WO2013172344A1 - 高血中高感度c反応性蛋白質患者の心血管疾患一次予防剤 - Google Patents
高血中高感度c反応性蛋白質患者の心血管疾患一次予防剤 Download PDFInfo
- Publication number
- WO2013172344A1 WO2013172344A1 PCT/JP2013/063419 JP2013063419W WO2013172344A1 WO 2013172344 A1 WO2013172344 A1 WO 2013172344A1 JP 2013063419 W JP2013063419 W JP 2013063419W WO 2013172344 A1 WO2013172344 A1 WO 2013172344A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- cardiovascular disease
- epa
- ratio
- subject
- risk
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Images


Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/185—Acids; Anhydrides, halides or salts thereof, e.g. sulfur acids, imidic, hydrazonic or hydroximic acids
- A61K31/19—Carboxylic acids, e.g. valproic acid
- A61K31/20—Carboxylic acids, e.g. valproic acid having a carboxyl group bound to a chain of seven or more carbon atoms, e.g. stearic, palmitic, arachidic acids
- A61K31/202—Carboxylic acids, e.g. valproic acid having a carboxyl group bound to a chain of seven or more carbon atoms, e.g. stearic, palmitic, arachidic acids having three or more double bonds, e.g. linolenic
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/21—Esters, e.g. nitroglycerine, selenocyanates
- A61K31/215—Esters, e.g. nitroglycerine, selenocyanates of carboxylic acids
- A61K31/22—Esters, e.g. nitroglycerine, selenocyanates of carboxylic acids of acyclic acids, e.g. pravastatin
- A61K31/23—Esters, e.g. nitroglycerine, selenocyanates of carboxylic acids of acyclic acids, e.g. pravastatin of acids having a carboxyl group bound to a chain of seven or more carbon atoms
- A61K31/232—Esters, e.g. nitroglycerine, selenocyanates of carboxylic acids of acyclic acids, e.g. pravastatin of acids having a carboxyl group bound to a chain of seven or more carbon atoms having three or more double bonds, e.g. etretinate
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P7/00—Drugs for disorders of the blood or the extracellular fluid
- A61P7/12—Antidiuretics, e.g. drugs for diabetes insipidus
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P9/00—Drugs for disorders of the cardiovascular system
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P9/00—Drugs for disorders of the cardiovascular system
- A61P9/10—Drugs for disorders of the cardiovascular system for treating ischaemic or atherosclerotic diseases, e.g. antianginal drugs, coronary vasodilators, drugs for myocardial infarction, retinopathy, cerebrovascula insufficiency, renal arteriosclerosis
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6893—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids related to diseases not provided for elsewhere
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/92—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving lipids, e.g. cholesterol, lipoproteins, or their receptors
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N30/00—Investigating or analysing materials by separation into components using adsorption, absorption or similar phenomena or using ion-exchange, e.g. chromatography or field flow fractionation
- G01N30/02—Column chromatography
- G01N30/88—Integrated analysis systems specially adapted therefor, not covered by a single one of the groups G01N30/04 - G01N30/86
- G01N2030/8809—Integrated analysis systems specially adapted therefor, not covered by a single one of the groups G01N30/04 - G01N30/86 analysis specially adapted for the sample
- G01N2030/8813—Integrated analysis systems specially adapted therefor, not covered by a single one of the groups G01N30/04 - G01N30/86 analysis specially adapted for the sample biological materials
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/46—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans from vertebrates
- G01N2333/47—Assays involving proteins of known structure or function as defined in the subgroups
- G01N2333/4701—Details
- G01N2333/4737—C-reactive protein
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/28—Neurological disorders
- G01N2800/2871—Cerebrovascular disorders, e.g. stroke, cerebral infarct, cerebral haemorrhage, transient ischemic event
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/32—Cardiovascular disorders
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/32—Cardiovascular disorders
- G01N2800/324—Coronary artery diseases, e.g. angina pectoris, myocardial infarction
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/32—Cardiovascular disorders
- G01N2800/325—Heart failure or cardiac arrest, e.g. cardiomyopathy, congestive heart failure
Definitions
- the present invention relates to a primary preventive agent for cardiovascular disease, a marker for evaluating cardiovascular disease risk, a method for extracting a subject having a high cardiovascular disease risk, and / or a primary preventive method for cardiovascular disease.
- Cardiovascular disease is the leading cause of death in developed countries. Although primary and secondary prevention has become an important national health issue, recently the importance of primary prevention to prevent disease has become more widely recognized.
- arteriosclerosis There is a common pathology of arteriosclerosis in the background of cardiovascular diseases such as coronary artery disease and stroke. Risk factors for arteriosclerosis include smoking, dyslipidemia (hyperlipidemia), hypertension, diabetes, obesity and lack of exercise. Therefore, in order to reduce the risk of developing cardiovascular disease, it is important to reduce these risk factors as much as possible.
- arteriosclerotic disease prevention guideline 2012 edition (Non-patent document 1), patients diagnosed with dyslipidemia have arteriosclerotic diseases (coronary artery disease based on atherosclerosis, stroke and obstructive artery). Targets are set for each management category based on the degree of risk (absolute risk) that occurs. More specifically, the management target is set by stratification according to the presence or absence of additional risk of diabetes, chronic kidney disease, non-cardiogenic cerebral infarction and peripheral arterial disease. In primary prevention (if you have never developed coronary artery disease), first improve your lifestyle, then consider taking medication, and in secondary prevention (if you have ever developed coronary artery disease) It is said that pharmacotherapy is considered along with improvement of lifestyle habits.
- statin drugs As a therapeutic agent for dyslipidemia (especially, high-low density lipoprotein (hereinafter sometimes referred to as “LDL”) cholesterolemia) used for drug therapy, a statin drug (hydroxymethylglutari-CoA (hereinafter referred to as “hydroxymethylglutarate-CoA”) Sometimes referred to as “HMG-CoA.” Reductase inhibitors) are commonly used.
- Statin drugs that appeared in the late 1980s are now sold in more than 100 countries around the world and are said to be taken by more than 30 million people every day.
- statin drugs are recommended as therapeutic agents for high LDL cholesterolemia, and icosapent can be used for high-risk dyslipidemias associated with cardiovascular diseases such as diabetes and hypertension.
- the administration of an acid (hereinafter sometimes referred to as “EPA”) is considered.
- the EPA formulation contains, for example, high purity icosapentic acid ethyl ester extracted from sardine oil, esterified and purified (hereinafter sometimes referred to as “EPA-E”) as an active ingredient, and neutral blood in blood.
- EPA-E high purity icosapentic acid ethyl ester extracted from sardine oil, esterified and purified
- Patent Document 1 discloses a cardiovascular event that is useful for prevention (secondary prevention) of recurrence of a cardiovascular event, and in particular, relapses despite treatment with an HMG-CoA reductase inhibitor in a hyperlipidemic patient. Or a composition for preventing recurrence of cardiovascular events containing EPA-E as an active ingredient, which is expected to be effective in preventing recurrence of cardiovascular events that occur after the instability period after performing cardiovascular reconstruction. .
- Patent Document 2 discloses that stroke is useful for prevention (secondary prevention) of stroke recurrence, and particularly, a stroke that recurs despite treatment with an HMG-CoA reductase inhibitor in a hyperlipidemic patient, or particularly A composition for preventing the recurrence of stroke containing EPA-E as an active ingredient, which is expected to have an effect of preventing the recurrence of stroke in patients 6 months after the onset of stroke, is described.
- Non-patent document 2 discloses that patients with hypercholesterolemia who received EPA-E and a statin drug were treated with a statin drug alone in the initial prevention (primary prevention) evaluation of coronary artery disease for about 5 years. It is described that the risk was reduced by 18% although it was not significant.
- Non-Patent Document 3 describes the ratio of plasma total lipid EPA concentration to arachidonic acid (hereinafter sometimes referred to as “AA”) concentration (hereinafter referred to as “EPA / AA ratio”) from the results of epidemiological studies. Is expected to be a new biomarker that predicts the risk of death from cardiovascular disease, and Non-Patent Document 4 shows that high-sensitivity C-reactivity in serum is based on the results of epidemiological studies.
- the protein (hereinafter sometimes referred to as “hs-CRP”) value is described as expected to be a new biomarker for predicting the risk of developing cardiovascular disease. Whether it was possible to accurately assess the risk of developing the disease (hereinafter sometimes referred to as “primary risk”) was not clear.
- An object of the present invention is to provide a primary preventive agent for cardiovascular disease, a marker for evaluating the primary risk of cardiovascular disease, a method for extracting a subject having a high cardiovascular disease risk, and / or a primary preventive method for cardiovascular disease. .
- the inventors of the present invention conducted intensive studies to achieve the above object.
- an epidemiological study examining the relationship between the serum EPA / AA ratio and the primary risk of cardiovascular disease in a population without a history of cardiovascular disease
- serum EPA / AA ratio There is no association between serum EPA / AA ratio and primary risk of cardiovascular disease in groups with hs-CRP values less than 1.0 mg / L, but serum EPA / AA in groups with 1.0 mg / L or more
- the primary risk of cardiovascular disease was significantly increased when the serum EPA / AA ratio was less than 0.50 in the group of 0 mg / L or more.
- the present inventors can reduce the risk of developing cardiovascular disease by administering EPA-E in subjects with no history of cardiovascular disease and serum hs-CRP value of 1.0 mg / L or more. It was found that the above effects were observed regardless of whether or not a statin drug was administered. That is, regardless of whether or not the patient is dyslipidemic, for example, whether or not blood LDL cholesterol is the value to be treated, a subject with a serum hs-CRP value of 1.0 mg / L or more is treated with EPA-E. It was learned that the risk of new onset of cardiovascular disease can be reduced. The present invention is based on these knowledges, and is described in more detail below.
- hs-CRP value in serum or plasma (hereinafter sometimes referred to as “blood hs-CRP value” or “hs-CRP value”) with no history of cardiovascular disease is 1.0 mg / L
- a primary preventive agent for cardiovascular disease comprising at least one selected from the group consisting of EPA, a salt thereof and an ester as an active ingredient for administration to the above subjects to reduce the risk of cardiovascular disease.
- the EPA / AA ratio hereinafter sometimes referred to as “serum EPA / AA ratio” or “EPA / AA ratio” in the total lipid in the serum or plasma of the subject is less than 0.50,
- the primary preventive agent for cardiovascular disease according to (2) above wherein the serum EPA / AA ratio is less than 0.25.
- the primary preventive agent for cardiovascular disease according to any one of (1) to (3) above which is effective when administered regardless of the presence or absence of dyslipidemia in the subject.
- the primary preventive agent for cardiovascular disease according to (4) above wherein the dyslipidemia is high LDL cholesterolemia.
- the primary preventive agent for cardiovascular disease according to any one of the above (1) to (6), wherein at least one selected from the group consisting of the EPA, a salt thereof and an ester is EPA-E.
- EPA-E at least one selected from the group consisting of docosahexaenoic acid (hereinafter sometimes referred to as “DHA”), salts and esters thereof
- DHA docosahexaenoic acid
- the at least one selected from the group consisting of the DHA, a salt thereof, and an ester is docosahexaenoic acid ethyl ester (hereinafter sometimes referred to as “DHA-E”), as described in (8) above Primary preventive agent for cardiovascular disease.
- DHA-E docosahexaenoic acid ethyl ester
- the primary preventive agent for cardiovascular disease according to any one of (1) to (9) above, wherein the cardiovascular disease is coronary artery disease or stroke.
- the primary preventive agent for cardiovascular disease according to (10) above, wherein the stroke is cerebral infarction or cerebral hemorrhage.
- a combination marker for evaluating the primary risk of cardiovascular disease in a subject who has no history of cardiovascular disease including blood hs-CRP value and serum EPA / AA ratio.
