotent germ cell tumors", PNAS, vol. 100, no. 23, 11 November 2003 (2003-11-11), pages 13350 - 13355, XP002350244 * |
| TUSHER VG ET AL.: "Significance analysis ofmicroarrays applied to the ionizing radiation response", PROC NATL ACAD SCI USA, vol. 98, no. 9, 2001, pages 5116 - 5121 |
| VAN DE VIJVER MJ ET AL.: "A gene-expression signature as a predictor of survival in breast cancer", N ENGL J MED, vol. 347, no. 25, 2002, pages 1999 - 2009, XP008032093, DOI: doi:10.1056/NEJMoa021967 |
| VAN'T VEER LJ ET AL.: "Gene expression profiling predicts clinical outcome of breast cancer", NATURE, vol. 415, no. 6871, 2002, pages 530 - 536, XP008138701, DOI: doi:10.1038/415530a |
| VARAMBALLY S ET AL.: "The polycomb group protein EZH2 is involved in progression of prostate cancer", NATURE, vol. 419, no. 6907, 2002, pages 624 - 629, XP002969193, DOI: doi:10.1038/nature01075 |
Cited By (23)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US8906864B2 (en) | 2005-09-30 | 2014-12-09 | AbbVie Deutschland GmbH & Co. KG | Binding domains of proteins of the repulsive guidance molecule (RGM) protein family and functional fragments thereof, and their use |
| US9605069B2 (en) | 2008-02-29 | 2017-03-28 | AbbVie Deutschland GmbH & Co. KG | Antibodies against the RGM a protein and uses thereof |
| US8962803B2 (en) | 2008-02-29 | 2015-02-24 | AbbVie Deutschland GmbH & Co. KG | Antibodies against the RGM A protein and uses thereof |
| US10316085B2 (en) | 2008-11-14 | 2019-06-11 | Children's Medical Center Corporation | Therapeutic and diagnostic methods relating to cancer stem cells |
| EP2356446A4 (en) * | 2008-11-14 | 2014-03-19 | Brigham & Womens Hospital | DIAGNOSTIC AND THERAPEUTIC METHODS RELATING TO CANCER STEM CELLS |
| US11542328B2 (en) | 2008-11-14 | 2023-01-03 | The Brigham And Women's Hospital, Inc. | Therapeutic and diagnostic methods relating to cancer stem cells |
| EP3978928A1 (en) * | 2008-11-14 | 2022-04-06 | The Brigham and Women's Hospital, Inc. | Therapeutic and diagnostic methods relating to cancer stem cells |
| EP3130923A1 (en) * | 2008-11-14 | 2017-02-15 | The Brigham and Women's Hospital, Inc. | Therapeutic and diagnostic methods relating to cancer stem cells |
| WO2011025542A1 (en) * | 2009-08-31 | 2011-03-03 | Ludwig Institute For Cancer Research Ltd. | Seromic analysis of ovarian cancer |
| US9175075B2 (en) | 2009-12-08 | 2015-11-03 | AbbVie Deutschland GmbH & Co. KG | Methods of treating retinal nerve fiber layer degeneration with monoclonal antibodies against a retinal guidance molecule (RGM) protein |
| CN104024436A (en) * | 2011-10-24 | 2014-09-03 | 纯德赛尔医药公司 | Marker genes for prostate cancer classification |
| CN104024436B (en) * | 2011-10-24 | 2016-10-19 | 纯德赛尔医药公司 | Marker genes for prostate cancer classification |
| US12060617B2 (en) | 2011-10-24 | 2024-08-13 | Prostatype Genomics Ab | Marker genes for prostate cancer classification |
| JP2015501151A (en) * | 2011-10-24 | 2015-01-15 | チュンドセル・メディカルズ・エービーChundsell Medicals AB | Marker genes for classification of prostate cancer |
| US9790555B2 (en) | 2011-10-24 | 2017-10-17 | Chundsell Medicals Ab | Marker genes for prostate cancer classification |
| US20140243433A1 (en) * | 2011-10-24 | 2014-08-28 | Chundsell Medicals Ab | Marker genes for prostate cancer classification |
| WO2013060739A1 (en) | 2011-10-24 | 2013-05-02 | Chundsell Medicals Ab | Marker genes for prostate cancer classification |
| US20210017606A1 (en) * | 2011-10-24 | 2021-01-21 | Chundsell Medicals Ab | Marker Genes for Prostate Cancer Classification |
| US9365643B2 (en) | 2012-01-27 | 2016-06-14 | AbbVie Deutschland GmbH & Co. KG | Antibodies that bind to repulsive guidance molecule A (RGMA) |
| US10106602B2 (en) | 2012-01-27 | 2018-10-23 | AbbVie Deutschland GmbH & Co. KG | Isolated monoclonal anti-repulsive guidance molecule A antibodies and uses thereof |
| US9102722B2 (en) | 2012-01-27 | 2015-08-11 | AbbVie Deutschland GmbH & Co. KG | Composition and method for the diagnosis and treatment of diseases associated with neurite degeneration |