- hs-CRP value is 1.0 mg / L or more, and EPA / AA ratio is less than 0.25, cardiovascular disease high risk, and hs-CRP value is 1.0 mg / L or more, and EPA / AA
- the combined marker according to any one of (13) to (15), wherein the cardiovascular disease is coronary artery disease or stroke.
- the combined marker according to (16), wherein the coronary artery disease is myocardial infarction or angina.
- the subject is extracted as a high-risk subject with cardiovascular disease, as described in (19) or (20) above A method of extracting subjects with a high risk of cardiovascular disease. (23) The method according to any one of (19) to (21) above, wherein the subject has no history of cardiovascular disease.
- test kit comprising at least means for measuring a blood hs-CRP value for use in the method according to any one of (19) to (23).
- a primary cardiovascular disease prevention method comprising the step of administering the primary cardiovascular disease prevention agent according to any of (1) to (12) above to a subject extracted by the method according to (23) above .
- a marker for evaluating primary risk of cardiovascular disease a method for extracting a subject having a high risk of cardiovascular disease, a subject having no history of cardiovascular disease and having a blood hs-CRP value of 1.0 mg / L or more
- the primary preventive agent for cardiovascular disease and / or primary cardiovascular disease containing at least one selected from the group consisting of EPA, its salts and esters as an active ingredient for reducing the risk of cardiovascular disease Prophylactic methods are provided.
- the primary preventive agent for cardiovascular disease of the present invention can be administered to both subjects who have been administered statins and subjects who have not received statins, and has no history of cardiovascular disease. Can reduce the risk of cardiovascular disease in subjects with a dose of 1.0 mg / L or more.
- the primary preventive agent for cardiovascular disease of the present invention can be administered to both dyslipidemic (hyperlipidemic) patients and subjects who have never been diagnosed with dyslipidemic (hyperlipidemic).
- the marker for evaluating cardiovascular disease risk of the present invention can accurately and objectively evaluate cardiovascular disease risk using the blood hs-CRP value and serum EPA / AA ratio.
- cardiovascular disease primary risk assessment marker of the present invention subjects with a high primary risk of cardiovascular disease to whom the primary preventive agent for cardiovascular disease of the present invention should be administered can be extracted.
- cardiovascular disease primary prevention method of the present invention regardless of the presence or absence of dyslipidemia (hyperlipidemia) and the presence or absence of administration of statin drugs regardless of the type and degree of dyslipidemia Therefore, it is possible to perform primary prevention of cardiovascular disease in a subject who has no history of cardiovascular disease and has a high primary risk of cardiovascular disease having a blood hs-CRP value of 1.0 mg / L or more.
- the primary method for preventing cardiovascular disease according to the present invention is to detect a subject at a high risk of cardiovascular disease at an early stage, by administering a statin drug and exhibiting a certain therapeutic effect in dyslipidemia. This is an effective method for reducing the risk of vascular disease.
- FIG. 1A is a graph showing the relationship between the serum EPA / AA ratio and the hazard ratio of a group having a blood hs-CRP value of less than 1.0 mg / L (low hs-CRP group).
- FIG. 1 (B) is a graph showing the relationship between the serum EPA / AA ratio and the hazard ratio of a group having a blood hs-CRP value of 1.0 mg / L or more (high hs-CRP group).
- FIG. 2 shows the presence / absence of statin drug administration and EPA administration, and cardiovascular, coronary artery, and stroke for blood hs-CRP values of 1.0 mg / L or more (high hs-CRP group). It is a graph showing the relationship with disease incidence (%).
- the primary preventive agent for cardiovascular disease of the present invention is administered to a subject who has no history of cardiovascular disease and has a blood hs-CRP value of 1.0 mg / L or more, and reduces the risk of cardiovascular disease, It is a primary preventive agent for cardiovascular disease containing as an active ingredient at least one selected from the group consisting of salts and esters thereof.
- the cardiovascular disease includes coronary artery disease, stroke (cerebrovascular disorder) and peripheral vascular disease, preferably includes coronary artery disease and stroke, and more preferably includes coronary artery disease.
- Coronary artery disease specifically includes, for example, myocardial infarction and angina.
- a stroke specifically includes, for example, cerebral infarction and cerebral hemorrhage.
- the absence of a history of cardiovascular disease means that coronary artery disease, stroke (cerebrovascular disorder) and peripheral vascular disease have not developed; specifically, for example, myocardial infarction, angina pectoris
- the patient has not received a definitive diagnosis of coronary artery disease such as cerebral vascular disease such as cerebral infarction or cerebral hemorrhage.
- cerebral vascular disease such as cerebral infarction or cerebral hemorrhage.
- a cardiovascular event occurs in a site different from the cardiovascular responsible site at the time of the onset of a previous cardiovascular disease, it can be classified as the first occurrence of cardiovascular disease. It can also be a cardiovascular event onset in a patient with no history.
- the primary preventive agent of the present invention has no history of cardiovascular disease, blood hs-CRP value is 1.0 mg / L or more, 1.5 mg / L or more, or 2.0 mg / L or more Administered to the subject.
- the primary preventive agent of the present invention can be administered regardless of the presence or absence of other diseases or the presence or absence of administration of other drugs as long as it is a subject satisfying the above requirements, and is effective.
- a method for measuring blood hs-CRP is a C-reactive protein (CRP) 0.1 mg / L or more, preferably 0.05 mg / L or more, more preferably 0.01 mg / L. If it is, it will not specifically limit.
- CRP C-reactive protein
- Examples of such high-sensitivity CRP measurement methods include ELISA, latex nepherometry, laser nepherometry, and improved latex immunoturbidimetry.
- ELISA methods include Banaristo ace hsCRP (Sanwa Chemical Laboratory, Nagoya, Japan), ELISA Kit High Sensitive C-Reactive Protein (Immuno-Biological Laboratories, Inc., USA), ) And hsCRP Human ELISA (BioVendor, Heidelberg, Germany), N-latex CRP II (Siemens Healthcare Diagnostics, Tokyo, Japan) as a latex nepherometry method, modified latex immunoturbidicity Laws include cities such as Vitros Microchip hsCRP (Ortho-Clinical Diagnostics, Tokyo, Japan) It is possible to use the measurement kit.
- the serum EPA / AA ratio is the ratio of EPA and AA in serum total lipid (unit: ⁇ g / mL), but the ratio of EPA and AA in plasma total lipid (unit: ⁇ g / mL) is also It is described in the meaning including. It can also be described as the molar concentration (unit: mol / mL) ratio of EPA and AA in serum total lipid or plasma total lipid.
- the serum EPA / AA ratio of the administration subject is not particularly limited, but is preferably less than 0.50, more preferably less than 0.40, still more preferably less than 0.25, still more preferably less than 0.20, Even less than 10 is even more preferred.
- the method for measuring EPA and AA is not particularly limited, but serum or plasma is hydrolyzed, and EPA and AA in total lipids are gas chromatograph (GC) method, gas chromatograph-mass spectrum (GC-MS) method, GC ⁇ Examples include the GC-MS method.
- dyslipidemia hyperlipidemia
- hypertension diabetes, chronic kidney disease, non-cardiogenic cerebral infarction and peripheral artery disease.
- the above dyslipidemias are hypercholesterolemia, high LDL cholesterolemia, low-density lipoprotein (HDL) cholesterolemia, low non-HDL cholesterolemia, high apolipoprotein Bemia, high lipoprotein-related phospholipase A 2.
- HDL low-density lipoprotein
- apolipoprotein Bemia high lipoprotein-related phospholipase A 2.
- hypertension and hypertriglyceridemia Including hypertension and hypertriglyceridemia.
- the therapeutic agent for dyslipidemia includes cholesterol synthesis inhibitors (HMG-CoA reductase inhibitors (statins)), cholesterol catabolism promoters (probucol, etc.), cholesterol absorption inhibitors (cholestyramine, etc. (anion exchange resin)) ), Triglyceride (TG) synthesis inhibitors (fibrate drugs), small intestinal cholesterol transporter inhibitors (eg ezetimibe) and the like.
- the agent for primary prevention of cardiovascular disease of the present invention contains at least one selected from the group consisting of EPA, salts thereof and esters as an active ingredient.
- the active ingredient selected from the group consisting of EPA, its salts and esters is contained in an amount of 40% by mass or more based on the total amount of fatty acids (including salts and esters) contained in the primary preventive agent for cardiovascular disease of the present invention. It is preferable that 60% by mass or more is contained, more preferably 80% by mass or more is contained, still more preferably 90% by mass or more is contained, and still more preferably 95% by mass or more is contained. It is more preferable that the content is 96.5% by mass or more, 97% by mass or more, 98% by mass or more, that is, the content is high.
- the EPA may be all-cis-5,8,11,14,17-icosapentanoic acid (all-cis-5,8,11,14,17-icosapentaenoic acid) or (5Z, 8Z, 11Z, 14Z, 17Z). ) -Icosa-5,8,11,14,17-pentaenoic acid.
- the EPA salt is not particularly limited, but a sodium salt (hereinafter sometimes referred to as “EPA-Na”) is preferable.
- the ester of EPA is not particularly limited, but glyceride ester or ethyl ester is preferable, and ethyl ester is more preferable.
- EPA-E is more preferable among EPA, its salts and esters.
- EPA-E is more preferable as at least one selected from the group consisting of the EPA, its salt and ester.
- the primary preventive agent for cardiovascular disease of the present invention further contains a long-chain unsaturated fatty acid other than the above active ingredients, particularly an ⁇ -3 long-chain unsaturated fatty acid, preferably an ⁇ -3 long-chain polyunsaturated fatty acid. Also good.
- Examples of the ⁇ -3 long-chain polyunsaturated fatty acid include at least one selected from the group consisting of DHA, salts and esters thereof, and fatty acids (salts and esters) contained in the primary preventive agent for cardiovascular disease of the present invention.
- 60% by mass or less more preferably 40% by mass or less, further preferably 20% by mass or less, and more preferably 10% by mass or less. More preferably, still more preferably 5% by mass or less, 3.5% by mass or less, 3% by mass or less, 2% by mass or less, 0 It is more preferable that the content is 3% by mass or less, that is, the content is low.
- the total amount of ⁇ -3 long-chain polyunsaturated fatty acids (including salts and esters) including at least one selected from the group consisting of EPA, salts thereof and esters is the primary preventive agent for cardiovascular disease of the present invention
- the DHA is all-cis-4,7,10,13,16,19-docosahexaenoic acid (all-cis-4,7,10,13,16,19-docosahexaenoic acid) or (4Z, 7Z, 10Z , 13Z, 16Z, 19Z) -docosa-4,7,10,13,16,19-hexaenoic acid.
- the salt of DHA is not particularly limited, but a sodium salt (hereinafter sometimes referred to as “DHA-Na”) is preferable.
- the ester of DHA is not particularly limited, but glyceride ester or ethyl ester is preferable, and ethyl ester is more preferable.
- DHA-E DHA-E is more preferred.
- DHA-E is more preferable as at least one selected from the group consisting of the above DHA, its salt and ester.
- the content of ⁇ -6 long-chain unsaturated fatty acid, particularly AA, is preferably 5% by mass or less based on the total amount of fatty acids (including salts and esters) contained in the primary preventive agent for cardiovascular disease of the present invention, 2 mass% or less is more preferable, 1 mass% or less is further more preferable, and it is still more preferable not to contain substantially.
- the agent for primary prevention of cardiovascular disease of the present invention may contain a pharmaceutically acceptable excipient in addition to the above components. Since EPA and DHA are both highly unsaturated, they contain an effective amount of antioxidants such as butylated hydroxytoluene, butylated hydroxyanisole, propyl gallate, gallic acid, pharmaceutically acceptable quinone and ⁇ -tocopherol be able to.
- the dosage form is orally administered to subjects in the form of tablets, capsules, microcapsules, granules, fine granules, acids, oral liquid preparations, self-emulsifying preparations, emulsions, syrups, and jelly preparations.
- oral administration in capsules such as soft capsules and microcapsules is preferred.
- Epadale (R) and Epadale (R) S which are high-purity EPA-E-containing soft capsules, are already marketed in Japan as safe occlusive arteriosclerosis and hyperlipidemia treatments with few side effects.
- the content of EPA-E in all fatty acids is 96.5% by mass or more.
- Bashipa (R) (Vascepa (R) ( Amarin Pharma) are already commercially available in the US as a high TG hyperlipidemia therapeutic agent.
- the total fatty acids in the EPA-E about 46% by weight and DHA-E of about 38 wt% content for soft capsules (Robaza (R), Lovaza (R) (GlaxoSmithKline), Omakoru (R), Omacor (R) (Pronova) and Rotriga (R) , Lotoriga (R) (Takeda Pharmaceutical Co., Ltd.) have already been marketed in the United States, Europe, Japan, etc. as therapeutic agents for hyperTGemia.
- EPA-E and DHA-E are commercially available products that can also be obtained and used as the primary preventive agent for cardiovascular disease of the present invention.
- the product containing EPA-E and DHA-E for example, Lovaza (R) , Omacol (R) or Rotriga (R) is preferable, and EPA-E content in all fatty acids is 96.5% by mass or more.
- High-purity EPA-E-containing agents such as (R) and Basiepa (R) are more preferred because they do not substantially contain AA.
- the dosage and administration period of the primary preventive agent for cardiovascular disease of the present invention are an amount and a period sufficient to represent the primary preventive effect of cardiovascular disease, but its dosage form, administration method, number of administrations per day It can be increased or decreased as appropriate according to body weight, age and the like.
- the primary preventive agent for cardiovascular disease of the present invention is preferably reduced by 0.25 mg / L or more so that the blood hs-CRP value is reduced by 0.1 mg / L or more compared to the value at the start of treatment or the previous measurement. More preferably, it is more preferably 0.5 mg / L or less, even more preferably 0.75 mg / L or more, still more preferably 1.0 mg / L or more. Maintain below 1.5 mg / L, or maintain below 2.0 mg / L, preferably below 1.5 mg / L, more preferably below 1.25 mg / L More preferably less than 1.0 mg / L, even more preferably less than 0.75 mg / L, even more preferably less than 0.5 mg / L.
- the serum EPA / AA ratio is increased by 0.1 or more, preferably 0.20 or more, more preferably 0.25 or more, compared to the value of the start of treatment or the previous measurement.
- To rise more preferably to rise above 0.40, more preferably above 0.50, even more preferably above 0.60, or to maintain above 0.50
- preferably maintain at 0.60 or more more preferably maintain at 0.70 or more, more preferably maintain at 0.75 or more, still more preferably maintain at 0.80 or more.
- 0.1 to 10 g / day preferably 0.3 to 6 g / day, more preferably 0.9 to 3.6 g / day, and further preferably 1.8 to 2.7 g as EPA-E. / Day is divided into 3 doses, but the total amount may be divided into 1 or several doses as needed.
- the total amount of ⁇ -3 long-chain polyunsaturated fatty acids is 0.1 to 10 g / day, preferably 0.3 to 9 g / day, more preferably 1 to Although 6 g / day, more preferably 2 to 4 g / day, is administered in three divided doses, the total amount may be administered once or in several divided doses as necessary.
- a single dose and the number of daily administration for example, 0.3 g once, 0.3 g twice, 0.3 g 3-10 times, 0.6 g once, 0.6 g 2 times, 0.6g 3-10 times, 0.9g once, 0.9g twice, 0.9g 3-10 times, 1g once, 1g twice, 1g 3-10 times 1.2g once, 1.2g twice, 1.2g 3-8 times, 1.8g once, 1.8g twice, 1.8g 3-5 times 2g 1 time, 2 g 2 times, 2 g 3-5 times, 2.4 g 1 time, 2.4 g 2 times, 2.4 g 3-4 times, 2.7 g 1 time, 2.7 g 2 times 2.7g 3 times 3g 1 time 3g 2 times 3g 3 times 3.6g 1 time 3.6g 2 times 4g 1 time 4g 2 times 5g once, 4.5g twice, 5g once, 5g twice, 6g once, 7g 1 1 time, 8 g once, 9 g once, 10 g once, or a combination of these single
- the administration time is preferably during or after meals, more preferably immediately after meals (within 30 minutes). Since the self-emulsifying type preparation is excellent in absorbability, it can be administered at any time without any restriction on the administration time. For example, it can be administered before meals, between meals or before going to bed.
- the administration period is 1 year or longer, preferably 2 years or longer, more preferably 3.5 years or longer, and even more preferably 5 years or longer. Onset and / or recurrence of cardiovascular events It is desirable to continue administration as long as the risk level is high. In some cases, a drug holiday of about 1 day to 3 months, preferably about 1 week to 1 month can be provided.
- the combined marker for evaluating the risk of cardiovascular disease in a subject who has no history of cardiovascular disease of the present invention includes both the blood hs-CRP value and the serum EPA / AA ratio.
- the blood high-sensitivity C-reactive protein value is also called blood high-sensitivity CRP value or blood hs-CRP value, and represents the concentration (unit: mg / L) of C-reactive protein in blood (serum or plasma). .
- the hs-CRP value and the normal C-reactive protein value both represent the blood concentration of the same protein (C-reactive protein), but the hs-CRP value is higher than that of the C-reactive protein.
- Reactive protein is quantified.
- the measurement limit of the usual C-reactive protein measurement method is about 1 mg / L, whereas the measurement limit of the hs-CRP measurement method is 0.1 mg / L, preferably 0.01 mg / L.
- As a measuring method there are an ELISA method, an LA / nepherometry method and the like.
- Serum EPA / AA ratio is the mass ratio of EPA to AA in serum total lipid.
- a quantification method serum or plasma is hydrolyzed, each of EPA and AA in total lipid is quantified, and the mass of EPA is divided by the mass of AA.
- Examples of EPA and AA quantitative methods include gas chromatograph (GC) method, gas chromatograph / mass spectrum (GC / MS) method, FTIR method (AOAC method) and the like.
- a blood hs-CRP value of 1.0 mg / L or more and a serum EPA / AA ratio of less than 0.50 are evaluated as high risk of cardiovascular disease.
- the blood hs-CRP value is 1.0 mg / L or more, and the serum EPA / AA ratio is less than 0.25, the cardiovascular disease has an extremely high risk
- the blood hs-CRP value is 1.0 mg / L or more
- a serum EPA / AA ratio of 0.25 or more and less than 0.50 may be evaluated as a high risk of cardiovascular disease.
- a blood hs-CRP value of 1.0 mg / L or more and a serum EPA / AA ratio of 0.50 or more may be evaluated as a medium risk.
- the threshold value of the serum EPA / AA ratio less than 0.50 can be set to any numerical value between less than 0.26 and less than 0.74, for example, less than 0.70, less than 0.60,.
- the risk can be evaluated as less than 40 or less than 0.30. Further, the risk can be evaluated by setting the serum EPA / AA ratio less than 0.25 as, for example, less than 0.20 or less than 0.10.
- the blood hs-CRP value is 1.0 mg / L or more and the serum EPA / AA ratio is 0.10 or more lower than the previous measured value, preferably 0.20 or more, more preferably Even if it is reduced by 0.25 or more, more preferably 0.30 or more, still more preferably 0.40 or more, even more preferably 0.50 or more is evaluated as an increase in risk. Good.
- the blood hs-CRP value is less than 1.0 mg / L, the serum EPA / AA ratio is not related to the risk of cardiovascular disease.
- the blood hs-CRP value of 1.0 mg / L or more in the risk evaluation standard can be changed to 1.5 mg / L or more or 2.0 mg / L or more for evaluation.
- An example of the combination marker of the present invention is a medium in which a subject and / or a doctor can simultaneously recognize both the blood hs-CRP value and the serum EPA / AA ratio of the subject. More specifically, the medium on which both the blood hs-CRP value and the serum EPA / AA ratio are described or recorded is preferably described or recorded with both measurement results and a combination thereof. Medium. Specifically, examples of the medium include a paper medium and an electronic recording medium.
- EPA blood C-reactive protein level
- serum EPA / AA ratio has not been clarified.
- EPA is said to have effects such as improvement of vascular endothelial dysfunction, suppression of platelet aggregation, and plaque stabilization by anti-inflammatory action.
- AA is said to produce a physiologically active substance having a strong platelet aggregation ability and a strong inflammation-inducing substance.
- an increase in blood C-reactive protein level is a risk factor for cardiovascular disease, and therefore a group with a high blood C-reactive protein level (high hs-CRP group; blood CRP level ⁇ 1. 0 mg / L), it is considered that there was a significant correlation between the serum EPA / AA ratio and the risk of cardiovascular disease.
- the first aspect of the method for extracting subjects with high cardiovascular disease risk of the present invention comprises: Measuring the blood hs-CRP level of the subject; Measuring a subject's serum EPA / AA ratio; And combining the blood hs-CRP value and the serum EPA / AA ratio to extract the subject as a high-risk subject with cardiovascular disease.
- the second aspect of the method for extracting a subject having a high risk of cardiovascular disease of the present invention comprises: Measuring a subject's blood hs-CRP level and measuring a serum EPA / AA ratio;
- the method includes a step of extracting the subject as a high-risk subject of cardiovascular disease by combining the blood hs-CRP value and the serum EPA / AA ratio.
- the blood hs-CRP value is 1.0 mg / L or more and the serum EPA / AA ratio is less than a certain value, for example, less than 0.50 or 0 And when it is less than 25, the subject is extracted as a high-risk subject with cardiovascular disease or a high-risk subject with cardiovascular disease.
- the threshold value of the serum EPA / AA ratio less than 0.50 can be set to any numerical value between less than 0.26 and less than 0.74, for example, less than 0.70, less than 0.60,.
- a step of extracting a vascular disease risk subject as less than 40 or less than 0.30.
- the extraction can be performed by changing the blood hs-CRP value of 1.0 mg / L or more in the above extraction method to 1.5 mg / L or more or 2.0 mg / L or more.
- the test kit of the present invention is a test kit including at least a means for measuring a blood hs-CRP value for use in the method for extracting a subject having a high risk of cardiovascular disease.
- a means for measuring a blood hs-CRP value for use in the method for extracting a subject having a high risk of cardiovascular disease.
- the means for measuring the hs-CRP value as already described, for obtaining the hs-CRP value by ELISA method, latex nepherometry method, laser nepherometry method, improved latex immunoturbidimetric method, etc. It is preferable to include reagents used in these methods.
- the blood hs-CRP value is decreased by 0.1 mg / L or more compared with the value at the start of treatment or the previous measurement, preferably 0 0.25 mg / L or more, more preferably 0.5 mg / L or more, more preferably 0.75 mg / L or more, more preferably 1.0 mg / L or more, even more Preferably it is reduced by 1.5 mg / L or more, or maintained at less than 2.0 mg / L, preferably maintained at less than 1.5 mg / L, more preferably maintained at less than 1.25 mg / L.
- HMG-CoA reductase inhibitors and other dyslipidemia, hypertension, diabetes, chronic kidney disease, non-cardiogenic cerebral infarction and peripheral arteries
- an HMG-CoA reductase inhibitor, other dyslipidemia treatment agent, hypertension treatment agent, diabetes mellitus The effects of a therapeutic agent, a chronic kidney disease therapeutic agent, a non-cardiogenic cerebral infarction therapeutic agent, a peripheral arterial disease therapeutic agent, and the like can be obtained together.