| US12448461B2 (en) | 2018-04-25 | 2025-10-21 | Children's Medical Center Corporation | ABCB5 ligands and substrates |
| US12460260B2 (en) | 2019-05-23 | 2025-11-04 | The Board Of Trustees Of Leland Stanford Junior University | Methods utilizing single cell genetic data for cell population analysis and applications thereof |
Also Published As
| Publication number | Publication date |
|---|---|
| EP2052089A4 (en) | 2010-05-05 |
| AU2007277508A1 (en) | 2008-01-31 |
| CA2659231A1 (en) | 2008-01-31 |
| US20100009858A1 (en) | 2010-01-14 |
| AU2007277508A2 (en) | 2009-05-14 |
| IL196774A0 (en) | 2009-11-18 |
| EP2052089A1 (en) | 2009-04-29 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| WO2008013492A1 (en) | Embryonic stem cell markers for cancer diagnosis and prognosis | |
| JP7042784B2 (en) | How to Quantify Prostate Cancer Prognosis Using Gene Expression | |
| Bibikova et al. | Expression signatures that correlated with Gleason score and relapse in prostate cancer | |
| JP4938672B2 (en) | Methods, systems, and arrays for classifying cancer, predicting prognosis, and diagnosing based on association between p53 status and gene expression profile | |
| US20110224313A1 (en) | Compositions and methods for classifying lung cancer and prognosing lung cancer survival | |
| JP2009528825A (en) | Molecular analysis to predict recurrence of Dukes B colorectal cancer | |
| JP2008521412A (en) | Lung cancer prognosis judging means | |
| EP1754795A1 (en) | Predicting bone relapse of breast cancer | |
| JP2014516531A (en) | Biomarkers for lung cancer | |
| CN103403543A (en) | Colon cancer gene expression signatures and methods of use | |
| US20090192045A1 (en) | Molecular staging of stage ii and iii colon cancer and prognosis | |
| WO2015073949A1 (en) | Method of subtyping high-grade bladder cancer and uses thereof | |
| US20160222461A1 (en) | Methods and kits for diagnosing the prognosis of cancer patients | |
| Gao et al. | Clinical significance of multiple gene detection with a 22-gene panel in formalin-fixed paraffin-embedded specimens of 207 colorectal cancer patients | |
| JP6106257B2 (en) | Diagnostic methods for determining the prognosis of non-small cell lung cancer | |
| US8728738B2 (en) | Method for predicting clinical outcome of patients with non-small cell lung carcinoma | |
| US20200370122A1 (en) | Immune index methods for predicting breast cancer outcome | |
| US20210404018A1 (en) | Unbiased dna methylation markers define an extensive field defect in histologically normal prostate tissues associated with prostate cancer: new biomarkers for men with prostate cancer | |
| JP7471601B2 (en) | Molecular signatures and their use for identifying low-grade prostate cancer - Patents.com | |
| JP2014501496A (en) | Signature of clinical outcome in gastrointestinal stromal tumor and method of treatment of gastrointestinal stromal tumor | |
| Furge et al. | Gene expression profiling in kidney cancer: combining differential expression and chromosomal and pathway analyses | |
| Parker | Clinical implementation of breast cancer genomics |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| DPE2 | Request for preliminary examination filed before expiration of 19th month from priority date (pct application filed from 20040101) | ||
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 07769001 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2007277508 Country of ref document: AU |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 173/MUMNP/2009 Country of ref document: IN |
|
| ENP | Entry into the national phase |
Ref document number: 2659231 Country of ref document: CA |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 12375177 Country of ref document: US |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2007277508 Country of ref document: AU Date of ref document: 20070716 Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2007769001 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: RU |