- the method of the present invention is also effective for patients who are administered statin drugs and whose LDL cholesterol is controlled to a certain value (for example, less than 120 mg / dL, less than 100 mg / dL, or less than 80 mg / dL). It is.
- a certain value for example, less than 120 mg / dL, less than 100 mg / dL, or less than 80 mg / dL.
- a subject who has a high risk of cardiovascular disease is extracted by the method described above, and then the primary of the present invention.
- Prophylactic agents can be used to reduce the risk of new onset of cardiovascular disease.
- Hisayama Town Research is an epidemiological survey of stroke, cardiovascular disease, etc., which has been conducted since 1961 for residents of Hisayama Town (population: about 8,400) adjacent to Fukuoka City, Fukuoka Prefecture. Hisayama residents have the same age and occupation distribution as the national average, and are considered to be an average Japanese group with little bias.
- the features of the Hisayama study include all residents (over 40 years old), prospective follow-up study (cohort study), screening / visiting by research staff, consultation rate (over 80%), autopsy rate (about 80%), follow-up The rate (99% or more) is mentioned.
- the biggest feature is the high autopsy rate.
- There is no more accurate diagnostic method than autopsy in terms of knowing the exact cause of death.
- the accuracy of the follow-up survey is considered high.
- since the study of Hisayama has newly added residents over the age of 40 to the group every five years, it is possible to know the effects of changes in lifestyle and the changes in risk factors.
- Subjects and follow-up period 3,103 residents aged 40 years or older who were registered in 2002 were subjects. Those with a history of cardiovascular disease and those without an EPA / AA ratio were excluded. The average follow-up period was 5.1 years. Of the 3,103 subjects, 191 were all dead. Among them, the causes of death are 48 cases of cardiovascular disease (International Statistical Classification of Diseases and Related Health Problems 10th edition (ICD10): I00-I99), 70 cases of cancer (ICD10: C00-D48), and infectious diseases (ICD10: A00-B99, J00-J39, J69, N13.6) 39 cases and other causes 34 cases. There were 127 cases of cardiovascular disease (survival and death), 49 of which were coronary artery cases and 83 of stroke cases.
- ICD10 International Statistical Classification of Diseases and Related Health Problems 10th edition
- Serum EPA / AA ratio The serum EPA / AA ratio of a subject is obtained by collecting blood of a subject, hydrolyzing serum or plasma, and quantifying EPA and AA in total lipid by gas chromatography. Was measured (unit: ⁇ g / mL), and the concentration ratio of EPA to AA was calculated.
- hs-CRP value The blood hs-CRP value of a subject is obtained by collecting the subject's blood, processing the sample with a commercially available latex reagent for high-sensitivity CRP measurement, and measuring it using a biochemical automatic analyzer. (Unit: mg / L).
- a subject with a serum EPA / AA ratio of less than 0.25 has a total mortality risk and a cardiovascular death risk of 2.04 times and 3 respectively, compared with a subject with a serum EPA / AA ratio of 0.75 or more. .06 times.
- the hazard ratio was calculated using the Cox proportional hazard model with the whole as the standard (1.00).
- Potential confounders such as age, gender, hypertension, diabetes, serum total cholesterol, use of dyslipidemia, BMI (body mass index), smoking habits and alcohol consumption were adjusted.
- BMI body mass index
- FIG. 1 shows (A) a bar graph representing the hazard ratio of the low hs-CRP group and (B) a bar graph representing the hazard ratio of the high hs-CRP group.
- the hazard ratio significantly increased as the serum EPA / AA ratio decreased, and the serum EPA / AA ratio was 0.75 or more.
- the group of 0.25 to 0.49 was 2.32 times larger, and the group of less than 0.25 was 3.39 times larger.
- a group having a blood hs-CRP value of 1.0 mg / L or more and a serum EPA / AA ratio of less than 0.50 is appropriate to evaluate a group having a blood hs-CRP value of 1.0 mg / L or more and a serum EPA / AA ratio of less than 0.50 as a high-risk group for cardiovascular disease. I found out that Furthermore, a group having a blood hs-CRP value of 1.0 mg / L or more and a serum EPA / AA ratio of less than 0.25 is more significant than a group having a serum EPA / AA ratio of 0.25 or more and less than 0.50.
- a group having a blood hs-CRP value of 1.0 mg / L or more and a serum EPA / AA ratio of less than 0.25 is an extremely high risk group for cardiovascular disease, and a blood hs-CRP value is 1 It was found that a group of 0.0 mg / L or more and 0.25 or more and less than 0.50 may be evaluated as a high risk group of cardiovascular disease.
- Cardiovascular disease The 5-year incidence rate is 3.5% in the group with a blood hs-CRP value of less than 1.0 mg / L, whereas it is 5.9 in the group with 1.0 mg / L or more. % And was rising.
- Coronary artery disease The 5-year incidence rate is 1.3% in the group with a blood hs-CRP value of less than 1.0 mg / L, whereas it is 2.4% in the group with 1.0 mg / L or more. It was rising.
- statin ( ⁇ ) + EPA ( ⁇ ) indicates that neither the statin drug nor EPA is administered to the subject
- statin (+) + EPA ( ⁇ ) indicates that the statin drug is administered
- tatin (-) + EPA (+) indicates that no statin drug is administered and EPA is administered
- tatin (+ ) + EPA (+) indicates that both a statin drug and EPA are administered.
- the event ( ⁇ ) and the event (+) indicate that the event has not occurred and has occurred, respectively.
- Table 4 shows the number and number of occurrences of cardiovascular disease, coronary artery disease and stroke events, and the number of subjects in each group for the high hs-CRP group.
- FIG. 2 shows the cardiovascular disease incidence (%), coronary artery disease incidence (%), and stroke incidence (%) for each group.
- Cardiovascular disease As for cardiovascular disease, no event occurred in the group administered with EPA in the high hs-CRP group irrespective of the presence or absence of administration of statin drugs. Moreover, in the group not administered EPA, the incidence of events was higher in the group administered the statin drug than in the group not administered, but this is the group administered the statin drug Because of having dyslipidemia (hyperlipidemia and / or hypercholesterolemia), or because the degree of dyslipidemia is higher than the non-administered group, It is thought that it has become. That is, regarding the cardiovascular disease, it is considered that no event occurred in the group administered with EPA regardless of the presence or absence of dyslipidemia or the degree of dyslipidemia in the high hs-CRP group. Therefore, the primary preventive agent for cardiovascular disease of the present invention is effective for the primary prevention of cardiovascular disease regardless of the presence or absence of administration of statin drugs, regardless of the presence or absence of dyslipidemia or the degree of dyslipidemia. .
- Coronary artery disease As for coronary artery disease, no event occurred in the group administered with EPA in the high hs-CRP group regardless of whether or not the statin drug was administered. Moreover, in the group not administered EPA, the incidence of events was higher in the group administered the statin drug than in the group not administered, but this is the group administered the statin drug Because of having dyslipidemia (hyperlipidemia and / or hypercholesterolemia), or because the degree of dyslipidemia is higher than the non-administered group, It is thought that it has become. That is, it is considered that no coronary artery disease occurred in the group administered with EPA regardless of the presence or absence of dyslipidemia or the degree of dyslipidemia in the high hs-CRP group. Therefore, the primary preventive agent for cardiovascular disease of the present invention is effective for primary prevention of coronary artery disease regardless of the presence or absence of administration of statin drugs, regardless of the presence or absence of dyslipidemia or the degree of dyslipidemia.
- the primary preventive agent for cardiovascular disease of the present invention is effective for primary prevention of stroke regardless of the presence or absence of administration of statin drugs, regardless of the presence or absence of dyslipidemia or the degree of dyslipidemia.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Engineering & Computer Science (AREA)
- General Health & Medical Sciences (AREA)
- Medicinal Chemistry (AREA)
- Molecular Biology (AREA)
- Urology & Nephrology (AREA)
- Hematology (AREA)
- Immunology (AREA)
- Biomedical Technology (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Pharmacology & Pharmacy (AREA)
- Animal Behavior & Ethology (AREA)
- Epidemiology (AREA)
- Biotechnology (AREA)
- Physics & Mathematics (AREA)
- Cell Biology (AREA)
- Pathology (AREA)
- General Physics & Mathematics (AREA)
- Food Science & Technology (AREA)
- Biochemistry (AREA)
- Microbiology (AREA)
- Analytical Chemistry (AREA)
- Emergency Medicine (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Endocrinology (AREA)
- Biophysics (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Organic Chemistry (AREA)
- General Chemical & Material Sciences (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Cardiology (AREA)
- Heart & Thoracic Surgery (AREA)
- Diabetes (AREA)
- Vascular Medicine (AREA)
- Acyclic And Carbocyclic Compounds In Medicinal Compositions (AREA)
Abstract
Description
(2)前記被験者の血清または血漿中の総脂質中のEPA/AA比(以下「血清EPA/AA比」あるいは「EPA/AA比」と記載する場合がある)が0.50未満である、上記(1)に記載の心血管疾患一次予防剤。
(3)前記血清EPA/AA比が0.25未満である、上記(2)に記載の心血管疾患一次予防剤。
(4)前記被験者の脂質異常症の有無によらず投与されて有効である、上記(1)~(3)のいずれかに記載の心血管疾患一次予防剤。
(5)前記脂質異常症が高LDLコレステロール血症である、上記(4)に記載の心血管疾患一次予防剤。
(6)前記被験者のHMG-CoA還元酵素阻害剤の投与の有無によらず投与されて有効である、上記(1)~(5)のいずれかに記載の心血管疾患一次予防剤。
(7)前記EPA、その塩およびエステルからなる群から選択される少なくとも1つが、EPA-Eである、上記(1)~(6)のいずれかに記載の心血管疾患一次予防剤。
(8)さらにドコサヘキサエン酸(以下「DHA」と記載する場合がある。)、その塩およびエステルからなる群から選択される少なくとも1つを含有する、上記(1)~(7)のいずれかに記載の心血管疾患一次予防剤。
(9)前記DHA、その塩およびエステルからなる群から選択される少なくとも1つが、ドコサヘキサエン酸エチルエステル(以下「DHA-E」と記載する場合がある。)である、上記(8)に記載の心血管疾患一次予防剤。
(10)前記心血管疾患が冠動脈疾患または脳卒中である、上記(1)~(9)のいずれかに記載の心血管疾患一次予防剤。
(11)前記冠動脈疾患が心筋梗塞または狭心症である、上記(10)に記載の心血管疾患一次予防剤。
(12)前記脳卒中が脳梗塞または脳出血である、上記(10)に記載の心血管疾患一次予防剤。
(14)hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.50未満を心血管疾患高リスクと評価する、上記(13)に記載の組合せマーカー。
(15)hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.25未満を心血管疾患特高リスク、およびhs-CRP値が1.0mg/L以上、かつEPA/AA比が0.25以上0.50未満を心血管疾患高リスクと評価する、上記(13)に記載の組合せマーカー。
(16)前記心血管疾患が冠動脈疾患または脳卒中である、上記(13)~(15)のいずれかに記載の組合せマーカー。
(17)前記冠動脈疾患が心筋梗塞または狭心症である、上記(16)に記載の組合せマーカー。
(18)前記脳卒中が脳梗塞または脳出血である、上記(16)に記載の組合せマーカー。
被験者の血清EPA/AA比を測定する工程と、
前記血中hs-CRP値と前記血清EPA/AA比とを組み合わせて、当該被験者を心血管疾患高リスク被験者として抽出する工程と
を備える、心血管疾患リスクが高い被験者を抽出する方法。
(20)被験者の血中hs-CRP値を測定する工程および血清EPA/AA比を測定する工程を有し、
前記血中hs-CRP値と前記血清EPA/AA比とを組み合わせて、当該被験者を心血管疾患高リスク被験者として抽出する工程
を備える、心血管疾患リスクが高い被験者を抽出する方法。
(21)前記工程において、hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.50未満である場合に、当該被験者を心血管疾患高リスク被験者として抽出する、上記(19)または(20)に記載の心血管疾患リスクが高い被験者を抽出する方法。
(22)前記工程において、hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.25未満である場合に、当該被験者を心血管疾患高リスク被験者、および
hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.25以上0.50未満である場合に、当該被験者を心血管疾患高リスク被験者として抽出する、上記(19)または(20)に記載の心血管疾患リスクが高い被験者を抽出する方法。
(23)前記被験者に心血管疾患の既往がない、上記(19)~(21)のいずれかに記載の方法。
[心血管疾患一次予防剤]
本発明の心血管疾患一次予防剤は、心血管疾患の既往がない、血中hs-CRP値が1.0mg/L以上の被験者に投与し、心血管疾患リスクを低下させるための、EPA、その塩およびエステルからなる群から選択される少なくとも1つを有効成分として含有する心血管疾患一次予防剤である。
本発明において、心血管疾患は、冠動脈疾患、脳卒中(脳血管障害)および末梢血管疾患を含み、好ましくは冠動脈疾患および脳卒中を含み、より好ましくは冠動脈疾患を含む。冠動脈疾患は、具体的には、例えば、心筋梗塞および狭心症を含む。脳卒中は、具体的には、例えば、脳梗塞および脳出血を含む。
また、本発明において、心血管疾患の既往がないとは、冠動脈疾患、脳卒中(脳血管障害)および末梢血管疾患を発症したことがないこと、具体的には、例えば、心筋梗塞、狭心症等の冠動脈疾患、および脳梗塞、脳出血等の脳血管疾患の確定診断を受けていないことをいう。また、既往の心血管疾患発症時の心血管責任部位と異なる部位において心血管イベントが発症した場合は、心血管疾患初発と分類することができ、広義にはこのような患者は心血管疾患の既往がない患者の心血管イベント発症とすることもできる。
本発明において、本発明の一次予防剤は、心血管疾患の既往がない、血中hs-CRP値が1.0mg/L以上の、1.5mg/L以上の、あるいは2.0mg/L以上の被験者に投与される。そして、本発明の一次予防剤は、上記要件を満たす被験者であれば、他の疾患の有無や、他の薬剤の投与の有無を問わず、投与することができ、しかも有効である。
血中hs-CRPの測定方法は、C反応性蛋白質(CRP) 0.1mg/L以上、好ましくは0.05mg/L以上、より好ましくは0.01mg/Lの感度を有する高感度CRP測定法であれば特に限定されない。このような高感度CRP測定法としては、ELISA法、ラテックス・ネフェロメトリー法、レーザー・ネフェロメトリー法、改良ラテックス免疫比濁法等が挙げられる。例えば、ELISA法としては、バナリストエースhsCRP(三和化学研究所、名古屋、日本)、ELISA Kit High Sensitivity C-Reactive Protein(イムノ-バイオロジカル ラボラトリーズ(Immuno-Biological Laboratories, Inc.)、ミネソタ、アメリカ)およびhsCRP Human ELISA(バイオベンダー(BioVendor)、ハイデルベルグ、ドイツ)、ラテックス・ネフェロメトリー法としては、N-ラテックス CRP II(シーメンスヘルスケア・ダイアグノスティクス、東京、日本)、改良ラテックス免疫比濁法としては、ビトロス マイクロチップ hsCRP(オーソ・クリニカル・ダイアグノスティクス、東京、日本)等の市販の測定キットを使用することができる。
血清EPA/AA比は、血清総脂質中のEPAとAAとの濃度(単位:μg/mL)比であるが、血漿総脂質中のEPAとAAとの濃度(単位:μg/mL)比も含む意味で記載される。また、血清総脂質中または血漿総脂質中のEPAとAAとのモル濃度(単位:mol/mL)比として記載することもできる。
上記投与対象被験者の血清EPA/AA比は、特に限定されないが、0.50未満が好ましく、0.40未満がより好ましく、0.25未満がさらに好ましく、0.20未満がなお好ましく、0.10未満がなおいっそう好ましい。
EPAおよびAAの測定方法は、特に限定されないが、血清または血漿を加水分解し、総脂質中のEPAおよびAAをガスクロマトグラフ(GC)法、ガスクロマトグラフ-マススペクトル(GC-MS)法、GC×GC-MS法等が挙げられる。
上記他の疾患としては、例えば、脂質異常症(高脂血症)、高血圧症、糖尿病、慢性腎臓病、非心原性脳梗塞および末梢動脈疾患等が含まれる。
上記脂質異常症は、高コレステロール血症、高LDLコレステロール血症、低高密度リポプロテイン(HDL)コレステロール血症、低非HDLコレステロール血症、高アポリポ蛋白質B血症、高リポ蛋白質関連ホスホリパーゼA2血症および高トリグリセリド血症を含む。
上記他の薬剤としては、例えば、脂質異常症治療剤が挙げられる。
上記脂質異常症治療剤は、コレステロール合成阻害剤(HMG-CoA還元酵素阻害剤(スタチン系薬剤))、コレステロール異化促進剤(プロブコール等)、コレステロール吸収阻害薬(コレスチラミン等(陰イオン交換樹脂))、トリグリセリド(TG)合成阻害剤(フィブラート系薬剤)、小腸コレステロールトランスポーター阻害剤(エゼチミブ等)等を含む。
本発明の心血管疾患一次予防剤は、有効成分として、EPA、その塩およびエステルからなる群から選択される少なくとも1つを含有する。EPA、その塩およびエステルからなる群から選択された有効成分は、本発明の心血管疾患一次予防剤が含有する脂肪酸(塩およびエステルを含む)の総量に対して、40質量%以上含有されることが好ましく、60質量%以上含有されることがより好ましく、80質量%以上含有されることがさらに好ましく、90質量%以上含有されることがなお好ましく、なおいっそう好ましくは、95質量%以上含有されること、96.5質量%以上含有されること、97質量%以上含有されること、98質量%以上含有されることであり、すなわち含有率が高いことがより好ましい。
本発明の心血管疾患一次予防剤は、さらに、上記有効成分以外の長鎖不飽和脂肪酸、特にω-3長鎖不飽和脂肪酸、好ましくはω-3長鎖多価不飽和脂肪酸を含有してもよい。
本発明の心血管疾患一次予防剤は、上記成分の他に、薬学的に許容され得る賦形剤を含有してもよい。EPAおよびDHAはいずれも高度に不飽和であるため、抗酸化剤、例えばブチレート化ヒドロキシトルエン、ブチレート化ヒドロキシアニソール、プロピルガレート、没食子酸、医薬として許容されうるキノンおよびα-トコフェロールを有効量含有させることができる。
剤形としては、錠剤、カプセル剤、マイクロカプセル剤、顆粒剤、細粒剤、酸剤、経口用液体製剤、自己乳化型製剤、乳剤、シロップ剤、ゼリー剤の形で、被験者に経口投与されるが、とりわけ、カプセル、例えば軟質カプセルやマイクロカプセルに封入しての経口投与が好ましい。
本発明の心血管疾患一次予防剤の投与量および投与期間は、心血管疾患の一次予防効果を表すのに十分な量および期間とされるが、その剤形、投与方法、1日当たりの投与回数、体重、年齢等によって適宜増減することができる。
本発明の心血管疾患の既往がない被験者の心血管疾患リスクを評価するための組合せマーカーは、血中hs-CRP値と、血清EPA/AA比との両方を含ものである。
血中高感度C反応性蛋白質値は、血中高感度CRP値または血中hs-CRP値ともいい、血中(血清中、血漿中)のC反応性蛋白質の濃度(単位:mg/L)を表す。
hs-CRP値および通常のC反応性蛋白質値は、どちらも同じ蛋白質(C反応性蛋白質)の血中濃度を表しているが、hs-CRP値の方が高感度の測定法を用いてC反応性蛋白質を定量している。通常のC反応性蛋白質の測定方法の測定限界が1mg/L程度であるのに対し、hs-CRPの測定方法の測定限界は0.1mg/L、好ましくは0.01mg/Lである。
測定方法としては、ELISA法、LA/ネフェロメトリー法等がある。
血清EPA/AA比は、血清総脂質中のEPAのAAに対する質量比である。
定量方法としては、血清または血漿を加水分解し、総脂質中のEPAおよびAAのそれぞれを定量し、EPAの質量をAAの質量で除して求める。
EPAおよびAAの定量方法としては、ガスクロマトグラフ(GC)法、ガスクロマトグラフ/マススペクトル(GC/MS)法、FTIR法(AOAC法)等が挙げられる。
血中hs-CRP値が1.0mg/L以上、かつ血清EPA/AA比が0.50未満を心血管疾患高リスクと評価する。
また、血中hs-CRP値が1.0mg/L以上、かつ血清EPA/AA比が0.25未満を心血管疾患特高リスク、血中hs-CRP値が1.0mg/L以上、かつ血清EPA/AA比が0.25以上0.50未満を心血管疾患高リスクと評価してもよい。
さらに、加えて、血中hs-CRP値が1.0mg/L以上、かつ血清EPA/AA比が0.50以上を中リスクと評価してもよい。
また、前記血清EPA/AA比の閾値0.50未満を0.26未満~0.74未満の間の任意の数値に設定することもでき、例えば0.70未満、0.60未満、0.40未満あるいは0.30未満としてリスク評価することができる。また、血清EPA/AA比の閾値0.25未満を、例えば0.20未満あるいは0.10未満としてリスク評価することもできる。
さらに、血中hs-CRP値が1.0mg/L以上、かつ血清EPA/AA比が前回の測定値に比べて0.10以上低下した場合、好ましくは0.20以上低下した場合、より好ましくは0.25以上低下した場合、さらに好ましくは0.30以上低下した場合、なお好ましくは0.40以上低下した場合、なおいっそう好ましくは0.50以上低下した場合をリスク上昇と評価してもよい。
ただし、血中hs-CRP値が1.0mg/L未満では、血清EPA/AA比と心血管疾患リスクとは関連しない。また、上記リスク評価基準の血中hs-CRP値1.0mg/L以上を、1.5mg/L以上あるいは2.0mg/L以上に変更して評価することもできる。
また、本発明により、血中C反応性蛋白質値上昇は心血管疾患のリスク因子であることから、血中C反応性蛋白質値が高い群(高hs-CRP群;血中CRP値≧1.0mg/L)で、血清EPA/AA比と心血管疾患リスクとの間に有意な相関がみられたと考えられる。
本発明の心血管疾患リスクが高い被験者を抽出する方法の第1態様は、
被験者の血中hs-CRP値を測定する工程と、
被験者の血清EPA/AA比を測定する工程と、
前記血中hs-CRP値と前記血清EPA/AA比とを組み合わせて、当該被験者を心血管疾患高リスク被験者として抽出する工程と
を備える方法である。
被験者の血中hs-CRP値を測定する工程および血清EPA/AA比を測定する工程を有し、
前記血中hs-CRP値と前記血清EPA/AA比とを組み合わせて、当該被験者を心血管疾患高リスク被験者として抽出する工程
を備える方法である。
また、前記血清EPA/AA比の閾値0.50未満を0.26未満~0.74未満の間の任意の数値に設定することもでき、例えば0.70未満、0.60未満、0.40未満あるいは0.30未満として血管疾患リスク被験者を抽出する工程とを備える方法である。また、血清EPA/AA比の閾値0.25未満を、例えば0.20未満あるいは0.10未満として血管疾患リスク被験者を抽出する工程とを備える方法である。
また、上記抽出方法の血中hs-CRP値1.0mg/L以上を、1.5mg/L以上あるいは2.0mg/L以上に変更して抽出することもできる。
本発明の検査キットは、上記心血管疾患リスクが高い被験者を抽出する方法に使用するための、少なくとも血中hs-CRP値を測定する手段を含む検査キットである。
hs-CRP値を測定するための手段としては、既に記載したとおり、ELISA法、ラテックス・ネフェロメトリー法、レーザー・ネフェロメトリー法、改良ラテックス免疫比濁法等によりhs-CRP値を求めるため、これらの方法に用いる試薬等を含めることが好ましい。
上記した方法によって心血管疾患リスクが高い被験者を抽出した後、当該被験者に対して本発明の心血管疾患一次予防剤を投与することで、心血管疾患の発症リスクを低減する方法である。発症リスクを低減するための指標として、本発明の予防方法においては、血中hs-CRP値を治療開始時または前回の測定の値に比べて0.1mg/L以上低下させること、好ましくは0.25mg/L以上低下させること、より好ましくは0.5mg/L以上低下させること、さらに好ましくは0.75mg/L以上低下させること、なお好ましくは1.0mg/L以上低下させること、なおいっそう好ましくは1.5mg/L以上低下させること、あるいは2.0mg/L未満に維持させること、好ましくは1.5mg/L未満に維持させること、より好ましくは1.25mg/L未満に維持させること、さらに好ましくは1.0mg/L未満に維持させること、なお好ましくは0.75mg/L未満に維持させること、なおいっそう好ましくは0.5mg/L未満に維持させること、かつ血清EPA/AA比を治療開始時または前回の測定の値に比べて0.1以上上昇させること、好ましくは0.20以上上昇させること、より好ましくは0.25以上上昇させること、さらに好ましくは0.40以上上昇させること、なお好ましくは0.50以上上昇させること、なおいっそう好ましくは0.60以上上昇させること、あるいは0.50以上に維持させること、好ましくは0.60以上に維持させること、より好ましくは0.70以上に維持させること、さらに好ましくは0.75以上に維持させること、なお好ましくは0.80以上に維持させること、なおいっそう好ましくは1.0以上に維持させること、を目標にすることもできる。
本実施例では、発明者らは、久山町研究の一環として、血清EPA/AA比と心血管疾患発症・死亡リスクとの関連を検討した。
久山町研究とは、福岡県福岡市に隣接した糟屋郡久山町(人口約8,400人)の住民を対象に1961年から行われている、脳卒中、心血管疾患等の疫学調査である。久山町住民は全国平均とほぼ同じ年齢・職業分布を持っており、偏りのほとんどない平均的な日本人集団であると考えられる。久山町研究の特徴として、全住民を対象(40歳以上)、前向きの追跡研究(コホート研究)、研究スタッフによる検診・往診、受診率(80%以上)、剖検率(約80%)、追跡率(99%以上)といった点が挙げられる。最大の特徴は、この剖検率の高さにある。正確な死因を知るという点において、剖検以上に正確な診断方法はない。しかも、追跡調査の精度も高いと考えられる。また、久山町研究では40歳以上の住民を5年ごとに集団に新しく加えているため、生活習慣の移り変わりの影響や、リスク因子の変遷をも窺い知ることができる。
2002年に登録された40歳以上の住民3,103例を被験者とした。心血管疾患の既往のある者およびEPA/AA比が得られていない者は除外された。また、平均追跡期間は5.1年であった。
被験者3,103例のうち、全死亡例は191例であった。このうち、死亡原因は、心血管疾患(疾病及び関連保健問題の国際統計分類第10版(ICD10):I00-I99)48例、癌(ICD10:C00-D48)70例、感染症(ICD10:A00-B99、J00-J39、J69、N13.6)39例、その他の原因34例であった。また、心血管疾患発症例(生存、死亡)は127例であり、このうち、冠動脈疾患発症例は49例、脳卒中発症例は83例であった。
(1)血清EPA/AA比
被験者の血清EPA/AA比は、被験者の血液を採取し、血清または血漿を加水分解し、総脂質中のEPAおよびAAをガスクロマトグラフ法で定量して濃度を測定し(単位:μg/mL)、EPAのAAに対する濃度比を算出した。
(2)hs-CRP値
被験者の血中hs-CRP値は、被験者の血液を採取し、市販の高感度CRP測定ラテックス試薬を用いて試料を処理し、生化学自動分析装置を用いて測定を行った(単位:mg/L)。
Cox比例ハザードモデルを用いて、血清EPA/AA比と、全死亡および心血管死との関係を、年齢および性別の潜在的交絡因子を調整して解析したところ、全死亡リスクは血清EPA/AA比が0.25未満、0.25-0.49、0.5-0.74および0.75以上の群で、それぞれ、1000人・年あたり、23.5、11.8、12.8および11.5人・年であった(傾向分析のp値=0.01)。同様に、心血管死リスクも血清EPA/AA比が低下するほど増加し、血清EPA/AA比が0.25未満、0.25-0.49、0.5-0.74および0.75以上の群で、それぞれ、1000人・年あたり、4.9、4.0、2.2および1.6人・年であった(傾向分析のp値=0.03)。すなわち、血清EPA/AA比が0.25未満の被験者は、血清EPA/AA比が0.75以上の被験者に比べて、全死亡リスクおよび心血管死リスクが、それぞれ、2.04倍および3.06倍であった。
被験者3,103例を、血中hs-CRP値が1.0mg/L未満の群(低hs-CRP群)と1.0mg/L以上の群(高hs-CRP群)との2群に分けた。さらに、両群を、それぞれ、血清EPA/AA比が0.25未満、0.25~0.49、0.50~0.74、0.75以上の4群ずつに分けた。
血中hs-CRP値および血清EPA/AA比によって区分した各群の被験者数は、表1および表2の「n」の欄に示すとおりであった。
また、図1には、(A)低hs-CRP群のハザード比を表す棒グラフ、および(B)高hs-CRP群のハザード比を表す棒グラフを示す。
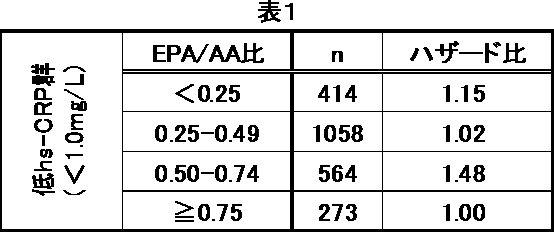

以上より、血中hs-CRP値と、血清EPA/AA比との組合せマーカーは、心血管疾患リスクを評価するためのマーカーとして有用であることがわかる。そして、この組み合わせマーカーを用いて、血中hs-CRP値が1.0mg/L以上、かつ血清EPA/AA比が0.50未満の群を心血管疾患の高リスク群と評価することが妥当であることがわかった。さらに、血中hs-CRP値が1.0mg/L以上で、血清EPA/AA比が0.25未満の群は、血清EPA/AA比が0.25以上0.50未満の群よりも有意に高いことから、血中hs-CRP値が1.0mg/L以上、かつ血清EPA/AA比が0.25未満の群を心血管疾患の特高リスク群、血中hs-CRP値が1.0mg/L以上、かつ0.25以上0.50未満の群を心血管疾患の高リスク群と評価してもよいことがわかった。
被験者を血中hs-CRP値が1.0mg/L以上の群と1.0mg/L未満の群との2群に分けた。血中hs-CRP値は、市販の測定キットを使用して定量した。
両群のそれぞれについて、心血管疾患、冠動脈疾患および脳卒中の5年発症率(5年間の発症率)およびハザード比を求め、表3の該当欄に表した。ハザード比は全体を基準(1.00)として、Cox比例ハザードモデルを用いて計算した。年齢、性別、高血圧、糖尿病、血清総コレステロール、脂質異常症治療剤の使用、BMI(ボディマス指数)、喫煙習慣およびアルコール摂取といった潜在的交絡因子を調整した。
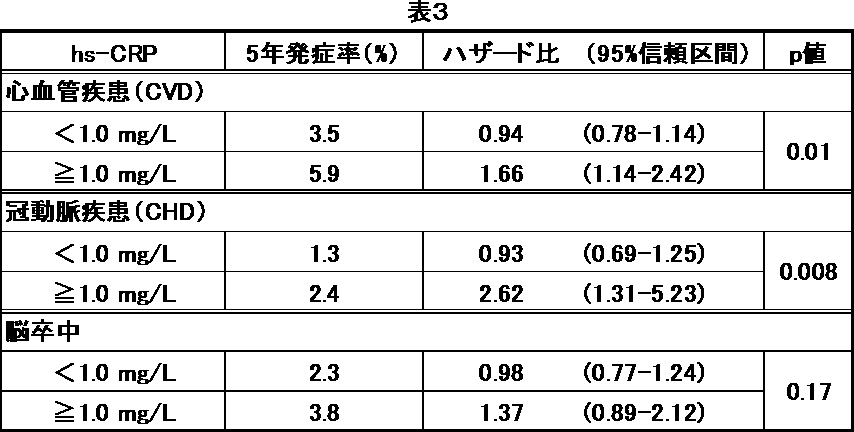
5年発症率は、血中hs-CRP値が1.0mg/L未満の群で3.5%であるのに対し、1.0mg/L以上の群では5.9%であり、上昇していた。
ハザード比は、血中hs-CRP値が1.0mg/L未満の群で0.94(95%信頼区間:0.78~1.14)であるのに対して、1.0mg/L以上の群では1.66(95%信頼区間:1.14~2.42)であり、血中hs-CRP値とハザード比との間に有意な関連が認められた(p値=0.01)。
血中hs-CRP値が1.0mg/L以上の被験者群では、血清EPA/AA比が0.25減少するごとに、心血管疾患の発症リスクが1.66倍有意に増加することが明らかとなった。
5年発症率は、血中hs-CRP値が1.0mg/L未満の群で1.3%であるのに対し、1.0mg/L以上の群では2.4%であり、上昇していた。
ハザード比は、血中hs-CRP値が1.0mg/L未満の群で0.93(95%信頼区間:0.69~1.25)であるのに対して、1.0mg/L以上の群では2.62(95%信頼区間:1.31~5.23)であり、血中hs-CRP値とハザード比との間に有意な関連が認められた(p値=0.008)。
血中hs-CRP値が1.0mg/L以上の被験者群では、血清EPA/AA比が0.25減少するごとに、冠動脈疾患の発症リスクが2.62倍有意に増加することが明らかとなった。
5年発症率は、血中hs-CRP値が1.0mg/L未満の群で2.3%であるのに対し、1.0mg/L以上の群では3.8%であり、上昇していた。
ハザード比は、血中hs-CRP値が1.0mg/L未満の群で0.98(95%信頼区間:0.77~1.24)であるのに対して、1.0mg/L以上の群では1.37(95%信頼区間:0.89~2.12)であった。また、血中hs-CRP値とハザード比との間では、異質性のp値=0.17であった。
血中hs-CRP値が1.0mg/L以上の被験者群では、血清EPA/AA比が0.25減少するごとに、脳卒中の発症リスクが1.37倍に増加することが明らかとなった。
被験者の全体から血中hs-CRP値が1.0mg/L以上の群(高hs-CRP群)を抽出した。血中hs-CRP値は、市販の測定キットを使用して定量した。
さらに、高hs-CRP群を、スタチン系薬剤投与の有無およびEPA投与の有無によって4群に分けた。
各群についての、心血管疾患、冠動脈疾患および脳卒中のイベントの有無を表4に表した。表中、「スタチン(-)+EPA(-)」は、被験者にスタチン系薬剤およびEPAのいずれも投与されていないことを表し、「スタチン(+)+EPA(-)」は、スタチン系薬剤は投与されているがEPAは投与されていないことを表し、「スタチン(-)+EPA(+)」は、スタチン系薬剤は投与されておらず、EPAは投与されていることを表し、「スタチン(+)+EPA(+)」は、スタチン系薬剤およびEPAがともに投与されていることを表す。さらに、イベント(-)およびイベント(+)は、それぞれ、イベントが発生しなかったことおよび発生したことを示す。

心血管疾患は、高hs-CRP群において、スタチン系薬剤の投与の有無によらず、EPAを投与した群では、イベントが発生しなかった。
また、EPAを投与しなかった群では、スタチン系薬剤を投与した群の方が、投与しなかった群よりもイベントの発生率が高かったが、これは、スタチン系薬剤を投与されている群は脂質異常症(高脂血症および/または高コレステロール血症)を有しているため、あるいは投与されていない群よりも脂質異常症の程度が重いため、ハイリスク群であることが原因となっていると考えられる。すなわち、心血管疾患は、高hs-CRP群おいて、脂質異常症の有無あるいは脂質異常症の程度によらず、EPAを投与した群では、イベントが発生しなかったと考えられる。
したがって、本発明の心血管疾患一次予防剤は、スタチン系薬剤投与の有無に関わらず、また、脂質異常症の有無あるいは脂質異常症の程度によらず、心血管疾患の一次予防に有効である。
冠動脈疾患は、高hs-CRP群において、スタチン系薬剤の投与の有無によらず、EPAを投与した群では、イベントが発生しなかった。
また、EPAを投与しなかった群では、スタチン系薬剤を投与した群の方が、投与しなかった群よりもイベントの発生率が高かったが、これは、スタチン系薬剤を投与されている群は脂質異常症(高脂血症および/または高コレステロール血症)を有しているため、あるいは投与されていない群よりも脂質異常症の程度が重いため、ハイリスク群であることが原因となっていると考えられる。すなわち、冠動脈疾患は、高hs-CRP群おいて、脂質異常症の有無あるいは脂質異常症の程度によらず、EPAを投与した群では、イベントが発生しなかったと考えられる。
したがって、本発明の心血管疾患一次予防剤は、スタチン系薬剤投与の有無に関わらず、また、脂質異常症の有無あるいは脂質異常症の程度によらず、冠動脈疾患の一次予防に有効である。
脳卒中は、高hs-CRP群および全体のいずれにおいても、スタチン系薬剤の投与の有無によらず、EPAを投与した群では、イベントが発生しなかった。
また、EPAを投与しなかった群では、スタチン系薬剤を投与した群と投与しなかった群との間に、イベントの発生率に大きな差はなかった。
したがって、本発明の心血管疾患一次予防剤は、スタチン系薬剤投与の有無に関わらず、また、脂質異常症の有無あるいは脂質異常症の程度によらず、脳卒中の一次予防に有効である。
Claims (24)
- 心血管疾患の既往がない、血中高感度C反応性蛋白質値が1.0mg/L以上の被験者に投与し、心血管疾患リスクを低下させるための、イコサペント酸、その塩およびエステルからなる群から選択される少なくとも1つを有効成分として含有する心血管疾患一次予防剤。
- 前記被験者の血清イコサペント酸/アラキドン酸比が0.50未満である、請求項1に記載の心血管疾患一次予防剤。
- 前記血清イコサペント酸/アラキドン酸比が0.25未満である、請求項2に記載の心血管疾患一次予防剤。
- 前記被験者の脂質異常症の有無によらず投与されて有効である、請求項1~3のいずれかに記載の心血管疾患一次予防剤。
- 前記脂質異常症が高LDLコレステロール血症である、請求項4に記載の心血管疾患一次予防剤。
- 前記被験者のHMG-CoA還元酵素阻害剤の適応の有無によらず投与されて有効である、請求項1~5のいずれかに記載の心血管疾患一次予防剤。
- 前記イコサペント酸、その塩およびエステルからなる群から選択される少なくとも1つが、イコサペント酸エチルエステルである、請求項1~6のいずれかに記載の心血管疾患一次予防剤。
- さらにドコサヘキサエン酸、その塩およびエステルからなる群から選択される少なくとも1つを含有する、請求項1~7のいずれかに記載の心血管疾患一次予防剤。
- 前記ドコサヘキサエン酸、その塩およびエステルからなる群から選択される少なくとも1つが、ドコサヘキエン酸エチルエステルである、請求項8に記載の心血管疾患一次予防剤。
- 前記心血管疾患が冠動脈疾患または脳卒中である、請求項1~9のいずれかに記載の心血管疾患一次予防剤。
- 前記冠動脈疾患が心筋梗塞または狭心症である、請求項10に記載の心血管疾患一次予防剤。
- 前記脳卒中が脳梗塞または脳出血である、請求項10に記載の心血管疾患一次予防剤。
- 血中高感度C反応性蛋白質値(hs-CRP値)と、血清イコサペント酸/アラキドン酸比(EPA/AA比)とを含む、心血管疾患の発症歴のない被験者の心血管疾患リスクを評価するための組合せマーカー。
- hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.50未満を心血管疾患高リスク
と評価する、請求項13に記載の組合せマーカー。 - hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.25未満を心血管疾患特高リスク、および
hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.25以上0.50未満を心血管疾患高リスク
と評価する、請求項13に記載の組合せマーカー。 - 前記心血管疾患が冠動脈疾患または脳卒中である、請求項13~15のいずれかに記載の組合せマーカー。
- 前記冠動脈疾患が心筋梗塞または狭心症である、請求項16に記載の組合せマーカー。
- 前記脳卒中が脳梗塞または脳出血である、請求項16に記載の組合せマーカー。
- 被験者のhs-CRP値を測定する工程と、
被験者のEPA/AA比を測定する工程と、
前記hs-CRP値と前記EPA/AA比とを組み合わせて、当該被験者を心血管疾患高リスク被験者として抽出する工程と
を備える、心血管疾患リスクが高い被験者の抽出方法。 - hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.50未満の被験者を心血管疾患高リスク被験者として抽出する、請求項19に記載の抽出方法。
- hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.25未満の被験者を心血管疾患特高リスク被験者、および
hs-CRP値が1.0mg/L以上、かつEPA/AA比が0.25以上0.50未満の被験者を心血管疾患高リスク被験者として抽出する、請求項19に記載の抽出方法。 - 被験者に心血管疾患の既往がない、請求項19~21のいずれかに記載の抽出方法。
- 請求項19~22のいずれかに記載の方法に使用するための、少なくとも血中hs-CRP値を測定する手段を含む検査キット。
- 請求項22に記載の方法によって抽出された被験者に、請求項1~12のいずれかに記載の心血管疾患一次予防剤を投与する工程を備える、心血管疾患一次予防方法。
Priority Applications (9)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| KR1020207017171A KR20200074259A (ko) | 2012-05-15 | 2013-05-14 | 고혈중 고감도 c반응성 단백질 환자의 심혈관 질병 1차 예방제 |
| CN201380024982.1A CN104271127A (zh) | 2012-05-15 | 2013-05-14 | 高血中高敏c反应蛋白患者的心血管疾病初级预防剂 |
| CA2873580A CA2873580C (en) | 2012-05-15 | 2013-05-14 | Cardiovascular disease primary prevention agent for patients having high blood levels of high-sensitivity c-reactive protein |
| JP2014515636A JP6254939B2 (ja) | 2012-05-15 | 2013-05-14 | 高血中高感度c反応性蛋白質患者の心血管疾患一次予防剤 |
| KR1020147031913A KR102125034B1 (ko) | 2012-05-15 | 2013-05-14 | 고혈중 고감도 c반응성 단백질 환자의 심혈관 질병 1차 예방제 |
| ES13790182T ES2749201T3 (es) | 2012-05-15 | 2013-05-14 | Agente de prevención primaria de enfermedad cardiovascular para pacientes que tienen altos niveles en sangre de proteína C reactiva de alta sensibilidad |
| EP13790182.3A EP2851069B1 (en) | 2012-05-15 | 2013-05-14 | Cardiovascular disease primary prevention agent for patients having high blood levels of high-sensitivity c-reactive protein |
| US14/400,777 US9700538B2 (en) | 2012-05-15 | 2013-05-14 | Cardiovascular disease primary prevention agent for patients having high blood levels of high-sensitivity C-reactive protein |
| US15/618,312 US20170273929A1 (en) | 2012-05-15 | 2017-06-09 | Cardiovascular disease primary prevention agent for patients having high blood levels of high-sensitivity c-reactive protein |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2012111900 | 2012-05-15 | ||
| JP2012-111900 | 2012-05-15 |
Related Child Applications (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| US14/400,777 A-371-Of-International US9700538B2 (en) | 2012-05-15 | 2013-05-14 | Cardiovascular disease primary prevention agent for patients having high blood levels of high-sensitivity C-reactive protein |
| US15/618,312 Continuation US20170273929A1 (en) | 2012-05-15 | 2017-06-09 | Cardiovascular disease primary prevention agent for patients having high blood levels of high-sensitivity c-reactive protein |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2013172344A1 true WO2013172344A1 (ja) | 2013-11-21 |
Family
ID=49583749
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2013/063419 Ceased WO2013172344A1 (ja) | 2012-05-15 | 2013-05-14 | 高血中高感度c反応性蛋白質患者の心血管疾患一次予防剤 |
Country Status (8)
| Country | Link |
|---|---|
| US (2) | US9700538B2 (ja) |
| EP (1) | EP2851069B1 (ja) |
| JP (1) | JP6254939B2 (ja) |
| KR (2) | KR20200074259A (ja) |
| CN (1) | CN104271127A (ja) |
| CA (1) | CA2873580C (ja) |
| ES (1) | ES2749201T3 (ja) |
| WO (1) | WO2013172344A1 (ja) |
Families Citing this family (31)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| PL2334295T3 (pl) | 2008-09-02 | 2017-12-29 | Amarin Pharmaceuticals Ltd | Kompozycja farmaceutyczna zawierająca kwas eikozapentaenowy i kwas nikotynowy oraz sposoby jej zastosowania |
| SG10201912687WA (en) | 2009-04-29 | 2020-02-27 | Amarin Pharmaceuticals Ie Ltd | Stable Pharmaceutical Composition And Methods Of Using Same |
| CN104042617A (zh) | 2009-04-29 | 2014-09-17 | 阿马里纳药物爱尔兰有限公司 | 含有epa和心血管剂的药物组合物以及使用其的方法 |
| EP3698781A1 (en) | 2009-06-15 | 2020-08-26 | Amarin Pharmaceuticals Ireland Limited | Compositions comprising eicosapentaenoic acid for treating myocardial infarction in a subject on concomitant statin therapy |
| RU2758369C2 (ru) | 2009-09-23 | 2021-10-28 | Амарин Фармасьютикалз Айрлэнд Лимитед | Фармацевтическая композиция, включающая омега-3 жирную кислоту и гидроксипроизводное статина, и способы ее применения |
| NZ744990A (en) | 2010-11-29 | 2019-10-25 | Amarin Pharmaceuticals Ie Ltd | Low eructation composition and methods for treating and/or preventing cardiovascular disease in a subject with fish allergy/hypersensitivity |
| US11712429B2 (en) | 2010-11-29 | 2023-08-01 | Amarin Pharmaceuticals Ireland Limited | Low eructation composition and methods for treating and/or preventing cardiovascular disease in a subject with fish allergy/hypersensitivity |
| US11291643B2 (en) | 2011-11-07 | 2022-04-05 | Amarin Pharmaceuticals Ireland Limited | Methods of treating hypertriglyceridemia |
| WO2013070735A1 (en) | 2011-11-07 | 2013-05-16 | Amarin Pharmaceuticals Ireland Limited | Methods of treating hypertriglyceridemia |
| US9827219B2 (en) | 2012-01-06 | 2017-11-28 | Amarin Pharmaceuticals Ireland Limited | Compositions and methods for lowering levels of high-sensitivity C-reactive protein (HS-CRP) in a subject |
| LT4338805T (lt) | 2012-06-29 | 2025-09-25 | Amarin Pharmaceuticals Ireland Limited | Eikozapentaeno rūgšties etilo esteris, skirtas panaudoti mažinant nemirtino miokardo infarkto riziką subjektui, gydomam statinais |
| US20150265566A1 (en) | 2012-11-06 | 2015-09-24 | Amarin Pharmaceuticals Ireland Limited | Compositions and Methods for Lowering Triglycerides without Raising LDL-C Levels in a Subject on Concomitant Statin Therapy |
| US9814733B2 (en) | 2012-12-31 | 2017-11-14 | A,arin Pharmaceuticals Ireland Limited | Compositions comprising EPA and obeticholic acid and methods of use thereof |
| US20140187633A1 (en) | 2012-12-31 | 2014-07-03 | Amarin Pharmaceuticals Ireland Limited | Methods of treating or preventing nonalcoholic steatohepatitis and/or primary biliary cirrhosis |
| US9452151B2 (en) | 2013-02-06 | 2016-09-27 | Amarin Pharmaceuticals Ireland Limited | Methods of reducing apolipoprotein C-III |
| US9624492B2 (en) | 2013-02-13 | 2017-04-18 | Amarin Pharmaceuticals Ireland Limited | Compositions comprising eicosapentaenoic acid and mipomersen and methods of use thereof |
| US9662307B2 (en) | 2013-02-19 | 2017-05-30 | The Regents Of The University Of Colorado | Compositions comprising eicosapentaenoic acid and a hydroxyl compound and methods of use thereof |
| US9283201B2 (en) | 2013-03-14 | 2016-03-15 | Amarin Pharmaceuticals Ireland Limited | Compositions and methods for treating or preventing obesity in a subject in need thereof |
| US20140271841A1 (en) | 2013-03-15 | 2014-09-18 | Amarin Pharmaceuticals Ireland Limited | Pharmaceutical composition comprising eicosapentaenoic acid and derivatives thereof and a statin |
| US10966968B2 (en) | 2013-06-06 | 2021-04-06 | Amarin Pharmaceuticals Ireland Limited | Co-administration of rosiglitazone and eicosapentaenoic acid or a derivative thereof |
| US20150065572A1 (en) | 2013-09-04 | 2015-03-05 | Amarin Pharmaceuticals Ireland Limited | Methods of treating or preventing prostate cancer |
| US9585859B2 (en) | 2013-10-10 | 2017-03-07 | Amarin Pharmaceuticals Ireland Limited | Compositions and methods for lowering triglycerides without raising LDL-C levels in a subject on concomitant statin therapy |
| US10561631B2 (en) | 2014-06-11 | 2020-02-18 | Amarin Pharmaceuticals Ireland Limited | Methods of reducing RLP-C |
| US10172818B2 (en) | 2014-06-16 | 2019-01-08 | Amarin Pharmaceuticals Ireland Limited | Methods of reducing or preventing oxidation of small dense LDL or membrane polyunsaturated fatty acids |
| US10406130B2 (en) | 2016-03-15 | 2019-09-10 | Amarin Pharmaceuticals Ireland Limited | Methods of reducing or preventing oxidation of small dense LDL or membrane polyunsaturated fatty acids |
| TW201900160A (zh) | 2017-05-19 | 2019-01-01 | 愛爾蘭商艾瑪琳製藥愛爾蘭有限公司 | 用於降低腎功能下降之個體中的三酸甘油酯之組合物及方法 |
| US11058661B2 (en) | 2018-03-02 | 2021-07-13 | Amarin Pharmaceuticals Ireland Limited | Compositions and methods for lowering triglycerides in a subject on concomitant statin therapy and having hsCRP levels of at least about 2 mg/L |
| EP3750535B1 (en) | 2018-09-24 | 2025-12-31 | Amarin Pharmaceuticals Ireland Limited | METHODS FOR REDUCING THE RISK OF CARDIOVASCULAR EVENTS IN A SUBJECT |
| BR112022009189A2 (pt) | 2019-11-12 | 2022-07-26 | Amarin Pharmaceuticals Ie Ltd | Métodos para reduzir o risco de eventos cardiovasculares em um sujeito com fibrilação atrial e/ou palpitação atrial |
| KR102362951B1 (ko) | 2020-08-13 | 2022-02-14 | 연세대학교 원주산학협력단 | 프로칼시토닌 대 c반응성 단백질의 비율을 이용한 허혈성 뇌졸중의 단기 사망률 예측 방법 |
| AU2022263358A1 (en) | 2021-04-21 | 2023-11-30 | Amarin Pharmaceuticals Ireland Limited | Methods of reducing the risk of heart failure |
Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2007039452A (ja) | 2005-07-08 | 2007-02-15 | Mochida Pharmaceut Co Ltd | 心血管イベント発症予防用組成物 |
| JP2007238594A (ja) | 2006-02-07 | 2007-09-20 | Mochida Pharmaceut Co Ltd | 脳卒中再発予防用組成物 |
Family Cites Families (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN102526733B (zh) | 2005-07-08 | 2014-09-03 | 持田制药株式会社 | 用于预防心血管事件发病的组合物 |
| BRPI0621313A2 (pt) | 2006-02-07 | 2011-12-06 | Mochilda Pharmaceutical Co Ltd | composição para previnir recorrência de acidente vascular cerebral |
| KR20140007973A (ko) * | 2009-02-10 | 2014-01-20 | 아마린 파마, 인크. | 고중성지방혈증 치료 방법 |
-
2013
- 2013-05-14 KR KR1020207017171A patent/KR20200074259A/ko not_active Ceased
- 2013-05-14 KR KR1020147031913A patent/KR102125034B1/ko active Active
- 2013-05-14 ES ES13790182T patent/ES2749201T3/es active Active
- 2013-05-14 US US14/400,777 patent/US9700538B2/en active Active
- 2013-05-14 CN CN201380024982.1A patent/CN104271127A/zh active Pending
- 2013-05-14 EP EP13790182.3A patent/EP2851069B1/en active Active
- 2013-05-14 WO PCT/JP2013/063419 patent/WO2013172344A1/ja not_active Ceased
- 2013-05-14 CA CA2873580A patent/CA2873580C/en active Active
- 2013-05-14 JP JP2014515636A patent/JP6254939B2/ja active Active
-
2017
- 2017-06-09 US US15/618,312 patent/US20170273929A1/en not_active Abandoned
Patent Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2007039452A (ja) | 2005-07-08 | 2007-02-15 | Mochida Pharmaceut Co Ltd | 心血管イベント発症予防用組成物 |
| JP2007238594A (ja) | 2006-02-07 | 2007-09-20 | Mochida Pharmaceut Co Ltd | 脳卒中再発予防用組成物 |
Non-Patent Citations (6)
| Title |
|---|
| "Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases 2012", 20 June 2012, JAPAN ATHEROSCLEROSIS SOCIETY |
| "The 75th Annual Scientific Meeting of the Japanese Circulation Society", ABSTRACT AND PROGRAM (CD-ROM), OJ-140, 2011 |
| ARTERIOSCLEROSIS, THROMBOSIS, AND VASCULAR BIOLOGY, vol. 28, 2008, pages 1385 - 1391 |
| HAYAKAWA ET AL.: "Association of plasma Omega- 3 to Omega-6 polyunsaturated fatty acid ratio with complexity of coronary artery lesion", INTERNAL MEDICINE, vol. 51, no. 9, 29 April 2012 (2012-04-29), pages 1009 - 14, XP055172967 * |
| SATOH ET AL.: "Purified Eicosapentaenoic Acid Reduces Small Dense LDL, Remnant Lipoprotein Particles, and C-Reactive Protein in Metabolic Syndrome", DIABETES CARE, vol. 30, no. 1, 2007, pages 144 - 6, XP002677407 * |
| THE LANCET, vol. 369, 2007, pages 1090 - 1098 |
Also Published As
| Publication number | Publication date |
|---|---|
| CA2873580C (en) | 2021-02-02 |
| EP2851069B1 (en) | 2019-08-28 |
| EP2851069A1 (en) | 2015-03-25 |
| US20150141510A1 (en) | 2015-05-21 |
| CA2873580A1 (en) | 2013-11-21 |
| JPWO2013172344A1 (ja) | 2016-01-12 |
| ES2749201T3 (es) | 2020-03-19 |
| US9700538B2 (en) | 2017-07-11 |
| KR102125034B1 (ko) | 2020-06-19 |
| EP2851069A4 (en) | 2015-12-23 |
| KR20200074259A (ko) | 2020-06-24 |
| US20170273929A1 (en) | 2017-09-28 |
| CN104271127A (zh) | 2015-01-07 |
| JP6254939B2 (ja) | 2017-12-27 |
| KR20150023258A (ko) | 2015-03-05 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| JP6254939B2 (ja) | 高血中高感度c反応性蛋白質患者の心血管疾患一次予防剤 | |
| JP6419927B2 (ja) | 対象の高感度(hs−crp)のレベルを低下させる組成物および方法 | |
| Tsujita et al. | Impact of dual lipid-lowering strategy with ezetimibe and atorvastatin on coronary plaque regression in patients with percutaneous coronary intervention: the multicenter randomized controlled PRECISE-IVUS trial | |
| JP7020756B2 (ja) | 対象の心血管イベントのリスクを低減する方法 | |
| Miller et al. | Normal triglyceride levels and coronary artery disease events: the Baltimore Coronary Observational Long-Term Study | |
| Libby et al. | Inflammation and atherosclerosis: role of C-reactive protein in risk assessment | |
| Berneis et al. | Low-density lipoprotein size and subclasses are markers of clinically apparent and non-apparent atherosclerosis in type 2 diabetes | |
| JP2019048843A (ja) | 心血管疾患を処置及び/又は予防するための組成物及び方法 | |
| US20110118350A1 (en) | Composition for preventing cardiovascular event in high-risk patient | |
| Andersson et al. | Echogenecity of the carotid intima–media complex is related to cardiovascular risk factors, dyslipidemia, oxidative stress and inflammation: The Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) study | |
| JP2025170360A (ja) | 心房細動および/または心房粗動を患う対象における心血管イベントのリスクを低減する方法 | |
| WO2014057522A1 (en) | Compositions and methods for treating non-alcoholic steatohepatitis | |
| Nakamura et al. | Different postprandial lipid metabolism and insulin resistance between non-diabetic patients with and without coronary artery disease | |
| Masuda et al. | Omega-3 fatty acid ethyl esters improve low-density lipoprotein subclasses without increasing low-density lipoprotein-cholesterol levels: A phase 4, randomized study | |
| Stein et al. | Treatment of severe hypertriglyceridemia lowers plasma viscosity | |
| JP2024527023A (ja) | His低応答者の治療 | |
| Ye et al. | Relation of C-reactive protein and carotid intima media thickness in Taiwanese with familial hypercholesterolemia | |
| Fukunaga et al. | Lipoprotein (a) as a risk factor for silent cerebral infarction in hemodialysis patients | |
| Krehić | Influence of modified diet and low grade physical activity on serum lipids in patients with type IIa and IIb dyslipoproteinaemia | |
| KR20240012390A (ko) | 심부전의 위험을 감소시키는 방법 | |
| BALLANTYNE | Lipid-Modifying Drugs | |
| Jee et al. | IP-0044 Does the Framingham risk score accurately predict coronary heart disease (CHD) risk in Korean men and women? Prospective analyses from the Korea medical insurance | |
| Jensen et al. | Prediction of ischemic heart disease by coronary calcium in patients with familial hypercholesterolemia |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 13790182 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 2014515636 Country of ref document: JP Kind code of ref document: A |
|
| ENP | Entry into the national phase |
Ref document number: 2873580 Country of ref document: CA |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 14400777 Country of ref document: US |
|
| ENP | Entry into the national phase |
Ref document number: 20147031913 Country of ref document: KR Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2013790182 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |