WO2014047432A1 - Clinical predictors of weight loss - Google Patents
Clinical predictors of weight loss Download PDFInfo
- Publication number
- WO2014047432A1 WO2014047432A1 PCT/US2013/060901 US2013060901W WO2014047432A1 WO 2014047432 A1 WO2014047432 A1 WO 2014047432A1 US 2013060901 W US2013060901 W US 2013060901W WO 2014047432 A1 WO2014047432 A1 WO 2014047432A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- metabolic
- subject
- gene
- procedure
- weight
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Classifications
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/68—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving nucleic acids
- C12Q1/6876—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes
- C12Q1/6883—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for diseases caused by alterations of genetic material
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/106—Pharmacogenomics, i.e. genetic variability in individual responses to drugs and drug metabolism
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/156—Polymorphic or mutational markers
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/158—Expression markers
Definitions
- the present invention relates to genetic predictors for treatment of metabolic disorders and diseases, such as obesity.
- identification of novel predictors of outcomes after metabolic and bariatric surgical procedures can both provide insight into the biological mechanisms of action of these procedures, as well as provide predictive markers that may be used to stratify those patients who may respond best to surgery or alternative treatments. Additionally, because numerous factors can affect a patient's outcomes following metabolic and bariatric surgery, and because some factors may be more relevant for some patients more than others depending on an individual's overall health and other biological characteristics, it can be difficult for medical professionals to consider and balance these factors to arrive at an accurate prediction as to how the surgery will affect a particular patient. It can be even more difficult, and likely impossible, for non-medical professionals, e.g., patients, to consider and balance such factors.
- a method of treating a subject having a metabolic disorder can include the steps of (a) obtaining a biological sample from the subject; (b) evaluating the sample for the presence or absence of at least one genetic indicator, and (c) performing a first metabolic procedure on the subject, if the at least one genetic indicator is/are absent, or (d) if the at least one genetic indicator is/are present, performing a second metabolic procedure, wherein the first metabolic procedure is different from a second metabolic procedure.
- a genetic indicator can include a genetic variation, such as a single nucleotide polymorphism, or a level of gene expression within or without a reference range.
- a method of treating a weight-related disorder in a subject can include (a) obtaining a sample comprising nucleic acids from the subject; (b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; and (c) based on if the genetic indicator(s) is absent in (b), performing a first metabolic procedure, or if the genetic indicator(s) is present in (b), performing a second metabolic procedure wherein the second metabolic procedure is different from the first metabolic procedure.
- the first and second metabolic procedures can be surgical, such as bariatric surgery, or non- surgical.
- the biological sample includes nucleic acids and evaluating the sample includes evaluating the nucleic acids for the presence or absence of at least one genetic indicator.
- the nucleic acids in the samples can be deoxyribonucleic acids (DNA) or ribonucleic acids (RNA).
- the nucleic acids can also be positive or negative for the genetic indicators.
- the genetic indicators can be at least one single nucleotide polymorphism (SNP) selected from Appendix A (i.e., SEQ ID NOs 129-837 (SNPs identified as statistically significant for percent weight loss)), Appendix B (additional SNPs identified as statistically significant for percent weight loss) and/or Appendix C (SNPs identified as statistically significant for percent excess body weight loss).
- Appendix A i.e., SEQ ID NOs 129-837 (SNPs identified as statistically significant for percent weight loss)
- Appendix B additional SNPs identified as statistically significant for percent weight loss
- Appendix C SNPs identified as statistically significant for percent excess body weight loss
- the absence or presence of the SNP can correlate with therapeutically effective weight loss of at least 20% weight change after a first metabolic procedure or a second metabolic procedure in the subject.
- the absence or presence of the SNP can correlate with therapeutically effective weight loss of at least 20% weight change after a first metabolic procedure or a second metabolic procedure without a bariatric surgery in the subject.
- additional clinical measurements can be obtained from the subject.
- the additional clinical measurements can be obtained prior to evaluating the nucleic acids in the sample or prior to performing a first metabolic procedure or a second metabolic procedure without a bariatric surgery.
- the additional clinical measurements can be obtained prior to evaluating the nucleic acids in the sample or prior to performing a first metabolic procedure or a second metabolic procedure without a bariatric surgery.
- the clinical measurement can include at least one of a pre-operative body mass index (BMI), anthropometric assessment, body composition, fat distribution, and energy expenditure assessment of the subject, a glucose tolerance or other marker of metabolic homeostasis, a bile acid profile, and a measurement of a biomarker obtained from a fluid, tissue, feces, or other sample obtained from the subject.
- BMI body mass index
- the clinical measurement is a pre-operative body mass index (BMI) of the subject.
- the clinical measurements can also include weight, gender, age, medical history, weight history, comorbid disease, physical activity, and/or status, BMI, ethnicity, prescription history and/or status, and types and outcomes of treatments previously tried (such as medications or other surgical and non-surgical treatments, etc).
- the nucleic acids can be negative for the genetic indicators and the clinical measurement is a pre-operative BMI of the subject, where the BMI is greater than 25 kg/m 2 .
- a method of treating a subject having a metabolic disorder can include the steps of (a) obtaining a biological sample from the subject; (b) evaluating expression of at least one gene in the sample, wherein the gene is differentially expressed after bariatric surgery or whose expression correlates with weight loss after a metabolic procedure; and (c) comparing the expression level of the gene(s) evaluated in (b) to a reference range, if expression of the gene(s) is outside the reference range, performing a first metabolic procedure on the subject, or if expression of the gene is inside the reference range, performing a second metabolic procedure on the subject.
- the first and second metabolic procedures can be surgical, such as bariatric surgery, or non-surgical.
- the gene(s) can be selected from SEQ ID NOs 1-128.
- the gene(s) can correlate with therapeutically significant weight loss associated with a metabolic procedure, such as bariatric surgery; improvement, alleviation or amelioration of one or more co- morbid conditions; absence of an adverse metabolic effect; and/or lack of therapeutically significant weight loss, lask of improvement, alleviation or amelioration of one or more co- morbid conditions, or an adverse metabolic event associated with bariatric surgery; or increased risk of obesity, or obesity-related co-morbid conditions in the subject.
- expression of the gene can correlate with therapeutically significant weight loss after a metabolic procedure, such as bariatric surgery.
- the reference range of gene expression can be determined from multiple patients having undergone a metabolic procedure, such as bariatric surgery.
- the reference range of gene expression can be an average of gene expression from multiple patients.
- the reference range of gene expression can be about +30%, +25%, +20%, +15%, +10%, or +5% of an average of gene expression from multiple patients.
- These may be a group of patients that have experienced therapeutically significant weight loss associated with a metabolic procedure, such as bariatric surgery; improvement, alleviation and/or amelioration of one or more co- morbid conditions, or the absence of an adverse metabolic event.
- the group of patients may have experienced lack of therapeutically significant weight loss, lack of
- the first and second metabolic procedures can be the same or different procedures.
- the first metabolic procedure can be a surgical procedure, such as bariatric surgery, including, but not limited to, gastric bypass, Roux-en-Y gastric bypass (RYGB), biliopancreatic diversion, partial gastrectomy procedures such as vertical sleeve gastrectomy, adjustable gastric banding, duodenal switch, duodenojejunal bypass, vertical banded
- gastroplasty intragastric balloon therapy, greater curvature plication, gastric placation (including anterior and anteroposterior plication) and other forms of gastric volume reduction, Magenstrasse and Mill, ileal transposition or interposition, small bowel transposition, biliary diversion, procedures involving anastomotic connections of the gastrointestinal tract, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, gastric electrical stimulation, small bowel electrical stimulation, vagal electrical stimulation, and vagal electrical inhibition.
- the first metabolic procedure can be a non-surgical procedure, such as, but not limited to, administering pharmacological and nutritional therapies, such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.; providing an alternative medical device based therapy, such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.; and/or the activation of brown adipose tissue.
- pharmacological and nutritional therapies such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.
- an alternative medical device based therapy such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.
- the activation of brown adipose tissue such as, but not limited to, administering pharmacological and nutritional therapies, such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.
- the second metabolic procedure can be the same as or different from the first metabolic procedure.
- the first metabolic procedure can be different from the second metabolic procedure.
- the first metabolic procedure can be a surgical procedure, such as bariatric surgery, and the second metabolic procedure can be non-surgical.
- the first metabolic procedure can be a surgical procedure, and the second metabolic procedure can be a different surgical procedure.
- the first metabolic procedure can be a non-surgical procedure and the second metabolic procedure can be a surgical procedure.
- a clinical measurement can be obtained from the subject.
- the clinical measurement can be obtained prior to or after obtaining a biological sample from the subject, prior to or after comparing the expression level of the gene(s), or prior to performing a first metabolic procedure or second metabolic procedure.
- the clinical measurement can include at least one of a pre-operative body mass index (BMI), a glucose tolerance, bile acid profile, and body composition/fat distribution of the subject.
- BMI pre-operative body mass index
- the clinical measurement is a pre-operative body mass index (BMI) of the subject.
- the nucleic acids can be negative for the genetic indicators and the clinical measurement is a pre-operative BMI of the subject, where the BMI is greater than 23 kg/m .
- kits for assessing the presence of a single nucleotide polymorphism (SNP) shown in Appendix A (SEQ ID NOs. 129-837), Appendix B, and/or Appendix C in a sample.
- the kit can include, but is not limited to, a pair of primers that specifically hybridize to regions proximal to the SNP selected from Appendix A (SEQ ID NOs. 129-837), Appendix B, and/or Appendix C and reagents for polymerase chain reaction (PCR).
- the kit can also include reagents for preparation, isolation and/or purification of nucleic acids from a sample.
- the kit can also be used in a method having the steps of (a) obtaining a sample comprising nucleic acids, such as deoxyribonucleic acids (DNA), from the subject; (b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; and if the genetic indicator(s) is absent in (b), performing a first metabolic procedure, such as a bariatric surgery, or if the genetic indicator(s) is present in (b), performing a second metabolic procedure, wherein the second metabolic procedure is different from the first metabolic procedure.
- the second metabolic procedure can exclude bariatric surgery.
- a method of treating obesity or a weight-related disorder in a subject can include (a) obtaining a sample comprising nucleic acids from the subject; (b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; (c) predicting an outcome of performing a first metabolic procedure based on the absence or presence of the genetic indicator(s); and (d) performing the first metabolic procedure or performing an alternative second metabolic procedure based on the predicted outcome.
- the method can include (a) obtaining a sample comprising nucleic acids from the subject; (b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; (c) predicting an outcome of performing a first metabolic procedure, such as a bariatric surgery, based on the absence or presence of the genetic indicator(s); and (d) performing the first metabolic procedure or performing an alternative second metabolic procedure.
- a first metabolic procedure such as a bariatric surgery
- the alternative second metabolic procedure can exclude bariatric surgery.
- the nucleic acids in the samples can be deoxyribonucleic acids (DNA) or ribonucleic acids (RNA).
- the nucleic acids can also be positive or negative for the genetic indicators.
- the genetic indicators can be at least one single nucleotide polymorphism (SNP) selected from Appendix A (SEQ ID NOs 129-837), Appendix B, and/or Appendix C that can be absence or presence in the nucleic acids.
- the outcome predicted from performing the metabolic procedure can be a therapeutically effective weight loss and/or the outcome can be an amelioration of or reduction of at least one weight-related co-morbid condition.
- the outcome when the outcome is a therapeutically effective weight loss, the weight loss can be at least 20% weight change.
- the outcome can also be a therapeutically effective weight loss when the genetic indicator(s) is absent.
- the outcome can further be a therapeutically effective weight loss and the metabolic procedure can be performed in the absence of the genetic indicator(s).
- the outcome predicted from performing the metabolic procedure can be lack of therapeutically significant weight loss or an adverse metabolic event associated with bariatric surgery, increased risk of obesity, or obesity-related co-morbid conditions in the subject, lack of therapeutically significant weight loss, lask of improvement, alleviation or amelioration of one or more co-morbid conditions, or an adverse metabolic event associated with bariatric surgery; or increased risk of obesity, or obesity-related co-morbid conditions in the subject.
- the outcome predicted from performing the metabolic procedure can be an amelioration of or reduction of at least one weight-related co-morbid condition.
- the co-morbid condition can be at least one of hypertension, dyslipidemia, triglyceride levels, diabetes, gastroesophageal reflux, fatty liver disease, steatohepatitis, heart or vascular disease, heart failure, cardiovascular risk, sleep apnea, Barrett's esophagus, asthma, osteoarthritis, compression fractures, gallstones, lymphedema, urinary incontinence, stroke, cognitive dysfunction, pseudotumor cerebri, inflammatory diseases, autoimmune diseases, gout, polycystic ovarian syndrome, infertility, depression, anxiety and/or panic disorders, cognitive or other neurological disorders, cancer risk and mortality (cancers including adenocarcinoma of pancreas, esophagus, gallbladder, pancreas, colon, rectum, breast, prostate; cervical carcinoma, endo
- predicting the outcome can include inputting the subject's data into a metabolic procedure outcome prediction system.
- the metabolic procedure outcome prediction system can be an interactive interface for modeling metabolic procedure outcomes, such as bariatric surgery outcomes.
- patient data that can be used for predicting outcomes can include the evaluation of the absence or presence of the genetic indicator(s), and at least one clinical measurement including a pre-operative body mass index (BMI), a glucose tolerance, bile acid profile, and body composition/fat distribution of the subject, or another measurement of gene expression in a cell or tissue, measurement of a peptide, protein, metabolite or other compound in blood or in a cell or in a tissue.
- BMI body mass index
- a method of treating a metabolic disorder in a subject is disclosed.
- the method can include measuring expression of the gene(s) in a sample from the subject;
- the method can result in a therapeutically significant weight loss.
- the method can also result in a therapeutically significant weight loss that is at least a 20% body weight change or an amelioration of or reduction of at least one weight-related co-morbid condition, where the co- morbid condition can be hypertension, dyslipidemia, triglyceride levels, diabetes,
- stomachsophageal reflux fatty liver disease, steatohepatitis, heart or vascular disease, heart failure, cardiovascular risk, sleep apnea, Barrett's esophagus, asthma, osteoarthritis, compression fractures, gallstones, lymphedema, urinary incontinence, stroke, cognitive dysfunction, pseudotumor cerebri, inflammatory diseases, autoimmune diseases, gout, polycystic ovarian syndrome, infertility, depression, anxiety and/or panic disorders, cognitive or other neurological disorders, cancer risk and mortality (cancers including adenocarcinoma of pancreas, esophagus, gallbladder, pancreas, colon, rectum, breast, prostate; cervical carcinoma, endometrial carcinoma, ovarian carcinoma, renal cell carcinoma, non-Hodgkins lymphoma), weight regain, excess weight loss, nutritional deficiency, constipation, diarrhea, marginal ulceration, dumping syndrome, reactive hypoglycemia, beta cell hyperfunction, gastrointestinal gastrointestinal
- kits are disclosed for assessing expression of at least one gene associated with response to a metabolic procedure in a sample.
- kits are disclosed for assessing the sequence of a gene or other chromosomal DNA.
- the kit can include, but is not limited to, a pair of primers that specifically hybridize to an expression product of the gene(s) selected from SEQ ID NOs 1-128.
- the kit can also include reagents for preparation, isolation and/or purification of nucleic acids and/or expression products from a sample.
- use of a single nucleotide polymorphism to evaluate a course of treatment for a metabolic disorder is disclosed.
- use of a gene expression level to evaluate a course of treatment for a metabolic disorder is disclosed.
- Figure 1 is a bar graph showing the excess body weight loss (EBWL) at postoperative weight nadir (achieved after at least 10 months of surgery without coexisting debilitating illness or use of weight lowering medications) after Roux-en-Y gastric bypass (RYGB) in 848 patients with severe obesity;
- EBWL excess body weight loss
- Figure 2 is a bar graph showing the mean difference in percent EBWL within patient pairs, according to type of relationship
- Figure 3 is a bar graph showing no difference on the residuals (deviations of the regressing postoperative BMI on preoperative BMI from the sample mean) from the cohort of 848 patients;
- Figure 4 is a bar graph showing absolute change in weight of the 848 patients after 1 year postoperative with patients in lower BMI groups losing significantly less weight;
- Figure 5 is a bar graph showing final weights obtained at 1 year postoperative of the 848 patients after 1 year postoperative;
- FIG. 6 is a bar graph showing the change in body mass index (BMI) of the 848 patients after 1 year postoperative with patients in lower BMI groups having significantly less change in BMI;
- Figure 7 is a bar graph showing final BMI obtained at 1 year postoperative of the 848 patients after 1 year postoperative;
- Figure 8 is a bar graph showing percent excess body weight lost ( EBWL) obtained at 1 year postoperative of the 848 patients after 1 year postoperative with patients at a lower pBMI losing more EBWL at both 1 year and weight nadir;
- EBWL percent excess body weight lost
- Figure 9 is a bar graph showing percent weight change (%WC) obtained at 1 year postoperative of the 848 patients after 1 year postoperative with no significant association between pBMI group and WC at one year, and a relatively weak association between pBMI and WC and weight nadir;
- Figure 10 is a bar graph showing percent change in weight in 858 unrelated
- Figure 11 is a bar graph showing percent change of weight nadir measured in a subgroup consisting of 693 patients (Cohort 1);
- Figure 12 is a bar graph showing percent change of weight nadir measured in an independent group of 349 Caucasian RYGB patients (Cohort 2);
- Figure 13 is a graphical representation of 112 significant (P ⁇ 5 x 10 "5 ) single nucleotide polymorphisms (SNPs) identified in Cohort 2;
- Figure 14 is a flow diagram illustrating direct or indirect association of the SNP with surrounding loci
- Figure 15 is a graphical representation of chromosome 11 with the SNPs identified as having significant association with percent total weight loss (%WL) at the lowest weight (weight nadir) after RYGB;
- Figure 16 is graph showing the association of carrying the minor allele (MA), rsl7702901, and percent weight change at nadir in patients homozygous null for MA, heterozygous for MA or homozygous for MA;
- Figure 17 is a bar graph showing percent weight change at nadir measured in pooled data from combination of Cohort 1 and Cohort 2 (953 RYGB patients).
- the shaded area identifies 171 patients having %WL categorized as less than or greater than or equal to 30% at weight nadir;
- Figure 18 is a bar graph showing percent weight loss with patients carrying at least one copy of the MA being 2.54 times more likely to fall below 30% WL (left shaded area) and no patients with this polymorphism lost more than 50% of his or her weight (right shaded area);
- Figure 19 is an area under the receiver operating characteristic curve (AUROC) showing that inclusion of rsl7709201 has a higher probability of being a predictor of weight loss than rsl7709201 as a random positive influence on weight loss;
- AUROC receiver operating characteristic curve
- Figure 20 is a bar graph of percent weight loss showing association of rs 17702901 with weight loss in RYGB patients.
- Figure 21 is a bar graph of percent weight loss showing a lack of an association of validated BMI locus, Melanocortin 4 Receptor (MC4R), with weight loss in RYGB patients.
- M4R Melanocortin 4 Receptor
- Figure 22 is a schematic diagram of the anatomy of Roux-en-Y gastric bypass.
- Tissues noted were dissected from mice 10 weeks after RYGB or sham operation;
- Figure 23A is a bar graph showing the comparative expression of st8sia2 in RYGB- treated and sham operated, weight matched mice (WMS). Grey bars denote the WMS group, blue bars the RYGB group. Error bars denote the standard error of the mean. * p ⁇ 0.05, ** p ⁇ 0.01, *** p ⁇ 0.001;
- Figure 23B is a bar graph showing the comparative expression of slco3al in RYGB- treated and sham operated, weight matched mice (WMS). Grey bars denote the WMS group, blue bars the RYGB group. Error bars denote the standard error of the mean. * p ⁇ 0.05, ** p ⁇ 0.01, *** p ⁇ 0.001;
- Figure 24A is a regional association plot showing the AQP11 locus.
- Each SNP is plotted as a diamond based on its chromosomal location (jc-axis) and -logw P value (left _y-axis). Recombination rates are plotted in grey toward the bottom of the graph (right _y-axis).
- the large upper diamond represents the top SNP in the region (rs7129556) from the genome- wide association study (GWAS), and the large lower diamond represents the p-value from that SNP in the replication cohort;
- Figure 24B is a bar graph showing the relative expression level of aqpll .
- Light bars denote the WMS group, dark bars the RYGB group.
- Error bars denote the standard error of the mean. * p ⁇ 0.05, ** p ⁇ 0.01, *** p ⁇ 0.001; and
- Figure 24C is a bar graph showing the relative expression level of clnsla. Light bars denote the WMS group, dark bars the RYGB group. Error bars denote the standard error of the mean * p ⁇ 0.05, ** p ⁇ 0.01, *** p ⁇ 0.001.
- SEQ ID NOs 1-128 in the present application correspond to SEQ ID NOs 1-128 of U.S. Provisional Application Serial No. 61/740,678, and SEQ ID NOs 129-837 correspond to the sequences from Appendix A of U.S. Provisional Application Serial No 61/704,434 (which is identical to Appendix A of the present application).
- Methods and kits are provided to evaluate genetic indicators, such as by identifying genetic indicators, and/or measuring and assessing gene expression for treatment of obesity and/or weight-related disorders.
- genetic indicators such as single nucleotide polymorphisms
- these genetic predictors can be indicators or predictors of improvements in comorbid conditions after bariatric surgery.
- certain genes demonstrate differential gene expression after a metabolic procedure, such as bariatric surgery. It has been further discovered that a correlation exists between the weight loss and other improvements in comorbidities and gene expression of certain genes.
- modulating certain gene expression can be therapeutic to improve comorbid conditions after bariatric surgery.
- the gene expression can serve a surrogate marker for whether a surgical procedure (e.g., bariatric surgery) is likely to lead to a successful outcome, or an alternative procedure is better suited for a certain patient or patient population. Therefore, the invention disclosed is generally directed to therapeutic methods and compositions for treating metabolic disorders, such as obesity and/or other weight-related disorders, in a subject by (1) evaluating genetic indicators, such as by evaluating the subject's deoxyribonucleic acids (DNA) for a presence or absence of one or more genetic indicators, and/or evaluating gene expression in the subject for an overexpression or an underexpression of one or more specific genes associated with metabolic disorders.
- DNA deoxyribonucleic acids
- Weight loss can be characterized using a number of different metrics, including the absolute number of pounds or body mass index (BMI) points lost, weight or BMI achieved after weight loss, the percent of baseline weight or BMI lost (% weight change (WC)), and percent excess body weight lost (% EBWL).
- BMI pounds or body mass index
- WC percent weight change
- % EBWL percent excess body weight lost
- weight-related disorder refers to disorders, diseases, and conditions that are caused or characterized by abnormal energy use or consumption leading to excessive weight gain or loss, altered responses to ingested or endogenous nutrients, energy sources, hormones or other signaling molecules within the body or altered metabolism of carbohydrates, lipids, proteins, nucleic acids or a combination thereof.
- a weight-related disorder can be associated with either a deficiency or excess in a metabolic pathway resulting in an imbalance in metabolism of nucleic acids, proteins, lipids, and/or carbohydrates.
- Factors affecting metabolism include, and are not limited to, the endocrine (hormonal) control system (e.g., the insulin pathway, the enteroendocrine hormones including GLP-1, PYY or the like), the neural control system (e.g., GLP-1 or other neurotransmitters in the brain, spinal cord, peripheral or enteric nervous systems) or the like.
- the endocrine (hormonal) control system e.g., the insulin pathway, the enteroendocrine hormones including GLP-1, PYY or the like
- the neural control system e.g., GLP-1 or other neurotransmitters in the brain, spinal cord, peripheral or enteric nervous systems
- weight-related disorders can be obesity, diabetes, including type II diabetes, insulin-deficiency, insulin-resistance, insulin- resistance related disorders, glucose intolerance, syndrome X, inflammatory and immune disorders, dyslipidemia, metabolic syndrome, non-alcoholic fatty liver, abnormal lipid metabolism, obstructive sleep apnea, asthma, autoimmune and inflammatory disorders, cancer, cognitive and neurodegenerative disorders, hypertension, high cholesterol, anxiety, congestive heart failure, ischemic heart disease, GERD, atherogenic dyslipidemia, hyperlipidemic conditions such as atherosclerosis, hypercholesterolemia, and other coronary artery diseases in mammals, and other disorders of metabolism.
- diabetes including type II diabetes, insulin-deficiency, insulin-resistance, insulin- resistance related disorders, glucose intolerance, syndrome X, inflammatory and immune disorders, dyslipidemia, metabolic syndrome, non-alcoholic fatty liver, abnormal lipid metabolism, obstructive sleep apnea, asthma, autoimmune and inflammatory disorders, cancer, cognitive and neuro
- the term "obesity" or “obese” typically refers to a non-Asian individual having a body mass index (BMI) of >30 kg/m 2 or >27 kg/m 2 in Asian individuals and "overweight” typically refers to a non-Asian individual having a body mass index (BMI) of >25 kg/m 2 or >23 kg/m 2 in Asian individuals.
- BMI is a measure expressing the relationship (or ratio) of weight-to-height based on a mathematical formula in which a person's body weight in kilograms is divided by the square of his or her height in meters (i.e., wt/(ht) ).
- co-morbidity typically refers to, but is not limited to, hypertension, dyslipidemia, triglyceride levels, diabetes,
- stomachsophageal reflux fatty liver disease, steatohepatitis, heart or vascular disease, heart failure, cardiovascular risk, sleep apnea, Barrett's esophagus, asthma, osteoarthritis, compression fractures, gallstones, lymphedema, urinary incontinence, stroke, cognitive dysfunction, pseudotumor cerebri, inflammatory diseases, autoimmune diseases, gout, polycystic ovarian syndrome, infertility, depression, anxiety and/or panic disorders, cognitive or other neurological disorders, cancer risk and mortality (cancers including adenocarcinoma of pancreas, esophagus, gallbladder, pancreas, colon, rectum, breast, prostate; cervical carcinoma, endometrial carcinoma, ovarian carcinoma, renal cell carcinoma, non-Hodgkins lymphoma), weight regain, excess weight loss, nutritional deficiency, constipation, diarrhea, marginal ulceration, dumping syndrome, reactive hypoglycemia, beta cell hyperfunction, gastrointestinal gastrointestinal
- Metabolic disorder or syndrome is tied to the body's metabolism, and more likely to conditions that influence metabolism, such as insulin resistance. Metabolic disorder or syndrome can also be characterized by excess body fat, atherogenic dyslipidemia, elevated blood pressure and insulin resistance, among others.
- Other weight-related disorders can include conditions that occur or cluster together, and/or increase the risk for heart disease, stroke, diabetes, and obesity. Having just one of these conditions such as increased blood pressure, elevated insulin levels, excess body fat around the waist or abnormal cholesterol levels can increase the risk of the above mentioned diseases. In combination, the risk for coronary heart disease, stroke, insulin-resistance syndrome, and diabetes is even greater.
- metabolic procedures can include surgical and nonsurgical procedures. Surgical procedures can achieve a sustained weight reduction of up to 70% of excess body weight in the majority of patients, and are often more effective than nonsurgical approaches. Nonlimiting examples of surgical procedures can include bariatric surgery.
- "bariatric surgery” generally refers and can include procedures often referred to as metabolic surgery or therapy, as well as a variety of procedures performed in a subject that leads to a physiologic improvement in energy balance, nutrient utilization, or metabolic disorders. These procedures often, but not always, result in weight loss.
- Bariatric surgery refers to a surgical procedure to alter gastrointestinal structure or function so as to affect body weight, body composition, or energy balance regulation or otherwise alter metabolic function.
- Some non-limiting examples of bariatric surgery can be any form of gastric bypass, Roux-en-Y gastric bypass (RYGB), biliopancreatic diversion, partial gastrectomy procedures such as vertical sleeve gastrectomy, adjustable gastric banding, duodenal switch, duodenojejunal bypass, vertical banded gastroplasty, intragastric balloon therapy, greater curvature plication, gastric plication (including anterior and anteroposterior plication) and other forms of gastric volume reduction, Magenstrasse and Mill, ileal transposition or interposition, small bowel transposition, biliary diversion, procedures involving anastomotic connections of the gastrointestinal tract (e.g., jejunoileostomy, etc.), gastric electrical stimulation, small bowel electrical stimulation, vagal electrical stimulation, vagal electrical inhibition
- Metabolic procedures can also include non- surgical procedures including, by way of non-limiting examples, administering pharmacological and nutritional therapies, such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.; providing an alternative medical device based therapy, such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.; and/or the activation of brown adipose tissue.
- pharmacological and nutritional therapies such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.
- an alternative medical device based therapy such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.
- an alternative medical device based therapy such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.
- a method of treating a metabolic disorder, such as obesity, in a subject can include obtaining a sample with DNA from the subject, evaluating the DNA for the presence or absence of one or more genetic indicators and performing a first metabolic procedure, such as bariatric surgery or a second metabolic procedure, excluding bariatric surgery, depending on the absence or presence of one or more genetic indicators.
- a method of treating a metabolic disorder in a subject can include obtaining a sample from the subject, evaluating the sample for expression of at least one gene (wherein the gene is shown to be differentially expressed after bariatric surgery or wherein expression of the gene correlates with weight loss after a metabolic procedure), and performing a first metabolic procedure or a second metabolic procedure excluding a bariatric surgery depending on the expression of gene(s).
- Identification of specific genetic indicators, such as SNPs associated with weight loss after RYGB, or expression patterns, such as expression of genes associated with weight loss after RYGB, may both enhance the understanding of the mechanisms of weight loss as well as help identify those patients for whom bariatric surgery procedures are most effective.
- polymorphism refers to a variation in the sequence of a gene in the genome amongst a population, such as allelic variations and other variations that arise or are observed.
- Genetic polymorphisms refers to the variant forms of DNA sequences that can arise as a result of nucleotide alteration or substitution, deletion, insertion, rearrangement or duplication, for example.
- a polymorphism refers to the occurrence of two or more genetically determined alternative sequences or alleles in a population.
- polymorphisms can occur in coding and non-coding portions of the genome, and can be manifested or detected as differences in nucleic acid sequences, gene expression, and/or other differences in mRNA structure and function, including, for example transcription, processing, translation, transport, protein processing, trafficking, DNA synthesis, expressed proteins, other gene products or products of biochemical pathways or in post-translational modifications and any other differences manifested among members of a population.
- a "single nucleotide polymorphism” or "SNP” refers to a polymorphism that arises as the result of a single base change, such as an insertion, deletion or change in a base.
- a polymorphic marker or site is the locus at which divergence occurs. Such a site may be as small as one base pair (an SNP).
- Polymorphic markers include, but are not limited to, restriction fragment length polymorphisms, copy number variations, variable number of tandem repeats (VNTR's), hypervariable regions, minisatellites, dinucleotide repeats, trinucleotide repeats, tetranucleotide repeats and other repeating patterns, simple sequence repeats and insertional elements, such as Alu.
- Polymorphic forms also are manifested as different mendelian alleles for a gene.
- the genomes of all organisms undergo spontaneous mutation in the course of their continuing evolution, generating variant forms of progenitor genetic sequences.
- a variant form may confer differences in proteins, protein modifications, RNA expression, RNA modification, DNA and RNA methylation, regulatory factors that alter gene expression and DNA replication, and any other manifestation of alterations in genomic nucleic acid or organelle nucleic acids.
- an "isolated" nucleic acid molecule such as a nucleic acid molecule containing a SNP genetic indicator or an expression product of a gene or other transcript (e.g., messenger RNA, microRNA or other non-coding RNA), can be substantially free of other cellular material, or culture medium when produced by recombinant techniques, or chemical precursors or other chemicals when chemically synthesized.
- a nucleic acid molecule can be fused to other coding or regulatory sequences and still be considered “isolated.”
- Nucleic acid molecules present in non-human transgenic animals, which do not naturally occur in the animal, are also considered “isolated.”
- recombinant DNA molecules contained in a vector are considered “isolated.”
- Further examples of "isolated” DNA molecules include recombinant DNA molecules maintained in heterologous host cells, and purified (partially or substantially) DNA molecules in solution.
- Isolated RNA molecules include in vivo or in vitro RNA transcripts of the isolated SNP-containing DNA molecules of the present invention.
- Isolated nucleic acid molecules according to the present invention further include such molecules produced synthetically.
- a nucleic acid molecule can include one or more SNPs with flanking nucleotide sequences on either side of the SNPs.
- a flanking sequence can include nucleotide residues that are naturally associated with the SNP site and/or heterologous nucleotide sequences.
- the flanking sequence can be up to about 500, 300, 100, 60, 50, 30, 25, 20, 15, 10, 8, or 4 nucleotides (or any other length in between) on either side of a SNP.
- an "isolated protein,” once expressed, can be isolated by lysing cells and applying standard protein isolation techniques to the lysates or the pellets. Monitoring the purification process can be accomplished by using Western blot techniques or radioimmunoassay or other standard immunoassay techniques.
- an "amplified polynucleotide” can include a nucleic acid molecule containing one or more SNPs or a gene that can be replicated by at least two fold through any nucleic acid amplification method performed in vitro.
- an amplified polynucleotide is the result of at least a ten fold, fifty fold, one hundred fold, one thousand fold, or even ten thousand fold increase as compared to its starting amount in a test sample.
- a polynucleotide of interest is often amplified at least fifty thousand fold in amount over the unamplified DNA template, but the precise amount of amplification needed for an assay depends on the sensitivity of the subsequent detection method used.
- a subject or patient may be homozygous or heterozygous for an allele at each SNP position.
- a SNP can, in some instances, be referred to as a "cSNP" to denote that the nucleotide sequence containing the SNP is an amino acid coding sequence. While SNPs can be bi-, tri-, or tetra-allelic, the vast majority of the SNPs are bi-allelic, and are thus often referred to as "bi- allelic markers,” or "di-allelic markers.”
- references to "SNPs" and SNP genotypes include individual SNPs and/or haplotypes, which are groups of SNPs that are generally inherited together. Haplotypes can have stronger correlations with diseases or other phenotypic effects compared with individual SNPs, and therefore may provide increased diagnostic accuracy in some cases.
- An "allele” is an alternative form or variation in a DNA sequence. Many SNPs have only two alleles: minor and major alleles. SNPs are routinely used in SNP-based genetic linkage analysis to map a disease to a particular locus, the position of a gene (or SNP) on a chromosome.
- Methods and kits are provided to identify genetic indicators and/or evaluate and assess expression of genes associated with response to a metabolic procedure, such as bariatric surgery, for treatment of metabolic disorders. It has been discovered that genetic indicators, such as single nucleotide polymorphisms, and gene expression, such as genes associated with response to a metabolic procedure, can indicate weight loss potential after the metabolic procedure, such as bariatric surgery. By obtaining a sample from a subject and extracting nucleic acids from or analyzing gene expression in the sample, response to the metabolic procedure, e.g. weight loss potential after the bariatric surgery, can be predicted and/or assessed.
- subject refers to any living organism, including, but not limited to, humans, nonhuman primates such as chimpanzees and other apes and monkey species; farm animals such as cattle, sheep, pigs, goats and horses; domestic mammals such as dogs and cats; laboratory animals including rodents such as mice, rats, rabbits and guinea pigs, and the like.
- the term does not denote a particular age or sex.
- the subject is human.
- the subject is a patient.
- sample is intended to include tissues, cells, fluids and biological samples isolated from a subject, as well as tissues, cells and fluids present within a subject.
- the sample can be a tissue sample, such as from an organ, or fluid, ascites, and any other sample that is used by those familiar with the art.
- the sample can be derived from any source which contains proteins or expression products and/or nucleic acids, DNA (e.g., chromosomal nucleic acids) or RNA, such as a blood sample, body excrements such as semen, saliva, stool, urine, amniotic fluid and so forth, sample of cerebrospinal fluid, or tissue sample from skin, muscle, buccal or conjunctival mucosa, placenta, gastrointestinal tract or other organs.
- DNA e.g., chromosomal nucleic acids
- RNA such as a blood sample, body excrements such as semen, saliva, stool, urine, amniotic fluid and so forth, sample of cerebrospinal fluid, or tissue sample from skin, muscle, buccal or conjunctival mucosa, placenta, gastrointestinal tract or other organs.
- a sample of proteins and/or nucleic acid from fetal cells or tissue can be obtained by appropriate methods, such as by amniocentesis or chorionic villus sampling (direct or cultured).
- the sample can be a biopsy sample or a small number of cells or a tissue sample removed for processing.
- biopsy methods can include, but are not limited to, oral swab, brush cytology, core needle biopsy, surgical biopsy, punch biopsy, shave biopsy, incisional/excisional biopsy and curettage biopsy.
- the sample of cells or tissue sample can be obtained from the subject by biopsy or surgical resection.
- a sample of cells, tissue, or fluid can be removed by needle aspiration biopsy.
- a fine needle attached to a syringe is inserted through the skin and into the organ or tissue of interest.
- the needle is typically guided to the region of interest using ultrasound or computed tomography (CT) imaging.
- CT computed tomography
- a sample of cells or tissue may also be removed by incisional or core biopsy. For this, a cone, a cylinder, or a tiny bit of tissue can be removed from the region of interest.
- CT imaging, ultrasound, or endoscopy can be used to guide this type of biopsy.
- RNA or protein may also be extracted from a fixed or wax-embedded tissue sample.
- Direct assessment for the presence of the genetic identifiers or for gene expression can be performed on a sample without processing to isolate nucleic acids or gene expression products.
- a sample can be processed to enhance access to gene expression products, nucleic acids, or copies of nucleic acids (e.g., amplification of nucleic acids), and the processed sample can then be used to assess for the presence of the genetic identifiers or for gene expression.
- cDNA is prepared from a sample comprising mRNA, for use in the methods. The mRNA can be isolated from the sample and converted into cDNA.
- an amplification method can be used to amplify nucleic acids for use as the test sample in the assessment for the presence or absence of a genetic identifier(s) or for gene expression.
- the nucleic acids can be isolated from the samples or can be processed and analyzed within the sample.
- Nucleic acids including RNA, DNA, or cDNA, proteins or other expression products can be analyzed for the genetic indicator(s) or measured to determine gene expression from a sample.
- the presence of genetic indicator(s) or gene expression can be evaluated in nucleic acids or proteins in vitro, in situ, as well as in vivo.
- in vitro techniques for detection of genetic indicator(s) in mRNA or for measuring expression can include assays such as ELISA assay and Western blot analysis, immunocytochemical assays, assessment of mRNA in PCR, q-PCR, northern hybridizations and in situ hybridizations, assessment of cDNA in Southern hybridizations, PCR, quantitative PCR (qPCR), and introduction of labeled nucleic acids for incorporation into the nucleic acids, for example, the radiolabeled nucleic acids whose presence and location in a subject can be detected by standard imaging techniques.
- assays such as ELISA assay and Western blot analysis, immunocytochemical assays, assessment of mRNA in PCR, q-PCR, northern hybridizations and in situ hybridizations, assessment of cDNA in Southern hybridizations, PCR, quantitative PCR (qPCR), and introduction of labeled nucleic acids for incorporation into the nucleic acids, for example, the radiolabeled nucleic acids whose presence and location in a subject
- Another embodiment for identifying genetic indicators in RNA or DNA or for measuring gene expression can include the use of a labeled nucleic acid probe capable of hybridizing to a mRNA or cDNA.
- a labeled nucleic acid probe capable of hybridizing to a mRNA or cDNA.
- a wide variety of conventional techniques are available, including mass spectrometry, chromatographic separations, 2-D gel separations, microarrays, binding assays (e.g., immunoassays), competitive inhibition assays, one- and two-dimensional gels and sandwiched ELISA.
- Typical methodologies for RNA detection include RNA extraction from a cell or tissue sample, followed by hybridization of a labeled probe, (e.g., a labeled probe, (e.g., a labeled probe, (e.g., a labeled probe, (e.g., a labeled probe, (e.g., a labeled probe, (e.g., a
- RNA complementary polynucleotide
- detection of the probe e.g., Northern blotting, direct sequencing, gel electrophoresis, column
- Primers based on a nucleotide sequence specific for one or more of the genetic indicators or genes can be used to analyze the presence or absence in or to measure expression of the corresponding gene(s) or genetic indicator(s).
- a primer pair can be designed by utilizing primer design software, such as GenScript, Primer3, PRIDE and Primer Express. Commercial primers are also available for purchase corresponding to multiple locations throughout the gene.
- the primers can be at least 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 20, 25, 30, 35, or 40 basepairs in length. In an exemplary embodiment, the primers can be at least 10 basepairs in length.
- the primers can also hybridize to a region of nucleic acids (mRNA, cDNA or genomic DNA) proximal or in the vicinity of the genetic indicator or the gene.
- the primer can be similar (sufficiently similar or identical to hybridize to the sequence) or complementary (sufficiently similar or identical to hybridize to the complement sequence) to a nucleic acid sequence upstream or downstream from the genetic indicator.
- the primer can hybridize to a sequence that is at least 50, 60, 70, 80, 90, 100, 110, 120, 130, 140, 150, 160, 170, 180, 190, 200, 250, 300, 350, 400, 450, 500, 550, 600, 650, 700, 750, 850, 900, 950, 1000 basepairs or more or any number of basepairs in between from the genetic indicator.
- the primers can specifically hybridize to a region proximal to one or more genetic indicators (such as a single nucleotide polymorphism (SNP) as shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C).
- the primers can be complementary to a nucleic acid sequence of at least 10 bases found at least 200 basepairs or more from the genetic indicator.
- the primer can be similar (sufficiently similar or identical to hybridize to the sequence) or complementary (sufficiently similar or identical to hybridize to the complement sequence) to a nucleic acid sequence of the gene.
- the primers can be specific for at least one of SEQ ID NOs 1-128. See Table 10 for correspondence of SEQ ID NO to gene
- the diagnostic kit and/or device can include, but is not limited to, sample collection materials (storage solutions and collection apparatus such as swab, biopsy needle, blood/body fluid needle, brush, etc), protein, DNA or RNA extraction and isolation materials (solutions and enzymes for performing such procedures); nucleic acid amplification materials (solutions, enzymes and primers specific for the genetic indicator(s) or primers for performing such procedures); and sequencing materials (solutions, enzymes and gene specific primers for performing such procedures).
- sample collection materials storage solutions and collection apparatus such as swab, biopsy needle, blood/body fluid needle, brush, etc
- protein DNA or RNA extraction and isolation materials
- nucleic acid amplification materials solutions, enzymes and primers specific for the genetic indicator(s) or primers for performing such procedures
- sequencing materials solutions, enzymes and gene specific primers for performing such procedures.
- the diagnostic kit and/or device can include any of the above and exclude any materials from the above.
- the diagnostic kit and/or device can include DNA polymerase chain reaction amplification solutions and/or enzymes and at least one set of primers specific for a genetic indicator. In another exemplary embodiment, the diagnostic kit and/or device can include DNA polymerase chain reaction amplification solutions and/or enzymes and at least one set of gene specific primers.
- a method of treating obesity or weight-related disorders includes evaluating DNA for the absence or presence of one or more genetic indicators, such as SNPs.
- the DNA can be positive or negative for one or more indicators.
- a DNA sample from a subject can be evaluated for the presence or absence of the genetic indicator(s).
- the DNA can be negative for the indicator(s) and the pre-operative BMI can be greater than 20 kg/m 2 .
- the presence or absence of the genetic indicator(s) can correlate with therapeutically effective weight loss associated with bariatric surgery; improvement, alleviation or amelioration of one or more co-morbid conditions; and/or lack of therapeutically effective weight loss associated with bariatric surgery, increased risk of obesity or obesity-related co- morbid conditions in the subject.
- the presence or absence of the genetic indicator(s) can correlate with therapeutically effective weight loss after bariatric surgery in the subject.
- Therapeutically effective weight loss can be characterized by loss of at least 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, 80%, 85% or more of excess body weight.
- Therapeutically effective weight loss can also be characterized as at least 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, or more weight change.
- therapeutically effective weight loss can be characterized by change of at least 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, 80%, 85% or more of body mass index.
- body weight, weight change, and/or body mass index measurements can be determined by taking the measurement of the subject prior to treatment or preoperatively and compare the
- the therapeutically effective weight loss is at least 20% weight change after bariatric surgery or alternative treatment in the subject.
- the presence or absence of one or more genetic indicator(s) can correlate with improvement, alleviation or amelioration of one or more co-morbid conditions in the subject.
- the presence or absence of the genetic indicator(s) can correlate with, for example, reduced hypertension, reduced dyslipidemia, improvement or alleviation of diabetes, reduced acid reflux, alleviation of fatty liver or steatohepatitis, reduced risk of heart disease, alleviation of depression, alleviation of sleep apnea, alleviation of asthmatic symptoms, alleviation of arthritis, reduced risk of compression fractures, reduced occurrence of gallstones, lymphoedema, alleviation of urinary incontinence, reduced risk of stroke, reduced risk of cancer and/or reduced risk of other metabolic syndromes.
- the presence or absence of one or more genetic indicator(s) can correlate with lack of therapeutically effective weight loss associated with bariatric surgery or increased risk of obesity, or obesity-related co-morbid conditions in the subject.
- the presence or absence of the genetic indicator(s) can correlate with, for example, lack of weight loss after bariatric surgery, increased hypertension, risk of dyslipidemia, development of diabetes, acid reflux, fatty liver disease or steatohepatitis, heart disease, depression, sleep apnea, asthmatic symptoms, arthritis, compression fractures, gallstones, lymphoedema, urinary incontinence, stroke, cancer and/or risk of other metabolic syndromes.
- the genetic indicators can be single nucleotide polymorphisms that occur in coding and non-coding portions of the genome, and can be manifested or detected as differences in nucleic acid sequences (DNA), gene expression products (RNA and proteins), including, for example transcripts (mRNA, miRNA, and others), proteins, other gene products or products of biochemical pathways or in post-translational modifications and any other differences manifested among members of a population.
- one or more genetic indicators are absent from the subject's nucleic acid sample, such as DNA, where at least one genetic indicator is a single nucleotide polymorphism (SNP) shown in Appendix A (SEQ ID NOs 129-837), Appendix
- SNP single nucleotide polymorphism
- one or more genetic indicators are present in the subject's nucleic acid sample, such as DNA, where at least one genetic indicator is a single nucleotide polymorphism (SNP) shown in Appendix A (i.e, SEQ ID NOs 129-837 (SNPs identified as statistically significant for percent weight loss)), Appendix B (additional SNPs identified as statistically significant for percent weight loss) or Appendix C (SNPs identified as statistically significant for percent excess body weight loss).
- SNP single nucleotide polymorphism
- Each SNP sequence is associated with a unique accession number (e.g., rs number) that is available in the Single Nucleotide Polymophism Database hosted by the National Center for Biotechnology Information (NCBI) to identify the genetic variation and sequence information.
- one or more genetic indicators are absent from the subject's nucleic acid sample, such as DNA, and one or more different genetic indicators are present in the subject's DNA sample, where at least one genetic indicator is a single nucleotide polymorphism (SNP) shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C.
- the genetic indicator(s) can be at least one single nucleotide
- SNP polymorphism
- Selected genetic indicators such as the SNPs shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C, can be positive or negative indicators for successful obesity or weight-related disorder treatment.
- the genetic indicator can be one or more SNPs shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C, such as SEQ ID NO 129-SEQ ID NO 138, SEQ ID NO 129-SEQ ID NO 148, SEQ ID NO 129-SEQ ID NO 158, SEQ ID NO 129-SEQ ID NO 168, SEQ ID NO 129-SEQ ID NO 178, SEQ ID NO 129- SEQ ID NO 188, SEQ ID NO 129-SEQ ID NO 198, SEQ ID NO 129-SEQ ID NO 208, SEQ ID NO 129-SEQ ID NO 218, SEQ ID NO 129-SEQ ID NO 228, SEQ ID NO 129-SEQ ID NO 328, SEQ ID NO
- the genetic indicator can be one or more SNPs shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C, as identified by the unique SNP identifier (e.g. rs number).
- the genetic indicator can be one or more SNPs located on chromosome 6, chromosome 11, and/or chromosome 15.
- the genetic indicators are one or more SNPs selected from rs7158359, rs7129556, rsl0899387, rs934760, rsl 104959, rsl7702901, rs588217 and rs9357419.
- At least one genetic indicator can be located on chromosome 15. In another exemplary embodiment, the at least one genetic indicator can be located within a cluster or cloud of SNPs within a region of a chromosome that may be in linkage disequilibrium with one another.
- the genetic indicator(s) can include one or more SNPs within the cloud and/or all the SNPs within the cloud.
- the genetic indicator(s) can also include one or more SNPs in linkage disequilibrium.
- at least one genetic indicator is rs 17702901. At least one genetic indicator can be rsl7702901 and the DNA can be negative for rsl7702901. In another embodiment, the DNA is negative for the rs 17702901 and the pre-operative BMI of the subject can be greater than 25 kg/m .
- a method of treating metabolic or weight-related disorders includes evaluating expression of one or more genes associated with response to a metabolic procedure.
- the gene can also be shown to be differentially expressed in patients before or after bariatric surgery.
- the expression level of the gene(s) can be compared to a reference range of expression of the gene and if expression of the gene(s) is outside the reference range, a first metabolic procedure can be performed, or if expression of the gene is inside the reference range, an alternative second metabolic procedure can be performed.
- the expression level of the gene(s) can be compared to a reference range of expression of the gene and if expression of the gene(s) is outside the reference range, a first metabolic procedure can be performed, or if expression of the gene is inside the reference range, an alternative second metabolic procedure without a bariatric surgery can be performed.
- the reference range of gene expression can be determined from multiple patients having undergone a metabolic procedure, such as bariatric surgery.
- the reference range of gene expression can be an average of gene expression from multiple patients.
- the reference range of gene expression can be about +30%, +25%, +20%, +15%, +10%, or +5% of an average of gene expression from multiple patients.
- the multiple patients may be a group of patients that have experienced therapeutically significant weight loss associated with a metabolic procedure, such as bariatric surgery;
- the group of patients may have experienced lack of therapeutically significant weight loss or an adverse metabolic event associated with a metabolic procedure, such as bariatric surgery, increased risk of obesity or obesity-related co-morbid conditions.
- the gene can be at least one of SEQ ID NOs 1-128, also shown in Table 10.
- the gene can correlate with therapeutically significant weight loss associated with a metabolic procedure, such as bariatric surgery; improvement, alleviation or amelioration of one or more co- morbid conditions; and/or lack of therapeutically significant weight loss or an adverse metabolic event associated with bariatric surgery, increased risk of obesity or obesity-related co-morbid conditions in the subject.
- gene expression can correlate with therapeutically significant weight loss after a metabolic procedure, such as bariatric surgery.
- Therapeutically significant weight loss can be characterized by loss of at least 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, 80%, 85% or more of excess body weight.
- Therapeutically significant weight loss can also be characterized as at least 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, or more weight change. Alternatively or in addition to, therapeutically significant weight loss can be characterized by change of at least 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, 80%, 85% or more of body mass index.
- gene expression can correlate with improvement, alleviation or amelioration of one or more co-morbid conditions in the subject.
- Gene expression can correlate with, for example, reduced hypertension, reduced dyslipidemia, improvement or alleviation of diabetes, reduced acid reflux, alleviation of fatty liver or steatohepatitis, reduced risk of heart disease, alleviation of depression, alleviation of sleep apnea, alleviation of asthmatic symptoms, alleviation of arthritis, reduced risk of compression fractures, reduced occurrence of gallstones, lymphedema, alleviation of urinary incontinence, reduced risk of stroke, reduced risk of cancer and/or reduced risk of other metabolic syndromes.
- gene expression can correlate with lack of therapeutically significant weight loss or an adverse metabolic event associated with bariatric surgery or increased risk of obesity, or obesity-related co-morbid conditions in the subject.
- Gene expression can correlate with, for example, lack of weight loss after bariatric surgery, increased hypertension, risk of dyslipidemia, development of diabetes, acid reflux, fatty liver disease or steatohepatitis, heart disease, depression, sleep apnea, asthmatic symptoms, arthritis, compression fractures, gallstones, lymphedema, urinary incontinence, stroke, cancer and/or risk of other metabolic syndromes.
- Gene expression can be measured prior to any metabolic procedure or preoperative procedure. Gene expression can be also be measured and compared to one or more
- Gene expression can be measured at 1, 3, 6, 9, 12, 18, 24, 36, 48, 72, 84, 96, 108, 120 months post metabolic procedure or postoperative or any number of months in between. In an exemplary embodiment, gene expression is measured prior to a metabolic procedure.
- Methods and compositions for modulating expression of at least one gene associated with response to a metabolic procedure in a target tissue to treat a subject having a metabolic disorder are also disclosed.
- Methods and pharmaceutical compositions to modulate gene expression can include delivering regulatory proteins, ligands, agonists and antagonists of expression of the gene to a target tissue.
- Gene therapy can be used to modulate gene expression and can also be accomplished by methods known to those skilled in the art. For example, one approach is to use an inducible promoter to drive expression of the gene delivered. In return, the in vivo steady state level of the gene can be increased, through augmented expression of the gene.
- modulate or “modulating” are used herein to refer to an increase or or change in expression of at least one target protein or gene.
- methods and composition are disclosed to modulate gene expression by providing a full-length, a portion or fragment of, or variant of the gene or its encoded protein and expressing the full-length, a portion or fragment of, or variant of the gene or its encoded protein in the target tissue.
- full-length refers to the entire open reading frame, capable of expressing a full-length encoded protein.
- a "portion" or “fragment” of the gene or encoded protein refers to any sequence that has fewer nucleic acids or amino acids than the entire sequence of the gene or its encoded protein. Sizes of nucleic acid fragments can be 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 99% or greater of the full-length gene.
- Sizes of peptide fragments can be about 500 amino acids, about 400 amino acids, about 300 amino acids, about 200 amino acids, about 100 amino acids, about 80 amino acids, about 60 amino acids, about 40 amino acids, about 20 amino acids, about 10 amino acids or any fragment in between of the full-length protein.
- Variant can be a polynucleotide or polypeptide that differs from a reference nucleic acid or protein (i.e., SEQ ID NOs 1-128), but may retain essential properties (i.e., biological activity or conserved domains).
- a typical variant of a polynucleotide differs in nucleotide sequence from another, reference polynucleotide. Changes in the nucleotide sequence of the variant may or may not alter the amino acid sequence of a polypeptide encoded by the gene or sequence including or affected by the reference
- nucleotide changes may result in amino acid substitutions, additions, deletions, fusions and truncations in the polypeptide encoded by the reference sequence, as discussed below. Generally, differences are limited so that the sequences of the reference polypeptide and the variant are closely similar overall and, in many regions, identical.
- Variant polynucleotides can include polynucleotides having at least 70% identity, at least 80% identity, at least 90% identity, at least 95% identity, at least 96% identity, at least 97% identity, at least 98% identity or at least 99% identity to the reference nucleotide sequence of the gene.
- Variant polypeptides can include any polypeptide having an amino acid residue sequence substantially identical to a sequence specifically shown herein in which one or more residues have been conservatively substituted with a functionally similar residue, and which displays the ability to mimic essential properties of the reference protein.
- Variant polypeptides can include polypeptides having at least 70% homology, at least 80% homology, at least 90% homology, at least 95% homology, at least 96% homology, at least 97% homology, at least 98% homology or at least 99% homology to the reference protein sequence.
- the compositions can include vectors to modulate expression of the gene.
- the vector can include a full-length, a portion or fragment of, or variant of at least one of the nucleic acid sequences found in SEQ ID NOs 1-128.
- the vector can also be a viral vector, such as adenoviral vectors, adeno-associated viral vectors, retroviral vectors (including lentiviral vectors), alphaviral vectors (e.g., Sindbis vectors), and herpes virus vectors.
- the vector can also include an inducible promoter.
- the inducible promoter can be inducible through response to a regulator, such as cellular conditions, inducer molecules or stimuli.
- Regulatable promoters include inducible promoters, which are usually “off,” but which may be induced to turn “on,” and “repressible” promoters, which are usually “on,” but may be turned off. Many different regulators are known to effect control over the activity of regulatable promoters, including temperature, hormones, growth factors, cytokines, heavy metals, and regulatory proteins.
- the promoter can be inducible through exposure to an energy source. In another embodiment, the promoter can be inducible through exposure to light.
- compositions include a therapeutic agent that may be administered in a variety of forms. These include, for example, liquid, semi-solid and solid dosage forms, such as liquid solutions (e.g., injectable and infusible solutions), dispersions or suspensions, tablets, pills, powders, liposomes and suppositories.
- liquid solutions e.g., injectable and infusible solutions
- dispersions or suspensions tablets, pills, powders, liposomes and suppositories.
- An exemplary form will depend on the intended mode of delivery and therapeutic application.
- Typical therapeutic agents are in the form of injectable or infusible solutions, such as therapeutic agents similar to those used for passive immunization of humans.
- Another mode of delivery is parenteral (e.g. , intravenous, subcutaneous,
- the therapeutic agent is delivered by intravenous infusion or injection. In another embodiment, the therapeutic agent is delivered by intramuscular or subcutaneous injection. In another embodiment, the therapeutic agent is delivered perorally. In yet another embodiment, the therapeutic agent is delivered to a specific location using stereotactic delivery. In an exemplary embodiment, the therapeutic agent is formulated for delivery to the target tissue selected from the group consisting of a brain, a spinal cord, a sympathetic nervous system, a parasympathetic nervous system, an enteric nervous system, a gastrointestinal tract and a pancreas.
- compositions typically must be sterile and stable under the conditions of manufacture and storage.
- the composition can be formulated as a solution, microemulsion, dispersion, liposome, or other ordered structure suitable to high drug concentration.
- Sterile injectable solutions can be prepared by incorporating the vector in the required amount in an appropriate solvent with one or a combination of ingredients enumerated above, as required, followed by filter sterilization.
- the composition can be administered by a variety of methods known in the art. As will be appreciated by the skilled artisan, the route and/or mode of administration will vary depending upon the desired results.
- the therapeutic agent may be prepared with a carrier that will protect the agent against rapid release, such as a controlled release formulation, including implants, transdermal patches, and microencapsulated delivery systems.
- the carrier may also target delivery to at least one of a brain, a spinal cord, a sympathetic nervous system, a parasympathetic nervous system, an enteric nervous system, a gastrointestinal tract and a pancreas.
- Carriers can be made of biodegradable, biocompatible polymers, such as ethylene vinyl acetate, polyanhydrides, polyglycolic acid, collagen, polyorthoesters, and polylactic acid. Many methods for the preparation of such formulations are generally known to those skilled in the art. See, e.g., Sustained and Controlled Release Drug Delivery Systems, J.R. Robinson, ed., Marcel Dekker, Inc., New York, 1978.
- the compositions may include a "therapeutically effective amount” to modulate expression of the gene(s).
- a “therapeutically effective amount” refers to an amount effective, at dosages and for periods of time necessary, to achieve the desired therapeutic result, such as gene expression modulation.
- the therapeutically effective amount may vary according to factors such as the disease state, age, sex, and weight of the individual, and the ability of the treatment to elicit a desired response in the individual. A therapeutically effective amount is also one in which any toxic or detrimental effects of the treatment are outweighed by the therapeutically beneficial effects.
- Dosage regimens may be adjusted to provide the optimum desired response (e.g., a therapeutic or prophylactic response). For example, a single bolus may be administered, several divided doses may be administered over time or the dose may be proportionally reduced or increased as indicated by the exigencies of the therapeutic situation. It is especially
- Dosage unit form refers to physically discrete units suited as unitary dosages for the mammalian subjects to be treated; each unit containing a predetermined quantity of active compound calculated to produce the desired therapeutic effect in association with the required pharmaceutical carrier.
- the specification for the dosage unit forms of the invention are dictated by and directly dependent on (a) the unique characteristics of the active compound and the particular therapeutic or prophylactic effect to be achieved, and (b) the limitations inherent in the art of compounding such an active compound for the treatment of sensitivity in individuals.
- a determination of whether to perform a first metabolic procedure or a second metabolic procedure, which is different than the first metabolic procedure can be made. For example, after analyzing for the presence or absence of genetic indicators or measuring expression of the gene(s), a determination of whether to perform a first metabolic procedure, such as a bariatric surgery, or a second metabolic procedure excluding bariatric surgery can be made.
- Bariatric surgery includes procedures often referred to as metabolic surgery or therapy, as well as a variety of procedures performed in a subject that leads to a physiologic improvement in energy balance, nutrient utilization, or metabolic disorders.
- Surgical procedures to treat severe obesity or obesity-related conditions have included various forms of bariatric surgery, such as but not limited to, gastric bypass, Roux-en-Y gastric bypass (RYGB), biliopancreatic diversion, partial gastrectomy procedures such as vertical sleeve gastrectomy, adjustable gastric banding, duodenal switch, duodenojejunal bypass, vertical banded
- gastroplasty intragastric balloon therapy, greater curvature plication, gastric plication (including anterior and anteroposterior plication) and other forms of gastric volume reduction, Magenstrasse and Mill, ileal transposition or interposition, small bowel transposition, biliary diversion, procedures involving anastomotic connections of the gastrointestinal tract (e.g., jejunoileostomy, etc.), gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, gastric electrical stimulation, small bowel electrical stimulation, vagal electrical stimulation, vagal electrical inhibition, and variations of the procedures above as well as other methods known by those skilled in the art. Such surgical procedures have increasingly been performed laparoscopically.
- Non-surgical procedures can include, but are not limited to, pharmacological and nutritional therapies, such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.; procedures including a device, such as gastric balloon
- the first metabolic procedure is a bariatric surgery.
- the first metabolic procedure is a non-surgical procedure.
- the second metabolic procedure is a non- surgical procedure.
- the second metabolic procedure is a procedure different from the first metabolic procedure.
- gastric bypass, biliopancreatic diversion, sleeve gastrectomy and endoluminal sleeve have shown similar effects on weight loss, food intake, insulin sensitivity, glucose tolerance, insulin secretion, and endogenous glucose production.
- bariatric surgical procedures have also shown similar effects on the gastrointestinal endocrine system.
- Some non-surgical examples of alternative metabolic procedures to bariatric surgery can include, but are not limited to, administering pharmacological and nutritional therapies, such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.; providing an alternative medical device based therapy, such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.; and/or the activation of brown adipose tissue.
- pharmacological and nutritional therapies such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.
- an alternative medical device based therapy such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.
- the activation of brown adipose tissue See US Pat. Pub. No. 2011/0263490 entitled "Diagnostic Methods And Combination Therapies Involving MC4R" filed December 29.
- assessment of the efficacy of the treatment can be made.
- evaluating the efficacy of the treatment can influence whether additional treatments need to be performed or if the treatment alone is sufficient to attain the desired weight loss and other clinical results.
- Hormone and neuropeptide therapy can also be used to regulate or suppress appetite, increase body energy expenditure, and/ or decrease fat mass accumulation (McMinn, J. E., Baskin, D. G. & Schwartz, M. W., Obes. Rev. 2000; 1:37-46; Drazen, D. L. & Woods, S. C, Curr. Opin. Clin. Nutr. Metab. Care 2003; 6:621-629).
- BAT activation can occur either directly or transcutaneously. Either can stimulate the sympathetic nervous system to physiologically activate BAT. Whether BAT is activated directly and/or transcutaneously, target areas for BAT stimulation can include areas in the vicinity of BAT depots, e.g., the nape of the neck, over the scapula, alongside the spinal cord, and around the kidneys. Any BAT depot can be selected for activation. In the course of treating a patient, BAT nerves can be stimulated at any one or more BAT depots and can be stimulated
- Sequential stimulation of BAT can help encourage more and/or faster energy expenditure. Sequential stimulation of BAT can help prevent the "burning out" of target nerves and can help stimulate the creation of new BAT cells. Sequential nerve stimulation can include stimulating the same BAT depot more than once, with at least one other BAT depot being activated before activating a previously activated BAT depot.
- direct activation of BAT can include implanting a device below the skin surface proximate to a BAT depot, e.g., within a BAT depot, and activating the device to deliver an electrical signal to the nerves innervating the BAT depot and/or to brown adipocytes directly.
- BAT itself is densely innervated, with each brown adipocyte being associated with its own nerve ending, which suggests that stimulating the BAT directly can target many if not all brown adipocytes and depolarize the nerves, leading to activation of BAT.
- the sympathetic nerves that innervate BAT can be accessed directly through standard surgical techniques, as will be appreciated by a person skilled in the art.
- the electrical signal can be configured in a variety of ways.
- the stimulation "on" time amplitude can be higher for shorter periods and increased or decreased for longer periods of application.
- the electrical signal can have any "geometry" of the applied voltage, e.g., square waves, ramp waves, sine waves, triangular waves, and waveforms that contain multiple geometries.
- a transcutaneous device can be used to transcutaneously activate BAT through a variety of sizes, shapes, and configurations. Generally, the device can be configured to generate and/or deliver an electrical signal to tissue at predetermined intervals, in response to a manual trigger by the patient or other human, in response to a predetermined trigger event, or any combination thereof.
- the transcutaneous device can include an electrical stimulation patch configured to be applied to an external skin surface and to deliver an electrical signal to tissue below the skin surface, e.g., to underlying BAT.
- PCT/US11/66399 entitled “Methods And Devices For Activating Brown Adipose Tissue With Targeted Substance Delivery” filed December 21, 2011, PCT Pat. App. No. PCT/US 11/66358 entitled “Brown Adipocyte Modification” filed December 21, 2011, PCT Pat. App. No.
- PCT/US 11/66409 entitled “Methods And Devices For Activating Brown Adipose Tissue With Light” filed December 21, 2011, and PCT Pat. App. No. PCT/US 11/66415 entitled “Methods And Devices For Activating Brown Adipose Tissue With Cooling” filed December 21, 2011.
- the electrical signal can be configured in a variety of ways.
- the stimulation "on" time amplitude can be higher for shorter periods and increased or decreased for longer periods of application.
- the electrical signal can have any "geometry" of the applied voltage, e.g., square waves, ramp waves, sine waves, triangular waves, and waveforms that contain multiple geometries.
- a transcutaneous device can be used to transcutaneously activate BAT through a variety of sizes, shapes, and configurations. Generally, the device can be configured to generate and/or deliver an electrical signal to tissue at predetermined intervals, in response to a manual trigger by the patient or other human, in response to a predetermined trigger event, or any combination thereof.
- the transcutaneous device can include an electrical stimulation patch configured to be applied to an external skin surface and to deliver an electrical signal to tissue below the skin surface, e.g., to underlying BAT.
- Indicators that predict outcomes after a metabolic procedure can also be measured and used in the methods disclosed herein.
- Such indicators can include genetic indicators and/or clinical measurements obtained from the patient. Examples of genetic indicators are described in more detail in U.S. Prov. Pat. App. No. 61/704,434 entitled “Clinical Predictors of Weight Loss” filed on September 21, 2012, Atty. Dkt. No. 100873-572 (END7094USPSP), which is incorporated herein by reference in its entirety.
- Examples of clinical measurements can include, but are not limited to, pre-operative BMI, a glucose tolerance, bile acid profile, and body composition/fat distribution of the subject.
- Pre-operative BMI can be greater than 23 kg/m in non-Asians or greater than 21 kg/m in Asians. Individuals at a lower than "overweight" BMI may also be at risk of at least one weight-related comorbidity and therefore be applicable subjects to be treated or assessed by methods of this invention (e.g., Caucasians having a BMI of greater than 23 and Asians, a BMI of greater than 21). In some embodiments, pre-operative BMI can be greater than 25 kg/m in non-Asians or greater than 23 kg/m in Asians.
- Additional non-limiting examples of indicators include, but are not limited to height, weight, gender, age, medical history and/or status, ethnicity, medical prescription history and/or status, types of previously received medical treatments for obesity (e.g., medications, BAT stimulation, gastric banding, gastric bypass, sleeve gastrectomy, etc), types of medical treatments previously received for health issues other than obesity (e.g., medications, surgical treatments, and non- surgical treatments), insurance information, diet information for the patient, and psychological history of the patient.
- types of previously received medical treatments for obesity e.g., medications, BAT stimulation, gastric banding, gastric bypass, sleeve gastrectomy, etc
- types of medical treatments previously received for health issues other than obesity e.g., medications, surgical treatments, and non- surgical treatments
- insurance information e.g., diet information for the patient, and psychological history of the patient.
- Various systems and methods are provided for predicting metabolic therapy, e.g., metabolic and bariatric surgery, outcomes, i.e., a composite predictive model.
- the systems and methods can also provide predictions for non-surgical metabolic and bariatric treatments.
- a user e.g., a patient, a medical professional involved with treating a patient, a medical student, a hospital administrator, a health insurance administrator, etc.
- a user can receive predictive outcomes of multiple metabolic therapies that could be performed on a patient.
- the collection of therapies for the treatment of obesity and metabolic disease e.g., diet and exercise,
- a user can electronically access a metabolic therapy outcome prediction system, e.g., using one or more web pages.
- the system can provide predictive outcomes of one or more different metabolic therapies, such as bariatric surgeries, for the patient based on data gathered from the user and on historical data regarding outcomes of the different bariatric surgeries.
- the system can additionally provide predictive outcomes for not having any treatment and/or a comparison of the predictive outcomes of the one or more different bariatric surgeries to the predictive outcomes for not having any treatment or for having non-surgical treatment.
- the predictive outcomes provided by the system can include a potential clinical metabolic outcome of each of the different bariatric surgeries, e.g., a predicted amount of weight loss, a predicted amount of body mass index (BMI) reduction, an improvement in a health condition associated with a metabolic disease, an associated risk of complications from the treatment, and/or an associated cost of the surgery and post-operative care.
- a potential clinical metabolic outcome of each of the different bariatric surgeries e.g., a predicted amount of weight loss, a predicted amount of body mass index (BMI) reduction, an improvement in a health condition associated with a metabolic disease, an associated risk of complications from the treatment, and/or an associated cost of the surgery and post-operative care.
- BMI body mass index
- the predictive outcomes can be based on a plurality of patient-specific characteristics, e.g., age, weight, height, BMI, ethnicity, medical prescription history and/or status, genetic data (e.g., a genetic indicator), gene expression profiles (expression of one or more genes, expression over a time period and/or in different tissues), types of previously received medical treatments for obesity (e.g., gastric banding, gastric bypass, sleeve gastrectomy, etc), medical history and/or status, gender, etc.
- the predictive outcomes can also be based on historic results of the different types of bariatric surgeries on other patients.
- the predictive outcomes can thus be based at least in part on data specific to the patient and not just on historical data, e.g., data gathered by the user from previous personal experience, friends or colleagues, journal articles, internet research, clinical data, etc.
- the outputs can thus be personalized to the patient.
- the system can help the user be more informed about which of the bariatric surgeries would be most effective if performed on the patient, help specifically compare and contrast the different bariatric surgeries, and help the user decide which of the different bariatric surgeries, if any, to pursue for the patient.
- the system can therefore help maximize effectiveness of treatment for the patient by allowing a most effective option to be identified and pursued by the patient and/or by medical practitioner(s) treating the patient.
- the system can also help inform the user about bariatric surgery options that they might not have been aware of at all, e.g., new procedures, and/or deepen understanding of bariatric surgery procedures previously known to the user.
- the system can be configured to allow the user to save the predictive outcomes, which can then be accessed at a later date/time by the user and/or one or more other users, e.g., the user's surgeon, the user's endocrinologist, the user's primary care physician, or other healthcare providers, etc., to which the user grants access to the saved data.
- Output results can be reported in multiple ways, either individually or simultaneously via the system.
- output results can be reported in parameters such as, but are not limited to, target weight loss in pounds or kilograms, target weight, percent excess body weight loss, percent weight change, percent change in BMI.
- output results can be reported as continuous or at various cutoff points ranging from 1-100%.
- An example of various cutoff may include achieving at least or at most 50% excess weight loss.
- Another example of various cutoff may include achieving at least or at most 70% excess weight loss.
- the output results can be reported as results obtained at various timepoints post metabolic procedure such as bariatric surgery or alternative metabolic procedure without bariatric surgery.
- Timepoints can include 1, 3, 6, 9, 12, 18, 24, 36, 48, 72, 84, 96, 108, 120 months post treatment or any number of months in between.
- the output results can be reported as nadir weight.
- Nadir weight as used herein is defined as the lowest weight achieved at least 10 months after surgery without coexisting debilitating illness, with or without use of weight lowering medications.
- the input parameters can be analyzed via the interface in a model algorithm.
- the algorithm can apply univariate analyses, multivariable regression analyses, advanced regression analyses, and other data mining techniques on multiple data sets to build, train and prospectively model predicted results after metabolic procedure such as bariatric surgery or alternative metabolic procedure without bariatric surgery.
- the interface can also be used to output varying levels of confidence of the prediction on the results after metabolic procedure such as bariatric surgery or alternative metabolic procedure without bariatric surgery.
- Such examples can include the predicted result based on variable changes in weight, e.g., 20% chance of 40 lb change in weight, 40% chance of 201b change in weight, etc.
- the output can further include predictions based on complications associated with a metabolic procedure such as bariatric surgery or an alternative metabolic procedure without bariatric surgery.
- the output results can be collected and used by patients, primary care providers, and/or other referring physicians or other healthcare providers.
- the information can be provided in the patient's home, during a health care provider seminar, during a physician's office visit, and/or prior to treatment.
- the interface can be accessed through various routes.
- the interface can be accessed via the internet to record and model the patient information.
- the interface can be accessed via a mobile device or "app," software application designed specifically for mobile or handheld devices.
- the interface can be accessed via application software that can be installed on a computer or other device.
- the system can optionally provide educational information regarding each of the different bariatric surgeries and/or other types of information related to bariatric surgery such as estimated patient monetary cost (based on one or more factors such as the patient' s insurance carrier, similar procedures performed in the patient' s geographic location, etc.), estimated insurance reimbursement (based on one or more factors such as the patient's insurance carrier, similar procedures performed in the patient's geographic location, etc.), estimated length of post-surgery hospital stay (based on one or more factors such as similar procedures performed in the patient's geographic location, the patient's age, the patient's other health conditions or disorders, etc.).
- estimated patient monetary cost based on one or more factors such as the patient' s insurance carrier, similar procedures performed in the patient' s geographic location, etc.
- estimated insurance reimbursement based on one or more factors such as the patient's insurance carrier, similar procedures performed in the patient's geographic location, etc.
- estimated length of post-surgery hospital stay based on one or more factors such as similar procedures performed in the patient's
- the system can therefore help the user be more fully informed about the various risks and benefits of the various bariatric surgeries before deciding which of the bariatric surgeries to pursue, if any. Applying similar modeling techniques, personalized predictions can be provided for use of one or more of the preceding educational and/or other information.
- Study Population To identify genetic factors contributing to weight loss after RYGB, an exploratory genome- wide association study of individuals of European descent undergoing RYGB was performed. The study was approved by and performed in accordance with the guidelines of the Human Studies Committee at the Massachusetts General Hospital. From February 2000 until April 2007, consent was obtained from 1018 (97%) of MGH Weight Center patients undergoing RYGB to collect and extract DNA from tissue samples removed at the time of surgery. Intraoperative liver, subcutaneous fat, omental fat, and stomach tissues were collected in RNAlater (Amnion/ Applied Biosystems) and stored at -80°C. Operations were either open (41%) or laparoscopic (59%) RYGB.
- the stomach was partitioned but not divided, and for the laparoscopic procedure the pouch was partitioned and divided from the remaining stomach. Otherwise, the techniques were the same, with an approximately 30 ml pouch, a 100-120 cm Roux (alimentary) limb fashioned in a retrocolic, retrogastric configuration, and a pancreaticobiliary limb extending approximately 75 cm beyond the ligament of Treitz.
- Surgical procedures For the open procedure, the stomach was partitioned but not divided, and for laparoscopic procedure the pouch was partitioned and divided from the remaining stomach. Otherwise, the techniques were the same, with an -30 ml pouch and a 100- 120 cm Roux limb fashioned in a retrocolic, retrogastric configuration, and the pancreaticobiliary limb extending -75 cm from the ligament of Treitz.
- first-degree relative pairs defined as pairs of individuals who share approximately 50% of their genetic variation, six second-degree relative pairs (-25% of genetic variation shared) and four third-degree relative pairs (-12.5% of genetic variation shared).
- An additional eight patients who were genetically related to established first-degree pairs were excluded, leading to a final sample of 848 (83.3%).
- the samples were matched on genetically identified race, randomly paired 794 unrelated individuals from the cohort, and compared for the similarity in their weight loss outcomes after surgery. Also identified were 20 cohabitating individuals by review of the medical records of all patients who had undergone RYGB at this center. No cohabitating individuals were genetically related.
- EBWL body weight lost
- Genotyping and Data Cleaning of Study Population Samples were shipped to the Rosetta Inpharmatics Gene Expression Laboratory (Seattle, WA) where genomic DNA was extracted from liver samples. Nine hundred fifty samples were successfully genotyped using the Illumina HumanHap 650 Y BeadChip array (Illumina Corp, San Diego, CA). Data were converted to PLINK format (Hatoum, I. J., Stein, H. K., Merrifield, B. F. & Kaplan, L. M., Capacity For Physical Activity Predicts Weight Loss After Roux-En-Y Gastric Bypass, Obesity (Silver Spring) 17, 92-99 (2009)), and all genetic analyses were performed using this software.
- IBD identity-by-descent
- oligonucleotide microarrays from Agilent Technologies (Santa Clara, CA, USA). A detailed description of the normalization and data cleaning methods has been described previously. (Shin, A. C, Zheng, H., Pistell, P. J. & Berthoud, H.-R., Roux-En-Y Gastric Bypass Surgery Changes Food Reward In Rats, Int J Obes (Lond) 35, 642-651 (2011).) 707, 870, and 916 samples were profiled from liver, subcutaneous fat, and omental fat, respectively.
- Replication Cohort From May 2007 until October 2009, we obtained consent from 369 Caucasian MGH Weight Center patients undergoing RYGB to collect and extract DNA from tissue samples removed at the time of surgery. Intraoperative liver tissue samples were collected in RNAlater (Amnion/ Applied Biosystems) and stored at -80°. Operations were as described for the GWAS cohort. Clinical traits were extracted from the electronic medical records, as described for the GWAS cohort.
- Genotyping and Data Cleaning of Replication Cohort Samples were shipped to the Eli and Edythe Broad Institute (Cambridge, MA) where genomic DNA was extracted from liver samples. Three hundred sixty-nine samples were successfully genotyped using Sequenom MassARRAY (Sequenom Inc., San Diego, CA). Of these, 327 had a recorded weight nadir value, were not on weight-lowering medications after surgery, did not have cancer or other severe illness, and were thus included in the final data set.
- mice were performed in compliance with and were approved by the Institutional Animal Care and Use Committee of the Massachusetts General Hospital.
- Male, diet-induced obese C57BL/6 mice on a high fat diet from weaning (Jackson Laboratories, Bar Harbor, ME) were randomized to RYGB, sham operation with post-operative ad libitum food intake, or sham operation with food restriction to match the weights of the RYGB mice weekly.
- the stomach was divided into a gastric pouch and distal stomach using a vascular clip (Ethicon Endo-Surgery, Inc., Cincinnati, OH).
- the length of the intestine was 6 cm, approximating the 12-15% instestinal bypass used in the human operation.
- the alimentary limb was then secured to the gastric fundus by a gastrojejunal anastamosis.
- Sham operations consisted of a laparotomy and repair. Mice were maintained on a high-fat diet (D12492 diet; Research Diets, New Brunswick, NJ) except during the 7-14 days after surgery, when all mice were maintained on a postoperative protocol that progressed from water only to liquid diet to solid diet. Animals were individually housed in a 12-hour light, 12-hour dark cycle under controlled temperature and humidity conditions.
- Tissue Samples Intraoperative liver, subcutaneous fat, omental fat, and stomach tissues were collected in RNAlater (Amnion/ Applied Biosystems) and stored at -80 °C.
- oligonucleotide microarrays from Agilent Technologies (Santa Clara, CA). A detailed description of the normalization and data cleaning methods has been described previously. Successful profiling of 707, 870, and 916 samples from liver, subcutaneous fat, and omental fat, respectively, was performed.
- patients in this cohort had an average BMI of 50.2+8.6kg/m2, an average age of 44.7+11.3 yr, and were 74.8% female and 86% Caucasian. These characteristics were similar among the different groups studied (see Table 1).
- Table 1 Patient demographics at baseline by type of relationship.
- the ICC represents the portion of total variation in outcome explained by the pair relationship.
- preoperative BMI is strongly associated with postoperative percent EBWL, we additionally matched the unrelated controls based on 5-kg/m2-wide BMI groups to mimic the distribution of differences in preoperative BMI between first-degree relatives.
- first-degree relatives have weight loss outcomes after surgery that closely and significantly resemble each other, a characteristic not shared by environmentally related (cohabitating) controls or randomly paired individuals. Similar results were seen when men and women were examined separately (data not shown).
- Study Population Participants were recruited from the population of patients undergoing RYGB at a single academic center that is part of a larger 13-hospital network in the Boston metropolitan area. From February 2000 until April 2007, we obtained consent from 1018 (97%) of the patients undergoing RYGB at this center. Operations included both open and laparoscopic RYGB performed by one of two surgeons using the same operative techniques; the surgical methods have been described previously. This study was approved by the institutional review board of the Massachusetts General Hospital.
- Endpoint and Covariate Assessment Demographic and clinical information was extracted from the medical record.
- We indentified a patient' s weight nadir defined as the lowest weight achieved at least 10 months after surgery without coexisting debilitating illness or use of weight-lowering medications.
- One-year weight was defined as the weight closest to 12 months from surgery, within the range of 10-14 months after surgery.
- Post- operative weights were available for 848 patients (83.3%).
- Diabetes diagnosis was extracted from patient charts and defined as the documentation of diabetes, a fasting glucose measurement > 126 mg/dL, or the use of diabetes medication (insulin or metformin).
- Weight loss was characterized at one year and at weight nadir using seven different metrics (Table 2). Residuals were calculated by regressing postoperative BMI (the dependent variable) on preoperative BMI (the independent variable) and outputting the residuals from this model. Because residuals derived from regressing postoperative BMI on preoperative BMI represent, by definition, postoperative BMI independent of preoperative BMI, these residuals were used as the benchmark of independence from preoperative BMI. Weight loss characterized by number of pounds lost was calculated by subtracting the patient's final weight from his or her baseline weight. As BMI is a function of weight and height, and height is almost always stable over the course of a weight loss study, BMI and pounds lost are closely similar methods for measuring weight loss.
- Percent weight change was calculated by dividing the absolute pounds lost by the patient's initial weight, and is statistically interchangeable with percent BMI change.
- Percent EBWL was calculated by dividing the difference between initial BMI and final BMI by the difference between initial BMI and a "normal" BMI.
- a BMI of 25 kg/m is commonly used to represent the target, or upper limit of a "normal” BMI, but other standards, including race- specific BMI standards or other "ideal weights" according to the Metropolitan Life Insurance Company (MLIC) life tables, may also be used to represent "normal.”
- MLIC Metropolitan Life Insurance Company
- Statistical Analyses Patients were divided into seven preoperative BMI (pBMI) groups (35-39.9, 40-44.9, 45-49.9, 50-54.9, 55-59.9, 60-64.9, 65+). Means for each weight loss metric were calculated for each pBMI group, and linear trends across the groups were assessed using a test for trend of the median value within each group. Correlations between pBMI and each continuous metric were assessed using Spearman correlations, and r measures were derived from linear regressions. All analyses were performed using SAS statistical software (SAS Institute, Cary, NC).
- Table 3 Weight loss parameterizations by preoperative BMI group.
- Cohort 1 To identify genetic factors contributing to weight loss after RYGB, an exploratory genome-wide association study of Caucasian individuals undergoing RYGB was performed. From February 2000 until April 2007, consent was obtained from 1018 (97%) of Massachusetts General Hospital (MGH) Weight Center patients undergoing RYGB to collect and extract DNA from tissue samples removed at the time of surgery. Cohort 1 may also be described herein as the original cohort, the GWAS cohort, the training cohort, or the training set.
- Genotyping and Data Cleaning of Cohort 1 Samples were shipped to Rosetta Inpharmatics Gene Expression Laboratory (Seattle, WA) where genomic DNA was extracted from liver samples. Nine hundred fifty samples were successfully genotyped using the Illumina HumanHap 650Y BeadChip array (Illumina Corp, San Diego, CA). Data were converted to PLINK format (Purcell, S. et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 81, 559-575 (2007)) and all genetic analyses were performed using this software. Using identity-by-descent (IBD) coefficients for all pairs of individuals, 36 related individuals were identified, defined as an IBD coefficient >0.125. One person per family was included for analysis, based on completeness of phenotypic and genetic information.
- IBD identity-by-descent
- Cohort 2 From May 2007 until October 2009, consent was obtained from 369 Caucasian MGH Weight Center patients undergoing RYGB to collect and extract DNA from tissue samples removed at the time of surgery. Intraoperative liver was collected in RNAlater (Amion/ Applied Biosystems) and stored at -80°. Operations were as described for the Cohort 1. Clinical traits were extracted from the electronic medical records, as described for the GWAS cohort. Cohort 2 may also be described herein as the replication cohort, the test cohort, or the test set.
- Genotyping and Data Cleaning of Cohort 2 Samples were shipped to the Eli and Edyth Broad Institute (Cambridge, MA) where genomic DNA was extracted from liver samples. Three hundred sixty-nine samples were successfully genotyped using Sequenom MassARRAY (Sequenom Inc., San Diego, CA). Of these, 327 had a weight nadir value, were not on weight- lowering medications after surgery, did not have cancer or other severe illness, and were thus included in the final data set.
- Tissue Samples Intraoperative liver, subcutaneous fat, omental fat, and stomach tissues were collected in RNAlater (Amion/ Applied Biosystems) and stored at -80 °C.
- oligonucleotide microarrays from Agilent Technologies (Santa Clara, CA, USA). A detailed description of the normalization and data cleaning methods has been described previously. 4 Successful profiling of 707, 870, and 916 samples from liver, subcutaneous fat, and omental fat, respectively, was performed.
- mice were maintained on a high-fat diet (D 12492 diet; Research Diets, New Brunswick, NJ) except during the 7-14 days after surgery, when all mice were maintained on a postoperative protocol that progressed from water only to liquid diet to solid diet. Animals were individually housed in a 12 hour light, 12 hour dark cycle under controlled temperature and humidity.
- D 12492 diet Research Diets, New Brunswick, NJ
- mice were sacrificed in a carbon monoxide chamber followed by cervical dislocation. Tissues were harvested immediately, flash frozen, and stored at -80°. Samples were shipped to Rosetta Inpharmatics Gene Expression Laboratory (Seattle, WA) where mRNA was extracted and converted to cDNA. Quantitative PCR was performed on genes of interest (to be expanded with primer and QC information as it becomes available).
- SNPs Single nucleotide polymorphisms in this cohort were genotyped using the Illumina HumanHap 650Y array. After implementing stringent quality control measures, 524,284 SNPs were available for analysis. To increase the coverage of genetic variants additional missing genotypes were imputed and applied to these imputed SNPs. The same quality control measures were performed on the genotyped SNPs. A total of 1,943,373 genetic markers were analyzed.
- Figure 12 shows the percent change of weight nadir measured in an independent cohort of 327 Caucasian RYGB patients (Cohort 2).
- One hundred and three marginally significant (P ⁇ 5 x 10 "5 ) SNPs were identified ( Figure 13; Table 5), representing 26 independent loci (pairwise r ⁇ 0.5) from Cohort 1.
- the top SNP per region was carried forward for validation in Cohort 2, 327 Caucasian RYGB patients (Table 5).
- Table 5 Association results for 103 SNPs with p ⁇ 5.0x10 for nadir WL in the Cohort 1.
- the top SNP per region underwent validation in Cohort 2. Twenty-three mutations were determined using Sequenom MassARRAY, see Figure 14. The association between SNPs and percent total weight loss (%WL) at the lowest weight (weight nadir) after RYGB were analyzed using linear regression models. A genomic control inflation factor of 1.00 was observed, indicating there was no inflation of test statistics due to population stratification.
- Table 6 SNPs Associated with WC at Nadir.
- Patients with at least one copy of the MA were 2.54 times more likely to fall below 30% WL, than patients with no copies of the MA (P ⁇ 0.001)(left shaded area in Figure 18).
- no patients with this polymorphism lost more than 50% of his or her weight (corresponding to the upper 10% of the weight loss distribution) (right shaded area in Figure 18).
- Variables for the genetic model included all of the variables in the clinical model with the addition of the following genetic variables: rsl 108723, rsl 1739371, rsl 1942914, rsl2425125, rsl7710780, rs2383289, rs3734399, rs4325727, rs4603757, rs6737079, rs6911751, rs6925786, rs9474779. Similar to the model with one SNP, the multi-SNP model was constructed by selecting multiple SNPs that met specific p-value criteria and then using backward and stepwise regression. For each model, coefficients for each variable were determined using the training population (Cohort 1).
- the AUROC in the test set (Cohort 2) was also improved (0.795) over the respective AUROC scores based on clinical data alone, verifying that inclusion of multiple SNPs (rsl 108723, rsl 1739371, rsl 1942914, rsl2425125, rsl7710780, rs2383289, rs3734399, rs4325727, rs4603757, rs6737079, rs6911751, rs6925786, rs9474779) significantly improves weight loss predictions.
- SNPs rsl 108723, rsl 1739371, rsl 1942914, rsl2425125, rsl7710780, rs2383289, rs3734399, rs4325727, rs4603757, rs6737079, rs6911751, rs6925786, rs9474779
- nphsl nephrosis 1 congenital, Finnish type AK141081
- Table 12 Top 50 expression transcripts associated with rsl7702901.
- SNP rsl7702901 at 15q26.1 was significantly associated with percent weight loss after Roux-en-Y gastric bypass (RYGB)
- RYGB Roux-en-Y gastric bypass
- rsl7702901 its association with the expression level of -44,000 transcripts in liver, omental fat and subcutaneous fat was examined. No multiple test- corrected, significant associations were detected between rs 17702901 and preoperative expression of any transcripts, including the two nearest genes - ST8SIA2, located -6.7 kilobases (kb) downstream of rsl7702901 and SLC03A1, ⁇ 223kb upstream of this SNP (Table 12).
- Table 13 SNP association results from the genome- wide association analysis.
- Absolute value of the distance from the start or stop site of the closest gene indicates that the SNP is located within the gene.
- Table 14 Top 50 association results for gene-based association tests.
- CNNM4 2 34 0.0028 rsl7119562 0.003587
- OPALIN 10 135 0.00298 rsl 1188734 0.0001968 KLK11 19 104 0.00301 rs 1701948 0.0005329
- Table 15 Top 50 expression transcripts associated with rsl7702901.
- Table 16 Association results for SNPs previously identified as associated with obesity.
- rs2890652 LRP1B 2 142676401 1.07 0.2291 rs4929949 RPL27A, TUB 11 8561169 -1.146 0.1109 rs2112347 FLJ35779, HMGCR 5 75050998 -0.252 0.6206 -1.337 0.08203 0.5839 0.1684 rsl558902 FTO 16 52361075 -0.1002 0.8373 0.7299 0.322
- Table 17 Association results for SNPs previously identified as associated with diabetes.
Landscapes
- Chemical & Material Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Health & Medical Sciences (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Organic Chemistry (AREA)
- Genetics & Genomics (AREA)
- Zoology (AREA)
- Analytical Chemistry (AREA)
- Wood Science & Technology (AREA)
- Engineering & Computer Science (AREA)
- Microbiology (AREA)
- Biochemistry (AREA)
- Biotechnology (AREA)
- Molecular Biology (AREA)
- Biophysics (AREA)
- Physics & Mathematics (AREA)
- Pathology (AREA)
- Immunology (AREA)
- Bioinformatics & Cheminformatics (AREA)
- General Engineering & Computer Science (AREA)
- General Health & Medical Sciences (AREA)
- Measuring Or Testing Involving Enzymes Or Micro-Organisms (AREA)
- Pharmaceuticals Containing Other Organic And Inorganic Compounds (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
Description
CLINICAL PREDICTORS OF WEIGHT LOSS
CROSS REFERENCE TO RELATED APPLICATIONS
[0001] The present invention claims priority to U.S. Patent Application Serial No.
13/828,809, filed on March 14, 2013, which claims priority to U.S. Provisional Application Serial No. 61/704,434, filed on September 21, 2012, to U.S. Provisional Application Serial No. 61/704,077, filed on September 21, 2012, and to U.S. Provisional Application Serial No.
61/740,678, filed on December 21, 2012, all of which are hereby incorporated by reference in their entirety. In the case of any inconsistency, the instant application supersedes the prior applications.
SEQUENCE LISTING
[0002] The instant application contains a Sequence Listing, which has been submitted in ASCII format via EFS-Web and is hereby incorporated by reference in its entirety. Said ASCII copy, created on March 14, 2013 is named 100873-629_SL.txt and is 1,318,653 bytes in size.
FIELD OF THE INVENTION
[0003] The present invention relates to genetic predictors for treatment of metabolic disorders and diseases, such as obesity.
BACKGROUND OF THE INVENTION
[0004] It is estimated that 66% of adults in the United States are overweight, including 32% who have obesity. The myriad metabolic, inflammatory, degenerative, cognitive, and neoplastic sequealae of obesity together cost more than $168 billion annually and account for nearly 10% of all healthcare expenditures in the United States.
[0005] Behavioral and pharmacotherapeutic treatments for severe obesity have been met with limited long-term success. In contrast, metabolic and bariatric operations such as Roux-en-Y gastric bypass (RYGB) lead to significant and sustained weight loss. Because of its excellent clinical outcomes, RYGB is currently the most commonly used surgical therapy for obesity. Metabolic and bariatric surgical procedures are increasingly being performed laparoscopically.
Reduced postoperative recovery time, markedly decreased post operative pain and wound infection, and improved cosmetic outcome are well established benefits of laparoscopic surgery, derived mainly from the ability of laparoscopic surgeons to perform an operation utilizing smaller incisions of the body cavity wall.
[0006] Despite the various metabolic and bariatric surgical procedures each providing chances for weight loss and associated improvements in comorbid conditions, there is wide variability in outcomes (e.g., weight loss, improvements in diabetes and other comorbidities of obesity, adverse sequelae, etc.) among individual patients who receive such surgeries. Several clinical, demographic, psychological, and surgical predictors of weight loss have been reported, but these factors explain only a small fraction of the variation in weight loss after surgery. The
identification of novel predictors of outcomes after metabolic and bariatric surgical procedures can both provide insight into the biological mechanisms of action of these procedures, as well as provide predictive markers that may be used to stratify those patients who may respond best to surgery or alternative treatments. Additionally, because numerous factors can affect a patient's outcomes following metabolic and bariatric surgery, and because some factors may be more relevant for some patients more than others depending on an individual's overall health and other biological characteristics, it can be difficult for medical professionals to consider and balance these factors to arrive at an accurate prediction as to how the surgery will affect a particular patient. It can be even more difficult, and likely impossible, for non-medical professionals, e.g., patients, to consider and balance such factors.
[0007] Accordingly, there remains a need for improved systems and methods for predicting metabolic and bariatric surgery outcomes and treatments that incorporate these systems and methods.
SUMMARY OF THE INVENTION
[0008] The present invention generally provides methods and compositions for treating a subject having a metabolic disorder, e.g., obesity and weight related disorders. In one embodiment, a method of treating a subject having a metabolic disorder can include the steps of (a) obtaining a biological sample from the subject; (b) evaluating the sample for the presence or absence of at least one genetic indicator, and (c) performing a first metabolic procedure on the
subject, if the at least one genetic indicator is/are absent, or (d) if the at least one genetic indicator is/are present, performing a second metabolic procedure, wherein the first metabolic procedure is different from a second metabolic procedure. A genetic indicator can include a genetic variation, such as a single nucleotide polymorphism, or a level of gene expression within or without a reference range.
[0009] In one embodiment, a method of treating a weight-related disorder in a subject can include (a) obtaining a sample comprising nucleic acids from the subject; (b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; and (c) based on if the genetic indicator(s) is absent in (b), performing a first metabolic procedure, or if the genetic indicator(s) is present in (b), performing a second metabolic procedure wherein the second metabolic procedure is different from the first metabolic procedure. The first and second metabolic procedures can be surgical, such as bariatric surgery, or non- surgical. In some aspects, the biological sample includes nucleic acids and evaluating the sample includes evaluating the nucleic acids for the presence or absence of at least one genetic indicator. In an exemplary embodiment, the nucleic acids in the samples can be deoxyribonucleic acids (DNA) or ribonucleic acids (RNA). The nucleic acids can also be positive or negative for the genetic indicators. In some instances, the genetic indicators can be at least one single nucleotide polymorphism (SNP) selected from Appendix A (i.e., SEQ ID NOs 129-837 (SNPs identified as statistically significant for percent weight loss)), Appendix B (additional SNPs identified as statistically significant for percent weight loss) and/or Appendix C (SNPs identified as statistically significant for percent excess body weight loss). The absence or presence of the SNP can correlate with therapeutically effective weight loss of at least 20% weight change after a first metabolic procedure or a second metabolic procedure in the subject. In an exemplary embodiment, the absence or presence of the SNP can correlate with therapeutically effective weight loss of at least 20% weight change after a first metabolic procedure or a second metabolic procedure without a bariatric surgery in the subject.
[0010] In another embodiment, additional clinical measurements can be obtained from the subject. The additional clinical measurements can be obtained prior to evaluating the nucleic acids in the sample or prior to performing a first metabolic procedure or a second metabolic procedure without a bariatric surgery. In an exemplary embodiment, the additional clinical
measurements can be obtained prior to evaluating the nucleic acids in the sample or prior to performing a first metabolic procedure or a second metabolic procedure without a bariatric surgery. The clinical measurement can include at least one of a pre-operative body mass index (BMI), anthropometric assessment, body composition, fat distribution, and energy expenditure assessment of the subject, a glucose tolerance or other marker of metabolic homeostasis, a bile acid profile, and a measurement of a biomarker obtained from a fluid, tissue, feces, or other sample obtained from the subject. In an exemplary embodiment, the clinical measurement is a pre-operative body mass index (BMI) of the subject. The clinical measurements can also include weight, gender, age, medical history, weight history, comorbid disease, physical activity, and/or status, BMI, ethnicity, prescription history and/or status, and types and outcomes of treatments previously tried (such as medications or other surgical and non-surgical treatments, etc). In another exemplary embodiment, the nucleic acids can be negative for the genetic indicators and the clinical measurement is a pre-operative BMI of the subject, where the BMI is greater than 25 kg/m2.
[0011] In one embodiment, a method of treating a subject having a metabolic disorder can include the steps of (a) obtaining a biological sample from the subject; (b) evaluating expression of at least one gene in the sample, wherein the gene is differentially expressed after bariatric surgery or whose expression correlates with weight loss after a metabolic procedure; and (c) comparing the expression level of the gene(s) evaluated in (b) to a reference range, if expression of the gene(s) is outside the reference range, performing a first metabolic procedure on the subject, or if expression of the gene is inside the reference range, performing a second metabolic procedure on the subject. The first and second metabolic procedures can be surgical, such as bariatric surgery, or non-surgical.
[0012] In one embodiment, the gene(s) can be selected from SEQ ID NOs 1-128. The gene(s) can correlate with therapeutically significant weight loss associated with a metabolic procedure, such as bariatric surgery; improvement, alleviation or amelioration of one or more co- morbid conditions; absence of an adverse metabolic effect; and/or lack of therapeutically significant weight loss, lask of improvement, alleviation or amelioration of one or more co- morbid conditions, or an adverse metabolic event associated with bariatric surgery; or increased risk of obesity, or obesity-related co-morbid conditions in the subject. In one embodiment,
expression of the gene can correlate with therapeutically significant weight loss after a metabolic procedure, such as bariatric surgery.
[0013] In some instances, the reference range of gene expression can be determined from multiple patients having undergone a metabolic procedure, such as bariatric surgery. The reference range of gene expression can be an average of gene expression from multiple patients. The reference range of gene expression can be about +30%, +25%, +20%, +15%, +10%, or +5% of an average of gene expression from multiple patients. These may be a group of patients that have experienced therapeutically significant weight loss associated with a metabolic procedure, such as bariatric surgery; improvement, alleviation and/or amelioration of one or more co- morbid conditions, or the absence of an adverse metabolic event. Alternatively, the group of patients may have experienced lack of therapeutically significant weight loss, lack of
improvement, alleviation and/or amelioration of one or more co-morbid conditions, or an adverse metabolic event associated with a metabolic procedure, such as bariatric surgery, or an increased risk of obesity or obesity-related co-morbid conditions.
[0014] In one embodiment, the first and second metabolic procedures can be the same or different procedures. The first metabolic procedure can be a surgical procedure, such as bariatric surgery, including, but not limited to, gastric bypass, Roux-en-Y gastric bypass (RYGB), biliopancreatic diversion, partial gastrectomy procedures such as vertical sleeve gastrectomy, adjustable gastric banding, duodenal switch, duodenojejunal bypass, vertical banded
gastroplasty, intragastric balloon therapy, greater curvature plication, gastric placation (including anterior and anteroposterior plication) and other forms of gastric volume reduction, Magenstrasse and Mill, ileal transposition or interposition, small bowel transposition, biliary diversion, procedures involving anastomotic connections of the gastrointestinal tract, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, gastric electrical stimulation, small bowel electrical stimulation, vagal electrical stimulation, and vagal electrical inhibition. Alternatively, the first metabolic procedure can be a non-surgical procedure, such as, but not limited to, administering pharmacological and nutritional therapies, such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.; providing an alternative medical device based therapy, such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation,
gastric, duodenal or intestinal endoluminal barrier implantation, etc.; and/or the activation of brown adipose tissue.
[0015] As mentioned above, the second metabolic procedure can be the same as or different from the first metabolic procedure. In one embodiment, the first metabolic procedure can be different from the second metabolic procedure. For example, the first metabolic procedure can be a surgical procedure, such as bariatric surgery, and the second metabolic procedure can be non-surgical. In another example, the first metabolic procedure can be a surgical procedure, and the second metabolic procedure can be a different surgical procedure. In one embodiment, the first metabolic procedure can be a non-surgical procedure and the second metabolic procedure can be a surgical procedure.
[0016] In another embodiment, a clinical measurement can be obtained from the subject. The clinical measurement can be obtained prior to or after obtaining a biological sample from the subject, prior to or after comparing the expression level of the gene(s), or prior to performing a first metabolic procedure or second metabolic procedure. The clinical measurement can include at least one of a pre-operative body mass index (BMI), a glucose tolerance, bile acid profile, and body composition/fat distribution of the subject. In an exemplary embodiment, the clinical measurement is a pre-operative body mass index (BMI) of the subject. The clinical
measurement can also include weight, gender, age, medical history and/or status, ethnicity, medical, prescription history and/or status, and types of treatments previously tried (such as medications or other surgical and non-surgical treatments, etc.). In another exemplary embodiment, the nucleic acids can be negative for the genetic indicators and the clinical measurement is a pre-operative BMI of the subject, where the BMI is greater than 23 kg/m .
[0017] In one aspect, diagnostic kits are disclosed for assessing the presence of a single nucleotide polymorphism (SNP) shown in Appendix A (SEQ ID NOs. 129-837), Appendix B, and/or Appendix C in a sample. The kit can include, but is not limited to, a pair of primers that specifically hybridize to regions proximal to the SNP selected from Appendix A (SEQ ID NOs. 129-837), Appendix B, and/or Appendix C and reagents for polymerase chain reaction (PCR). The kit can also include reagents for preparation, isolation and/or purification of nucleic acids from a sample. The kit can also be used in a method having the steps of (a) obtaining a sample
comprising nucleic acids, such as deoxyribonucleic acids (DNA), from the subject; (b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; and if the genetic indicator(s) is absent in (b), performing a first metabolic procedure, such as a bariatric surgery, or if the genetic indicator(s) is present in (b), performing a second metabolic procedure, wherein the second metabolic procedure is different from the first metabolic procedure. In an exemplary embodiment, the second metabolic procedure can exclude bariatric surgery.
[0018] In another aspect, a method of treating obesity or a weight-related disorder in a subject is disclosed. The method can include (a) obtaining a sample comprising nucleic acids from the subject; (b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; (c) predicting an outcome of performing a first metabolic procedure based on the absence or presence of the genetic indicator(s); and (d) performing the first metabolic procedure or performing an alternative second metabolic procedure based on the predicted outcome. For example, the method can include (a) obtaining a sample comprising nucleic acids from the subject; (b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; (c) predicting an outcome of performing a first metabolic procedure, such as a bariatric surgery, based on the absence or presence of the genetic indicator(s); and (d) performing the first metabolic procedure or performing an alternative second metabolic procedure. In an exemplary embodiment, the alternative second metabolic procedure can exclude bariatric surgery.
[0019] In one embodiment, the nucleic acids in the samples can be deoxyribonucleic acids (DNA) or ribonucleic acids (RNA). The nucleic acids can also be positive or negative for the genetic indicators. In some instances, the genetic indicators can be at least one single nucleotide polymorphism (SNP) selected from Appendix A (SEQ ID NOs 129-837), Appendix B, and/or Appendix C that can be absence or presence in the nucleic acids.
[0020] In another embodiment, the outcome predicted from performing the metabolic procedure can be a therapeutically effective weight loss and/or the outcome can be an amelioration of or reduction of at least one weight-related co-morbid condition. In some embodiments when the outcome is a therapeutically effective weight loss, the weight loss can be
at least 20% weight change. The outcome can also be a therapeutically effective weight loss when the genetic indicator(s) is absent. The outcome can further be a therapeutically effective weight loss and the metabolic procedure can be performed in the absence of the genetic indicator(s). In some embodiments, the outcome predicted from performing the metabolic procedure can be lack of therapeutically significant weight loss or an adverse metabolic event associated with bariatric surgery, increased risk of obesity, or obesity-related co-morbid conditions in the subject, lack of therapeutically significant weight loss, lask of improvement, alleviation or amelioration of one or more co-morbid conditions, or an adverse metabolic event associated with bariatric surgery; or increased risk of obesity, or obesity-related co-morbid conditions in the subject.
[0021] In yet another embodiment, the outcome predicted from performing the metabolic procedure can be an amelioration of or reduction of at least one weight-related co-morbid condition. The co-morbid condition can be at least one of hypertension, dyslipidemia, triglyceride levels, diabetes, gastroesophageal reflux, fatty liver disease, steatohepatitis, heart or vascular disease, heart failure, cardiovascular risk, sleep apnea, Barrett's esophagus, asthma, osteoarthritis, compression fractures, gallstones, lymphedema, urinary incontinence, stroke, cognitive dysfunction, pseudotumor cerebri, inflammatory diseases, autoimmune diseases, gout, polycystic ovarian syndrome, infertility, depression, anxiety and/or panic disorders, cognitive or other neurological disorders, cancer risk and mortality (cancers including adenocarcinoma of pancreas, esophagus, gallbladder, pancreas, colon, rectum, breast, prostate; cervical carcinoma, endometrial carcinoma, ovarian carcinoma, renal cell carcinoma, non-Hodgkins lymphoma), weight regain, excess weight loss, nutritional deficiency, constipation, diarrhea, marginal ulceration, dumping syndrome, reactive hypoglycemia, beta cell hyperfunction, gastrointestinal stenosis, liver disorders, nausea/vomiting and/or other metabolic syndromes.
[0022] In yet another aspect, predicting the outcome can include inputting the subject's data into a metabolic procedure outcome prediction system. The metabolic procedure outcome prediction system can be an interactive interface for modeling metabolic procedure outcomes, such as bariatric surgery outcomes. Examples of patient data that can be used for predicting outcomes can include the evaluation of the absence or presence of the genetic indicator(s), and at least one clinical measurement including a pre-operative body mass index (BMI), a glucose
tolerance, bile acid profile, and body composition/fat distribution of the subject, or another measurement of gene expression in a cell or tissue, measurement of a peptide, protein, metabolite or other compound in blood or in a cell or in a tissue.
[0023] In another aspect, a method of treating a metabolic disorder in a subject is disclosed. The method can include measuring expression of the gene(s) in a sample from the subject;
comparing the expression level of the gene(s) to a reference range of expression of the gene, wherein the reference range is determined from multiple patients having undergone a bariatric surgery; and administering to the subject a composition that modulates expression of the gene(s) to mimic the expression after bariatric surgery, thereby treating the metabolic disorder. The method can result in a therapeutically significant weight loss. The method can also result in a therapeutically significant weight loss that is at least a 20% body weight change or an amelioration of or reduction of at least one weight-related co-morbid condition, where the co- morbid condition can be hypertension, dyslipidemia, triglyceride levels, diabetes,
gastroesophageal reflux, fatty liver disease, steatohepatitis, heart or vascular disease, heart failure, cardiovascular risk, sleep apnea, Barrett's esophagus, asthma, osteoarthritis, compression fractures, gallstones, lymphedema, urinary incontinence, stroke, cognitive dysfunction, pseudotumor cerebri, inflammatory diseases, autoimmune diseases, gout, polycystic ovarian syndrome, infertility, depression, anxiety and/or panic disorders, cognitive or other neurological disorders, cancer risk and mortality (cancers including adenocarcinoma of pancreas, esophagus, gallbladder, pancreas, colon, rectum, breast, prostate; cervical carcinoma, endometrial carcinoma, ovarian carcinoma, renal cell carcinoma, non-Hodgkins lymphoma), weight regain, excess weight loss, nutritional deficiency, constipation, diarrhea, marginal ulceration, dumping syndrome, reactive hypoglycemia, beta cell hyperfunction, gastrointestinal stenosis, liver disorders, nausea/vomiting and/or other metabolic syndromes.
[0024] In yet another aspect, kits are disclosed for assessing expression of at least one gene associated with response to a metabolic procedure in a sample. In yet another aspect, kits are disclosed for assessing the sequence of a gene or other chromosomal DNA. The kit can include, but is not limited to, a pair of primers that specifically hybridize to an expression product of the gene(s) selected from SEQ ID NOs 1-128. The kit can also include reagents for preparation, isolation and/or purification of nucleic acids and/or expression products from a sample.
[0025] In another aspect, use of a single nucleotide polymorphism to evaluate a course of treatment for a metabolic disorder is disclosed. In yet another aspect, use of a gene expression level to evaluate a course of treatment for a metabolic disorder is disclosed.
BRIEF DESCRIPTION OF THE DRAWINGS
[0026] The invention will be more fully understood from the following detailed description taken in conjunction with the accompanying drawings, in which:
[0027] Figure 1 is a bar graph showing the excess body weight loss (EBWL) at postoperative weight nadir (achieved after at least 10 months of surgery without coexisting debilitating illness or use of weight lowering medications) after Roux-en-Y gastric bypass (RYGB) in 848 patients with severe obesity;
[0028] Figure 2 is a bar graph showing the mean difference in percent EBWL within patient pairs, according to type of relationship;
[0029] Figure 3 is a bar graph showing no difference on the residuals (deviations of the regressing postoperative BMI on preoperative BMI from the sample mean) from the cohort of 848 patients;
[0030] Figure 4 is a bar graph showing absolute change in weight of the 848 patients after 1 year postoperative with patients in lower BMI groups losing significantly less weight;
[0031] Figure 5 is a bar graph showing final weights obtained at 1 year postoperative of the 848 patients after 1 year postoperative;
[0032] Figure 6 is a bar graph showing the change in body mass index (BMI) of the 848 patients after 1 year postoperative with patients in lower BMI groups having significantly less change in BMI;
[0033] Figure 7 is a bar graph showing final BMI obtained at 1 year postoperative of the 848 patients after 1 year postoperative;
[0034] Figure 8 is a bar graph showing percent excess body weight lost ( EBWL) obtained at 1 year postoperative of the 848 patients after 1 year postoperative with patients at a lower pBMI losing more EBWL at both 1 year and weight nadir;
[0035] Figure 9 is a bar graph showing percent weight change (%WC) obtained at 1 year postoperative of the 848 patients after 1 year postoperative with no significant association between pBMI group and WC at one year, and a relatively weak association between pBMI and WC and weight nadir;
[0036] Figure 10 is a bar graph showing percent change in weight in 858 unrelated
Caucasian individuals grouped according to preoperative BMI;
[0037] Figure 11 is a bar graph showing percent change of weight nadir measured in a subgroup consisting of 693 patients (Cohort 1);
[0038] Figure 12 is a bar graph showing percent change of weight nadir measured in an independent group of 349 Caucasian RYGB patients (Cohort 2);
[0039] Figure 13 is a graphical representation of 112 significant (P < 5 x 10"5) single nucleotide polymorphisms (SNPs) identified in Cohort 2;
[0040] Figure 14 is a flow diagram illustrating direct or indirect association of the SNP with surrounding loci;
[0041] Figure 15 is a graphical representation of chromosome 11 with the SNPs identified as having significant association with percent total weight loss (%WL) at the lowest weight (weight nadir) after RYGB;
[0042] Figure 16 is graph showing the association of carrying the minor allele (MA), rsl7702901, and percent weight change at nadir in patients homozygous null for MA, heterozygous for MA or homozygous for MA;
[0043] Figure 17 is a bar graph showing percent weight change at nadir measured in pooled data from combination of Cohort 1 and Cohort 2 (953 RYGB patients). The shaded area
identifies 171 patients having %WL categorized as less than or greater than or equal to 30% at weight nadir;
[0044] Figure 18 is a bar graph showing percent weight loss with patients carrying at least one copy of the MA being 2.54 times more likely to fall below 30% WL (left shaded area) and no patients with this polymorphism lost more than 50% of his or her weight (right shaded area);
[0045] Figure 19 is an area under the receiver operating characteristic curve (AUROC) showing that inclusion of rsl7709201 has a higher probability of being a predictor of weight loss than rsl7709201 as a random positive influence on weight loss;
[0046] Figure 20 is a bar graph of percent weight loss showing association of rs 17702901 with weight loss in RYGB patients; and
[0047] Figure 21 is a bar graph of percent weight loss showing a lack of an association of validated BMI locus, Melanocortin 4 Receptor (MC4R), with weight loss in RYGB patients.
[0048] Figure 22 is a schematic diagram of the anatomy of Roux-en-Y gastric bypass.
Tissues noted were dissected from mice 10 weeks after RYGB or sham operation;
[0049] Figure 23A is a bar graph showing the comparative expression of st8sia2 in RYGB- treated and sham operated, weight matched mice (WMS). Grey bars denote the WMS group, blue bars the RYGB group. Error bars denote the standard error of the mean. * p<0.05, ** p<0.01, *** p<0.001;
[0050] Figure 23B is a bar graph showing the comparative expression of slco3al in RYGB- treated and sham operated, weight matched mice (WMS). Grey bars denote the WMS group, blue bars the RYGB group. Error bars denote the standard error of the mean. * p<0.05, ** p<0.01, *** p<0.001;
[0051] Figure 24A is a regional association plot showing the AQP11 locus. Each SNP is plotted as a diamond based on its chromosomal location (jc-axis) and -logw P value (left _y-axis). Recombination rates are plotted in grey toward the bottom of the graph (right _y-axis). The large upper diamond represents the top SNP in the region (rs7129556) from the genome- wide
association study (GWAS), and the large lower diamond represents the p-value from that SNP in the replication cohort;
[0052] Figure 24B is a bar graph showing the relative expression level of aqpll . Light bars denote the WMS group, dark bars the RYGB group. Error bars denote the standard error of the mean. * p<0.05, ** p<0.01, *** p<0.001; and
[0053] Figure 24C is a bar graph showing the relative expression level of clnsla. Light bars denote the WMS group, dark bars the RYGB group. Error bars denote the standard error of the mean * p<0.05, ** p<0.01, *** p<0.001.
DETAILED DESCRIPTION OF THE INVENTION
[0054] Certain exemplary embodiments will now be described to provide an overall understanding of the principles of the structure, function, manufacture, and use of the therapeutics and methods disclosed herein. One or more examples of these embodiments are illustrated in the accompanying drawings. Those skilled in the art will understand that the therapeutics and methods specifically described herein and illustrated in the accompanying drawings are non-limiting exemplary embodiments and that the scope of the present invention is defined solely by the claims. The features illustrated or described in connection with one exemplary embodiment may be combined with the features of other embodiments. Such modifications and variations are intended to be included within the scope of the present invention.
[0055] SEQ ID NOs 1-128 in the present application correspond to SEQ ID NOs 1-128 of U.S. Provisional Application Serial No. 61/740,678, and SEQ ID NOs 129-837 correspond to the sequences from Appendix A of U.S. Provisional Application Serial No 61/704,434 (which is identical to Appendix A of the present application).
Metabolic Disorders (Obesity and Other Weight-Related Disorders)
[0056] Methods and kits are provided to evaluate genetic indicators, such as by identifying genetic indicators, and/or measuring and assessing gene expression for treatment of obesity and/or weight-related disorders. It has been discovered that genetic indicators, such as single
nucleotide polymorphisms, can be indicators for weight loss potential after metabolic surgery, such as bariatric surgery. Given the correlation between weight loss and improvements in comorbidities associated with excess weight, these genetic predictors can be indicators or predictors of improvements in comorbid conditions after bariatric surgery. It has also been discovered that certain genes demonstrate differential gene expression after a metabolic procedure, such as bariatric surgery. It has been further discovered that a correlation exists between the weight loss and other improvements in comorbidities and gene expression of certain genes. Therefore, modulating certain gene expression can be therapeutic to improve comorbid conditions after bariatric surgery. Further, the gene expression can serve a surrogate marker for whether a surgical procedure (e.g., bariatric surgery) is likely to lead to a successful outcome, or an alternative procedure is better suited for a certain patient or patient population. Therefore, the invention disclosed is generally directed to therapeutic methods and compositions for treating metabolic disorders, such as obesity and/or other weight-related disorders, in a subject by (1) evaluating genetic indicators, such as by evaluating the subject's deoxyribonucleic acids (DNA) for a presence or absence of one or more genetic indicators, and/or evaluating gene expression in the subject for an overexpression or an underexpression of one or more specific genes associated with metabolic disorders.
[0057] Weight loss can be characterized using a number of different metrics, including the absolute number of pounds or body mass index (BMI) points lost, weight or BMI achieved after weight loss, the percent of baseline weight or BMI lost (% weight change (WC)), and percent excess body weight lost (% EBWL).
[0058] The phrase "weight-related disorder" as used herein, refers to disorders, diseases, and conditions that are caused or characterized by abnormal energy use or consumption leading to excessive weight gain or loss, altered responses to ingested or endogenous nutrients, energy sources, hormones or other signaling molecules within the body or altered metabolism of carbohydrates, lipids, proteins, nucleic acids or a combination thereof. A weight-related disorder can be associated with either a deficiency or excess in a metabolic pathway resulting in an imbalance in metabolism of nucleic acids, proteins, lipids, and/or carbohydrates. Factors affecting metabolism include, and are not limited to, the endocrine (hormonal) control system (e.g., the insulin pathway, the enteroendocrine hormones including GLP-1, PYY or the like), the
neural control system (e.g., GLP-1 or other neurotransmitters in the brain, spinal cord, peripheral or enteric nervous systems) or the like. Some non-limiting examples of weight-related disorders can be obesity, diabetes, including type II diabetes, insulin-deficiency, insulin-resistance, insulin- resistance related disorders, glucose intolerance, syndrome X, inflammatory and immune disorders, dyslipidemia, metabolic syndrome, non-alcoholic fatty liver, abnormal lipid metabolism, obstructive sleep apnea, asthma, autoimmune and inflammatory disorders, cancer, cognitive and neurodegenerative disorders, hypertension, high cholesterol, anxiety, congestive heart failure, ischemic heart disease, GERD, atherogenic dyslipidemia, hyperlipidemic conditions such as atherosclerosis, hypercholesterolemia, and other coronary artery diseases in mammals, and other disorders of metabolism.
[0059] As used herein, the term "obesity" or "obese" typically refers to a non-Asian individual having a body mass index (BMI) of >30 kg/m 2 or >27 kg/m 2 in Asian individuals and "overweight" typically refers to a non-Asian individual having a body mass index (BMI) of >25 kg/m 2 or >23 kg/m 2 in Asian individuals. BMI is a measure expressing the relationship (or ratio) of weight-to-height based on a mathematical formula in which a person's body weight in kilograms is divided by the square of his or her height in meters (i.e., wt/(ht) ). Individuals having BMI of >25 kg/m 2 in non-Asians or >23 kg/m 2 in Asians have a substantially increased risk of at least one weight-related co-morbid condition or having a metabolic disorder or syndrome. As used herein, the terms "co-morbidity" or "co-morbid condition" typically refers to, but is not limited to, hypertension, dyslipidemia, triglyceride levels, diabetes,
gastroesophageal reflux, fatty liver disease, steatohepatitis, heart or vascular disease, heart failure, cardiovascular risk, sleep apnea, Barrett's esophagus, asthma, osteoarthritis, compression fractures, gallstones, lymphedema, urinary incontinence, stroke, cognitive dysfunction, pseudotumor cerebri, inflammatory diseases, autoimmune diseases, gout, polycystic ovarian syndrome, infertility, depression, anxiety and/or panic disorders, cognitive or other neurological disorders, cancer risk and mortality (cancers including adenocarcinoma of pancreas, esophagus, gallbladder, pancreas, colon, rectum, breast, prostate; cervical carcinoma, endometrial carcinoma, ovarian carcinoma, renal cell carcinoma, non-Hodgkins lymphoma), weight regain, excess weight loss, nutritional deficiency, constipation, diarrhea, marginal ulceration, dumping syndrome, reactive hypoglycemia, beta cell hyperfunction, gastrointestinal stenosis, liver
disorders, nausea/vomiting and/or other metabolic syndromes. As the name suggests, "metabolic disorder or syndrome" is tied to the body's metabolism, and more likely to conditions that influence metabolism, such as insulin resistance. Metabolic disorder or syndrome can also be characterized by excess body fat, atherogenic dyslipidemia, elevated blood pressure and insulin resistance, among others.
[0060] Other weight-related disorders can include conditions that occur or cluster together, and/or increase the risk for heart disease, stroke, diabetes, and obesity. Having just one of these conditions such as increased blood pressure, elevated insulin levels, excess body fat around the waist or abnormal cholesterol levels can increase the risk of the above mentioned diseases. In combination, the risk for coronary heart disease, stroke, insulin-resistance syndrome, and diabetes is even greater.
[0061] The increasing prevalence of obesity in the population has led to a parallel rise in metabolic procedures, like bariatric surgery, as a treatment for obesity and related comorbid conditions. As used herein, the term "metabolic procedures" can include surgical and nonsurgical procedures. Surgical procedures can achieve a sustained weight reduction of up to 70% of excess body weight in the majority of patients, and are often more effective than nonsurgical approaches. Nonlimiting examples of surgical procedures can include bariatric surgery. As used herein, "bariatric surgery" generally refers and can include procedures often referred to as metabolic surgery or therapy, as well as a variety of procedures performed in a subject that leads to a physiologic improvement in energy balance, nutrient utilization, or metabolic disorders. These procedures often, but not always, result in weight loss. Bariatric surgery refers to a surgical procedure to alter gastrointestinal structure or function so as to affect body weight, body composition, or energy balance regulation or otherwise alter metabolic function. Some non-limiting examples of bariatric surgery can be any form of gastric bypass, Roux-en-Y gastric bypass (RYGB), biliopancreatic diversion, partial gastrectomy procedures such as vertical sleeve gastrectomy, adjustable gastric banding, duodenal switch, duodenojejunal bypass, vertical banded gastroplasty, intragastric balloon therapy, greater curvature plication, gastric plication (including anterior and anteroposterior plication) and other forms of gastric volume reduction, Magenstrasse and Mill, ileal transposition or interposition, small bowel transposition, biliary diversion, procedures involving anastomotic connections of the
gastrointestinal tract (e.g., jejunoileostomy, etc.), gastric electrical stimulation, small bowel electrical stimulation, vagal electrical stimulation, vagal electrical inhibition, and variations of the procedures above as well as other methods known by those skilled in the art. Metabolic procedures can also include non- surgical procedures including, by way of non-limiting examples, administering pharmacological and nutritional therapies, such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.; providing an alternative medical device based therapy, such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.; and/or the activation of brown adipose tissue. Each of the surgical and non-surgical procedures may be performed alone or in addition to other treatments.
[0062] It has been discovered that subjects with certain diagnostic markers respond to therapeutic interventions, such as gastric bypass surgery. Therefore, in an exemplary
embodiment, a method of treating a metabolic disorder, such as obesity, in a subject can include obtaining a sample with DNA from the subject, evaluating the DNA for the presence or absence of one or more genetic indicators and performing a first metabolic procedure, such as bariatric surgery or a second metabolic procedure, excluding bariatric surgery, depending on the absence or presence of one or more genetic indicators.
[0063] It has also been discovered that expression of certain genes is associated with a better response to therapeutic interventions, such as gastric bypass surgery. Therefore, in an exemplary embodiment, a method of treating a metabolic disorder in a subject can include obtaining a sample from the subject, evaluating the sample for expression of at least one gene (wherein the gene is shown to be differentially expressed after bariatric surgery or wherein expression of the gene correlates with weight loss after a metabolic procedure), and performing a first metabolic procedure or a second metabolic procedure excluding a bariatric surgery depending on the expression of gene(s).
Differentially Expressed Genes and Genetic Indicators
[0064] Identification of specific genetic indicators, such as SNPs associated with weight loss after RYGB, or expression patterns, such as expression of genes associated with weight loss after
RYGB, may both enhance the understanding of the mechanisms of weight loss as well as help identify those patients for whom bariatric surgery procedures are most effective.
[0065] As used herein, "polymorphism" refers to a variation in the sequence of a gene in the genome amongst a population, such as allelic variations and other variations that arise or are observed. "Genetic polymorphisms" refers to the variant forms of DNA sequences that can arise as a result of nucleotide alteration or substitution, deletion, insertion, rearrangement or duplication, for example. Thus, a polymorphism refers to the occurrence of two or more genetically determined alternative sequences or alleles in a population. These polymorphisms can occur in coding and non-coding portions of the genome, and can be manifested or detected as differences in nucleic acid sequences, gene expression, and/or other differences in mRNA structure and function, including, for example transcription, processing, translation, transport, protein processing, trafficking, DNA synthesis, expressed proteins, other gene products or products of biochemical pathways or in post-translational modifications and any other differences manifested among members of a population. A "single nucleotide polymorphism" or "SNP" refers to a polymorphism that arises as the result of a single base change, such as an insertion, deletion or change in a base.
[0066] A polymorphic marker or site is the locus at which divergence occurs. Such a site may be as small as one base pair (an SNP). Polymorphic markers include, but are not limited to, restriction fragment length polymorphisms, copy number variations, variable number of tandem repeats (VNTR's), hypervariable regions, minisatellites, dinucleotide repeats, trinucleotide repeats, tetranucleotide repeats and other repeating patterns, simple sequence repeats and insertional elements, such as Alu.
[0067] Polymorphic forms also are manifested as different mendelian alleles for a gene. The genomes of all organisms undergo spontaneous mutation in the course of their continuing evolution, generating variant forms of progenitor genetic sequences. A variant form may confer differences in proteins, protein modifications, RNA expression, RNA modification, DNA and RNA methylation, regulatory factors that alter gene expression and DNA replication, and any other manifestation of alterations in genomic nucleic acid or organelle nucleic acids.
[0068] As used herein, an "isolated" nucleic acid molecule, such as a nucleic acid molecule containing a SNP genetic indicator or an expression product of a gene or other transcript (e.g., messenger RNA, microRNA or other non-coding RNA), can be substantially free of other cellular material, or culture medium when produced by recombinant techniques, or chemical precursors or other chemicals when chemically synthesized. A nucleic acid molecule can be fused to other coding or regulatory sequences and still be considered "isolated." Nucleic acid molecules present in non-human transgenic animals, which do not naturally occur in the animal, are also considered "isolated." For example, recombinant DNA molecules contained in a vector are considered "isolated." Further examples of "isolated" DNA molecules include recombinant DNA molecules maintained in heterologous host cells, and purified (partially or substantially) DNA molecules in solution. Isolated RNA molecules include in vivo or in vitro RNA transcripts of the isolated SNP-containing DNA molecules of the present invention. Isolated nucleic acid molecules according to the present invention further include such molecules produced synthetically.
[0069] A nucleic acid molecule can include one or more SNPs with flanking nucleotide sequences on either side of the SNPs. A flanking sequence can include nucleotide residues that are naturally associated with the SNP site and/or heterologous nucleotide sequences. Preferably the flanking sequence can be up to about 500, 300, 100, 60, 50, 30, 25, 20, 15, 10, 8, or 4 nucleotides (or any other length in between) on either side of a SNP.
[0070] As used herein, an "isolated protein," once expressed, can be isolated by lysing cells and applying standard protein isolation techniques to the lysates or the pellets. Monitoring the purification process can be accomplished by using Western blot techniques or radioimmunoassay or other standard immunoassay techniques.
[0071] As used herein, an "amplified polynucleotide" can include a nucleic acid molecule containing one or more SNPs or a gene that can be replicated by at least two fold through any nucleic acid amplification method performed in vitro. In one embodiment, an amplified polynucleotide is the result of at least a ten fold, fifty fold, one hundred fold, one thousand fold, or even ten thousand fold increase as compared to its starting amount in a test sample. In a typical PCR amplification, a polynucleotide of interest is often amplified at least fifty thousand
fold in amount over the unamplified DNA template, but the precise amount of amplification needed for an assay depends on the sensitivity of the subsequent detection method used.
[0072] A subject or patient may be homozygous or heterozygous for an allele at each SNP position. A SNP can, in some instances, be referred to as a "cSNP" to denote that the nucleotide sequence containing the SNP is an amino acid coding sequence. While SNPs can be bi-, tri-, or tetra-allelic, the vast majority of the SNPs are bi-allelic, and are thus often referred to as "bi- allelic markers," or "di-allelic markers."
[0073] As used herein, references to "SNPs" and SNP genotypes include individual SNPs and/or haplotypes, which are groups of SNPs that are generally inherited together. Haplotypes can have stronger correlations with diseases or other phenotypic effects compared with individual SNPs, and therefore may provide increased diagnostic accuracy in some cases. An "allele" is an alternative form or variation in a DNA sequence. Many SNPs have only two alleles: minor and major alleles. SNPs are routinely used in SNP-based genetic linkage analysis to map a disease to a particular locus, the position of a gene (or SNP) on a chromosome.
[0074] Methods and kits are provided to identify genetic indicators and/or evaluate and assess expression of genes associated with response to a metabolic procedure, such as bariatric surgery, for treatment of metabolic disorders. It has been discovered that genetic indicators, such as single nucleotide polymorphisms, and gene expression, such as genes associated with response to a metabolic procedure, can indicate weight loss potential after the metabolic procedure, such as bariatric surgery. By obtaining a sample from a subject and extracting nucleic acids from or analyzing gene expression in the sample, response to the metabolic procedure, e.g. weight loss potential after the bariatric surgery, can be predicted and/or assessed.
[0075] The term "subject" as used herein refers to any living organism, including, but not limited to, humans, nonhuman primates such as chimpanzees and other apes and monkey species; farm animals such as cattle, sheep, pigs, goats and horses; domestic mammals such as dogs and cats; laboratory animals including rodents such as mice, rats, rabbits and guinea pigs, and the like. The term does not denote a particular age or sex. In a specific embodiment, the subject is human. In an exemplary embodiment, the subject is a patient.
[0076] The term "sample" is intended to include tissues, cells, fluids and biological samples isolated from a subject, as well as tissues, cells and fluids present within a subject. The sample can be a tissue sample, such as from an organ, or fluid, ascites, and any other sample that is used by those familiar with the art. The sample can be derived from any source which contains proteins or expression products and/or nucleic acids, DNA (e.g., chromosomal nucleic acids) or RNA, such as a blood sample, body excrements such as semen, saliva, stool, urine, amniotic fluid and so forth, sample of cerebrospinal fluid, or tissue sample from skin, muscle, buccal or conjunctival mucosa, placenta, gastrointestinal tract or other organs. A sample of proteins and/or nucleic acid from fetal cells or tissue can be obtained by appropriate methods, such as by amniocentesis or chorionic villus sampling (direct or cultured). In one aspect, the sample can be a biopsy sample or a small number of cells or a tissue sample removed for processing. Common examples of biopsy methods can include, but are not limited to, oral swab, brush cytology, core needle biopsy, surgical biopsy, punch biopsy, shave biopsy, incisional/excisional biopsy and curettage biopsy.
[0077] In some embodiments, the sample of cells or tissue sample can be obtained from the subject by biopsy or surgical resection. A sample of cells, tissue, or fluid can be removed by needle aspiration biopsy. For this, a fine needle attached to a syringe is inserted through the skin and into the organ or tissue of interest. The needle is typically guided to the region of interest using ultrasound or computed tomography (CT) imaging. Once the needle is inserted into the tissue, a vacuum is created with the syringe such that cells or fluid may be sucked through the needle and collected in the syringe. A sample of cells or tissue may also be removed by incisional or core biopsy. For this, a cone, a cylinder, or a tiny bit of tissue can be removed from the region of interest. CT imaging, ultrasound, or endoscopy can be used to guide this type of biopsy.
[0078] Once a sample of cells or sample of tissue is removed from the subject, it may be processed for the isolation of RNA or protein using techniques well known in the art and disclosed in standard molecular biology reference books. A sample of tissue may also be stored in RNAlater (Ambion; Austin, TX) or flash frozen and stored at -80 °C for later use. The tissue sample may also be fixed with a fixative, such as formaldehyde, paraformaldehyde, or acetic acid/ethanol. The fixed tissue sample may be embedded in wax (paraffin) or a plastic resin. The
embedded tissue sample (or frozen tissue sample) may be cut into thin sections. RNA or protein may also be extracted from a fixed or wax-embedded tissue sample.
[0079] Direct assessment for the presence of the genetic identifiers or for gene expression can be performed on a sample without processing to isolate nucleic acids or gene expression products. Alternatively, a sample can be processed to enhance access to gene expression products, nucleic acids, or copies of nucleic acids (e.g., amplification of nucleic acids), and the processed sample can then be used to assess for the presence of the genetic identifiers or for gene expression. For example, in one embodiment, cDNA is prepared from a sample comprising mRNA, for use in the methods. The mRNA can be isolated from the sample and converted into cDNA. Alternatively or in addition, if desired, an amplification method can be used to amplify nucleic acids for use as the test sample in the assessment for the presence or absence of a genetic identifier(s) or for gene expression. The nucleic acids can be isolated from the samples or can be processed and analyzed within the sample.
[0080] Nucleic acids, including RNA, DNA, or cDNA, proteins or other expression products can be analyzed for the genetic indicator(s) or measured to determine gene expression from a sample. The presence of genetic indicator(s) or gene expression can be evaluated in nucleic acids or proteins in vitro, in situ, as well as in vivo. For example, in vitro techniques for detection of genetic indicator(s) in mRNA or for measuring expression can include assays such as ELISA assay and Western blot analysis, immunocytochemical assays, assessment of mRNA in PCR, q-PCR, northern hybridizations and in situ hybridizations, assessment of cDNA in Southern hybridizations, PCR, quantitative PCR (qPCR), and introduction of labeled nucleic acids for incorporation into the nucleic acids, for example, the radiolabeled nucleic acids whose presence and location in a subject can be detected by standard imaging techniques.
[0081] Another embodiment for identifying genetic indicators in RNA or DNA or for measuring gene expression can include the use of a labeled nucleic acid probe capable of hybridizing to a mRNA or cDNA. A wide variety of conventional techniques are available, including mass spectrometry, chromatographic separations, 2-D gel separations, microarrays, binding assays (e.g., immunoassays), competitive inhibition assays, one- and two-dimensional gels and sandwiched ELISA. Typical methodologies for RNA detection include RNA extraction
from a cell or tissue sample, followed by hybridization of a labeled probe, (e.g., a
complementary polynucleotide) specific for the target RNA to the extracted RNA, and detection of the probe (e.g., Northern blotting), direct sequencing, gel electrophoresis, column
chromatography, and quantitative PCR.
[0082] Primers based on a nucleotide sequence specific for one or more of the genetic indicators or genes can be used to analyze the presence or absence in or to measure expression of the corresponding gene(s) or genetic indicator(s). In some embodiments, a primer pair can be designed by utilizing primer design software, such as GenScript, Primer3, PRIDE and Primer Express. Commercial primers are also available for purchase corresponding to multiple locations throughout the gene. The primers can be at least 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 20, 25, 30, 35, or 40 basepairs in length. In an exemplary embodiment, the primers can be at least 10 basepairs in length. The primers can also hybridize to a region of nucleic acids (mRNA, cDNA or genomic DNA) proximal or in the vicinity of the genetic indicator or the gene.
[0083] The primer can be similar (sufficiently similar or identical to hybridize to the sequence) or complementary (sufficiently similar or identical to hybridize to the complement sequence) to a nucleic acid sequence upstream or downstream from the genetic indicator. The primer can hybridize to a sequence that is at least 50, 60, 70, 80, 90, 100, 110, 120, 130, 140, 150, 160, 170, 180, 190, 200, 250, 300, 350, 400, 450, 500, 550, 600, 650, 700, 750, 850, 900, 950, 1000 basepairs or more or any number of basepairs in between from the genetic indicator. In one embodiment, the primers can specifically hybridize to a region proximal to one or more genetic indicators (such as a single nucleotide polymorphism (SNP) as shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C). In an exemplary embodiment, the primers can be complementary to a nucleic acid sequence of at least 10 bases found at least 200 basepairs or more from the genetic indicator.
[0084] The primer can be similar (sufficiently similar or identical to hybridize to the sequence) or complementary (sufficiently similar or identical to hybridize to the complement sequence) to a nucleic acid sequence of the gene. In one embodiment, the primers can be specific for at least one of SEQ ID NOs 1-128. See Table 10 for correspondence of SEQ ID NO to gene
name/description and accession number.
[0085] Diagnostic kits and/or devices are also included. The diagnostic kit and/or device can include, but is not limited to, sample collection materials (storage solutions and collection apparatus such as swab, biopsy needle, blood/body fluid needle, brush, etc), protein, DNA or RNA extraction and isolation materials (solutions and enzymes for performing such procedures); nucleic acid amplification materials (solutions, enzymes and primers specific for the genetic indicator(s) or primers for performing such procedures); and sequencing materials (solutions, enzymes and gene specific primers for performing such procedures). The diagnostic kit and/or device can include any of the above and exclude any materials from the above. In an exemplary embodiment, the diagnostic kit and/or device can include DNA polymerase chain reaction amplification solutions and/or enzymes and at least one set of primers specific for a genetic indicator. In another exemplary embodiment, the diagnostic kit and/or device can include DNA polymerase chain reaction amplification solutions and/or enzymes and at least one set of gene specific primers.
[0086] In one aspect, a method of treating obesity or weight-related disorders includes evaluating DNA for the absence or presence of one or more genetic indicators, such as SNPs. The DNA can be positive or negative for one or more indicators. A DNA sample from a subject can be evaluated for the presence or absence of the genetic indicator(s). In some instances, the DNA can be negative for the indicator(s) and the pre-operative BMI can be greater than 20 kg/m2.
[0087] Also, the presence or absence of the genetic indicator(s) can correlate with therapeutically effective weight loss associated with bariatric surgery; improvement, alleviation or amelioration of one or more co-morbid conditions; and/or lack of therapeutically effective weight loss associated with bariatric surgery, increased risk of obesity or obesity-related co- morbid conditions in the subject.
[0088] In one embodiment, the presence or absence of the genetic indicator(s) can correlate with therapeutically effective weight loss after bariatric surgery in the subject. Therapeutically effective weight loss can be characterized by loss of at least 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, 80%, 85% or more of excess body weight. Therapeutically effective weight loss can also be characterized as at least 10%, 15%, 20%, 25%, 30%, 35%,
40%, 45%, 50%, 60%, 65%, 70%, 75%, or more weight change. Alternatively or in addition to, therapeutically effective weight loss can be characterized by change of at least 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, 80%, 85% or more of body mass index. Excess body weight, weight change, and/or body mass index measurements can be determined by taking the measurement of the subject prior to treatment or preoperatively and compare the
measurement to another measurement taken at a time point after treatment or surgery. The time point for taking the measurement can be 1, 3, 6, 9, 12, 18, 24, 36, 48, 72, 84, 96, 108, 120 months post treatment or postoperative or any number of months in between. In an exemplary embodiment, the therapeutically effective weight loss is at least 20% weight change after bariatric surgery or alternative treatment in the subject.
[0089] Also, the presence or absence of one or more genetic indicator(s) can correlate with improvement, alleviation or amelioration of one or more co-morbid conditions in the subject. The presence or absence of the genetic indicator(s) can correlate with, for example, reduced hypertension, reduced dyslipidemia, improvement or alleviation of diabetes, reduced acid reflux, alleviation of fatty liver or steatohepatitis, reduced risk of heart disease, alleviation of depression, alleviation of sleep apnea, alleviation of asthmatic symptoms, alleviation of arthritis, reduced risk of compression fractures, reduced occurrence of gallstones, lymphoedema, alleviation of urinary incontinence, reduced risk of stroke, reduced risk of cancer and/or reduced risk of other metabolic syndromes.
[0090] Alternatively, the presence or absence of one or more genetic indicator(s) can correlate with lack of therapeutically effective weight loss associated with bariatric surgery or increased risk of obesity, or obesity-related co-morbid conditions in the subject. The presence or absence of the genetic indicator(s) can correlate with, for example, lack of weight loss after bariatric surgery, increased hypertension, risk of dyslipidemia, development of diabetes, acid reflux, fatty liver disease or steatohepatitis, heart disease, depression, sleep apnea, asthmatic symptoms, arthritis, compression fractures, gallstones, lymphoedema, urinary incontinence, stroke, cancer and/or risk of other metabolic syndromes.
[0091] The genetic indicators can be single nucleotide polymorphisms that occur in coding and non-coding portions of the genome, and can be manifested or detected as differences in
nucleic acid sequences (DNA), gene expression products (RNA and proteins), including, for example transcripts (mRNA, miRNA, and others), proteins, other gene products or products of biochemical pathways or in post-translational modifications and any other differences manifested among members of a population. In one embodiment, one or more genetic indicators are absent from the subject's nucleic acid sample, such as DNA, where at least one genetic indicator is a single nucleotide polymorphism (SNP) shown in Appendix A (SEQ ID NOs 129-837), Appendix
B, and/or Appendix C. In another embodiment, one or more genetic indicators are present in the subject's nucleic acid sample, such as DNA, where at least one genetic indicator is a single nucleotide polymorphism (SNP) shown in Appendix A (i.e, SEQ ID NOs 129-837 (SNPs identified as statistically significant for percent weight loss)), Appendix B (additional SNPs identified as statistically significant for percent weight loss) or Appendix C (SNPs identified as statistically significant for percent excess body weight loss). Each SNP sequence is associated with a unique accession number (e.g., rs number) that is available in the Single Nucleotide Polymophism Database hosted by the National Center for Biotechnology Information (NCBI) to identify the genetic variation and sequence information. In yet another embodiment, one or more genetic indicators are absent from the subject's nucleic acid sample, such as DNA, and one or more different genetic indicators are present in the subject's DNA sample, where at least one genetic indicator is a single nucleotide polymorphism (SNP) shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C.
[0092] For example, the genetic indicator(s) can be at least one single nucleotide
polymorphism (SNP) shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix
C. Selected genetic indicators, such as the SNPs shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C, can be positive or negative indicators for successful obesity or weight-related disorder treatment. In one embodiment, the genetic indicator can be one or more SNPs shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C, such as SEQ ID NO 129-SEQ ID NO 138, SEQ ID NO 129-SEQ ID NO 148, SEQ ID NO 129-SEQ ID NO 158, SEQ ID NO 129-SEQ ID NO 168, SEQ ID NO 129-SEQ ID NO 178, SEQ ID NO 129- SEQ ID NO 188, SEQ ID NO 129-SEQ ID NO 198, SEQ ID NO 129-SEQ ID NO 208, SEQ ID NO 129-SEQ ID NO 218, SEQ ID NO 129-SEQ ID NO 228, SEQ ID NO 129-SEQ ID NO 328, SEQ ID NO 129-SEQ ID NO 428, SEQ ID NO 129-SEQ ID NO 528, SEQ ID NO 129-SEQ ID
NO 628, SEQ ID NO 129-SEQ ID NO 728, SEQ ID NO 129-SEQ ID NO 828, SEQ ID NO 129- 837, SEQ ID NO 129-SEQ ID NO 928, SEQ ID NO 129-SEQ ID NO 1028, SEQ ID NO 129- SEQ ID NO 1128, SEQ ID NO 129-SEQ ID NO 2128, SEQ ID NO 129-SEQ ID NO 3128, SEQ ID NO 129-SEQ ID NO 4128, SEQ ID NO 129-SEQ ID NO 5128, etc. In another embodiment, the genetic indicator can be one or more SNPs shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C, as identified by the unique SNP identifier (e.g. rs number). In another embodiment, the genetic indicator can be one or more SNPs located on chromosome 6, chromosome 11, and/or chromosome 15. In yet another embodiment, the genetic indicators are one or more SNPs selected from rs7158359, rs7129556, rsl0899387, rs934760, rsl 104959, rsl7702901, rs588217 and rs9357419. In an exemplary embodiment, at least one genetic indicator can be located on chromosome 15. In another exemplary embodiment, the at least one genetic indicator can be located within a cluster or cloud of SNPs within a region of a chromosome that may be in linkage disequilibrium with one another. The genetic indicator(s) can include one or more SNPs within the cloud and/or all the SNPs within the cloud. The genetic indicator(s) can also include one or more SNPs in linkage disequilibrium. In yet another exemplary embodiment, at least one genetic indicator is rs 17702901. At least one genetic indicator can be rsl7702901 and the DNA can be negative for rsl7702901. In another embodiment, the DNA is negative for the rs 17702901 and the pre-operative BMI of the subject can be greater than 25 kg/m .
[0093] In one aspect, a method of treating metabolic or weight-related disorders includes evaluating expression of one or more genes associated with response to a metabolic procedure. The gene can also be shown to be differentially expressed in patients before or after bariatric surgery. The expression level of the gene(s) can be compared to a reference range of expression of the gene and if expression of the gene(s) is outside the reference range, a first metabolic procedure can be performed, or if expression of the gene is inside the reference range, an alternative second metabolic procedure can be performed. For example, the expression level of the gene(s) can be compared to a reference range of expression of the gene and if expression of the gene(s) is outside the reference range, a first metabolic procedure can be performed, or if expression of the gene is inside the reference range, an alternative second metabolic procedure without a bariatric surgery can be performed. In some instances, the reference range of gene
expression can be determined from multiple patients having undergone a metabolic procedure, such as bariatric surgery. The reference range of gene expression can be an average of gene expression from multiple patients. The reference range of gene expression can be about +30%, +25%, +20%, +15%, +10%, or +5% of an average of gene expression from multiple patients. The multiple patients may be a group of patients that have experienced therapeutically significant weight loss associated with a metabolic procedure, such as bariatric surgery;
improvement, alleviation and/or amelioration of one or more co-morbid conditions.
Alternatively, the group of patients may have experienced lack of therapeutically significant weight loss or an adverse metabolic event associated with a metabolic procedure, such as bariatric surgery, increased risk of obesity or obesity-related co-morbid conditions.
[0094] The gene can be at least one of SEQ ID NOs 1-128, also shown in Table 10. The gene can correlate with therapeutically significant weight loss associated with a metabolic procedure, such as bariatric surgery; improvement, alleviation or amelioration of one or more co- morbid conditions; and/or lack of therapeutically significant weight loss or an adverse metabolic event associated with bariatric surgery, increased risk of obesity or obesity-related co-morbid conditions in the subject. In one embodiment, gene expression can correlate with therapeutically significant weight loss after a metabolic procedure, such as bariatric surgery. Therapeutically significant weight loss can be characterized by loss of at least 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, 80%, 85% or more of excess body weight. Therapeutically significant weight loss can also be characterized as at least 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, or more weight change. Alternatively or in addition to, therapeutically significant weight loss can be characterized by change of at least 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 65%, 70%, 75%, 80%, 85% or more of body mass index.
[0095] Also, gene expression can correlate with improvement, alleviation or amelioration of one or more co-morbid conditions in the subject. Gene expression can correlate with, for example, reduced hypertension, reduced dyslipidemia, improvement or alleviation of diabetes, reduced acid reflux, alleviation of fatty liver or steatohepatitis, reduced risk of heart disease, alleviation of depression, alleviation of sleep apnea, alleviation of asthmatic symptoms, alleviation of arthritis, reduced risk of compression fractures, reduced occurrence of gallstones,
lymphedema, alleviation of urinary incontinence, reduced risk of stroke, reduced risk of cancer and/or reduced risk of other metabolic syndromes.
[0096] Alternatively, gene expression can correlate with lack of therapeutically significant weight loss or an adverse metabolic event associated with bariatric surgery or increased risk of obesity, or obesity-related co-morbid conditions in the subject. Gene expression can correlate with, for example, lack of weight loss after bariatric surgery, increased hypertension, risk of dyslipidemia, development of diabetes, acid reflux, fatty liver disease or steatohepatitis, heart disease, depression, sleep apnea, asthmatic symptoms, arthritis, compression fractures, gallstones, lymphedema, urinary incontinence, stroke, cancer and/or risk of other metabolic syndromes.
[0097] Gene expression can be measured prior to any metabolic procedure or preoperative procedure. Gene expression can be also be measured and compared to one or more
measurements taken at different time points, such as after a metabolic procedure or post-surgery. Gene expression can be measured at 1, 3, 6, 9, 12, 18, 24, 36, 48, 72, 84, 96, 108, 120 months post metabolic procedure or postoperative or any number of months in between. In an exemplary embodiment, gene expression is measured prior to a metabolic procedure.
Modulating Gene Expression
[0098] Methods and compositions for modulating expression of at least one gene associated with response to a metabolic procedure in a target tissue to treat a subject having a metabolic disorder are also disclosed. Methods and pharmaceutical compositions to modulate gene expression can include delivering regulatory proteins, ligands, agonists and antagonists of expression of the gene to a target tissue. Gene therapy can be used to modulate gene expression and can also be accomplished by methods known to those skilled in the art. For example, one approach is to use an inducible promoter to drive expression of the gene delivered. In return, the in vivo steady state level of the gene can be increased, through augmented expression of the gene.
The terms "modulate" or "modulating" are used herein to refer to an increase or or change in expression of at least one target protein or gene.
[00100] In one aspect, methods and composition are disclosed to modulate gene expression by providing a full-length, a portion or fragment of, or variant of the gene or its encoded protein and expressing the full-length, a portion or fragment of, or variant of the gene or its encoded protein in the target tissue. The term "full-length" refers to the entire open reading frame, capable of expressing a full-length encoded protein.
[00101] A "portion" or "fragment" of the gene or encoded protein refers to any sequence that has fewer nucleic acids or amino acids than the entire sequence of the gene or its encoded protein. Sizes of nucleic acid fragments can be 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 99% or greater of the full-length gene. Sizes of peptide fragments can be about 500 amino acids, about 400 amino acids, about 300 amino acids, about 200 amino acids, about 100 amino acids, about 80 amino acids, about 60 amino acids, about 40 amino acids, about 20 amino acids, about 10 amino acids or any fragment in between of the full-length protein.
[00102] "Variant" as the term is used herein, can be a polynucleotide or polypeptide that differs from a reference nucleic acid or protein (i.e., SEQ ID NOs 1-128), but may retain essential properties (i.e., biological activity or conserved domains). A typical variant of a polynucleotide differs in nucleotide sequence from another, reference polynucleotide. Changes in the nucleotide sequence of the variant may or may not alter the amino acid sequence of a polypeptide encoded by the gene or sequence including or affected by the reference
polynucleotide. Nucleotide changes may result in amino acid substitutions, additions, deletions, fusions and truncations in the polypeptide encoded by the reference sequence, as discussed below. Generally, differences are limited so that the sequences of the reference polypeptide and the variant are closely similar overall and, in many regions, identical. Variant polynucleotides can include polynucleotides having at least 70% identity, at least 80% identity, at least 90% identity, at least 95% identity, at least 96% identity, at least 97% identity, at least 98% identity or at least 99% identity to the reference nucleotide sequence of the gene.
[00103] Variant polypeptides can include any polypeptide having an amino acid residue sequence substantially identical to a sequence specifically shown herein in which one or more residues have been conservatively substituted with a functionally similar residue, and which
displays the ability to mimic essential properties of the reference protein. Variant polypeptides can include polypeptides having at least 70% homology, at least 80% homology, at least 90% homology, at least 95% homology, at least 96% homology, at least 97% homology, at least 98% homology or at least 99% homology to the reference protein sequence.
[00104] In another embodiment, the compositions can include vectors to modulate expression of the gene. In an exemplary embodiment, the vector can include a full-length, a portion or fragment of, or variant of at least one of the nucleic acid sequences found in SEQ ID NOs 1-128. The vector can also be a viral vector, such as adenoviral vectors, adeno-associated viral vectors, retroviral vectors (including lentiviral vectors), alphaviral vectors (e.g., Sindbis vectors), and herpes virus vectors. The vector can also include an inducible promoter. The inducible promoter can be inducible through response to a regulator, such as cellular conditions, inducer molecules or stimuli. Regulatable promoters include inducible promoters, which are usually "off," but which may be induced to turn "on," and "repressible" promoters, which are usually "on," but may be turned off. Many different regulators are known to effect control over the activity of regulatable promoters, including temperature, hormones, growth factors, cytokines, heavy metals, and regulatory proteins. In one embodiment, the promoter can be inducible through exposure to an energy source. In another embodiment, the promoter can be inducible through exposure to light.
[00105] The compositions include a therapeutic agent that may be administered in a variety of forms. These include, for example, liquid, semi-solid and solid dosage forms, such as liquid solutions (e.g., injectable and infusible solutions), dispersions or suspensions, tablets, pills, powders, liposomes and suppositories. An exemplary form will depend on the intended mode of delivery and therapeutic application. Typical therapeutic agents are in the form of injectable or infusible solutions, such as therapeutic agents similar to those used for passive immunization of humans. Another mode of delivery is parenteral (e.g. , intravenous, subcutaneous,
intraperitoneal, intramuscular). In one embodiment, the therapeutic agent is delivered by intravenous infusion or injection. In another embodiment, the therapeutic agent is delivered by intramuscular or subcutaneous injection. In another embodiment, the therapeutic agent is delivered perorally. In yet another embodiment, the therapeutic agent is delivered to a specific location using stereotactic delivery. In an exemplary embodiment, the therapeutic agent is
formulated for delivery to the target tissue selected from the group consisting of a brain, a spinal cord, a sympathetic nervous system, a parasympathetic nervous system, an enteric nervous system, a gastrointestinal tract and a pancreas.
[00106] Therapeutic compositions typically must be sterile and stable under the conditions of manufacture and storage. The composition can be formulated as a solution, microemulsion, dispersion, liposome, or other ordered structure suitable to high drug concentration. Sterile injectable solutions can be prepared by incorporating the vector in the required amount in an appropriate solvent with one or a combination of ingredients enumerated above, as required, followed by filter sterilization.
[00107] The composition can be administered by a variety of methods known in the art. As will be appreciated by the skilled artisan, the route and/or mode of administration will vary depending upon the desired results. In certain embodiments, the therapeutic agent may be prepared with a carrier that will protect the agent against rapid release, such as a controlled release formulation, including implants, transdermal patches, and microencapsulated delivery systems. The carrier may also target delivery to at least one of a brain, a spinal cord, a sympathetic nervous system, a parasympathetic nervous system, an enteric nervous system, a gastrointestinal tract and a pancreas.
[00108] Carriers can be made of biodegradable, biocompatible polymers, such as ethylene vinyl acetate, polyanhydrides, polyglycolic acid, collagen, polyorthoesters, and polylactic acid. Many methods for the preparation of such formulations are generally known to those skilled in the art. See, e.g., Sustained and Controlled Release Drug Delivery Systems, J.R. Robinson, ed., Marcel Dekker, Inc., New York, 1978. The compositions may include a "therapeutically effective amount" to modulate expression of the gene(s). A "therapeutically effective amount" refers to an amount effective, at dosages and for periods of time necessary, to achieve the desired therapeutic result, such as gene expression modulation. The therapeutically effective amount may vary according to factors such as the disease state, age, sex, and weight of the individual, and the ability of the treatment to elicit a desired response in the individual. A therapeutically effective amount is also one in which any toxic or detrimental effects of the treatment are outweighed by the therapeutically beneficial effects.
[00109] Dosage regimens may be adjusted to provide the optimum desired response (e.g., a therapeutic or prophylactic response). For example, a single bolus may be administered, several divided doses may be administered over time or the dose may be proportionally reduced or increased as indicated by the exigencies of the therapeutic situation. It is especially
advantageous to formulate parenteral compositions in dosage unit form for ease of administration and uniformity of dosage. Dosage unit form as used herein refers to physically discrete units suited as unitary dosages for the mammalian subjects to be treated; each unit containing a predetermined quantity of active compound calculated to produce the desired therapeutic effect in association with the required pharmaceutical carrier. The specification for the dosage unit forms of the invention are dictated by and directly dependent on (a) the unique characteristics of the active compound and the particular therapeutic or prophylactic effect to be achieved, and (b) the limitations inherent in the art of compounding such an active compound for the treatment of sensitivity in individuals.
Bariatric Surgery and Alternative Metabolic Procedures
[00110] After analyzing for the presence or absence of genetic indicators or measuring expression of the gene(s), a determination of whether to perform a first metabolic procedure or a second metabolic procedure, which is different than the first metabolic procedure, can be made. For example, after analyzing for the presence or absence of genetic indicators or measuring expression of the gene(s), a determination of whether to perform a first metabolic procedure, such as a bariatric surgery, or a second metabolic procedure excluding bariatric surgery can be made.
[00111] Bariatric surgery includes procedures often referred to as metabolic surgery or therapy, as well as a variety of procedures performed in a subject that leads to a physiologic improvement in energy balance, nutrient utilization, or metabolic disorders. Surgical procedures to treat severe obesity or obesity-related conditions have included various forms of bariatric surgery, such as but not limited to, gastric bypass, Roux-en-Y gastric bypass (RYGB), biliopancreatic diversion, partial gastrectomy procedures such as vertical sleeve gastrectomy, adjustable gastric banding, duodenal switch, duodenojejunal bypass, vertical banded
gastroplasty, intragastric balloon therapy, greater curvature plication, gastric plication (including
anterior and anteroposterior plication) and other forms of gastric volume reduction, Magenstrasse and Mill, ileal transposition or interposition, small bowel transposition, biliary diversion, procedures involving anastomotic connections of the gastrointestinal tract (e.g., jejunoileostomy, etc.), gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, gastric electrical stimulation, small bowel electrical stimulation, vagal electrical stimulation, vagal electrical inhibition, and variations of the procedures above as well as other methods known by those skilled in the art. Such surgical procedures have increasingly been performed laparoscopically. Reduced postoperative recovery time, markedly decreased post-operative pain and wound infection, and improved cosmetic outcome are well established benefits of laparoscopic surgery, derived mainly from the ability of laparoscopic surgeons to perform an operation utilizing smaller incisions of the body cavity wall. Non-surgical procedures can include, but are not limited to, pharmacological and nutritional therapies, such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.; procedures including a device, such as gastric balloon
implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.; and/or the activation of brown adipose tissue. In one embodiment, the first metabolic procedure is a bariatric surgery. In one embodiment, the first metabolic procedure is a non-surgical procedure. In another embodiment, the second metabolic procedure is a non- surgical procedure. In another embodiment, the second metabolic procedure is a procedure different from the first metabolic procedure.
[00112] Different metabolic procedures, like bariatric surgery, can also produce similar end results, such as weight loss or amelioration of co-morbid conditions, by acting through similar mechanisms. Studies done by Chambers et al. in Gastroenterology 2011; 141(3):950-958, which is incorporated herein by reference in its entirety, have shown similar effects of vertical sleeve gastrectomy and gastric bypass on weight loss, food intake, insulin sensitivity, glucose tolerance, insulin secretion, endogenous glucose production, and glucagon-like peptide- 1 secretion. In addition, studies performed by Peterli et al. in Ann Surg 2009; 250(2):234-41, which is incorporated herein by reference in its entirety, have reproduced similar studies in humans showing that vertical sleeve gastrectomies and RYGB have similar effects on glucose
production, and glucagon-like peptide- 1 secretion. In particular, gastric bypass, biliopancreatic
diversion, sleeve gastrectomy and endoluminal sleeve have shown similar effects on weight loss, food intake, insulin sensitivity, glucose tolerance, insulin secretion, and endogenous glucose production. Moreover, bariatric surgical procedures have also shown similar effects on the gastrointestinal endocrine system. Levels of ghrelin, glucagon-like peptide- 1, peptide YY, amylin and gastric inhibitory polypeptide have shown similar changes in post-prandial secretion levels in individuals who have undergone gastric bypass, biliopancreatic diversion, sleeve gastrectomy, ileal interposition or duodenal endoluminal sleeve.
[00113] Some non-surgical examples of alternative metabolic procedures to bariatric surgery can include, but are not limited to, administering pharmacological and nutritional therapies, such as hormone and neuropeptide therapy, receptor agonists and antagonists, etc.; providing an alternative medical device based therapy, such as, but not limited to, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, etc.; and/or the activation of brown adipose tissue. (See US Pat. Pub. No. 2011/0263490 entitled "Diagnostic Methods And Combination Therapies Involving MC4R" filed December 29.2010, which is hereby incorporated by reference in its entirety.) The treatments can be temporary. By temporarily performing the treatments, assessment of the efficacy of the treatment can be made. Moreover, as the treatment can be temporary, and possibly reversible, evaluating the efficacy of the treatment can influence whether additional treatments need to be performed or if the treatment alone is sufficient to attain the desired weight loss and other clinical results.
[00114] Hormone and neuropeptide therapy can also be used to regulate or suppress appetite, increase body energy expenditure, and/ or decrease fat mass accumulation (McMinn, J. E., Baskin, D. G. & Schwartz, M. W., Obes. Rev. 2000; 1:37-46; Drazen, D. L. & Woods, S. C, Curr. Opin. Clin. Nutr. Metab. Care 2003; 6:621-629).
[00115] Activation of brown adipose tissue (BAT) can further lead to mobilization of fat stores within brown adipocytes to increase fat metabolism. The controlled activation of BAT can be optimized, leading to weight loss by reducing the stores of triglycerides in white adipose tissue (WAT).
[00116] BAT activation can occur either directly or transcutaneously. Either can stimulate the sympathetic nervous system to physiologically activate BAT. Whether BAT is activated directly and/or transcutaneously, target areas for BAT stimulation can include areas in the vicinity of BAT depots, e.g., the nape of the neck, over the scapula, alongside the spinal cord, and around the kidneys. Any BAT depot can be selected for activation. In the course of treating a patient, BAT nerves can be stimulated at any one or more BAT depots and can be stimulated
simultaneously, e.g., two or more BAT depots being concurrently stimulated, or stimulated sequentially, e.g., different BAT depots being stimulated at different times. Simultaneous stimulation of BAT can help encourage more and/or faster energy expenditure. Sequential stimulation of BAT can help prevent the "burning out" of target nerves and can help stimulate the creation of new BAT cells. Sequential nerve stimulation can include stimulating the same BAT depot more than once, with at least one other BAT depot being activated before activating a previously activated BAT depot.
[00117] Generally, direct activation of BAT can include implanting a device below the skin surface proximate to a BAT depot, e.g., within a BAT depot, and activating the device to deliver an electrical signal to the nerves innervating the BAT depot and/or to brown adipocytes directly. BAT itself is densely innervated, with each brown adipocyte being associated with its own nerve ending, which suggests that stimulating the BAT directly can target many if not all brown adipocytes and depolarize the nerves, leading to activation of BAT. The sympathetic nerves that innervate BAT can be accessed directly through standard surgical techniques, as will be appreciated by a person skilled in the art.
[00118] The electrical signal, whether transcutaneously or directly delivered to BAT, can be configured in a variety of ways. The stimulation "on" time amplitude can be higher for shorter periods and increased or decreased for longer periods of application. The electrical signal can have any "geometry" of the applied voltage, e.g., square waves, ramp waves, sine waves, triangular waves, and waveforms that contain multiple geometries. A transcutaneous device can be used to transcutaneously activate BAT through a variety of sizes, shapes, and configurations. Generally, the device can be configured to generate and/or deliver an electrical signal to tissue at predetermined intervals, in response to a manual trigger by the patient or other human, in response to a predetermined trigger event, or any combination thereof. In an exemplary
embodiment, the transcutaneous device can include an electrical stimulation patch configured to be applied to an external skin surface and to deliver an electrical signal to tissue below the skin surface, e.g., to underlying BAT.
[00119] Stimulation of BAT using an electrical signal is described in further detail in US Pat. Pub. No. 2011/0270360 entitled "Methods And Devices For Activating Brown Adipose Tissue Using Electrical Energy" filed December 29, 2010, and stimulation of BAT using other exemplary modes of stimulation are described in further detail in PCT Pat. App. No.
PCT/US11/66399 entitled "Methods And Devices For Activating Brown Adipose Tissue With Targeted Substance Delivery" filed December 21, 2011, PCT Pat. App. No. PCT/US 11/66358 entitled "Brown Adipocyte Modification" filed December 21, 2011, PCT Pat. App. No.
PCT/US 11/66409 entitled "Methods And Devices For Activating Brown Adipose Tissue With Light" filed December 21, 2011, and PCT Pat. App. No. PCT/US 11/66415 entitled "Methods And Devices For Activating Brown Adipose Tissue With Cooling" filed December 21, 2011.
[00120] The electrical signal, whether transcutaneously or directly delivered, can be configured in a variety of ways. The stimulation "on" time amplitude can be higher for shorter periods and increased or decreased for longer periods of application. The electrical signal can have any "geometry" of the applied voltage, e.g., square waves, ramp waves, sine waves, triangular waves, and waveforms that contain multiple geometries. A transcutaneous device can be used to transcutaneously activate BAT through a variety of sizes, shapes, and configurations. Generally, the device can be configured to generate and/or deliver an electrical signal to tissue at predetermined intervals, in response to a manual trigger by the patient or other human, in response to a predetermined trigger event, or any combination thereof. In an exemplary embodiment, the transcutaneous device can include an electrical stimulation patch configured to be applied to an external skin surface and to deliver an electrical signal to tissue below the skin surface, e.g., to underlying BAT.
Procedure Outcome Indicators
[00121] Indicators that predict outcomes after a metabolic procedure can also be measured and used in the methods disclosed herein. Such indicators can include genetic indicators and/or clinical measurements obtained from the patient. Examples of genetic indicators are described in
more detail in U.S. Prov. Pat. App. No. 61/704,434 entitled "Clinical Predictors of Weight Loss" filed on September 21, 2012, Atty. Dkt. No. 100873-572 (END7094USPSP), which is incorporated herein by reference in its entirety. Examples of clinical measurements can include, but are not limited to, pre-operative BMI, a glucose tolerance, bile acid profile, and body composition/fat distribution of the subject. Pre-operative BMI can be greater than 23 kg/m in non-Asians or greater than 21 kg/m in Asians. Individuals at a lower than "overweight" BMI may also be at risk of at least one weight-related comorbidity and therefore be applicable subjects to be treated or assessed by methods of this invention (e.g., Caucasians having a BMI of greater than 23 and Asians, a BMI of greater than 21). In some embodiments, pre-operative BMI can be greater than 25 kg/m in non-Asians or greater than 23 kg/m in Asians.
[00122] Additional non-limiting examples of indicators include, but are not limited to height, weight, gender, age, medical history and/or status, ethnicity, medical prescription history and/or status, types of previously received medical treatments for obesity (e.g., medications, BAT stimulation, gastric banding, gastric bypass, sleeve gastrectomy, etc), types of medical treatments previously received for health issues other than obesity (e.g., medications, surgical treatments, and non- surgical treatments), insurance information, diet information for the patient, and psychological history of the patient.
Predicting Bariatric Surgery Outcomes
[00123] Various systems and methods are provided for predicting metabolic therapy, e.g., metabolic and bariatric surgery, outcomes, i.e., a composite predictive model. The systems and methods can also provide predictions for non-surgical metabolic and bariatric treatments. In general, a user, e.g., a patient, a medical professional involved with treating a patient, a medical student, a hospital administrator, a health insurance administrator, etc., can receive predictive outcomes of multiple metabolic therapies that could be performed on a patient. The collection of therapies for the treatment of obesity and metabolic disease (e.g., diet and exercise,
pharmaceutical therapy, medically supervised therapy), metabolic surgery (open, laparoscopic, natural orifice, etc.), bariatric surgery (open, laparoscopic, natural orifice, etc.) are collectively defined herein as metabolic therapies. In one embodiment, a user can electronically access a metabolic therapy outcome prediction system, e.g., using one or more web pages. The system
can provide predictive outcomes of one or more different metabolic therapies, such as bariatric surgeries, for the patient based on data gathered from the user and on historical data regarding outcomes of the different bariatric surgeries. The system can additionally provide predictive outcomes for not having any treatment and/or a comparison of the predictive outcomes of the one or more different bariatric surgeries to the predictive outcomes for not having any treatment or for having non-surgical treatment. Generally, the predictive outcomes provided by the system can include a potential clinical metabolic outcome of each of the different bariatric surgeries, e.g., a predicted amount of weight loss, a predicted amount of body mass index (BMI) reduction, an improvement in a health condition associated with a metabolic disease, an associated risk of complications from the treatment, and/or an associated cost of the surgery and post-operative care. The predictive outcomes can be based on a plurality of patient- specific characteristics, e.g., age, weight, height, BMI, ethnicity, medical prescription history and/or status, genetic data (e.g., a genetic indicator), gene expression profiles (expression of one or more genes, expression over a time period and/or in different tissues), types of previously received medical treatments for obesity (e.g., gastric banding, gastric bypass, sleeve gastrectomy, etc), medical history and/or status, gender, etc. The predictive outcomes can also be based on historic results of the different types of bariatric surgeries on other patients. The predictive outcomes can thus be based at least in part on data specific to the patient and not just on historical data, e.g., data gathered by the user from previous personal experience, friends or colleagues, journal articles, internet research, clinical data, etc. The outputs can thus be personalized to the patient. The system can help the user be more informed about which of the bariatric surgeries would be most effective if performed on the patient, help specifically compare and contrast the different bariatric surgeries, and help the user decide which of the different bariatric surgeries, if any, to pursue for the patient. The system can therefore help maximize effectiveness of treatment for the patient by allowing a most effective option to be identified and pursued by the patient and/or by medical practitioner(s) treating the patient. The system can also help inform the user about bariatric surgery options that they might not have been aware of at all, e.g., new procedures, and/or deepen understanding of bariatric surgery procedures previously known to the user. The system can be configured to allow the user to save the predictive outcomes, which can then be accessed at a later date/time by the user and/or one or more other users, e.g., the user's surgeon, the user's
endocrinologist, the user's primary care physician, or other healthcare providers, etc., to which the user grants access to the saved data.
[00124] Methods and systems for providing predictive outcomes are described in more detail in U.S. Prov. Pat. App. No. 61/704,077 entitled "Systems and Methods for Predicting Bariatric Surgery Outcomes" filed on September 21, 2012, Atty. Dkt. No. 100873-610
(END7094USPSP1)), which is incorporated herein by reference in its entirety.
[00125] Output results can be reported in multiple ways, either individually or simultaneously via the system. In one embodiment, output results can be reported in parameters such as, but are not limited to, target weight loss in pounds or kilograms, target weight, percent excess body weight loss, percent weight change, percent change in BMI. In another embodiment, output results can be reported as continuous or at various cutoff points ranging from 1-100%. An example of various cutoff may include achieving at least or at most 50% excess weight loss. Another example of various cutoff may include achieving at least or at most 70% excess weight loss. In yet another embodiment, the output results can be reported as results obtained at various timepoints post metabolic procedure such as bariatric surgery or alternative metabolic procedure without bariatric surgery. Timepoints can include 1, 3, 6, 9, 12, 18, 24, 36, 48, 72, 84, 96, 108, 120 months post treatment or any number of months in between. In another embodiment, the output results can be reported as nadir weight. "Nadir weight" as used herein is defined as the lowest weight achieved at least 10 months after surgery without coexisting debilitating illness, with or without use of weight lowering medications.
[00126] The input parameters can be analyzed via the interface in a model algorithm. The algorithm can apply univariate analyses, multivariable regression analyses, advanced regression analyses, and other data mining techniques on multiple data sets to build, train and prospectively model predicted results after metabolic procedure such as bariatric surgery or alternative metabolic procedure without bariatric surgery.
[00127] The interface can also be used to output varying levels of confidence of the prediction on the results after metabolic procedure such as bariatric surgery or alternative metabolic procedure without bariatric surgery. Such examples can include the predicted result based on variable changes in weight, e.g., 20% chance of 40 lb change in weight, 40% chance of 201b
change in weight, etc. The output can further include predictions based on complications associated with a metabolic procedure such as bariatric surgery or an alternative metabolic procedure without bariatric surgery.
[00128] The output results can be collected and used by patients, primary care providers, and/or other referring physicians or other healthcare providers. The information can be provided in the patient's home, during a health care provider seminar, during a physician's office visit, and/or prior to treatment. Moreover, the interface can be accessed through various routes. In one embodiment, the interface can be accessed via the internet to record and model the patient information. In another embodiment, the interface can be accessed via a mobile device or "app," software application designed specifically for mobile or handheld devices. In yet another embodiment, the interface can be accessed via application software that can be installed on a computer or other device.
[00129] In addition to providing predictive outcomes, the system can optionally provide educational information regarding each of the different bariatric surgeries and/or other types of information related to bariatric surgery such as estimated patient monetary cost (based on one or more factors such as the patient' s insurance carrier, similar procedures performed in the patient' s geographic location, etc.), estimated insurance reimbursement (based on one or more factors such as the patient's insurance carrier, similar procedures performed in the patient's geographic location, etc.), estimated length of post-surgery hospital stay (based on one or more factors such as similar procedures performed in the patient's geographic location, the patient's age, the patient's other health conditions or disorders, etc.). The system can therefore help the user be more fully informed about the various risks and benefits of the various bariatric surgeries before deciding which of the bariatric surgeries to pursue, if any. Applying similar modeling techniques, personalized predictions can be provided for use of one or more of the preceding educational and/or other information.
[00130] One skilled in the art will appreciate further features and advantages of the invention based on the above-described embodiments. Accordingly, the invention is not to be limited by what has been particularly shown and described in the examples or figures, except as indicated
by the appended claims. All publications and references cited herein are expressly incorporated herein by reference in their entirety.
EXAMPLES
Example 1: Genetic Analysis Materials and Methods
[00131] Study Population: To identify genetic factors contributing to weight loss after RYGB, an exploratory genome- wide association study of individuals of European descent undergoing RYGB was performed. The study was approved by and performed in accordance with the guidelines of the Human Studies Committee at the Massachusetts General Hospital. From February 2000 until April 2007, consent was obtained from 1018 (97%) of MGH Weight Center patients undergoing RYGB to collect and extract DNA from tissue samples removed at the time of surgery. Intraoperative liver, subcutaneous fat, omental fat, and stomach tissues were collected in RNAlater (Amnion/ Applied Biosystems) and stored at -80°C. Operations were either open (41%) or laparoscopic (59%) RYGB. For the open procedure, the stomach was partitioned but not divided, and for the laparoscopic procedure the pouch was partitioned and divided from the remaining stomach. Otherwise, the techniques were the same, with an approximately 30 ml pouch, a 100-120 cm Roux (alimentary) limb fashioned in a retrocolic, retrogastric configuration, and a pancreaticobiliary limb extending approximately 75 cm beyond the ligament of Treitz.
[00132] Demographic and clinical information was extracted from review of the electronic medical records. Weight nadir was defined as the lowest weight achieved at least 10 months after surgery. Chart-derived nadir weight was validated through telephone interviews in a subset of patients (n=306); there was a 97% correlation between these two sources. Percent weight loss (%WL) at weight nadir was calculated by subtracting the patient's weight at nadir from his or her presurgical weight, and then dividing by the patient' s presurgical weight.
[00133] The following materials and methods apply to Examples 2 through 8:
[00134] Surgical procedures: For the open procedure, the stomach was partitioned but not divided, and for laparoscopic procedure the pouch was partitioned and divided from the remaining stomach. Otherwise, the techniques were the same, with an -30 ml pouch and a 100-
120 cm Roux limb fashioned in a retrocolic, retrogastric configuration, and the pancreaticobiliary limb extending -75 cm from the ligament of Treitz.
[00135] DNA analysis: Genomic DNA was extracted from collected liver samples, and genotyping was performed using the Illumina HumanHap 650Y BeadChip array (Illumina Inc., San Diego, CA). Race was genetically determined by principal component analysis using EIGENSTRAT; there was 97% concordance with self -reported race. Patients were excluded if they were on weight-lowering medications after surgery (1.7%), had cancer or other severe illness (including severe postoperative complications or reoperations; 2.4%), their DNA was not available (4.7%), or their postoperative body mass index (BMI) at least 10 months after RYGB could not be determined (7.9%). Using identity-by-descent methods (PLINK software), we identified 13 first-degree relative pairs, defined as pairs of individuals who share approximately 50% of their genetic variation, six second-degree relative pairs (-25% of genetic variation shared) and four third-degree relative pairs (-12.5% of genetic variation shared). An additional eight patients who were genetically related to established first-degree pairs were excluded, leading to a final sample of 848 (83.3%). Then the samples were matched on genetically identified race, randomly paired 794 unrelated individuals from the cohort, and compared for the similarity in their weight loss outcomes after surgery. Also identified were 20 cohabitating individuals by review of the medical records of all patients who had undergone RYGB at this center. No cohabitating individuals were genetically related.
[00136] Endpoint and covariate assessment: Demographic and clinical information was extracted from the medical record. A patient's weight nadir was identified, defined as the lowest weight achieved at least 10 months after surgery without coexisting debilitating illness or use of weight lowering medications. The percent excess body weight lost (EBWL) at weight nadir was calculated by subtracting the patient's nadir BMI from his or her preoperative BMI and dividing this difference by the difference between the patient's initial BMI and the upper normal BMI of 25 kg/m . Chart-derived weights were validated via telephone interviews in a subset of patients (n = 306); there was a 97% concordance between these two sources.
[00137] Statistical analyses: The average difference in outcome was calculated by pair, and analyses based on these mean differences were based on one entry per pair. Wilcoxon rank sum
tests were used to test differences in mean response between groups. Linear mixed effects models were constructed to determine the intraclass correlation coefficients (ICC) by type of relationship. All nongenetic analyses were performed using SAS statistical software (SAS Institute, Cary, NC).
[00138] The following materials and methods apply to Example 9:
[00139] Genotyping and Data Cleaning of Study Population: Samples were shipped to the Rosetta Inpharmatics Gene Expression Laboratory (Seattle, WA) where genomic DNA was extracted from liver samples. Nine hundred fifty samples were successfully genotyped using the Illumina HumanHap 650 Y BeadChip array (Illumina Corp, San Diego, CA). Data were converted to PLINK format (Hatoum, I. J., Stein, H. K., Merrifield, B. F. & Kaplan, L. M., Capacity For Physical Activity Predicts Weight Loss After Roux-En-Y Gastric Bypass, Obesity (Silver Spring) 17, 92-99 (2009)), and all genetic analyses were performed using this software. Using identity-by-descent (IBD) coefficients for all pairs of individuals, 36 related individuals were identified, defined as an IBD coefficient >0.125. One person per family was included for analysis, based on completeness of phenotypic and genetic information. In addition, one person was removed from the analysis because >10 of the person's genetic information was missing. Of the remaining 933 individuals, 806 self-identified as European. To address population structure not captured through self-identification, EIGENSTRAT (Hatoum, I. J. et al. Heritability Of The Weight Loss Response To Gastric Bypass Surgery, / Clin Endocrinol Metab 96, E1630- 3 (2011)) was used to calculate principal components of ancestry, and identified 25 outlying samples (greater than six standard deviations) for a sample of 781 patients. Of these 781 samples, 693 had a weight nadir value, were not on weight-lowering medications after surgery, did not have cancer or other severe illness, and were thus included in the final data set.
Imputation of 1,674,205 additional SNPs was performed using MACH software. (Ochner, C. N. et al,. Selective Reduction In Neural Responses To High Calorie Foods Following Gastric Bypass Surgery, Ann. Surg. 253, 502-507 (2011).) A SNP was excluded from analyses if it was missing in >10 of the samples, if it had less than 1% minor allele frequency, or if it was not in Hardy- Weinberg equilibrium, resulting in a SNP set of 1,943,373 SNPs. A genomic control inflation factor of 1.01 was observed, indicating minimal inflation of test statistics due to population stratification (Figure 1).
[00140] Gene Expression Profiling: Total RNA was extracted from liver, subcutaneous fat, and omental fat tissues. Liver, subcutaneous fat and omental fat RNA was amplified and converted to fluorescently labeled cRNA that was hybridized to custom 44K DNA
oligonucleotide microarrays from Agilent Technologies (Santa Clara, CA, USA). A detailed description of the normalization and data cleaning methods has been described previously. (Shin, A. C, Zheng, H., Pistell, P. J. & Berthoud, H.-R., Roux-En-Y Gastric Bypass Surgery Changes Food Reward In Rats, Int J Obes (Lond) 35, 642-651 (2011).) 707, 870, and 916 samples were profiled from liver, subcutaneous fat, and omental fat, respectively.
[00141] Replication Cohort: From May 2007 until October 2009, we obtained consent from 369 Caucasian MGH Weight Center patients undergoing RYGB to collect and extract DNA from tissue samples removed at the time of surgery. Intraoperative liver tissue samples were collected in RNAlater (Amnion/ Applied Biosystems) and stored at -80°. Operations were as described for the GWAS cohort. Clinical traits were extracted from the electronic medical records, as described for the GWAS cohort.
[00142] Genotyping and Data Cleaning of Replication Cohort: Samples were shipped to the Eli and Edythe Broad Institute (Cambridge, MA) where genomic DNA was extracted from liver samples. Three hundred sixty-nine samples were successfully genotyped using Sequenom MassARRAY (Sequenom Inc., San Diego, CA). Of these, 327 had a recorded weight nadir value, were not on weight-lowering medications after surgery, did not have cancer or other severe illness, and were thus included in the final data set.
[00143] Endpoint and Covariate Assessment: Demographic and clinical information was extracted from review of electronic medical records. Weight nadir was defined as the lowest weight achieved at least 10 months after surgery. Chart-derived nadir weight was validated through telephone interviews in a subset of patients (n=306); there was a 97% correlation between these two sources. Percent weight loss (%WL) at weight nadir was calculated by subtracting the patient's weight at nadir from his or her presurgical weight, and then dividing by the patient's presurgical weight. Percent excess body weight loss (%EBWL) was calculated by subtracting the patient's current weight from the patient's presurgical weight, and dividing this
difference by the difference between the patient's presurgical weight and the patient's ideal or target weight.
[00144] Animal Studies: All experiments in mice were performed in compliance with and were approved by the Institutional Animal Care and Use Committee of the Massachusetts General Hospital. We have developed a mouse model of RYGB that closely mimics the procedure in humans. At 12 weeks of age, male, diet-induced obese C57BL/6 mice on a high fat diet from weaning (Jackson Laboratories, Bar Harbor, ME) were randomized to RYGB, sham operation with post-operative ad libitum food intake, or sham operation with food restriction to match the weights of the RYGB mice weekly. In the RYGB procedure, the stomach was divided into a gastric pouch and distal stomach using a vascular clip (Ethicon Endo-Surgery, Inc., Cincinnati, OH). For each of the Roux (alimentary) and biliopancreatic limbs, the length of the intestine was 6 cm, approximating the 12-15% instestinal bypass used in the human operation. The alimentary limb was then secured to the gastric fundus by a gastrojejunal anastamosis. Sham operations consisted of a laparotomy and repair. Mice were maintained on a high-fat diet (D12492 diet; Research Diets, New Brunswick, NJ) except during the 7-14 days after surgery, when all mice were maintained on a postoperative protocol that progressed from water only to liquid diet to solid diet. Animals were individually housed in a 12-hour light, 12-hour dark cycle under controlled temperature and humidity conditions.
[00145] Animals were euthanized by carbon dioxide inhalation followed by cervical dislocation at 10 weeks after surgery. All tissues were harvested immediately, flash frozen and stored at -80°C until further processing. For gene expression studies, total RNA was extracted using Superscript® III First-Strand Synthesis System for RT-PCR kit (Invitrogen, Carlsbad CA), according to the manufacturer's instructions. One μg of total RNA was used as template for cDNA synthesis using TaqMan® Gene Expression Master Mix kit (Applied Biosciences, Carlsbad CA), according to the manufacturer's instructions. Relative expression level was determined by qPCR using pre- optimized, gene-specific primer probe sets purchased from Applied Biosciences for AQP11 (Mm00613023_ml; Cat# 4331182), SLC03A1
(Mm00452449_ml; Cat# 4331182), CLNS1A (Mm00445821_ml; Cat# 4331182) and ST8SIA2 (Mm01311039_ml; Cat# 4331182) and a CFX96™ Real-Time PCR Detection System
(BioRad:, Hercules, CA). All expression level data was presented relative to actin.
[00146] Tissue Samples: Intraoperative liver, subcutaneous fat, omental fat, and stomach tissues were collected in RNAlater (Amnion/ Applied Biosystems) and stored at -80 °C.
Operations were either open (41%) or laparoscopic (59%) RYGB. For the open procedure, the stomach was partitioned but not divided, and for the laparoscopic procedure the pouch was partitioned and divided from the remaining stomach. Otherwise, the techniques were the same, with an approximately 30 ml pouch, a 100-120 cm Roux limb fashioned in a retrocolic, retrogastric configuration, and a pancreaticobiliary limb extending approximately 75 cm beyond the ligament of Treitz.
[00147] Gene Expression Profiling: Total RNA was extracted from liver, subcutaneous fat, and omental fat tissues. Liver, subcutaneous fat and omental fat RNA was amplified and converted to fluorescently labeled cRNA that was hybridized to custom 44K DNA
oligonucleotide microarrays from Agilent Technologies (Santa Clara, CA). A detailed description of the normalization and data cleaning methods has been described previously. Successful profiling of 707, 870, and 916 samples from liver, subcutaneous fat, and omental fat, respectively, was performed.
Example 2: Genetic Analysis
[00148] Preoperatively, patients in this cohort had an average BMI of 50.2+8.6kg/m2, an average age of 44.7+11.3 yr, and were 74.8% female and 86% Caucasian. These characteristics were similar among the different groups studied (see Table 1).
Table 1: Patient demographics at baseline by type of relationship.
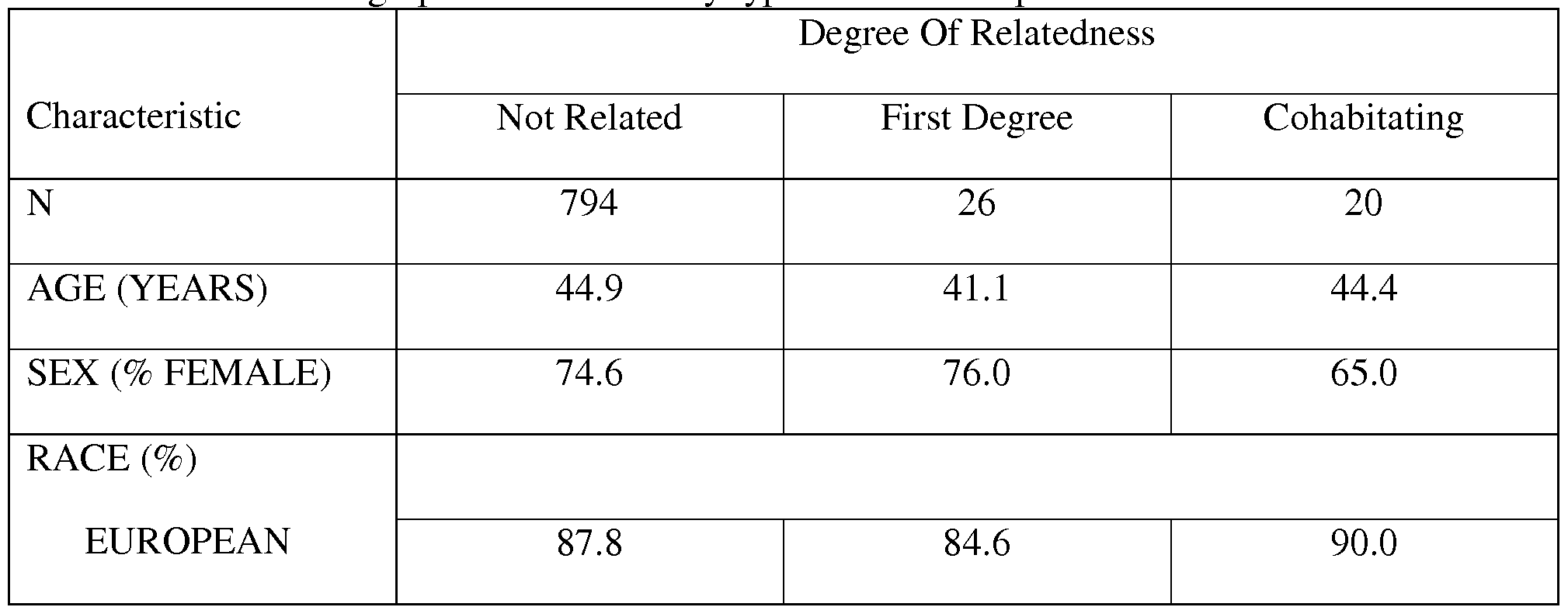
BLACK 4.4 7.7 0
[00149] After RYGB, patients lost an average of 119.2 + 41.7 pounds at weight nadir, corresponding to an EBWL of 79.7+21.8%; the population pattern of percent excess weight loss follows the wide and normal distribution observed previously (Figure 1).
[00150] To determine whether there is a genetic component to the variation in weight loss after surgery, weight loss after RYGB within pairs of genetically related was compared to genetically unrelated individuals. Unrelated individuals demonstrated far less similar weight loss after surgery than first-degree relatives (Figure 2), with an average difference in EBWL of 25.4% in unrelated individuals and 9.9% in first-degree relatives (P = 0.001). Because the observed similarity in weight loss could result primarily from shared environmental influences, weight loss within pairs of individuals who were living together but who are genetically unrelated was compared. Pairs of these environmentally related controls had a shared response similar to completely unrelated individuals (mean 26.1% difference in EBWL; P = 0.60), a response that was substantially different from that of first-degree relatives (P = 0.005). The small number of second- and third-degree relative pairs in this cohort precludes statistical analysis of these groups.
[00151] The ICC represents the portion of total variation in outcome explained by the pair relationship. Using mixed-effects models adjusted for age, sex, year of surgery, and preoperative BMI, the ICC were 70.4% for first-degree relatives (P = 0.02), 14.3% for environmentally related controls (P = 0.67), and 0.9% for randomly paired individuals (P = 0.48). Because preoperative BMI is strongly associated with postoperative percent EBWL, we additionally matched the unrelated controls based on 5-kg/m2-wide BMI groups to mimic the distribution of differences in preoperative BMI between first-degree relatives. After this adjustment, first degree relative pairs still demonstrated significantly less difference in weight loss compared with the unrelated controls (difference in EBWL for unrelated pairs 22.3+17.9%; P = 0.01 vs. first- degree relatives). Thus, first-degree relatives have weight loss outcomes after surgery that closely and significantly resemble each other, a characteristic not shared by environmentally
related (cohabitating) controls or randomly paired individuals. Similar results were seen when men and women were examined separately (data not shown).
Example 3: Reporting Methods Materials and Methods
[00152] Study Population: Participants were recruited from the population of patients undergoing RYGB at a single academic center that is part of a larger 13-hospital network in the Boston metropolitan area. From February 2000 until April 2007, we obtained consent from 1018 (97%) of the patients undergoing RYGB at this center. Operations included both open and laparoscopic RYGB performed by one of two surgeons using the same operative techniques; the surgical methods have been described previously. This study was approved by the institutional review board of the Massachusetts General Hospital.
[00153] Endpoint and Covariate Assessment: Demographic and clinical information was extracted from the medical record. We indentified a patient' s weight nadir, defined as the lowest weight achieved at least 10 months after surgery without coexisting debilitating illness or use of weight-lowering medications. One-year weight was defined as the weight closest to 12 months from surgery, within the range of 10-14 months after surgery. Post- operative weights were available for 848 patients (83.3%). Chart-derived nadir weights were validated by telephone interviews in a subset of patients (n=306); there was a 94% concordance between these two sources. Diabetes diagnosis was extracted from patient charts and defined as the documentation of diabetes, a fasting glucose measurement > 126 mg/dL, or the use of diabetes medication (insulin or metformin).
[00154] Weight loss was characterized at one year and at weight nadir using seven different metrics (Table 2). Residuals were calculated by regressing postoperative BMI (the dependent variable) on preoperative BMI (the independent variable) and outputting the residuals from this model. Because residuals derived from regressing postoperative BMI on preoperative BMI represent, by definition, postoperative BMI independent of preoperative BMI, these residuals were used as the benchmark of independence from preoperative BMI. Weight loss characterized by number of pounds lost was calculated by subtracting the patient's final weight from his or her baseline weight. As BMI is a function of weight and height, and height is almost always stable over the course of a weight loss study, BMI and pounds lost are closely similar methods for
measuring weight loss. Percent weight change was calculated by dividing the absolute pounds lost by the patient's initial weight, and is statistically interchangeable with percent BMI change. Percent EBWL was calculated by dividing the difference between initial BMI and final BMI by the difference between initial BMI and a "normal" BMI. A BMI of 25 kg/m is commonly used to represent the target, or upper limit of a "normal" BMI, but other standards, including race- specific BMI standards or other "ideal weights" according to the Metropolitan Life Insurance Company (MLIC) life tables, may also be used to represent "normal." In this study, EBWL was calculated as described above, using a reference BMI of 25 kg/m .
[00155] Statistical Analyses: Patients were divided into seven preoperative BMI (pBMI) groups (35-39.9, 40-44.9, 45-49.9, 50-54.9, 55-59.9, 60-64.9, 65+). Means for each weight loss metric were calculated for each pBMI group, and linear trends across the groups were assessed using a test for trend of the median value within each group. Correlations between pBMI and each continuous metric were assessed using Spearman correlations, and r measures were derived from linear regressions. All analyses were performed using SAS statistical software (SAS Institute, Cary, NC).
Example 4: Reporting Methods of Weight Loss
[00156] At baseline, participants had an average BMI of 50.0 (SD ± 8.3) kg/m , an average age of 44.7 (± 11.5) years, 74.3% were female and 26.2% had diabetes. One year after RYGB, patients lost an average of 17.1 kg/m , 34.2 % of baseline weight, and 71.7 % of excess body weight (Table 2). By weight nadir, which on average occurred 28.5 months after surgery, patients lost an average of 19.4 kg/m , 38.7 % of baseline weight, and 81.2% of excess body weight (Table 3).
Table 2: Different Parameterizations of Weight Loss.
Metric Abbreviation Formula
e = Observed Final BMI— Predicted Final BMI
Residuals Predicted BMI from the equation:
Final BMI = Initial BMI
Weight lost (in pounds or kg) Δ pounds, Δ kg Initial Weight(lbs or kgs) - Final Weight(lbs or kgs) Weight achieved (in pounds
Final Weight (lbs or kgs) or kg)
BMI units lost Δ BMI Initial BMI - Final BMI
BMI achieved Final BMI
Percent excess body weight Initial BMI - Final BMI
% EBWL * 100
Initial BMI - Ideal BMI
lost
Initial Weight - Final Weight
Percent weight change % WC * 100
Initial Weight
Attorney uocKei ΓΝΟ.: IUU»/J-03J ( i u vwtw

Table 3: Weight loss parameterizations by preoperative BMI group.
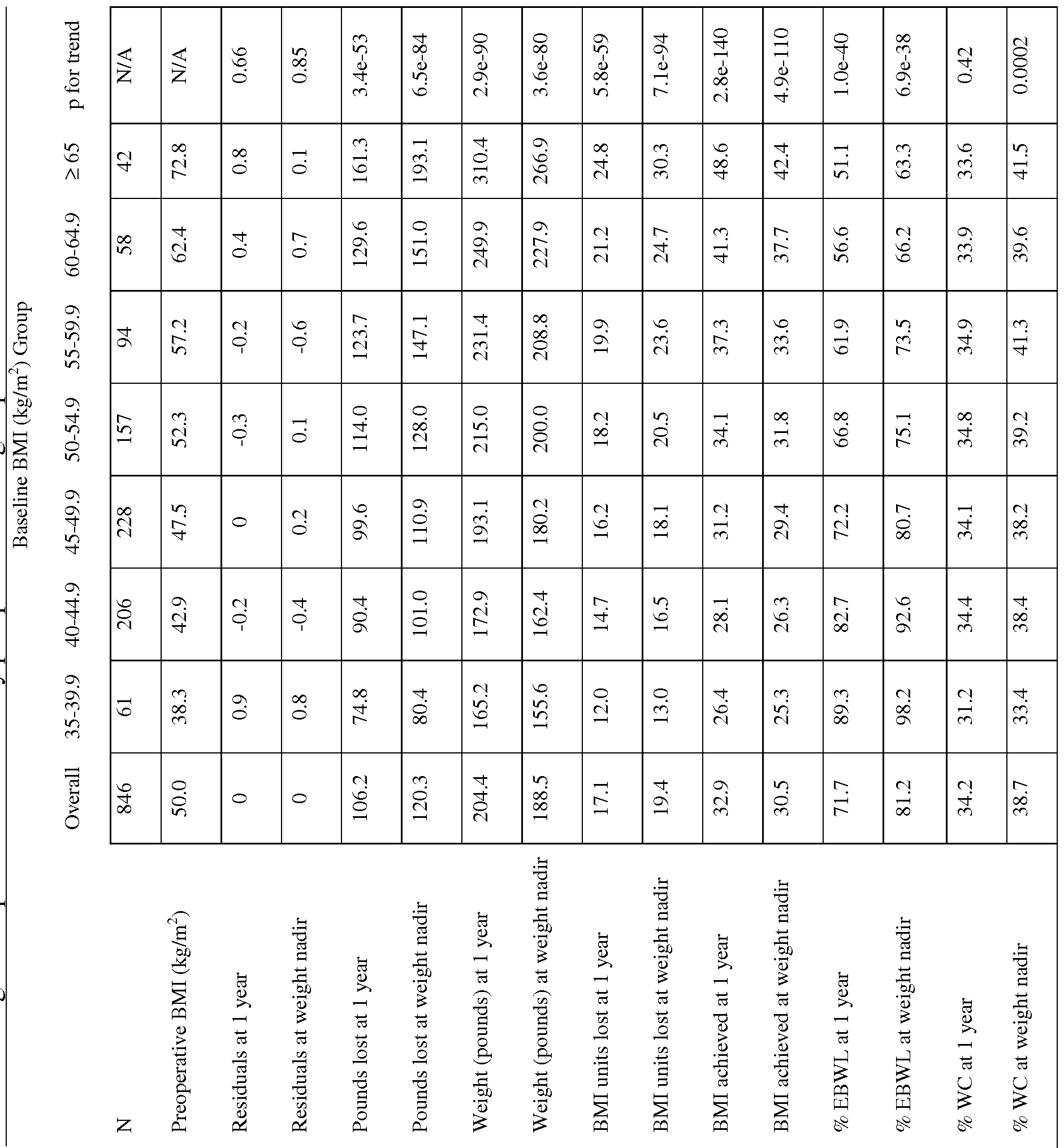
[00157] The residuals derived from regressing postoperative BMI on preoperative BMI showed no difference across pBMI groups (r=0, p=0.9 at both one year and weight nadir; Table 3, Figure 3). In contrast, there was a strong positive association between absolute change in weight (pounds lost or gained) and pBMI, with patients in lower BMI groups losing significantly less weight (rly = 0.52, ply = 3.4 * 10"53; rnadir = 0.54, pnadir = 6.5 * 10~84; Table 3, Figure 4).
[00158] The same pattern is observed when change in BMI, final attained weight, or final attained BMI is used (Table 3, Figures 3-7). When weight loss was characterized as EBWL, the opposite pattern was observed, with patients at a lower pBMI lose more EBWL at both 1 year and weight nadir (rly = -0.51, ply = 1.0 * 10"40; rnadir = -0.43, pnadir = 6.9 * 10~38; Table 3, Figure 8). In contrast, there was no association (rly = 0.04, ply = 0.52) between pBMI group and WC at one year, and a relatively weak association between pBMI and WC and weight nadir (rnadir = 0.13, pnadir = 0.003; Figure 9).
[00159] Similar patterns were seen when a continuous characterization of pBMI was used (Table 3). The number of pounds lost was strongly and positively correlated with pBMI at both one year (rSpearman=0.53, p = 4.3 * 10"46) and at weight nadir (rSpearman=0.55, p = 5.1 * 10"69); BMI units lost showed a similar pattern (Table 3). EBWL was strongly negatively correlated with pBMI at both one year
 -0.45, p =
-0.45, p =
7.2 * 10 ). In contrast, WC was not associated with pBMI at one year (rS SpPeeaarrmmaann=" 0.04, p =
0.33) and was only weakly associated with pBMI at weight nadir (rspearman= 0.13, p = 0.0002). While pBMI explains a substantial proportion of the variability in number of pounds lost (r ly =
2 2 2
0.36, r nadir = 0.39) and EBWL (r ly = 0.25, r na(jir = 0.18), it explains only a small percentage of the variability in WC (r2 iy = 0.002, r2 nadir = 0.02).
[00160] The findings reflect the biology of weight loss after RYGB - to the extent that a higher pBMI represents a more severe form of obesity, severe obesity may "normalize" less completely after RYGB. A parallel can be drawn to other metabolic conditions, such as systolic blood pressure (SBP), where patients with more extreme levels of SBP are less likely to achieve a normal SBP and are more likely to need aggressive treatment with multiple antihypertensive treatments.
[00161] Conversely, in this study patients with a lower pBMI lost less absolute weight relative to those patients with a higher pBMI, thus appearing less "successful" if absolute pounds are chosen as the weight loss metric. Whether the association between the weight loss metric and preoperative BMI is observed for biological or artificial reasons, the results indicate a potential for confounding by preoperative BMI (hidden variables associated with BMI) when searching for novel predictors. While it may be possible to partly account for the effects of preoperative BMI through adjustment for preoperative BMI using statistical models, if a relationship between the potential predictor and preoperative BMI exists there will be the potential for collinearity, which can result in incorrect estimation of the effect size and standard error of the novel predictor. Thus, it is advantageous to utilize a weight loss metric that both minimizes the association with pBMI (unlike pounds lost or EBWL) and that is clinically interpretable (unlike the use of residuals).
Example 5: Genetic Factors Materials and Methods
[00162] Cohort 1: To identify genetic factors contributing to weight loss after RYGB, an exploratory genome-wide association study of Caucasian individuals undergoing RYGB was performed. From February 2000 until April 2007, consent was obtained from 1018 (97%) of Massachusetts General Hospital (MGH) Weight Center patients undergoing RYGB to collect and extract DNA from tissue samples removed at the time of surgery. Cohort 1 may also be described herein as the original cohort, the GWAS cohort, the training cohort, or the training set.
[00163] In addition, one person was removed from analyses due to >10% of genetic information missing. Of the remaining 933 individuals, 806 self-identified as Caucasian. To address population structure not captured through self-identification, EIGENSTRAT (Price, A. L. et ah, Nat. Genet. 38, 904-909 (2006)) was used to calculate principal components of ancestry, and identified 25 outlying samples (greater than six standard deviations) for a sample of 781 patients. Of these 781 samples, 693 had a weight nadir value, were not on weight- lowering medications after surgery, did not have cancer or other severe illness, and were thus included in the final data set. Imputation of 1,674,205 SNPs was performed using MACH software (Li, Y., Wilier, C. J., Ding, J., Scheet, P. & Abecasis, G. R., Genet. Epidemiol. 34, 816- 834 (2010)). A SNP was excluded from analyses if it was missing in >10% of samples, if it has
less than 1% minor allele frequency, or if it was not in Hardy- Weinberg equilibrium, resulting in a SNP set of 1,943,373 SNPs.
[00164] Genotyping and Data Cleaning of Cohort 1: Samples were shipped to Rosetta Inpharmatics Gene Expression Laboratory (Seattle, WA) where genomic DNA was extracted from liver samples. Nine hundred fifty samples were successfully genotyped using the Illumina HumanHap 650Y BeadChip array (Illumina Corp, San Diego, CA). Data were converted to PLINK format (Purcell, S. et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 81, 559-575 (2007)) and all genetic analyses were performed using this software. Using identity-by-descent (IBD) coefficients for all pairs of individuals, 36 related individuals were identified, defined as an IBD coefficient >0.125. One person per family was included for analysis, based on completeness of phenotypic and genetic information.
[00165] Cohort 2: From May 2007 until October 2009, consent was obtained from 369 Caucasian MGH Weight Center patients undergoing RYGB to collect and extract DNA from tissue samples removed at the time of surgery. Intraoperative liver was collected in RNAlater (Amion/ Applied Biosystems) and stored at -80°. Operations were as described for the Cohort 1. Clinical traits were extracted from the electronic medical records, as described for the GWAS cohort. Cohort 2 may also be described herein as the replication cohort, the test cohort, or the test set.
[00166] Genotyping and Data Cleaning of Cohort 2: Samples were shipped to the Eli and Edyth Broad Institute (Cambridge, MA) where genomic DNA was extracted from liver samples. Three hundred sixty-nine samples were successfully genotyped using Sequenom MassARRAY (Sequenom Inc., San Diego, CA). Of these, 327 had a weight nadir value, were not on weight- lowering medications after surgery, did not have cancer or other severe illness, and were thus included in the final data set.
[00167] Tissue Samples: Intraoperative liver, subcutaneous fat, omental fat, and stomach tissues were collected in RNAlater (Amion/ Applied Biosystems) and stored at -80 °C.
Operations were either open (41%) or laparoscopic (59%) RYGB. For the open procedure, the stomach was partitioned but not divided, and for the laparoscopic procedure the pouch was
partitioned and divided from the remaining stomach. Otherwise, the techniques were the same, with an approximately 30ml pouch, a 100-120 cm Roux limb fashioned in a retrocolic, retrogastric configuration, and a pancreaticobiliary limb extending approximately 75 cm beyond the ligament of Treitz.
[00168] Endpoint and Covariate Assessment: Demographic and clinical information was extracted from review of the electronic medical charts. Weight nadir was defined as the lowest weight achieved after surgery. Chart-derived nadir weight was validated through telephone interviews in a subset of patients (n=306); there was a 94% correlation between these two sources. Percent weight loss (%WL) at weight nadir was calculated by subtracting the patient's weight at nadir from his or her presurgical weight, and then dividing by the patient's presurgical weight. Percent excess body weight loss (%EBWL) was calculated by subtracting the the patient's current weight from the patient's presurgical weight, and dividing this difference by the difference between the patient's presurgical weight and the patient's ideal weight.
[00169] Gene Expression Profiling: Total RNA was extracted from liver, subcutaneous fat, and omental fat tissues. Liver, subcutaneous fat and omental fat RNA was amplified and converted to fluorescently labeled cRNA that was hybridized to custom 44K DNA
oligonucleotide microarrays from Agilent Technologies (Santa Clara, CA, USA). A detailed description of the normalization and data cleaning methods has been described previously.4 Successful profiling of 707, 870, and 916 samples from liver, subcutaneous fat, and omental fat, respectively, was performed.
[00170] Statistical Analysis: Each SNP was compared to %WL using linear regression in
PLINK. SNPs within a 250 kb window of each other with a r > 0.5 were not considered independent; only the strongest associated SNP for each block was considered for replication and follow-up analyses. Association results from the GWAS and replication cohorts were meta- analzyed. The association between rsl7702901 and gene expression in liver, subcutaneous fat, and omental fat was determined using Kruskal-Wallace tests with adjustment for the effect of surgery year, age, race, and gender using a principle components analysis. All genetic analyses were performed using PLINK. All non-genetic analyses were performed using SAS statistical software (SAS Institute, Cary, NC).
[00171] Animal Studies: All experiments in mice were performed in compliance with and were approved by the Institutional Animal Care and Use Committee of the Massachusetts General Hospital. We have developed a mouse model of RYGB that closely mimics the procedure in humans. At 12 weeks of age, mice with a C57BL/6 background (Jackson
Laboratories, Bar Harbor, ME) were randomized to RYGB, sham operation with post-operative ad libitum food intake, or sham operation with food restriction to match the weights of the RYGB mice weekly. In the RYGB procedure, the stomach was divided into a gastric pouch and distal stomach using a vascular clip (Ethicon Endo-Surgery, Inc., Cincinnati, OH). For each of the Roux and biliopancreatic limbs, the length of the intestine was 6cm, approximating the 12- 15% instestinal bypass in human RYGB. The Roux limb was then secured to the gastric fundus by a gastrojejunal anastamosis. Sham operations consisted of a laparotomy and repair. Mice were maintained on a high-fat diet (D 12492 diet; Research Diets, New Brunswick, NJ) except during the 7-14 days after surgery, when all mice were maintained on a postoperative protocol that progressed from water only to liquid diet to solid diet. Animals were individually housed in a 12 hour light, 12 hour dark cycle under controlled temperature and humidity.
[00172] At 10 weeks post-surgery, mice were sacrificed in a carbon monoxide chamber followed by cervical dislocation. Tissues were harvested immediately, flash frozen, and stored at -80°. Samples were shipped to Rosetta Inpharmatics Gene Expression Laboratory (Seattle, WA) where mRNA was extracted and converted to cDNA. Quantitative PCR was performed on genes of interest (to be expanded with primer and QC information as it becomes available).
Example 6: Genetic Factors Contributing to Weight Loss
[00173] To identify genetic factors contributing to weight loss after RYGB, an exploratory genome-wide association study (GWAS) of cohorts of 858 unrelated Caucasian individuals undergoing RYGB was performed. The individuals were grouped according to preoperative BMI (>40, 40-45, 45-50, 50-55, 55-60, 60-65, 65+) and percent change in weight can be found in Figure 10 and demographic information is shown in Table 4.
Table 4. Pre- and post-operative characteristics of the RYGB original and replication cohorts
Original Cohort Replication p-value
Cohort
Age (years; ± SD) 45.8 ± 11.2 47.1 ± 11.1 0.07
Preoperative BMI (mean kg/m ; ± SD) 50.3 ± 8.4 48.1 ± 8.5 0.0002
Sex (% female) 73.2 71.7 0.65
Diabetes (%) 40.2 41.5 0.19
BMI at weight nadir (mean kg/m ; ± SD) 30.6 ± 6.4 29.9 ± 6.0 0.32
%WL at nadir (%; ± SD) 39.0 ± 9.1 37.5 0.01
[00174] Single nucleotide polymorphisms (SNPs) in this cohort were genotyped using the Illumina HumanHap 650Y array. After implementing stringent quality control measures, 524,284 SNPs were available for analysis. To increase the coverage of genetic variants additional missing genotypes were imputed and applied to these imputed SNPs. The same quality control measures were performed on the genotyped SNPs. A total of 1,943,373 genetic markers were analyzed.
[00175] To minimize heterogeneity due to underlying population structure, the patients who self-identified as Caucasian using principle components analysis were analyzed. There was 97% concordance between self-identified and genetically-identified race, and only patients genetically determined to be Caucasian were included in analyses. Additionally, patients who were related, patients who had complete follow-up information, patients who were on weight- altering medications or had severe illness after surgery were excluded, leaving 693 patients (Cohort 1) for analysis. Figure 11 shows the percent change of weight nadir measured in Cohort 1.
[00176] Figure 12 shows the percent change of weight nadir measured in an independent cohort of 327 Caucasian RYGB patients (Cohort 2). One hundred and three marginally significant (P < 5 x 10"5) SNPs were identified (Figure 13; Table 5), representing 26 independent loci (pairwise r < 0.5) from Cohort 1. The top SNP per region was carried forward for validation in Cohort 2, 327 Caucasian RYGB patients (Table 5).
Table 5. Association results for 103 SNPs with p < 5.0x10 for nadir WL in the Cohort 1.
Distance from R2 with index
Index SNP Chr Position Other SNPs P-value index SNP (kb) SNP
rsl 051508 159753509 8.21e-08 rs7158359 88664048 3.36e-07 rs4904510 -1.28 1.0 5.4e-07 rs7129556 11 76977696 4.28e-07 rsl 1605638 -61 0.986 5.79e-06 rs 11823651 -46 0.997 1.6e-06 rs7481282 -36 1.0 8.64e-07 rsl 1237220 -31 0.997 5.41e-07 rsl0899387 -23 0.993 4.87e-07 rs20323951 14 1.0 6.51e-07 rs6592738 23 0.967 3.18e-06 rsl 0899394 24 0.961 4.26e-06 rsl 1237249 41 0.957 1.91e-06 rsl 1604207 67 0.71 2.5e-06 rsl 2286317 89 0.711 6.48e-06 rs7950873 113 0.709 4.29e-06 rs4344516 138 0.703 3.61e-05 rsl 0899404 163 0.696 2.95e-05 rs537811 168 0.696 2.95e-05 rs684813 195 0.691 3.86e-05 rs650171 198 0.696 2.34e-05 rs7123080 199 0.696 2.34e-05 rs4945220 228 0.695 2.29e-05 rs7951033 234 0.695 2.29e-05 rs7185923 16 49802988 8.08e-07 rs2994537 1 44650917 1.17e-06 rs934760 2 122002672 4.6e-06 rs6712661 -183 0.907 3.19e-05 rsl 2622908 -182 0.906 4.58e-05 rs735483 -181 0.908 3.19e-05 rsl 2615396 -176 0.908 3.19e-05 rsl 2615068 -171 0.907 4.58e-05 rs7601226 -171 0.908 3.19e-05 rsl 7006394 -168 0.907 4.58e-05 rsl3414513 -167 0.908 3.19e-05 rs9653407 -166 0.908 3.19e-05 rs7564564 -152 0.898 4.68e-05 rsl2711551 -123 0.917 3.22e-05 rsl 7006485 -79 0.902 3.1e-05 rs2164796 -67 0.918 3.35e-05 rs2118387 -67 0.918 3.35e-05 rsl 3000440 -49 0.918 3.35e-05 rs724403 -48 0.918 3.5e-05 rsl 3413270 -46 0.918 3.35e-05 rs6711921 -13 0.918 3.35e-05 rs9678017 2 0.918 3.35e-05 rs 10177322 4 0.918 3.47e-05 rs7580531 19 0.909 4.11e-05
rsl2711559 120 0.859 3.7e-05 rs 1104959 5 149722429 5.83e-06 rs9403832 6 147296219 9.77e-06 rs7383179 -6.69 1 9.77e-06 rs9322082 -2.17 0.985 1.37e-05 rsl 1155492 -0.453 0.985 1.37e-05 rs9403834 5 1 1.35e-05 rsl 1155494 5.34 1 1.35e-05 rs 1408577 12.6 0.98 1.93e-05 rs7742886 13.8 0.995 1.38e-05 rs4267966 17.7 0.956 4.74e-05 rs4452660 21.9 0.972 2.23e-05 rs4323329 22.3 0.972 2.23e-05 rs9377038 27.4 0.957 3.05e-05 rs7775644 47.8 0.667 2.11e-05 rs9322085 58.6 0.632 4.17e-05 rs6570781 58.8 0.6 3.13e-05 rs6902235 60.8 0.611 2.31e-05 rs7745042 66.9 0.6 2.18e-05 rs8032450 15 87573927 1.09e-05 rs 17702901 15 90731415 1.19e-05 rsl 7646351 -3.58 1 3.17e-05 rsl 7646434 0.93 1 2.38e-05 rsl 7702960 2.12 1 2.38e-05 rsl 7646492 3.45 1 3.21e-05 rs588217 11 77261024 1.36e-05 rs621456 -30.3 0.805 3.93e-05 rs4085813 -15.8 0.985 2.24e-05 rs648601 3.53 0.985 1.86e-05 rs6554217 4 55672161 1.49e-05 rs4450992 0.861 0.979 3.72e-05 rs9357419 6 12690973 1.79e-05 rs7744769 -1.12 1 4.29e-05 rs 11260025 19 7687753 2.21e-05 rs8111760 0.267 1 2.35e-05 rs7749399 6 96086077 2.39e-05 rs443673 5 3265963 2.62e-05 rs 12803675 11 49858702 2.74e-05 rsl3380914 18 69312767 2.94e-05 rsl954888 -8.71 1 4.08e-05 rsl 2968184 44.7 0.626 3.31e-05 rsl0518316 4 120241167 2.98e-05 rs6911409 6 73910091 3.52e-05 rs6911751 0.198 1 4.87e-05 rs4703388 5 34834358 3.92e-05 rsl6867581 1.58 1 3.92e-05 rsl 2659689 1.75 1 3.92e-05 rs 1952291 14 45410504 4.3e-05 rs 1289666 1 117350312 4.35e-05 rs 10242229 7 92996322 4.37e-05 rs2157814 1.37 1 4.73e-05
rsl 1788785 9 96111183 4.53e-05 rsl883264 22 41834344 4.59e-05 rsl 2696123 3 163099074 4.71e-05 rs2029600 -2.47 1 4.71e-05
[00177] The top SNP per region underwent validation in Cohort 2. Twenty-three mutations were determined using Sequenom MassARRAY, see Figure 14. The association between SNPs and percent total weight loss (%WL) at the lowest weight (weight nadir) after RYGB were analyzed using linear regression models. A genomic control inflation factor of 1.00 was observed, indicating there was no inflation of test statistics due to population stratification.
Results of the original and validation cohorts were meta- analyzed using fixed effects models.
[00178] Multiple regions on several chromosomes, such as chromosome 11, were found to have numerous SNPs or "clouds" of SNPs with signification association to percent total weight loss (%WL) at the lowest weight (weight nadir) after RYGB (Figure 15). Additionally, a SNP at 15q26.1, rsl7702901 was identified as being significantly associated with WL after RYGB
-8
(^replication = 0.002; Pmeta-anaiyzed = 7.4 x 10" ). The magnitude of effect was strikingly similar across the two cohorts, with betas of -6.70 and -6.52, respectively (Table 6).
Table 6: SNPs Associated with WC at Nadir.
Cohort 1 Cohort 2 Meta-Analyzed
SNP Chr p-value β p-value β p-value β rs7158359 14 3.361E-07 -3.029 0.6593 -0.4075 0.00000456 2.2731 rs7129556 11 4.276E-07 -2.803 0.441 -0.6013 0.000003866 2.073 rsl0899387 11 4.873E-07 -2.876 0.5991 4.336 rs934760 2 0.000004595 -4.276 0.68 0.5647 rsl 104959 5 0.000005829 7.748 0.6605 0.8592 0.0001832 4.7901 rsl 7702901 15 0.00001188 -6.703 0.002259 -6.524 7.439E-08 6.6422 rs588217 11 0.00001363 -2.547 0.4659 -0.5852 0.00006972 1.8713
rs9357419 6 0.0000179 -2.95 0.5694 0.5581 0.001292 1.8029
[00179] Because the physiological mechanisms of weight gain to generate obesity and weight loss after RYGB may be related, previously reported and validated BMI loci associated with weight loss after RYGB in humans were assessed. None of the 32 previously reported BMI loci was associated with weight loss after surgery, nor did loci previously reported to be associated with diabetes (Table 8).
Attorney uocKei ΓΝΟ.: IUU»/J-03J ( i u vwtw

Table 7. Association results for SNPs previously identified as associated with obesity.

Attorney uocKei ΓΝΟ.: IUU»/J-03J ( i u vwtw


[00180] After pooling data from the two cohorts (n=953), patients lacking the minor allele (MA) of rsl7702901 lost an average of 38.7% of their body weight, while patients carrying a single copy of this mutation (n=52, 5.0% of the population) lost an average of 33.5%. The sole patient with two copies of the MA had a percent weight loss of 28.8% (Figure 16).
[00181] To examine the potential predictive utility of this SNP for discriminating amongst patients, %WL was categorized as less than or greater than or equal to 30% at weight nadir (n=171, 17.9%), Figure 17. Patients with at least one copy of the MA were 2.54 times more likely to fall below 30% WL, than patients with no copies of the MA (P < 0.001)(left shaded area in Figure 18). Notably, no patients with this polymorphism lost more than 50% of his or her weight (corresponding to the upper 10% of the weight loss distribution) (right shaded area in Figure 18).
Example 7: Genetic Models
[00182] The predictive ability of this SNP was further tested by adding this marker to a clinical model for predicting weight loss after RYGB, Table 8. The model was constructed by selecting one or more SNPs that met specific p-value criteria and then using backward and stepwise regression. The coefficients for each variable were determined using the training population (Cohort 1) and then the genetic information was entered into a regression model to determine the improvement genetics has on weight loss predictions. In a multivariable model that included age, sex, preoperative BMI (pBMI), and diabetes as variables, the area under the receiver operating characteristic curve (AUROC) was calculated as 0.620. After inclusion of rsl7709201 in the model, the AUROC improved to 0.633 (Figure 19), showing that inclusion of rsl7709201 has a higher probability of being a predictor of weight loss than rsl7709201 as a random positive influence on weight loss.
Table 8: Model Performance.

[00183] To further demonstrate the predictive ability of incorporating genetic information with clinical data, multivariable models were tested by adding multiple SNPs to a clinical model for predicting weight loss after RYGB, Table 9. Variables for the clinical model included age, sex, diabetes, and preoperative BMI (pBMI). Variables for the genetic model included all of the variables in the clinical model with the addition of the following genetic variables: rsl 108723, rsl 1739371, rsl 1942914, rsl2425125, rsl7710780, rs2383289, rs3734399, rs4325727, rs4603757, rs6737079, rs6911751, rs6925786, rs9474779. Similar to the model with one SNP, the multi-SNP model was constructed by selecting multiple SNPs that met specific p-value criteria and then using backward and stepwise regression. For each model, coefficients for each variable were determined using the training population (Cohort 1). Validation that these coefficients are applicable to other data sets was assessed using Cohort 2 as a test set of data. Data from Cohort 2 was not used in establishing the coefficients and therefore serves as a valid test case. For the clinical multivariable model that included age, sex, diabetes, and preoperative BMI (pBMI) as variables, the AUROC score was calculated to be 0.665 in Cohort 1. The AUROC score in the test population, Cohort 2, showed significant similarity (0.699) and affirmed the performance of the model. For the genetic multivariable model that included clinical and genetic factors, the AUROC was significantly better (0.971) after determining the optimal coefficients to this model in the training set (Cohort 1). Using the genetic multivariable model with the coefficients derived from Cohort 1, the AUROC in the test set (Cohort 2) was also improved (0.795) over the respective AUROC scores based on clinical data alone, verifying that inclusion of multiple SNPs (rsl 108723, rsl 1739371, rsl 1942914, rsl2425125, rsl7710780,
rs2383289, rs3734399, rs4325727, rs4603757, rs6737079, rs6911751, rs6925786, rs9474779) significantly improves weight loss predictions.
Table 9: Model Performance.

[00184] To determine the potential biological function of this SNP, the presence of the MA associated with expression of any of -44,000 gene expression transcripts in liver, omental fat tissue, and subcutaneous fat tissue was examined. No obvious association between rs 17702901 and expression of other transcripts was found upon initial inspection, including expression of two genes located closest to rsl7702901 - ST8SIA2 (-6.7 kilobases (kb) downstream of rsl7702901) and SLC03A1 (~223kb upstream of rsl7702901).
[00185] Because expression of transcripts may be influenced by the patient's physiological state, expression of these genes in a controlled environment was analyzed. Expression of ST8SIA2 and SLC03A1 were previously analyzed in a mouse model of RYGB (Hatoum, I.J. et al., / Clin Endocrinol Metab, vol 97, pp E1023-E1031, 2012). Age- and sex-matched animals were randomized to RYGB, sham operation with ad libitum food intake (SO-AL), or sham operation with food restriction to match the weight of the RYGB animals (SO-WM). After ten weeks, animals were sacrificed and expression was determined in upper bypassed limb (BL), the upper Roux limb (RL), the upper common limb (CL), the colon, the liver, the muscle, the epididymal fat and the subcutaneous fat.
[00186] Expression of ST8SIA2 was not significantly altered in any tissue after RYGB relative to SO-AL and SO-WM. In contrast, expression of SLC03A1 was significantly altered in the RL, CL, and subcutaneous fat after RYGB, relative to ad libitum-fed shams. It appeared that effects in RL and CL were weight loss-independent, as these remained significant in the RYGB compared to SO-WM animals. The effects in the BL and colon were also significant in Roux animals compared to weight matched animals. The biological relationship between rsl7702901 and regulation of ST8SIA2 or SLC03A1 does not appear to be in strong linkage disequilibrium.
[00187] Because the mechanisms of weight gain and weight loss may be shared, previously reported and validated BMI loci (Speliotes, E.K. et al., Nat Genet, vol 42, pp 937-48, 2010) were analyzed for association with weight loss after surgery. Unlike the association of rsl7702901 with weight loss after RYGB (Figure 20), deep sequencing of the MC4R locus did not indicate any association between variants in this gene and weight loss after surgery (Figure 21).
Example 8: Different Bariatric Surgeries Act Through Similar Mechanisms
[00188] To determine if different metabolic procedures produce similar results, possibly using similar mechanisms of action, patients that have undergone gastric bypass, biliopancreatic diversion, sleeve gastrectomy and duodenal endoluminal sleeve were analyzed for effects of weight loss, food intake, insulin sensitivity, glucose tolerance, insulin secretion, and endogenous glucose production. Despite the disparity in the type of procedure performed, gastric bypass, biliopancreatic diversion, sleeve gastrectomy and duodenal endoluminal sleeve surprisingly had similar effects, increased weight loss, decreased food intake, increased energy expenditure, greater insulin sensitivity, increased glucose tolerance and enhanced insulin secretion. (Data not shown.)
[00189] Moreover, the different metabolic procedures also had similar effects on the gastrointestinal endocrine system. Levels of ghrelin, glucagon-like peptide- 1, peptide YY and gastric inhibitory polypeptide demonstrated similar changes in post-prandial secretion levels in individuals that have undergone gastric bypass, biliopancreatic diversion, sleeve gastrectomy, ileal interposition or duodenal endoluminal sleeve.
Example 9: Genetic Factors Contributing to Weight Loss
[00190] The effect of RYGB on expression of genes in a previously described (McAuley, E. Z. et ah, Identification Of Sialyltransferase 8B As A Generalized Susceptibility Gene For Psychotic And Mood Disorders On Chromosome 15q25-26, PLoS ONE 7, e38172 (2012)) mouse model was determined. Mice were randomized to RYGB or sham operation with food restriction to match the weight of the RYGB animals (WMS). Animals were sacrificed after 10 weeks, and gene expression was measured in the alimentary limb, liver, and epididymal fat (Figure 22, Table 10).
Table 10: Differentially expressed genes.

slcl2a4 solute carrier family 12 NM_009195
(potassium/chloride transporters),
member 4
eraf NM_133245
hoxal homeobox Al NM_010449
satll spermidine/spermine Nl -acetyl ENSMUST00000026601 transferase-like 1
adiporl adiponectin receptor 1 AK182949
adiporl adiponectin receptor 1 NM_028320
adiporl adiponectin receptor 1 AK143680
abcf2 ATP-binding cassette, sub-family F NM_013853
(GCN20), member 2
abcf2 ATP-binding cassette, sub-family F CA751126
(GCN20), member 2
mier3 mesoderm induction early response 1, NM_172593
family member 3
ddr2 discoidin domain receptor tyrosine BB613073
kinase 2
ddr2 discoidin domain receptor tyrosine AK028767
kinase 2
ddr2 discoidin domain receptor tyrosine NM_022563
kinase 2
nphsl nephrosis 1, congenital, Finnish type AK141081
(nephrin)
zranb3 zinc finger, RAN-binding domain ENSMUST00000097598 containing 3
zranb3 zinc finger, RAN-binding domain NM_172642
containing 3
cldnl6 NM_053241
dhrs3 dehydrogenase/reductase (SDR family) AF061743
member 3
dhrs3 dehydrogenase/reductase (SDR family) NM_011303
member 3
adnp2 ADNP homeobox 2 ENSMUST00000066743 scrtl NM_130893
trappc5 trafficking protein particle complex 5 NM_025701
trappc5 trafficking protein particle complex 5 AK003633
polk polymerase (DNA directed) kappa ENSMUST00000091386 polk polymerase (DNA directed) kappa NM_012048
clnsla chloride channel, nucleotide- sensitive, NM_023671
1A
col4a3bp collagen, type IV, alpha 3 AK020301
(Goodpasture antigen) binding protein
 104 akap8 A kinase (PRKA) anchor protein 8 ENSMUST00000002699
104 akap8 A kinase (PRKA) anchor protein 8 ENSMUST00000002699
105 med21 mediator complex subunit 21 NM_025315
106 aplm2 adaptor-related protein complex 1, mu NM_009678
2 subunit
107 ulk4 unc-51-like kinase 4 NM_177589
108 ulk4 unc-51-like kinase 4 ENSMUST00000098284
109 ulk4 unc-51-like kinase 4 BU946109
110 ift57 intraflagellar transport protein 57 NM_028680
111 ift57 intraflagellar transport protein 57 AK014731
112 lca51 NM_001001492
113 armc9 armadillo repeat containing 9 NM_030184
114 armc9 armadillo repeat containing 9 NM_027456
115 armc9 armadillo repeat containing 9 AK019600
116 dio3 deiodinase, iodothyronine, type III NM_172119
117 wfdc8 NM_001080550
118 cfb complement factor B NM_008198
119 eif4e eukaryotic translation initiation factor NM_007917
4e
120 eif4e eukaryotic translation initiation factor M61731
4e
121 eif4e eukaryotic translation initiation factor AK146757
4e
122 igj immunoglobulin J polypeptide, linker NM_152839
protein for immunoglobulin alpha and
mu polypeptides
123 ctnnd2 catenin (cadherin-associated protein), ENSMUST00000081728 delta 2 (neural plakophilin-related arm- repeat protein)
124 ampd2 adenosine monophosphate deaminase 2 NM_028779
(isoform L)
125 rtkn rhotekin NM_009106
126 rslldl ribosomal LI domain containing 1 NM_025546
127 elk4 ELK4, ETS-domain protein AK156537
128 elk4 ELK4, ETS-domain protein ENSMUST00000086556
[00191] To identify genetic factors contributing to weight loss after RYGB, an exploratory genome wide association study (GWAS) of 858 genetically unrelated individuals was performed (Table 2). After stringent quality control measures, 1,943,373 single nucleotide polymorphisms (SNPs) were analyzed. To minimize heterogeneity from the underlying population structure, we limited the analyses to 693 patients genetically determined to be Caucasian. The association between SNPs and percent total weight loss ( WL) at the lowest weight (nadir) after RYGB using additive models of quantitative trait associations was assessed.
Table 11: Pre- and post-operative characteristics of the RYGB study population and replication cohort.

[00192] 103 marginally significant (P<5xl0~5) SNPs were identified (Table 12), representing
26 independent loci (pairwise r <0.5). The most highly associated SNP per region was carried forward for validation in an independent cohort of 327 Caucasian RYGB patients. 23 of the SNPs were successfully genotyped, and associations with percent weight loss were analyzed using linear regression models. Results of the original and validation cohorts were then meta- analyzed using fixed effects models.
Table 12: Top 50 expression transcripts associated with rsl7702901.

Contig34964 0.000125475 liver
BC009871 0.000139822 liver hCT1646793 0.000169095 liver
HSS00381099 0.000178477 liver
FAM10A4 0.000193237 subcutaneous fat
Contigl2033 0.000200709 omental fat
CNTNAP3B 0.000212491 omental fat
AK094533 0.00022344 liver
ERAF 0.000249779 omental fat
HOXA1 0.000251027 liver
SATL1 0.000251598 subcutaneous fat
U84510 0.000259264 liver
ADIPOR1 0.000260775 liver
ABCF2 0.000289326 liver
HCT1958096 0.000291375 liver
MIER3 0.000305798 liver
DDR2 0.000308075 liver
NPHS1 0.000315369 liver
HSS00053942 0.000327271 liver
ZRANB3 0.000339101 subcutaneous fat
CLDN16 0.000362854 liver
DHRS3 0.000398518 liver
OR2A2 0.000430517 liver
BC022568 0.000463747 liver
Contig34719 0.000468504 liver
HCT1845647 0.000470327 liver
ADNP2 0.000470332 liver
HCT2297022 0.000487732 liver
HSS00299143 0.000491702 liver
AF400502 0.000519205 omental fat
SCRT1 0.000521866 liver
Contig43708 0.000537265 liver
HSS00214508 0.000540097 subcutaneous fat
C2orf29 0.000543099 liver
HCT1956088 0.000566656 liver
Contig57822 0.000581398 subcutaneous fat
HCT1641204 0.000589909 liver
CR749513 0.000590453 liver
[00193] SNP rsl7702901 at 15q26.1 was significantly associated with percent weight loss after Roux-en-Y gastric bypass (RYGB)
 To determine the potential biological function of rsl7702901, its association with the expression level of -44,000 transcripts in liver, omental fat and subcutaneous fat was examined. No multiple test- corrected, significant associations were detected between rs 17702901 and preoperative expression of any transcripts, including the two nearest genes - ST8SIA2, located -6.7 kilobases (kb) downstream of rsl7702901 and SLC03A1, ~223kb upstream of this SNP (Table 12). The magnitude of effect was similar in the study population and replication cohorts, with betas of - 6.70 and -6.52, respectively (Table 13).
Attorney uocKet ΓΝΟ.: IUU» /J-03J ( i u vwtw
To determine the potential biological function of rsl7702901, its association with the expression level of -44,000 transcripts in liver, omental fat and subcutaneous fat was examined. No multiple test- corrected, significant associations were detected between rs 17702901 and preoperative expression of any transcripts, including the two nearest genes - ST8SIA2, located -6.7 kilobases (kb) downstream of rsl7702901 and SLC03A1, ~223kb upstream of this SNP (Table 12). The magnitude of effect was similar in the study population and replication cohorts, with betas of - 6.70 and -6.52, respectively (Table 13).
Attorney uocKet ΓΝΟ.: IUU» /J-03J ( i u vwtw

Table 13: SNP association results from the genome- wide association analysis.
GWAS Cohort Replication Cohort Combined
Distance from Gene
SNP Closest Gene MA2 Chr Position Beta P-value Beta P-value Beta P-val to SNP (bp)1
rsl0515808 C1QTNF2 23283 A 5 159753509 -4.06 8.2 x 10"8 -1.17 0.27 -3.08 4.2 x rs7158359 CHES1 28219 G 14 88664048 -3.03 3.4 x 10"7 -0.41 0.65 -2.27 4.6 x rs7129556 AQP11 631 T 11 76977696 -2.80 4.3 x 10"7 -0.60 0.44 -2.07 3.9 x rs7185923 SALL1 60335 c 16 49802988 -2.40 8.1 x 10"7 -0.63 0.40 -1.89 3.5 x rs934760 CLASP1 0 G 2 12202672 -4.28 4.6 x 10"6 0.56 0.68
rs 1104959 RPS14 79991 T 5 149722429 7.75 5.8 x 10"6 0.86 0.66 4.79 1.8 x rs9403832 STXBP5 0 c 6 14795969 2.17 9.8 x 10"6 -0.51 0.47 1.30 O.OC rs 17702901 ST8SIA2 6728 A 15 90731415 -6.70 1.1 x 10"5 -6.52 0.002 -6.64 7.4 x rs588217 INTS4 6391 A 11 77261024 -2.55 1.4 x 10"5 -0.59 0.47 -1.87 7.0 x rs6554217 RNU5B 63795 T 4 55672161 2.89 1.5 x 10"5 -1.43 0.15
rs9357419 PHACTR1 134845 C 6 12690973 -2.95 1.8 x 10"5 0.56 0.56 -1.80 O.OC rs 11260025 CLEC4G 12090 c 19 7687753 3.33 2.2 x 10"5 -1.06 0.32 1.82 O.OC rs 12803675 OR4C13 71848 A 11 49858702 3.69 2.7 x 10"5 0.37 0.79 2.80 1.8 x rsl3380914 FBX015 578813 A 18 69312767 -2.50 2.9 x 10"5 -0.57 0.51 1.89 1.2 x
Attorney uocKei ΓΝΟ.: IUU»/J-03J ( i u vwtw
 rs!0518316 SYNP02 120241167 -2.52 3.0 x 10- 1.37 0.15
rs!0518316 SYNP02 120241167 -2.52 3.0 x 10- 1.37 0.15
rs6911409 KCNQ5 A 73910091 -3.71 3.5 x 10- -1.14 0.32 -2.74 rs 12659689 KAU4 C 34836108 -1.98 3.9 x 10- -0.11 0.87 -1.39 rs 1952291 C14orfl06 618149 A 14 45410504 -4.32 4.3 X 10- 1.27 0.42 -2.65 rs 1289666 TTF2 C 117350312 2.73 4.3 X 10- -0.24 0.80
rsl 1788785 HSD17B3 A 96111183 -2.79 4.5 X 10- -0.68 0.50
rsl 883264 BIK C 22 41834344 2.85 4.6 X 10- 0.76 0.46
rsl 2696123 MIRN135A2 66339 C 163099074 -2.36 4.7 x 10- 0.24 0.77
Absolute value of the distance from the start or stop site of the closest gene. A distance of 0 indicates that the SNP is located within the gene.
MA=Minor allele
[00194] Expression of sta8sia2, the mouse orthologue of the gene closest to rsl7702901, was significantly lower in the epididymal fat and liver of RYGB-treated than WMS mice (Figure 23A). In addition, intestinal alimentary limb expression of slco3al was significantly greater in the RYGB group than WMS controls (Figure 23B).
[00195] Results in humans using a gene-based association test that integrates SNP
associations with linkage disequilibrium patterns within each gene was analyzed and identified a marginally significant association (p=8.0xl0~ ) for the aquaporin 11 gene (AQPll ; Table 14). While there were 27 SNPs in this region with a P-value<0.001, there was no statistically significant association between the top SNP in this region, rs7129556, and percent weight loss in the replication cohort (Figure 24A). No genome- wide, multiple test-corrected, significant associations between rs7129556 and the expression of any transcripts in humans was detected, but this SNP was marginally associated with expression of AQPll itself (Pomentai=9 xlO'5 , Puver =1.6xl0"4; Table 15).
[00196] In the mouse models, aqpll expression in the alimentary limb and liver was significantly lower after RYGB than in WMS mice (Figure 24B). In contrast, expression of clnsla, the gene closest to aqpll, was not significantly changed after RYGB (Figure 24C).
Table 14: Top 50 association results for gene-based association tests.

CLEC4M 19 46 0.00071 rsl 1260025 2.21E-05
CLNS1A 11 39 0.000747 rs7129556 4.276E-07
COL4A3BP 5 82 0.000873 rs6453134 0.0001267
GCNT4 5 61 0.001 rs4632781 0.0002618
INTS4 11 115 0.00102 rs588217 1.363E-05
CKAP2 13 26 0.001241 rsl l618716 0.0007868
SPAG6 10 4 0.001533 rs9665348 0.03949
C3orf39 3 86 0.00167 rs536119 6.329E-05
RPS27A 2 56 0.001706 rsl561231 0.0009679
Clorf87 1 165 0.001751 rs686119 0.0004618
VPS36 13 46 0.00176 rs4884452 0.0003805
CALML4 15 41 0.00197 rs8025947 0.0005017
THSD1 13 43 0.002 rs4884452 0.0003805
TBC1D3B 17 2 0.00204 rs4500794 0.0004894
HMGCR 5 66 0.00214 rs7700468 0.000152
CLN6 15 43 0.00219 rs8025947 0.0005017
KLK8 19 81 0.00223 rsl 701948 0.0005329
RSF1 11 104 0.002362 rsl 1237249 1.906E-06
KRT7 12 121 0.002513 rs7953684 0.0001044
ZNF223 19 80 0.00261 rs8105003 0.0003053
LMAN2L 2 25 0.00276 rs2872633 0.001663
LVRN 5 243 0.00276 rsl593872 0.0003657
CNNM4 2 34 0.0028 rsl7119562 0.003587
SLC06A1 5 157 0.002973 rsl0041015 0.0006075
GJA4 1 28 0.00298 rs4653105 0.001588
OPALIN 10 135 0.00298 rsl 1188734 0.0001968
KLK11 19 104 0.00301 rs 1701948 0.0005329
HOXA4 7 60 0.00304 rs983184 0.0005409
RETN 19 33 0.00305 rs 11260025 2.21E-05
KLK9 19 84 0.00307 rs 1701948 0.0005329
ZNF284 19 74 0.003167 rs8105003 0.0003053
KRT81 12 150 0.00317 rs7953684 0.0001044
SIRPG 20 123 0.00318 rs4254565 0.0006302
KLK10 19 95 0.00323 rs 1701948 0.0005329
Clor 212 1 46 0.00329 rs4653105 0.001588
KLK12 19 110 0.00334 rs 1701948 0.0005329
PHF3 6 53 0.00334 rs4710437 0.0001252
GRPEL1 4 74 0.00338 rs 12648134 0.0005674
HOXA5 7 58 0.00349 rs983184 0.0005409
Table 15: Top 50 expression transcripts associated with rsl7702901.

ULK4 0.000234395 liver
Contig36748_RC 0.000248422 omental fat
ZNF711 0.000258753 omental fat
IFT57 0.000266345 liver
IGLV2J4 0.000267441 subcutaneous fat
LCA5L 0.000271869 liver
ADAM3A 0.000276415 liver
AL833696 0.000303924 liver
ARMC9 0.000311108 omental fat
BC040305 0.000315233 liver
DI03 0.000324871 liver
WFDC8 0.000338595 omental fat
CFB 0.000339373 subcutaneous fat
EIF4E 0.000381093 liver
IGJ 0.000381533 liver
ZNF509 0.000394645 liver
PI4KAP2 0.000415647 liver
CTNND2 0.00042246 subcutaneous fat
C3orf38 0.000423274 liver
AMPD2 0.000424693 liver
XM_173060 0.000429279 liver
XM_065192 0.00045425 omental fat
RTKN 0.000455737 liver
Contig41220_RC 0.000481428 omen
RSL1D1 0.00048159 subq
AK097908 0.000496614 omental fat
XM_210217 0.000505951 liver
HSS00095153 0.000506833 subq
Contig45100_RC 0.000518199 liver
AK074192 0.000560538 omental fat
CFB 0.000563012 subq hCT1955907_l 0.000617333 liver
XM 73120 0.000620047 liver
AK022383 0.000638859 omental fat
AL833662 0.000639129 omental fat
Contigl5012_RC 0.000641473 omental fat
Contig31661_RC 0.000646011 subcutaneous fat
PEA15 0.000647577 subcutaneous fat
ELK4 0.000650268 liver
[00197] Because the physiological mechanisms of weight gain to generate obesity and weight loss after RYGB may be related, previously reported and validated BMI-associated loci were assessed for association with weight loss after RYGB in humans. None of the 32 previously- reported BMI-associated or 28 diabetes-associated loci was associated with weight loss after surgery (Tables 16 and 17). Deep sequencing of the MC4R locus showed no evidence of an association between variants in this gene and weight loss after RYGB.
Attorney uocKei ΓΝΟ.: IUU»/J-03J ( i u vwtw

Table 16: Association results for SNPs previously identified as associated with obesity.
GWAS Cohort Validation Cohort Combined
SNP Closest Genes Chr Position Beta P-value Beta P-value Beta P-value rs3810291 TMEM160, ZC3H4 19 52260843 0.8816 0.09116 1.627 0.03188 1.1222 0.008874 rs9816226 ETV5 3 187317193 1.18 0.08907 0.04788 0.9598 rs713586 RBJ, ADCY3, POMC 2 25011512 0.2023 0.678 1.117 0.1079 rs206936 NUDT3, HMGA1 6 34410847 0.8864 0.1432 -1.133 0.1898 0.2204 0.6562 rs 12444979 GPRC5B, IQCK 16 19841101 0.4432 0.5179 0.1076 0.9165 0.3396 0.551 rs3817334 MTCH2, NDUFS3, 11 47607569 0.7219 0.1428 0.2568 0.7194 0.5722 0.1579
CUGBP1
rs2890652 LRP1B 2 142676401 1.07 0.2291 rs4929949 RPL27A, TUB 11 8561169 -1.146 0.1109 rs2112347 FLJ35779, HMGCR 5 75050998 -0.252 0.6206 -1.337 0.08203 0.5839 0.1684 rsl558902 FTO 16 52361075 -0.1002 0.8373 0.7299 0.322
Attorney uocKei ΓΝΟ.: IUU»/J-03J ( i u vwtw


Attorney uocKei ΓΝΟ.: IUU»/J-03J ( i u vwtw


Table 17: Association results for SNPs previously identified as associated with diabetes.

1 1
rs2237892 KCNQ1 2796327 2.437 0.01667
1 1
rs231362 KCNQ1 2648047 0.169 0.7283
1 1
rs5215 KCNJ11 17365206 -0.2529 0.6285 rs 1552224 CENTD2 region 72110746
1 1
rsl0830963 MTNR1B 92348358 0.9426 0.2734
1 1
rs2943634 IRS1 region 226776324 -0.291 0.5857
1 1
rs7961581 TSPAN8/LGR5 12 69949369 -0.1602 0.7799 rs7957197 HNF1A 12 119945069 -0.2222 0.7284 rsl 1642841 FTO 16 52402988 -0.5849 0.2549 rs4430796 HNF1B 17 33172153 0.1217 0.8362
APPENDIX A
The sequences as provided in Appendix A of U.S. Patent Application Serial No. 13/828,809, filed on March 14, 2013, which is hereby incorporated by reference in its entirety. These sequences directly correspond to (i.e., are identical to) SEQ ID NOs 129-837 provided in the sequence listing of the present application.
2252681.1
Appendi xB . txt
SNP p
rs7481282 8. . 636E-7
rs9322082 0. .00001371
rs648601 0. .00001859
rsl408577 0. .00001929
rs4323329 0. .00002226
rs4452660 0. .00002226
rs4085813 0. .00002238
rs4945220 0. .00002292
rs650171 0. .00002343
rs7123080 0. .00002343
rs8111760 0. .00002345
rsl7646434 0. .00002376
rsl7702960 0. .00002376
rsl0899404 0. .00002945
rsl7006485 0. .00003101
rsl7646351 0. .00003173
rsl3414513 0. .00003186
rs6712661 0. .00003186
rs735483 0. .00003186
rs7601226 0. .00003186
rs9653407 0. .00003186
rsl7646492 0. .00003213
rsl2711551 0. .00003219
rsl2968184 0. .00003313
rsl3000440 0. .00003348
rsl3413270 0. .00003348
rs2118387 0. .00003348
rs2164796 0. .00003348
rs6711921 0. .00003348
rs9678017 0. .00003348
rsl0177322 0. .00003468
rsl7006496 0. .00003502
rs724403 0. .00003502
rs4344516 0. .0000361
rsl2711559 0. .000037
rs4450992 0. .0000372
rs684813 0. .00003859
rsl6867581 0. .00003915
rs4703388 0. .00003915
rs621456 0. .00003926
rsl954888 0. .00004077
rs7580531 0. .00004105
rs7744769 0. .00004291
rsl0242229 0. .00004375
rsl2615068 0. .00004576
rsl2622908 0. .00004576
rsl7006394 0. .00004576
rs7564564 0. .00004681
rs2157814 0. .00004726
rs4267966 0. .00004741
rsl2614155 0. .00005011
rsll707244 0. .00005025
rsl7050208 0. .00005125
rs6913861 0. .00005196
rsl0936257 0. .00005258
rsl529014 0. .00005471
rs9386176 0. .00005646
rs9399592 0. .00005646
rs9403837 0. .00005646
rs2328774 0. .00005782
rs6554218 0. .00005783
rs4551178 0. .00005824
rsl456243 0. .00005826
rs7116127 0. .00005826
rs4134463 0. .0000585
rsl945747 0. .00005922
rsl0137389 0. .00006177
rsl0496569 0. .00006274
rs477594 0. .00006589
Page 1
Appendi xB . txt rs504973 0. .00006589
rs834194 0. .00006589
rsl0179345 0. .00006609
rs6756225 0. .00006609
rsl3302476 0. .00006648
rs9360640 0. .00006802
rs484363 0. .00006837
rsl365832 0. .00006923
rs4445078 0. .00006973
rsl2614379 0. .00007143
rsl2087475 0. .00007264
rsl3403769 0. .00007504
rs643388 0. .0000771
rs663674 0. .00007742
rs415234 0. .00007831
rs687037 0. .00007853
rsl2073831 0. .00008024
rs6023633 0. .00008146
rs6736269 0. .00008288
rs7772526 0. .00008298
rs6441408 0. .00008446
rsll018434 0. .00008495
rs2594536 0. .0000852
rsl0185512 0. .00008828
rs2034137 0. .00008828
rsl7087674 0. .00008992
rsl456244 0. .00009005
rslll22861 0. .00009285
rs6746090 0. .00009285
rs9840287 0. .00009301
rs2048504 0. .00009427
rs6014185 0. .00009427
rsl420582 0. .0000946
rs668701 0. .00009522
rsl0170935 0. .00009539
rs6714671 0. .00009539
rs7595601 0. .00009539
rs3912845 0. .00009655
rsl7764592 0. .0000985
rsl0496570 0. .00009884
rsl2611458 0. .00009884
rsl3395695 0. .00009884
rs2304560 0. .00009884
rs2304561 0. .00009884
rs6704587 0. .00009884
rs7566558 0. .00009884
rs934761 0. .00009884
rs6541782 0. .0001021
rs6760211 0. .0001021
rsl633749 0. .000103
rs7538154 0. .0001038
rsl0255791 0. .0001039
rs9446844 0. .0001046
rsl2614123 0. .0001058
rsl0184008 0. .000106
rs6064117 0. .0001079
rs7760644 0. .000109
rs877191 0. .00011
rs611232 0. .0001113
rs6912526 0. .0001153
rs911196 0. .0001162
rs2181942 0. .0001182
rsl512065 0. .0001192
rsl0179294 0. .0001196
rsl3395277 0. .0001196
rs6023645 0. .0001201
rs594406 0. .0001204
rs595459 0. .0001204
rs4811538 0. .0001212
rsl505006 0. .0001214
Page 2
Appendi xB . txt rs8180176 0. .000123
rs4848712 0. .0001243
rsl551151 0. .0001253
rs4711162 0. .0001253
rs2034136 0. .0001279
rs7558771 0. .0001279
rs7188211 0. .0001294
rsl628613 0. .0001301
rsl666790 0. .0001301
rsl666797 0. .0001301
rsl700572 0. .0001301
rsl2493604 0. .0001308
rsl388702 0. .0001327
rsl492146 0. .0001327
rsl492147 0. .0001327
rsl2190601 0. .0001328
rs6704842 0. .0001361
rsl2622810 0. .0001364
rs7599081 0. .0001364
rs9653406 0. .0001364
rsl2614362 0. .0001376
rs6729454 0. .0001376
rs669738 0. .0001384
rs2289192 0. .0001396
rs7672513 0. .00014
rsl0498676 0. .0001406
rs3778166 0. .0001406
rsl388705 0. .000144
rs675079 0. .0001444
rs2962621 0. .0001458
rs638807 0. .000146
rs7943055 0. .000147
rs7765767 0. .0001483
rs685553 0. .0001488
rs608382 0. .0001491
rs7700468 0. .000152
rsl057530 0. .0001524
rs488824 0. .0001535
rs553727 0. .0001535
rs611536 0. .0001535
rs947841 0. .0001535
rs9322081 0. .0001545
rs3916911 0. .000156
rsl0942739 0. .0001566
rs7709282 0. .0001566
rs4121744 0. .0001568
rs524874 0. .0001585
rsl0765186 0. .0001588
rs4440336 0. .0001599
rs6872314 0. .0001599
rs7356637 0. .0001599
rsl881665 0. .0001601
rs9386177 0. .0001601
rslll55493 0. .0001617
rslll89415 0. .0001621
rsl881663 0. .0001627
rsl7389893 0. .000165
rsl2419587 0. .0001697
rsl6922585 0. .0001697
rs6541784 0. .0001716
rs2092859 0. .0001741
rs2591107 0. .0001755
rs9468304 0. .0001759
rslll9723 0. .0001781
rsl2662634 0. .0001793
rs4811532 0. .00018
rsl3401792 0. .000182
rsl388706 0. .0001823
rs6023649 0. .0001843
rsl0929465 0. .0001848
Page 3
Appendi xB . txt rs4669141 0. .0001848
rs4804226 0. .0001852
rs8009216 0. .000186
rs7001847 0. .0001888
rsl2440999 0. .0001898
rs2200674 0. .0001898
rsl7766596 0. .0001927
rs2280565 0. .0001928
rsl335955 0. .0001932
rsl889102 0. .0001942
rs2784465 0. .0001942
rs4358853 0. .0001942
rs4685652 0. .000195
rs2678801 0. .0001951
rsl0816127 0. .0001972
rs4271025 0. .0001972
rs4279660 0. .0001972
rs4403465 0. .0001972
rs4892107 0. .0001981
rsl0177273 0. .0002003
rslll5356 0. .0002006
rs2167107 0. .0002006
rs7926062 0. .0002024
rsl023329 0. .000203
rs9620115 0. .000203
rsl0457864 0. .0002047
rs7250467 0. .0002048
rs4804788 0. .0002064
rs4685650 0. .0002065
rs4685651 0. .0002065
rs2328777 0. .0002073
rs9322084 0. .0002073
rs9497675 0. .0002073
rs6747693 0. .0002075
rsl0150607 0. .000208
rsl420577 0. .0002091
rs2827489 0. .0002098
rs2786262 0. .0002099
rsl0969252 0. .0002105
rs687781 0. .0002105
rs4988386 0. .0002129
rs4988388 0. .0002129
rs4988389 0. .0002129
rsl912890 0. .0002133
rsl553047 0. .0002145
rs2412616 0. .0002145
rsl2454494 0. .0002153
rs608240 0. .0002155
rs9497679 0. .0002176
rs2786258 0. .000218
rs595106 0. .000219
rs596159 0. .000219
rs618472 0. .000219
rs652539 0. .000219
rs6679824 0. .0002201
rs6688321 0. .0002201
rsl0969267 0. .0002222
rsl7105190 0. .0002249
rsl7105228 0. .000225
rs2186053 0. .000225
rsl0755432 0. .0002282
rsl591906 0. .0002284
rs6921180 0. .0002289
rs2027733 0. .0002297
rsl532212 0. .0002308
rs6532675 0. .0002309
rsll014929 0. .0002316
rsll014931 0. .0002316
rsll014933 0. .0002316
rsll014935 0. .0002316
Page 4
Appendi xB . txt rsll014936 0. .0002316
rsl2784683 0. .0002316
rs7862503 0. .0002316
rs7894301 0. .0002316
rs4445901 0. .0002341
rs9929708 0. .0002341
rsl559604 0. .0002351
rs9377040 0. .0002354
rsll014932 0. .0002361
rs2368120 0. .0002361
rs4703674 0. .0002367
rs767676 0. .0002367
rs2786263 0. .0002368
rsl3018316 0. .000237
rsl2232770 0. .0002384
rsl6982264 0. .0002393
rsl6870906 0. .0002398
rs4045166 0. .0002419
rsl402436 0. .0002421
rs748040 0. .0002422
rs6717225 0. .0002436
rs4711170 0. .0002465
rs2658785 0. .0002489
rsl2205302 0. .00025
rsl3084500 0. .00025
rs2919051 0. .0002524
rs296325 0. .0002541
rs296329 0. .0002541
rs296333 0. .0002541
rs296334 0. .0002541
rs296318 0. .0002561
rs296319 0. .0002561
rs296320 0. .0002561
rsl0147303 0. .0002574
rsl2718626 0. .0002594
rsl2718627 0. .0002594
rsl2718628 0. .0002594
rs3118041 0. .0002608
rs2295599 0. .0002629
rs7740233 0. .000265
rsl412727 0. .0002658
rs3949639 0. .0002658
rs7043400 0. .0002658
rs2153356 0. .0002667
rs870913 0. .0002667
rs870914 0. .0002667
rs870915 0. .0002667
rs2857682 0. .0002672
rs6023640 0. .0002673
rsl0281294 0. .0002674
rs234589 0. .0002689
rs6023625 0. .0002699
rsl0209628 0. .0002718
rsl892159 0. .0002728
rsl892160 0. .0002732
rs7917879 0. .0002749
rs9535895 0. .0002751
rsl2599944 0. .0002759
rs995365 0. .0002773
rsl595288 0. .0002785
rs234586 0. .000279
rsl7671266 0. .0002792
rs4685654 0. .000281
rsl0853651 0. .0002816
rs4685649 0. .000282
rsl0491676 0. .0002832
rsl0491679 0. .0002832
rsl7698884 0. .0002842
rs2492279 0. .0002846
rsl2278691 0. .0002857
Page 5
AppendixB.txt rsl0069744 0. .0002892
rsl0484891 0. .0002892
rs7871542 0. .0002892
rs4988398 0. .0002896
rsl455048 0. .000294
rsl943559 0. .0002946
rs2839314 0. .0002946
rsl0457082 0. .0002953
rs6541794 0. .0002962
rs6023624 0. .0002981
rsl0448170 0. .0002986
rsl0969241 0. .0002986
rsl0969245 0. .0002986
rsl0969247 0. .0002986
rsl0969248 0. .0002986
rs736508 0. .0003
rsl513680 0. .0003002
rsl838408 0. .0003002
rsl849566 0. .0003002
rsl521034 0. .0003006
rs2139795 0. .0003006
rs2251640 0. .0003012
rs2784464 0. .0003012
rs7231534 0. .0003017
rsl0491681 0. .0003052
rsl998199 0. .0003053
rs582351 0. .0003058
rsll811546 0. .0003061
rsl0969272 0. .0003081
rsl2771164 0. .0003098
rsl0205258 0. .0003102
rs6100191 0. .0003127
rsl943553 0. .0003128
rsl0139222 0. .0003129
rsl2615868 0. .0003137
rsl2711546 0. .0003137
rs6735895 0. .0003137
rsll635771 0. .0003143
rslll2833 0. .0003155
rsl0196761 0. .0003161
rsl0496568 0. .0003161
rsl7006463 0. .0003161
rs6725314 0. .0003161
rs7383045 0. .0003161
rs7599933 0. .0003161
rs7770235 0. .0003161
rs7038904 0. .0003163
rs9293920 0. .0003169
rs7851775 0. .0003177
rsl0490196 0. .0003193
rs4873792 0. .0003196
rsl0510271 0. .0003201
rsl0969230 0. .0003203
rs4233172 0. .000323
rsl344506 0. .0003237
rs7864733 0. .000324
rsl0203617 0. .0003251
rsl398112 0. .0003255
rslll55742 0. .0003258
rsl2611456 0. .0003268
rsl2611457 0. .0003268
rsl7039719 0. .0003268
rs6761493 0. .0003268
rsl355827 0. .000327
rs7239670 0. .000327
rsll084821 0. .0003278
rsl6962574 0. .000328
rs2025129 0. .0003285
rs4323568 0. .0003289
rs6070587 0. .000329
Page 6
Appendi xB . txt rs657426 0. .0003301
rs4685648 0. .0003311
rs7482394 0. .0003312
rs2889741 0. .0003316
rsl0214511 0. .0003325
rsl885235 0. .0003327
rsl0756650 0. .0003332
rs4804787 0. .0003338
rsll920714 0. .0003353
rsl580569 0. .0003353
rs4855516 0. .0003353
rs4855517 0. .0003353
rs4855518 0. .0003353
rs6549147 0. .0003353
rs6764924 0. .0003353
rsl0123940 0. .0003357
rs9468414 0. .000336
rsl335957 0. .0003361
rs2786266 0. .0003361
rs2312587 0. .0003365
rs6477537 0. .0003375
rsl513686 0. .0003391
rsl3146442 0. .0003393
rs7866684 0. .0003402
rsll085134 0. .0003422
rs2901113 0. .0003445
rs2901114 0. .0003445
rs4560873 0. .000345
rs610199 0. .000345
rslll29637 0. .0003451
rs7741525 0. .000346
rs9398017 0. .000346
rs6509137 0. .0003481
rsll920741 0. .0003485
rsl602200 0. .0003485
rsl6960857 0. .0003485
rsl0813132 0. .0003501
rs2067951 0. .0003504
rs7747720 0. .0003517
rsl7802700 0. .0003522
rs4490947 0. .0003524
rs2327566 0. .0003534
rs2492274 0. .0003552
rs2492276 0. .0003552
rsl6942896 0. .0003579
rsl2662569 0. .000358
rs4570560 0. .0003585
rsl895320 0. .0003596
rsl3078681 0. .0003605
rsl3065961 0. .0003615
rsl3076600 0. .0003615
rsl474276 0. .0003618
rs6482531 0. .0003633
rsl0969240 0. .0003635
rsl7698983 0. .0003653
rs2327567 0. .0003653
rs6914579 0. .0003656
rsl593872 0. .0003657
rs9482270 0. .0003671
rs902246 0. .0003679
rs902247 0. .0003679
rs7894273 0. .0003693
rs7899880 0. .0003693
rs7475020 0. .0003694
rsl3300699 0. .0003697
rsl885236 0. .0003697
rsl807403 0. .0003706
rsl0830220 0. .0003715
rs4688519 0. .0003733
rs6509134 0. .0003734
Page 7
Appendi xB . txt rsl041752 0. .0003735
rs2828109 0. .0003735
rs2828110 0. .0003735
rs7998892 0. .000375
rs319919 0. .0003754
rsl0510604 0. .0003758
rsl0481554 0. .0003772
rsl556463 0. .0003788
rs6570450 0. .0003794
rs9403262 0. .0003794
rs4884452 0. .0003805
rs9526845 0. .0003815
rs8087567 0. .0003825
rs6888545 0. .0003832
rsl2904291 0. .0003857
rs7193895 0. .0003858
rs9630225 0. .0003862
rs6502586 0. .0003884
rsl0518270 0. .0003892
rsl893692 0. .0003893
rsl0176760 0. .0003912
rsl943579 0. .0003952
rsl943580 0. .0003952
rsl943581 0. .0003952
rs2591098 0. .0003952
rs2591099 0. .0003952
rs2733134 0. .0003952
rsl943582 0. .0003962
rs2212962 0. .0003962
rs6932538 0. .0004003
rs9341408 0. .0004005
rs597462 0. .0004006
rs8129099 0. .000401
rsll970254 0. .0004022
rs2236426 0. .000403
rsl7108636 0. .0004039
rs2417752 0. .0004066
rsll946608 0. .0004076
rs4468712 0. .0004082
rsl387731 0. .0004093
rsl602199 0. .0004093
rs9812027 0. .0004093
rs991807 0. .0004093
rs991808 0. .0004093
rsl965118 0. .0004134
rs8041853 0. .0004134
rs876535 0. .0004141
rs2088403 0. .0004147
rs789900 0. .0004147
rs761937 0. .0004165
rsll886348 0. .0004167
rsll891264 0. .0004167
rs6716674 0. .0004167
rs6745850 0. .0004167
rs2328194 0. .0004175
rs9321803 0. .0004175
rs4609047 0. .0004194
rsl349710 0. .0004197
rs9321804 0. .0004208
rs7095668 0. .0004211
rsl435684 0. .0004226
rs6911913 0. .0004246
rs9390445 0. .0004246
rsll24329 0. .0004265
rsl0977739 0. .0004278
rsl2610472 0. .0004282
rs3826941 0. .0004282
rs4742595 0. .0004283
rsl368299 0. .0004288
rs8109615 0. .0004305
Page 8
AppendixB.txt rs662041 0. .0004335
rsl7403480 0. .000434
rs789887 0. .000436
rs789888 0. .000436
rs9428429 0. .0004363
rs4703645 0. .00044
rslll22898 0. .0004414
rs3860383 0. .0004414
rs7605443 0. .0004414
rs4912173 0. .0004421
rs8028380 0. .0004424
rsl547872 0. .0004433
rs7504838 0. .0004433
rs7765349 0. .0004446
rs9596651 0. .000445
rsll854288 0. .0004461
rs3759846 0. .0004461
rs6570443 0. .0004465
rsl332207 0. .0004476
rsll073855 0. .0004481
rs8036314 0. .0004481
rs8028882 0. .0004486
rs9806190 0. .0004486
rsll016936 0. .0004502
rs4503789 0. .0004521
rs9376586 0. .0004523
rsl344196 0. .0004524
rs6468799 0. .0004528
rs7015311 0. .0004528
rs3757508 0. .0004533
rs3948710 0. .0004533
rsl0204078 0. .0004539
rsl0207199 0. .0004539
rs6945109 0. .0004539
rsl0867221 0. .0004545
rslll37747 0. .0004545
rsl2339181 0. .0004545
rsl452990 0. .000456
rs6570441 0. .000456
rs9403252 0. .000456
rslll37748 0. .0004567
rs3761743 0. .0004571
rs370177 0. .0004578
rs403461 0. .0004578
rsl7112249 0. .0004586
rslll37755 0. .00046
rs769289 0. .00046
rs8109313 0. .0004607
rsl0835824 0. .0004609
rsl2986567 0. .0004619
rsl6831392 0. .0004628
rsll853075 0. .0004629
rsl6960864 0. .0004629
rsl0508710 0. .0004638
rsl2248210 0. .0004638
rsl2252825 0. .0004638
rsl2253015 0. .0004638
rsl2260321 0. .0004638
rsl2263561 0. .0004638
rsl2267071 0. .0004638
rsl2765561 0. .0004638
rsl2766929 0. .0004638
rsl2767114 0. .0004638
rsl2768879 0. .0004638
rsl2770526 0. .0004638
rsl2771414 0. .0004638
rsl2773856 0. .0004638
rsl2776584 0. .0004638
rsl2781790 0. .0004638
rsl521029 0. .0004638
Page 9
Appendi xB . txt rsl521030 0. .0004638
rsl521032 0. .0004638
rsl546702 0. .0004638
rsl7739106 0. .0004638
rs2176937 0. .0004638
rs3758441 0. .0004638
rs3758443 0. .0004638
rs3758444 0. .0004638
rs3817419 0. .0004638
rs4581343 0. .0004638
rs4631780 0. .0004638
rs5012431 0. .0004638
rs7084483 0. .0004638
rs7095982 0. .0004638
rs7096274 0. .0004638
rs7097387 0. .0004638
rs7475023 0. .0004638
rs7475188 0. .0004638
rsl352638 0. .0004646
rs4484195 0. .0004646
rsll049887 0. .0004688
rsl480630 0. .0004688
rsl452989 0. .0004689
rs7872398 0. .0004689
rs7989297 0. .0004704
rsl2243741 0. .0004719
rsl2248769 0. .0004719
rsl2249006 0. .0004719
rsl2263998 0. .0004719
rsl2780744 0. .0004719
rs7893838 0. .0004719
rs7915315 0. .0004719
rs3937845 0. .0004723
rs4771400 0. .0004723
rs4855515 0. .0004723
rs7621668 0. .0004723
rs7635448 0. .0004723
rsl489995 0. .0004733
rs6748226 0. .000474
rsll897514 0. .0004765
rs2170466 0. .0004776
rs7529541 0. .0004783
rsl2676502 0. .0004809
rsl0497107 0. .0004811
rsl6831399 0. .0004811
rs7452495 0. .0004842
rs7500154 0. .0004854
rs399355 0. .0004878
rsl3208784 0. .0004884
rsll073091 0. .0004921
rsll073092 0. .0004921
rsll635913 0. .0004921
rs6495766 0. .0004921
rs8031712 0. .0004921
rs8041062 0. .0004921
rs8041339 0. .0004921
rs4298240 0. .0004923
rs4704170 0. .0004923
rsl0765819 0. .0004936
rs6885454 0. .0004946
rs9390449 0. .0004947
rsl6831410 0. .0004961
rs6560561 0. .0004971
rs9403836 0. .0004984
rsll33174 0. .0004993
rsl0969259 0. .0004994
rs679094 0. .0004994
rsl2289316 0. .0005001
rs2070435 0. .0005002
rsl3264258 0. .0005011
Page 10
Appendi xB . txt rs7042831 0. .0005017
rsl414121 0. .000503
rsl6855165 0. .0005031
rsl873263 0. .0005049
rsl7406994 0. .0005058
rs6468794 0. .0005058
rs6468796 0. .0005058
rsl0093531 0. .0005069
rsl0107399 0. .0005069
rsll987293 0. .0005069
rsll989758 0. .0005069
rsll855819 0. .0005077
rs2356558 0. .000508
rs4544345 0. .000508
rs4140424 0. .0005085
rs6076819 0. .0005085
rs6076820 0. .0005085
rs6076823 0. .0005085
rs6516026 0. .0005085
rs234595 0. .0005095
rsl0152716 0. .0005105
rsl0519999 0. .0005105
rsl0520001 0. .0005105
rsll637062 0. .0005105
rsll853444 0. .0005105
rsll853446 0. .0005105
rsl455047 0. .0005105
rsl6960879 0. .0005105
rsl6960916 0. .0005105
rs8038618 0. .0005105
rs8040254 0. .0005105
rsl0488687 0. .0005112
rs6039529 0. .0005141
rs6056764 0. .0005141
rs341870 0. .0005146
rsl0515405 0. .0005147
rsl349541 0. .0005178
rs4241220 0. .0005178
rs9858963 0. .0005182
rs6936461 0. .0005183
rs9497673 0. .0005183
rs3118045 0. .0005216
rs212293 0. .0005221
rs567990 0. .000524
rsll632343 0. .000525
rsll636113 0. .000525
rsl455045 0. .000525
rs8034582 0. .000525
rs8034766 0. .000525
rs6576603 0. .0005251
rs7165604 0. .0005251
rsl0107160 0. .0005258
rsl2203394 0. .000526
rsl0129671 0. .000528
rsl0483588 0. .000528
rsl2586169 0. .000528
rsl2588980 0. .000528
rsl3075703 0. .0005282
rsl354439 0. .0005282
rs7871453 0. .0005323
rs2850287 0. .0005334
rs534815 0. .0005352
rs2277882 0. .0005383
rs7043954 0. .0005383
rsll629935 0. .0005422
rsl431603 0. .0005461
rs2163996 0. .000547
rs4373347 0. .000547
rsl452988 0. .0005474
rsl489992 0. .0005476
Page 11
Appendi xB . txt rsl7537990 0. .0005476
rsl0491673 0. .0005485
rsl408508 0. .0005485
rsl0767906 0. .0005493
rsl2221893 0. .0005493
rsl0418179 0. .0005497
rs6689022 0. .0005542
rs7539805 0. .0005542
rsl0064203 0. .0005544
rs6495767 0. .0005545
rs684371 0. .0005599
rs2828132 0. .0005603
rs4896533 0. .0005623
rsll676548 0. .0005633
rsl489993 0. .0005669
rsll947379 0. .0005687
rsl746338 0. .0005689
rs3823764 0. .0005695
rsl7154523 0. .0005714
rs6468793 0. .0005725
rsl2176199 0. .0005741
rsl3269411 0. .0005775
rsl405252 0. .0005776
rs6916676 0. .0005796
rsll923978 0. .0005808
rs6711537 0. .0005816
rs6730732 0. .0005816
rsl0969221 0. .0005818
rsl2376718 0. .0005818
rsl6851002 0. .0005824
rs9946863 0. .0005827
rsll678315 0. .0005834
rsl529013 0. .0005852
rsl3257327 0. .0005855
rs4666283 0. .0005865
rsl3377546 0. .0005889
rs6810192 0. .0005952
rsl595286 0. .0005958
rs7646856 0. .0005984
rs2138823 0. .0005987
rs2138824 0. .0005987
rs2176431 0. .0005987
rs8104694 0. .0005987
rs663651 0. .0005994
rs4131293 0. .0005996
rs4131455 0. .0006005
rsll31497 0. .0006007
rs6570784 0. .000601
rs4284720 0. .0006015
rsl70347 0. .000603
rs296323 0. .0006035
rs296328 0. .0006035
rs296335 0. .0006035
rs4740981 0. .0006042
rsl943545 0. .0006062
rsl954972 0. .0006062
rs2591104 0. .0006062
rs2733113 0. .0006062
rs2850276 0. .0006062
rsl943555 0. .0006064
rsl332204 0. .0006065
rsl332206 0. .0006065
rs3902451 0. .0006065
rs6914395 0. .0006067
rsl901515 0. .0006075
rsll237338 0. .0006098
rsl540023 0. .0006098
rsl7429236 0. .0006098
rsl7501198 0. .0006098
rsl943546 0. .0006098
Page 12
Appendi xB . txt rs2097049 0. .0006098
rs2591102 0. .0006098
rs9990383 0. .0006098
rsl0106459 0. .0006138
rs2278155 0. .0006145
rs967444 0. .0006151
rs414509 0. .0006181
rs4839651 0. .0006194
rs6440181 0. .0006194
rsl3258631 0. .0006196
rs890343 0. .000621
rs4326011 0. .0006213
rsl481110 0. .0006225
rsll607512 0. .000624
rsl567819 0. .0006251
rs4734595 0. .0006254
rs7667878 0. .0006261
rslll07212 0. .0006279
rs9490520 0. .0006285
rs8086418 0. .0006292
rsl0781390 0. .0006298
rs9749801 0. .0006324
rs4452425 0. .0006327
rs944559 0. .0006327
rsl0813114 0. .0006347
rs3918322 0. .000635
rs7319214 0. .0006355
rsll56491 0. .000637
rs2504906 0. .0006382
rsll097562 0. .0006383
rsl0813115 0. .0006391
rsl7709654 0. .0006391
rs7745871 0. .0006407
rs6468797 0. .0006434
rs6468798 0. .0006434
rs7925289 0. .0006499
rs6663538 0. .0006506
rsl575054 0. .0006533
rsl7090631 0. .0006562
rs6449263 0. .0006564
rsl2279880 0. .0006572
rsl823507 0. .0006572
rs7115801 0. .0006572
rsl7671496 0. .0006632
rs6453116 0. .0006632
rs6890143 0. .0006632
rs6890320 0. .0006632
rs6893216 0. .0006632
rs717587 0. .0006632
rs6668923 0. .0006636
rsl408507 0. .0006639
rs319924 0. .000664
rs319925 0. .000664
rs6100193 0. .000664
rs2121777 0. .0006647
rs7681041 0. .0006666
rsl0876268 0. .0006675
rsl532763 0. .0006693
rs2209168 0. .0006702
rs2588844 0. .0006712
rs8122333 0. .0006718
rsl0497108 0. .0006725
rsl0497111 0. .0006725
rsl6823807 0. .0006725
rsl0961885 0. .000673
rsl407978 0. .000673
rs427608 0. .0006739
rs451388 0. .0006739
rs3754205 0. .0006745
rs9965748 0. .0006781
Page 13
Appendi xB . txt rs875429 0. .0006792
rs7871676 0. .0006819
rsl7752458 0. .0006822
rs7745473 0. .0006822
rsl0464926 0. .0006833
rsl0464928 0. .0006833
rsll787096 0. .0006833
rsl2679840 0. .0006833
rsl2680350 0. .0006833
rsl543010 0. .0006833
rs9293488 0. .000684
rsl2711699 0. .0006843
rs2421357 0. .0006843
rsl974868 0. .0006848
rs2305317 0. .0006858
rsl2066808 0. .0006862
rsl6840486 0. .0006874
rs292209 0. .0006876
rs9376605 0. .0006901
rs756274 0. .0006926
rs7336398 0. .0006934
rs7039335 0. .0006974
rs627387 0. .0006978
rsll261299 0. .0006982
rs7534106 0. .0006986
rs493412 0. .0006989
rsl7054953 0. .0006996
rs403668 0. .0006996
rs4368235 0. .0007
rs7106157 0. .0007007
rsl862245 0. .0007025
rs986861 0. .0007037
rs7452823 0. .0007051
rsl2441919 0. .0007053
rs6688496 0. .0007057
rslll06529 0. .0007058
rs6934306 0. .000709
rs978960 0. .000709
rs598741 0. .0007093
rs622020 0. .0007093
rs7046871 0. .0007102
rs9536632 0. .0007103
rsl3243392 0. .0007121
rsl2319366 0. .0007123
rs601519 0. .0007132
rsl0790449 0. .0007143
rs4729093 0. .0007143
rs6468795 0. .0007144
rsl6831413 0. .0007156
rsl2368136 0. .0007159
rsl480639 0. .0007159
rsl0876257 0. .000718
rsl2149168 0. .0007181
rs2854516 0. .0007225
rs4236869 0. .0007253
rs7345130 0. .0007269
rs3935754 0. .0007284
rsll892222 0. .0007302
rs4803668 0. .0007322
rs4242641 0. .0007326
rs4895591 0. .0007326
rs6570456 0. .0007326
rsl0786282 0. .000733
rsl0736107 0. .0007335
rs6721161 0. .0007336
rsl2308231 0. .0007337
rsl013507 0. .0007338
rsl225740 0. .0007341
rsl0206342 0. .0007383
rs4517379 0. .0007383
Page 14
Appendi xB . txt rs632496 0. .0007383
rs7760482 0. .0007387
rsl342404 0. .0007392
rs7420862 0. .0007428
rs275737 0. .0007437
rs2588849 0. .0007438
rs7029062 0. .0007456
rsl0501696 0. .0007463
rs6686154 0. .0007466
rs7537518 0. .0007466
rs873982 0. .0007486
rsl0455430 0. .00075
rsl333201 0. .00075
rs7996728 0. .0007502
rsl949914 0. .0007516
rs2063034 0. .000753
rs2016496 0. .0007532
rs7431080 0. .0007557
rsl573515 0. .0007565
rsl945295 0. .0007565
rs226478 0. .0007591
rs438666 0. .0007592
rsl3092390 0. .0007605
rs9937891 0. .000761
rs4603646 0. .0007621
rsl925558 0. .0007634
rs7914124 0. .0007634
rsl7061059 0. .0007639
rs6560559 0. .0007642
rs440980 0. .0007662
rsl406538 0. .0007681
rs9526913 0. .0007699
rsl513681 0. .0007704
rs9952567 0. .0007704
rs7835485 0. .0007712
rsl7704557 0. .0007715
rs8036702 0. .0007715
rs8037124 0. .0007715
rsl2681932 0. .000774
rsll682773 0. .0007748
rs9399593 0. .000775
rsl393914 0. .0007753
rsll698603 0. .0007779
rsl2625034 0. .0007779
rsl2625431 0. .0007779
rsl2625628 0. .0007779
rsl2625665 0. .0007779
rsl438106 0. .0007779
rsl550266 0. .0007779
rs4254564 0. .0007779
rs4353709 0. .0007779
rs6034368 0. .0007779
rs6034370 0. .0007779
rs6043726 0. .0007779
rs7509079 0. .0007779
rs585721 0. .0007782
rs7222072 0. .0007793
rs4880981 0. .0007826
rsl2063812 0. .000783
rs4839649 0. .0007863
rsll618716 0. .0007868
rsl448822 0. .000787
rs7087620 0. .000788
rs4749914 0. .0007883
rsll245624 0. .0007902
rs3096735 0. .0007905
rs2023256 0. .0007907
rs4710440 0. .0007935
rs6936487 0. .0007936
rs7656857 0. .000794
Page 15
AppendixB.txt rs6914649 0. .0007951
rsl0876266 0. .0007952
rsl0876267 0. .0007952
rsl3121574 0. .0007987
rs7067673 0. .0007992
rs3735530 0. .0008004
rsll845831 0. .0008031
rsl7278718 0. .000804
rsl2005037 0. .0008041
rsl2454081 0. .0008046
rsl2149202 0. .000806
rsl943530 0. .0008061
rslll67538 0. .0008066
rsl2519170 0. .0008066
rs4814547 0. .0008091
rsl513679 0. .0008093
rsl3277059 0. .0008098
rsl0748673 0. .00081
rs2015439 0. .00081
rsl0027730 0. .0008101
rs268899 0. .0008104
rs2225595 0. .0008127
rs7136664 0. .0008146
rs985652 0. .0008156
rsl2510520 0. .0008166
rsl2510610 0. .0008166
rsl3338089 0. .000817
rsl7483533 0. .0008171
rs402617 0. .0008206
rs569420 0. .0008214
rs4319886 0. .0008219
rsl0818876 0. .0008236
rs2895621 0. .0008248
rs7600875 0. .0008261
rsl3123933 0. .0008268
rs7601126 0. .0008273
rsll25335 0. .0008274
rsl2297679 0. .0008288
rsl2303248 0. .0008288
rsl2309427 0. .0008288
rsl388688 0. .0008288
rsl2352641 0. .0008295
rsl889054 0. .0008314
rs2303021 0. .0008315
rs2303022 0. .0008315
rslll27237 0. .0008317
rsl073373 0. .000832
rs2892324 0. .000832
rslll48252 0. .0008322
rsll620062 0. .0008322
rs4886018 0. .0008322
rs7166935 0. .0008325
rsl3105679 0. .000833
rsl6836521 0. .0008337
rs4371301 0. .0008384
rs7616888 0. .0008394
rs2186392 0. .0008397
rs9946213 0. .0008399
rsl924036 0. .0008422
rsl2625207 0. .0008429
rs6043688 0. .0008429
rs4485297 0. .000843
rsl009359 0. .0008444
rsll782123 0. .0008448
rsllll886 0. .0008465
rsl497482 0. .0008473
rsl0257555 0. .0008487
rs980608 0. .0008491
rs949391 0. .0008498
rsl6940979 0. .00085
Page 16
Appendi xB . txt rs6730351 0. .0008508
rslll07218 0. .0008509
rsl7280309 0. .0008524
rs4921281 0. .0008532
rs7664389 0. .0008544
rs2123451 0. .0008552
rs4896534 0. .0008552
rs6905756 0. .0008552
rs9376601 0. .0008552
rs9403280 0. .0008552
rs7338409 0. .0008561
rsl7478082 0. .0008573
rsl2619716 0. .0008574
rsl335307 0. .0008576
rsl722545 0. .0008578
rsl722546 0. .0008578
rs6848514 0. .0008578
rsl2466324 0. .0008581
rsll07436 0. .0008615
rsl2677525 0. .0008626
rs2609115 0. .0008649
rs2301721 0. .0008656
rsll040444 0. .0008659
rs605323 0. .0008672
rs607160 0. .0008672
rsl6950049 0. .0008694
rs6557545 0. .0008695
rs9327842 0. .0008696
rs2248674 0. .0008704
rs4671750 0. .0008714
rs912507 0. .0008723
rslll88735 0. .0008737
rs317221 0. .0008738
rsl2292560 0. .0008766
rs2159106 0. .0008769
rsl557336 0. .0008787
rsl893305 0. .0008788
rsl3360698 0. .0008789
rsl037293 0. .0008799
rsl2149210 0. .00088
rsl907153 0. .00088
rsl701916 0. .0008816
rsl2472272 0. .0008822
rs7418932 0. .0008822
rsll639204 0. .0008825
rs7179938 0. .0008825
rs7179940 0. .0008825
rs6689433 0. .0008838
rs6123426 0. .0008852
rs912512 0. .0008852
rs2387616 0. .0008854
rsl2205984 0. .000886
rs450855 0. .000886
rs2081725 0. .0008887
rsl350072 0. .0008922
rs4949165 0. .0008926
rs6934166 0. .0008931
rs6911292 0. .0008934
rs9657649 0. .000894
rsl2292039 0. .0008947
rs7179747 0. .0008966
rsll668398 0. .0008968
rs4848983 0. .0008984
rsl2797590 0. .0008991
rsl0786281 0. .0009004
rs319920 0. .0009027
rs3792775 0. .000903
rs7999587 0. .0009054
rsl370500 0. .0009058
rs7164397 0. .0009065
Page 17
Appendi xB . txt rsl2643660 0. .0009071
rs6468792 0. .0009071
rs6987380 0. .0009071
rs7769835 0. .0009082
rslll90728 0. .0009084
rs906190 0. .0009101
rsl345170 0. .0009108
rs4839650 0. .0009108
rsl7764682 0. .0009125
rs2636723 0. .000916
rs3742297 0. .0009183
rsl2049174 0. .0009201
rs7829940 0. .0009232
rsl0209582 0. .0009239
rsl2052554 0. .0009239
rsl2053338 0. .0009239
rsl3419898 0. .0009239
rsl3429785 0. .0009239
rs2045041 0. .0009239
rs6746493 0. .0009239
rsl64734 0. .0009241
rsl64735 0. .0009241
rs351689 0. .0009241
rs351693 0. .0009241
rs6838150 0. .0009247
rs914804 0. .0009255
rsl971167 0. .0009265
rs2013356 0. .0009265
rs9965899 0. .0009265
rs2414594 0. .000927
rs2414597 0. .000927
rs2414598 0. .000927
rs2414599 0. .000927
rsl539948 0. .0009274
rsll46931 0. .000928
rsl0076638 0. .0009285
rs7742698 0. .0009289
rsl6962582 0. .0009298
rs7131359 0. .0009319
rs2764609 0. .0009358
rs4483986 0. .0009381
rs4591380 0. .0009382
rs6750501 0. .0009382
rs2256121 0. .0009393
rsl0091905 0. .0009414
rs9482272 0. .0009415
rs7764184 0. .0009423
rsl533172 0. .0009442
rs7096228 0. .0009443
rs4659424 0. .0009459
rs2120054 0. .0009466
rs771620 0. .0009467
rs7608301 0. .0009486
rs608539 0. .0009512
rs611671 0. .0009512
rs9388315 0. .0009517
rs3767999 0. .0009525
rsl0079948 0. .0009534
rsl2995362 0. .0009537
rs2835027 0. .0009553
rsl0876271 0. .0009555
rsl0876272 0. .0009555
rs6545476 0. .0009566
rs4769474 0. .0009571
rs4769475 0. .0009571
rs5022638 0. .0009583
rslll37756 0. .0009589
rslll37757 0. .0009589
rsl049868 0. .0009592
rsl654559 0. .0009616
Page 18
Appendi xB . txt rsl701921 0. .0009616
rs996609 0. .0009628
rs9371462 0. .0009667
rs6921058 0. .0009668
rsl0795234 0. .000967
rsl561231 0. .0009679
rs2118283 0. .0009679
rs2164715 0. .0009679
rs6723870 0. .0009679
rsl0049352 0. .0009692
rsl2476575 0. .0009699
rsl335304 0. .000972
rs6678949 0. .0009722
rsl7593128 0. .0009731
rsl0876270 0. .0009755
rsl7627505 0. .0009756
rs319923 0. .0009756
rs9313918 0. .0009761
rs761228 0. .0009773
rs9977734 0. .0009774
rs7993748 0. .000978
rs9946774 0. .0009786
rsl0882777 0. .0009788
rs4282632 0. .0009797
rs4744313 0. .0009797
rs7239336 0. .0009806
rs4395124 0. .0009808
rsll694900 0. .0009822
rs4799513 0. .0009828
rs6854195 0. .0009836
rsl015669 0. .0009842
rs7714352 0. .0009842
rs7714503 0. .0009842
rs2154652 0. .0009843
rs3864151 0. .0009844
rs7585690 0. .0009844
rs7586111 0. .0009844
rs4767012 0. .0009847
rsl749689 0. .0009848
rsl0765183 0. .0009851
rs7929619 0. .0009851
rs7932640 0. .0009851
rsl613720 0. .0009858
rslll01266 0. .0009871
rsl0737329 0. .0009919
rs4142492 0. .0009919
rs867541 0. .0009919
rs477424 0. .0009937
rs2788872 0. .0009947
rs667213 0. .0009953
rsll747342 0. .0009956
rsl0183953 0. .0009965
rs6545479 0. .0009965
rs6715694 0. .0009965
rs7588591 0. .0009965
rsl2189092 0. .0009975
rs7709412 0. .0009975
rsl0505012 0. .0009983
rs4777023 0. .0009993
rsl981815 0. .0009999
rs834194
rs473467
rs4085813
rs24356
rs6502586
rs4924773
rs6532675
rs4482769
rs6888545
rs420828
Page 19
Appendi xB . txt rs7116127
rs2658787
rs7383045
rs4895590
rs7475020
rs4378287
rs7475023
rs4313469
rs7475188
rs4581344
rs7481282
rs4509797
rs7482394
rs4517513
rs7504838
rs2850277
rs7509079
rs4254566
rs7926062
rs2605589
rsl0936257
rs9810082
rsll084821
rs7249031
rsll635913
rs9788669
rsl2176199
rs9371463
rsl2493604
rs9857513
Page 20
Appendi xB . txt
SNP p
rs7481282 8. . 636E-7
rs9322082 0. .00001371
rs648601 0. .00001859
rsl408577 0. .00001929
rs4323329 0. .00002226
rs4452660 0. .00002226
rs4085813 0. .00002238
rs4945220 0. .00002292
rs650171 0. .00002343
rs7123080 0. .00002343
rs8111760 0. .00002345
rsl7646434 0. .00002376
rsl7702960 0. .00002376
rsl0899404 0. .00002945
rsl7006485 0. .00003101
rsl7646351 0. .00003173
rsl3414513 0. .00003186
rs6712661 0. .00003186
rs735483 0. .00003186
rs7601226 0. .00003186
rs9653407 0. .00003186
rsl7646492 0. .00003213
rsl2711551 0. .00003219
rsl2968184 0. .00003313
rsl3000440 0. .00003348
rsl3413270 0. .00003348
rs2118387 0. .00003348
rs2164796 0. .00003348
rs6711921 0. .00003348
rs9678017 0. .00003348
rsl0177322 0. .00003468
rsl7006496 0. .00003502
rs724403 0. .00003502
rs4344516 0. .0000361
rsl2711559 0. .000037
rs4450992 0. .0000372
rs684813 0. .00003859
rsl6867581 0. .00003915
rs4703388 0. .00003915
rs621456 0. .00003926
rsl954888 0. .00004077
rs7580531 0. .00004105
rs7744769 0. .00004291
rsl0242229 0. .00004375
rsl2615068 0. .00004576
rsl2622908 0. .00004576
rsl7006394 0. .00004576
rs7564564 0. .00004681
rs2157814 0. .00004726
rs4267966 0. .00004741
rsl2614155 0. .00005011
rsll707244 0. .00005025
rsl7050208 0. .00005125
rs6913861 0. .00005196
rsl0936257 0. .00005258
rsl529014 0. .00005471
rs9386176 0. .00005646
rs9399592 0. .00005646
rs9403837 0. .00005646
rs2328774 0. .00005782
rs6554218 0. .00005783
rs4551178 0. .00005824
rsl456243 0. .00005826
rs7116127 0. .00005826
rs4134463 0. .0000585
rsl945747 0. .00005922
rsl0137389 0. .00006177
rsl0496569 0. .00006274
rs477594 0. .00006589
Page 1
Appendi xB . txt rs504973 0. .00006589
rs834194 0. .00006589
rsl0179345 0. .00006609
rs6756225 0. .00006609
rsl3302476 0. .00006648
rs9360640 0. .00006802
rs484363 0. .00006837
rsl365832 0. .00006923
rs4445078 0. .00006973
rsl2614379 0. .00007143
rsl2087475 0. .00007264
rsl3403769 0. .00007504
rs643388 0. .0000771
rs663674 0. .00007742
rs415234 0. .00007831
rs687037 0. .00007853
rsl2073831 0. .00008024
rs6023633 0. .00008146
rs6736269 0. .00008288
rs7772526 0. .00008298
rs6441408 0. .00008446
rsll018434 0. .00008495
rs2594536 0. .0000852
rsl0185512 0. .00008828
rs2034137 0. .00008828
rsl7087674 0. .00008992
rsl456244 0. .00009005
rslll22861 0. .00009285
rs6746090 0. .00009285
rs9840287 0. .00009301
rs2048504 0. .00009427
rs6014185 0. .00009427
rsl420582 0. .0000946
rs668701 0. .00009522
rsl0170935 0. .00009539
rs6714671 0. .00009539
rs7595601 0. .00009539
rs3912845 0. .00009655
rsl7764592 0. .0000985
rsl0496570 0. .00009884
rsl2611458 0. .00009884
rsl3395695 0. .00009884
rs2304560 0. .00009884
rs2304561 0. .00009884
rs6704587 0. .00009884
rs7566558 0. .00009884
rs934761 0. .00009884
rs6541782 0. .0001021
rs6760211 0. .0001021
rsl633749 0. .000103
rs7538154 0. .0001038
rsl0255791 0. .0001039
rs9446844 0. .0001046
rsl2614123 0. .0001058
rsl0184008 0. .000106
rs6064117 0. .0001079
rs7760644 0. .000109
rs877191 0. .00011
rs611232 0. .0001113
rs6912526 0. .0001153
rs911196 0. .0001162
rs2181942 0. .0001182
rsl512065 0. .0001192
rsl0179294 0. .0001196
rsl3395277 0. .0001196
rs6023645 0. .0001201
rs594406 0. .0001204
rs595459 0. .0001204
rs4811538 0. .0001212
rsl505006 0. .0001214
Page 2
Appendi xB . txt rs8180176 0. .000123
rs4848712 0. .0001243
rsl551151 0. .0001253
rs4711162 0. .0001253
rs2034136 0. .0001279
rs7558771 0. .0001279
rs7188211 0. .0001294
rsl628613 0. .0001301
rsl666790 0. .0001301
rsl666797 0. .0001301
rsl700572 0. .0001301
rsl2493604 0. .0001308
rsl388702 0. .0001327
rsl492146 0. .0001327
rsl492147 0. .0001327
rsl2190601 0. .0001328
rs6704842 0. .0001361
rsl2622810 0. .0001364
rs7599081 0. .0001364
rs9653406 0. .0001364
rsl2614362 0. .0001376
rs6729454 0. .0001376
rs669738 0. .0001384
rs2289192 0. .0001396
rs7672513 0. .00014
rsl0498676 0. .0001406
rs3778166 0. .0001406
rsl388705 0. .000144
rs675079 0. .0001444
rs2962621 0. .0001458
rs638807 0. .000146
rs7943055 0. .000147
rs7765767 0. .0001483
rs685553 0. .0001488
rs608382 0. .0001491
rs7700468 0. .000152
rsl057530 0. .0001524
rs488824 0. .0001535
rs553727 0. .0001535
rs611536 0. .0001535
rs947841 0. .0001535
rs9322081 0. .0001545
rs3916911 0. .000156
rsl0942739 0. .0001566
rs7709282 0. .0001566
rs4121744 0. .0001568
rs524874 0. .0001585
rsl0765186 0. .0001588
rs4440336 0. .0001599
rs6872314 0. .0001599
rs7356637 0. .0001599
rsl881665 0. .0001601
rs9386177 0. .0001601
rslll55493 0. .0001617
rslll89415 0. .0001621
rsl881663 0. .0001627
rsl7389893 0. .000165
rsl2419587 0. .0001697
rsl6922585 0. .0001697
rs6541784 0. .0001716
rs2092859 0. .0001741
rs2591107 0. .0001755
rs9468304 0. .0001759
rslll9723 0. .0001781
rsl2662634 0. .0001793
rs4811532 0. .00018
rsl3401792 0. .000182
rsl388706 0. .0001823
rs6023649 0. .0001843
rsl0929465 0. .0001848
Page 3
Appendi xB . txt rs4669141 0. .0001848
rs4804226 0. .0001852
rs8009216 0. .000186
rs7001847 0. .0001888
rsl2440999 0. .0001898
rs2200674 0. .0001898
rsl7766596 0. .0001927
rs2280565 0. .0001928
rsl335955 0. .0001932
rsl889102 0. .0001942
rs2784465 0. .0001942
rs4358853 0. .0001942
rs4685652 0. .000195
rs2678801 0. .0001951
rsl0816127 0. .0001972
rs4271025 0. .0001972
rs4279660 0. .0001972
rs4403465 0. .0001972
rs4892107 0. .0001981
rsl0177273 0. .0002003
rslll5356 0. .0002006
rs2167107 0. .0002006
rs7926062 0. .0002024
rsl023329 0. .000203
rs9620115 0. .000203
rsl0457864 0. .0002047
rs7250467 0. .0002048
rs4804788 0. .0002064
rs4685650 0. .0002065
rs4685651 0. .0002065
rs2328777 0. .0002073
rs9322084 0. .0002073
rs9497675 0. .0002073
rs6747693 0. .0002075
rsl0150607 0. .000208
rsl420577 0. .0002091
rs2827489 0. .0002098
rs2786262 0. .0002099
rsl0969252 0. .0002105
rs687781 0. .0002105
rs4988386 0. .0002129
rs4988388 0. .0002129
rs4988389 0. .0002129
rsl912890 0. .0002133
rsl553047 0. .0002145
rs2412616 0. .0002145
rsl2454494 0. .0002153
rs608240 0. .0002155
rs9497679 0. .0002176
rs2786258 0. .000218
rs595106 0. .000219
rs596159 0. .000219
rs618472 0. .000219
rs652539 0. .000219
rs6679824 0. .0002201
rs6688321 0. .0002201
rsl0969267 0. .0002222
rsl7105190 0. .0002249
rsl7105228 0. .000225
rs2186053 0. .000225
rsl0755432 0. .0002282
rsl591906 0. .0002284
rs6921180 0. .0002289
rs2027733 0. .0002297
rsl532212 0. .0002308
rs6532675 0. .0002309
rsll014929 0. .0002316
rsll014931 0. .0002316
rsll014933 0. .0002316
rsll014935 0. .0002316
Page 4
Appendi xB . txt rsll014936 0. .0002316
rsl2784683 0. .0002316
rs7862503 0. .0002316
rs7894301 0. .0002316
rs4445901 0. .0002341
rs9929708 0. .0002341
rsl559604 0. .0002351
rs9377040 0. .0002354
rsll014932 0. .0002361
rs2368120 0. .0002361
rs4703674 0. .0002367
rs767676 0. .0002367
rs2786263 0. .0002368
rsl3018316 0. .000237
rsl2232770 0. .0002384
rsl6982264 0. .0002393
rsl6870906 0. .0002398
rs4045166 0. .0002419
rsl402436 0. .0002421
rs748040 0. .0002422
rs6717225 0. .0002436
rs4711170 0. .0002465
rs2658785 0. .0002489
rsl2205302 0. .00025
rsl3084500 0. .00025
rs2919051 0. .0002524
rs296325 0. .0002541
rs296329 0. .0002541
rs296333 0. .0002541
rs296334 0. .0002541
rs296318 0. .0002561
rs296319 0. .0002561
rs296320 0. .0002561
rsl0147303 0. .0002574
rsl2718626 0. .0002594
rsl2718627 0. .0002594
rsl2718628 0. .0002594
rs3118041 0. .0002608
rs2295599 0. .0002629
rs7740233 0. .000265
rsl412727 0. .0002658
rs3949639 0. .0002658
rs7043400 0. .0002658
rs2153356 0. .0002667
rs870913 0. .0002667
rs870914 0. .0002667
rs870915 0. .0002667
rs2857682 0. .0002672
rs6023640 0. .0002673
rsl0281294 0. .0002674
rs234589 0. .0002689
rs6023625 0. .0002699
rsl0209628 0. .0002718
rsl892159 0. .0002728
rsl892160 0. .0002732
rs7917879 0. .0002749
rs9535895 0. .0002751
rsl2599944 0. .0002759
rs995365 0. .0002773
rsl595288 0. .0002785
rs234586 0. .000279
rsl7671266 0. .0002792
rs4685654 0. .000281
rsl0853651 0. .0002816
rs4685649 0. .000282
rsl0491676 0. .0002832
rsl0491679 0. .0002832
rsl7698884 0. .0002842
rs2492279 0. .0002846
rsl2278691 0. .0002857
Page 5
AppendixB.txt rsl0069744 0. .0002892
rsl0484891 0. .0002892
rs7871542 0. .0002892
rs4988398 0. .0002896
rsl455048 0. .000294
rsl943559 0. .0002946
rs2839314 0. .0002946
rsl0457082 0. .0002953
rs6541794 0. .0002962
rs6023624 0. .0002981
rsl0448170 0. .0002986
rsl0969241 0. .0002986
rsl0969245 0. .0002986
rsl0969247 0. .0002986
rsl0969248 0. .0002986
rs736508 0. .0003
rsl513680 0. .0003002
rsl838408 0. .0003002
rsl849566 0. .0003002
rsl521034 0. .0003006
rs2139795 0. .0003006
rs2251640 0. .0003012
rs2784464 0. .0003012
rs7231534 0. .0003017
rsl0491681 0. .0003052
rsl998199 0. .0003053
rs582351 0. .0003058
rsll811546 0. .0003061
rsl0969272 0. .0003081
rsl2771164 0. .0003098
rsl0205258 0. .0003102
rs6100191 0. .0003127
rsl943553 0. .0003128
rsl0139222 0. .0003129
rsl2615868 0. .0003137
rsl2711546 0. .0003137
rs6735895 0. .0003137
rsll635771 0. .0003143
rslll2833 0. .0003155
rsl0196761 0. .0003161
rsl0496568 0. .0003161
rsl7006463 0. .0003161
rs6725314 0. .0003161
rs7383045 0. .0003161
rs7599933 0. .0003161
rs7770235 0. .0003161
rs7038904 0. .0003163
rs9293920 0. .0003169
rs7851775 0. .0003177
rsl0490196 0. .0003193
rs4873792 0. .0003196
rsl0510271 0. .0003201
rsl0969230 0. .0003203
rs4233172 0. .000323
rsl344506 0. .0003237
rs7864733 0. .000324
rsl0203617 0. .0003251
rsl398112 0. .0003255
rslll55742 0. .0003258
rsl2611456 0. .0003268
rsl2611457 0. .0003268
rsl7039719 0. .0003268
rs6761493 0. .0003268
rsl355827 0. .000327
rs7239670 0. .000327
rsll084821 0. .0003278
rsl6962574 0. .000328
rs2025129 0. .0003285
rs4323568 0. .0003289
rs6070587 0. .000329
Page 6
Appendi xB . txt rs657426 0. .0003301
rs4685648 0. .0003311
rs7482394 0. .0003312
rs2889741 0. .0003316
rsl0214511 0. .0003325
rsl885235 0. .0003327
rsl0756650 0. .0003332
rs4804787 0. .0003338
rsll920714 0. .0003353
rsl580569 0. .0003353
rs4855516 0. .0003353
rs4855517 0. .0003353
rs4855518 0. .0003353
rs6549147 0. .0003353
rs6764924 0. .0003353
rsl0123940 0. .0003357
rs9468414 0. .000336
rsl335957 0. .0003361
rs2786266 0. .0003361
rs2312587 0. .0003365
rs6477537 0. .0003375
rsl513686 0. .0003391
rsl3146442 0. .0003393
rs7866684 0. .0003402
rsll085134 0. .0003422
rs2901113 0. .0003445
rs2901114 0. .0003445
rs4560873 0. .000345
rs610199 0. .000345
rslll29637 0. .0003451
rs7741525 0. .000346
rs9398017 0. .000346
rs6509137 0. .0003481
rsll920741 0. .0003485
rsl602200 0. .0003485
rsl6960857 0. .0003485
rsl0813132 0. .0003501
rs2067951 0. .0003504
rs7747720 0. .0003517
rsl7802700 0. .0003522
rs4490947 0. .0003524
rs2327566 0. .0003534
rs2492274 0. .0003552
rs2492276 0. .0003552
rsl6942896 0. .0003579
rsl2662569 0. .000358
rs4570560 0. .0003585
rsl895320 0. .0003596
rsl3078681 0. .0003605
rsl3065961 0. .0003615
rsl3076600 0. .0003615
rsl474276 0. .0003618
rs6482531 0. .0003633
rsl0969240 0. .0003635
rsl7698983 0. .0003653
rs2327567 0. .0003653
rs6914579 0. .0003656
rsl593872 0. .0003657
rs9482270 0. .0003671
rs902246 0. .0003679
rs902247 0. .0003679
rs7894273 0. .0003693
rs7899880 0. .0003693
rs7475020 0. .0003694
rsl3300699 0. .0003697
rsl885236 0. .0003697
rsl807403 0. .0003706
rsl0830220 0. .0003715
rs4688519 0. .0003733
rs6509134 0. .0003734
Page 7
Appendi xB . txt rsl041752 0. .0003735
rs2828109 0. .0003735
rs2828110 0. .0003735
rs7998892 0. .000375
rs319919 0. .0003754
rsl0510604 0. .0003758
rsl0481554 0. .0003772
rsl556463 0. .0003788
rs6570450 0. .0003794
rs9403262 0. .0003794
rs4884452 0. .0003805
rs9526845 0. .0003815
rs8087567 0. .0003825
rs6888545 0. .0003832
rsl2904291 0. .0003857
rs7193895 0. .0003858
rs9630225 0. .0003862
rs6502586 0. .0003884
rsl0518270 0. .0003892
rsl893692 0. .0003893
rsl0176760 0. .0003912
rsl943579 0. .0003952
rsl943580 0. .0003952
rsl943581 0. .0003952
rs2591098 0. .0003952
rs2591099 0. .0003952
rs2733134 0. .0003952
rsl943582 0. .0003962
rs2212962 0. .0003962
rs6932538 0. .0004003
rs9341408 0. .0004005
rs597462 0. .0004006
rs8129099 0. .000401
rsll970254 0. .0004022
rs2236426 0. .000403
rsl7108636 0. .0004039
rs2417752 0. .0004066
rsll946608 0. .0004076
rs4468712 0. .0004082
rsl387731 0. .0004093
rsl602199 0. .0004093
rs9812027 0. .0004093
rs991807 0. .0004093
rs991808 0. .0004093
rsl965118 0. .0004134
rs8041853 0. .0004134
rs876535 0. .0004141
rs2088403 0. .0004147
rs789900 0. .0004147
rs761937 0. .0004165
rsll886348 0. .0004167
rsll891264 0. .0004167
rs6716674 0. .0004167
rs6745850 0. .0004167
rs2328194 0. .0004175
rs9321803 0. .0004175
rs4609047 0. .0004194
rsl349710 0. .0004197
rs9321804 0. .0004208
rs7095668 0. .0004211
rsl435684 0. .0004226
rs6911913 0. .0004246
rs9390445 0. .0004246
rsll24329 0. .0004265
rsl0977739 0. .0004278
rsl2610472 0. .0004282
rs3826941 0. .0004282
rs4742595 0. .0004283
rsl368299 0. .0004288
rs8109615 0. .0004305
Page 8
AppendixB.txt rs662041 0. .0004335
rsl7403480 0. .000434
rs789887 0. .000436
rs789888 0. .000436
rs9428429 0. .0004363
rs4703645 0. .00044
rslll22898 0. .0004414
rs3860383 0. .0004414
rs7605443 0. .0004414
rs4912173 0. .0004421
rs8028380 0. .0004424
rsl547872 0. .0004433
rs7504838 0. .0004433
rs7765349 0. .0004446
rs9596651 0. .000445
rsll854288 0. .0004461
rs3759846 0. .0004461
rs6570443 0. .0004465
rsl332207 0. .0004476
rsll073855 0. .0004481
rs8036314 0. .0004481
rs8028882 0. .0004486
rs9806190 0. .0004486
rsll016936 0. .0004502
rs4503789 0. .0004521
rs9376586 0. .0004523
rsl344196 0. .0004524
rs6468799 0. .0004528
rs7015311 0. .0004528
rs3757508 0. .0004533
rs3948710 0. .0004533
rsl0204078 0. .0004539
rsl0207199 0. .0004539
rs6945109 0. .0004539
rsl0867221 0. .0004545
rslll37747 0. .0004545
rsl2339181 0. .0004545
rsl452990 0. .000456
rs6570441 0. .000456
rs9403252 0. .000456
rslll37748 0. .0004567
rs3761743 0. .0004571
rs370177 0. .0004578
rs403461 0. .0004578
rsl7112249 0. .0004586
rslll37755 0. .00046
rs769289 0. .00046
rs8109313 0. .0004607
rsl0835824 0. .0004609
rsl2986567 0. .0004619
rsl6831392 0. .0004628
rsll853075 0. .0004629
rsl6960864 0. .0004629
rsl0508710 0. .0004638
rsl2248210 0. .0004638
rsl2252825 0. .0004638
rsl2253015 0. .0004638
rsl2260321 0. .0004638
rsl2263561 0. .0004638
rsl2267071 0. .0004638
rsl2765561 0. .0004638
rsl2766929 0. .0004638
rsl2767114 0. .0004638
rsl2768879 0. .0004638
rsl2770526 0. .0004638
rsl2771414 0. .0004638
rsl2773856 0. .0004638
rsl2776584 0. .0004638
rsl2781790 0. .0004638
rsl521029 0. .0004638
Page 9
Appendi xB . txt rsl521030 0. .0004638
rsl521032 0. .0004638
rsl546702 0. .0004638
rsl7739106 0. .0004638
rs2176937 0. .0004638
rs3758441 0. .0004638
rs3758443 0. .0004638
rs3758444 0. .0004638
rs3817419 0. .0004638
rs4581343 0. .0004638
rs4631780 0. .0004638
rs5012431 0. .0004638
rs7084483 0. .0004638
rs7095982 0. .0004638
rs7096274 0. .0004638
rs7097387 0. .0004638
rs7475023 0. .0004638
rs7475188 0. .0004638
rsl352638 0. .0004646
rs4484195 0. .0004646
rsll049887 0. .0004688
rsl480630 0. .0004688
rsl452989 0. .0004689
rs7872398 0. .0004689
rs7989297 0. .0004704
rsl2243741 0. .0004719
rsl2248769 0. .0004719
rsl2249006 0. .0004719
rsl2263998 0. .0004719
rsl2780744 0. .0004719
rs7893838 0. .0004719
rs7915315 0. .0004719
rs3937845 0. .0004723
rs4771400 0. .0004723
rs4855515 0. .0004723
rs7621668 0. .0004723
rs7635448 0. .0004723
rsl489995 0. .0004733
rs6748226 0. .000474
rsll897514 0. .0004765
rs2170466 0. .0004776
rs7529541 0. .0004783
rsl2676502 0. .0004809
rsl0497107 0. .0004811
rsl6831399 0. .0004811
rs7452495 0. .0004842
rs7500154 0. .0004854
rs399355 0. .0004878
rsl3208784 0. .0004884
rsll073091 0. .0004921
rsll073092 0. .0004921
rsll635913 0. .0004921
rs6495766 0. .0004921
rs8031712 0. .0004921
rs8041062 0. .0004921
rs8041339 0. .0004921
rs4298240 0. .0004923
rs4704170 0. .0004923
rsl0765819 0. .0004936
rs6885454 0. .0004946
rs9390449 0. .0004947
rsl6831410 0. .0004961
rs6560561 0. .0004971
rs9403836 0. .0004984
rsll33174 0. .0004993
rsl0969259 0. .0004994
rs679094 0. .0004994
rsl2289316 0. .0005001
rs2070435 0. .0005002
rsl3264258 0. .0005011
Page 10
Appendi xB . txt rs7042831 0. .0005017
rsl414121 0. .000503
rsl6855165 0. .0005031
rsl873263 0. .0005049
rsl7406994 0. .0005058
rs6468794 0. .0005058
rs6468796 0. .0005058
rsl0093531 0. .0005069
rsl0107399 0. .0005069
rsll987293 0. .0005069
rsll989758 0. .0005069
rsll855819 0. .0005077
rs2356558 0. .000508
rs4544345 0. .000508
rs4140424 0. .0005085
rs6076819 0. .0005085
rs6076820 0. .0005085
rs6076823 0. .0005085
rs6516026 0. .0005085
rs234595 0. .0005095
rsl0152716 0. .0005105
rsl0519999 0. .0005105
rsl0520001 0. .0005105
rsll637062 0. .0005105
rsll853444 0. .0005105
rsll853446 0. .0005105
rsl455047 0. .0005105
rsl6960879 0. .0005105
rsl6960916 0. .0005105
rs8038618 0. .0005105
rs8040254 0. .0005105
rsl0488687 0. .0005112
rs6039529 0. .0005141
rs6056764 0. .0005141
rs341870 0. .0005146
rsl0515405 0. .0005147
rsl349541 0. .0005178
rs4241220 0. .0005178
rs9858963 0. .0005182
rs6936461 0. .0005183
rs9497673 0. .0005183
rs3118045 0. .0005216
rs212293 0. .0005221
rs567990 0. .000524
rsll632343 0. .000525
rsll636113 0. .000525
rsl455045 0. .000525
rs8034582 0. .000525
rs8034766 0. .000525
rs6576603 0. .0005251
rs7165604 0. .0005251
rsl0107160 0. .0005258
rsl2203394 0. .000526
rsl0129671 0. .000528
rsl0483588 0. .000528
rsl2586169 0. .000528
rsl2588980 0. .000528
rsl3075703 0. .0005282
rsl354439 0. .0005282
rs7871453 0. .0005323
rs2850287 0. .0005334
rs534815 0. .0005352
rs2277882 0. .0005383
rs7043954 0. .0005383
rsll629935 0. .0005422
rsl431603 0. .0005461
rs2163996 0. .000547
rs4373347 0. .000547
rsl452988 0. .0005474
rsl489992 0. .0005476
Page 11
Appendi xB . txt rsl7537990 0. .0005476
rsl0491673 0. .0005485
rsl408508 0. .0005485
rsl0767906 0. .0005493
rsl2221893 0. .0005493
rsl0418179 0. .0005497
rs6689022 0. .0005542
rs7539805 0. .0005542
rsl0064203 0. .0005544
rs6495767 0. .0005545
rs684371 0. .0005599
rs2828132 0. .0005603
rs4896533 0. .0005623
rsll676548 0. .0005633
rsl489993 0. .0005669
rsll947379 0. .0005687
rsl746338 0. .0005689
rs3823764 0. .0005695
rsl7154523 0. .0005714
rs6468793 0. .0005725
rsl2176199 0. .0005741
rsl3269411 0. .0005775
rsl405252 0. .0005776
rs6916676 0. .0005796
rsll923978 0. .0005808
rs6711537 0. .0005816
rs6730732 0. .0005816
rsl0969221 0. .0005818
rsl2376718 0. .0005818
rsl6851002 0. .0005824
rs9946863 0. .0005827
rsll678315 0. .0005834
rsl529013 0. .0005852
rsl3257327 0. .0005855
rs4666283 0. .0005865
rsl3377546 0. .0005889
rs6810192 0. .0005952
rsl595286 0. .0005958
rs7646856 0. .0005984
rs2138823 0. .0005987
rs2138824 0. .0005987
rs2176431 0. .0005987
rs8104694 0. .0005987
rs663651 0. .0005994
rs4131293 0. .0005996
rs4131455 0. .0006005
rsll31497 0. .0006007
rs6570784 0. .000601
rs4284720 0. .0006015
rsl70347 0. .000603
rs296323 0. .0006035
rs296328 0. .0006035
rs296335 0. .0006035
rs4740981 0. .0006042
rsl943545 0. .0006062
rsl954972 0. .0006062
rs2591104 0. .0006062
rs2733113 0. .0006062
rs2850276 0. .0006062
rsl943555 0. .0006064
rsl332204 0. .0006065
rsl332206 0. .0006065
rs3902451 0. .0006065
rs6914395 0. .0006067
rsl901515 0. .0006075
rsll237338 0. .0006098
rsl540023 0. .0006098
rsl7429236 0. .0006098
rsl7501198 0. .0006098
rsl943546 0. .0006098
Page 12
Appendi xB . txt rs2097049 0. .0006098
rs2591102 0. .0006098
rs9990383 0. .0006098
rsl0106459 0. .0006138
rs2278155 0. .0006145
rs967444 0. .0006151
rs414509 0. .0006181
rs4839651 0. .0006194
rs6440181 0. .0006194
rsl3258631 0. .0006196
rs890343 0. .000621
rs4326011 0. .0006213
rsl481110 0. .0006225
rsll607512 0. .000624
rsl567819 0. .0006251
rs4734595 0. .0006254
rs7667878 0. .0006261
rslll07212 0. .0006279
rs9490520 0. .0006285
rs8086418 0. .0006292
rsl0781390 0. .0006298
rs9749801 0. .0006324
rs4452425 0. .0006327
rs944559 0. .0006327
rsl0813114 0. .0006347
rs3918322 0. .000635
rs7319214 0. .0006355
rsll56491 0. .000637
rs2504906 0. .0006382
rsll097562 0. .0006383
rsl0813115 0. .0006391
rsl7709654 0. .0006391
rs7745871 0. .0006407
rs6468797 0. .0006434
rs6468798 0. .0006434
rs7925289 0. .0006499
rs6663538 0. .0006506
rsl575054 0. .0006533
rsl7090631 0. .0006562
rs6449263 0. .0006564
rsl2279880 0. .0006572
rsl823507 0. .0006572
rs7115801 0. .0006572
rsl7671496 0. .0006632
rs6453116 0. .0006632
rs6890143 0. .0006632
rs6890320 0. .0006632
rs6893216 0. .0006632
rs717587 0. .0006632
rs6668923 0. .0006636
rsl408507 0. .0006639
rs319924 0. .000664
rs319925 0. .000664
rs6100193 0. .000664
rs2121777 0. .0006647
rs7681041 0. .0006666
rsl0876268 0. .0006675
rsl532763 0. .0006693
rs2209168 0. .0006702
rs2588844 0. .0006712
rs8122333 0. .0006718
rsl0497108 0. .0006725
rsl0497111 0. .0006725
rsl6823807 0. .0006725
rsl0961885 0. .000673
rsl407978 0. .000673
rs427608 0. .0006739
rs451388 0. .0006739
rs3754205 0. .0006745
rs9965748 0. .0006781
Page 13
Appendi xB . txt rs875429 0. .0006792
rs7871676 0. .0006819
rsl7752458 0. .0006822
rs7745473 0. .0006822
rsl0464926 0. .0006833
rsl0464928 0. .0006833
rsll787096 0. .0006833
rsl2679840 0. .0006833
rsl2680350 0. .0006833
rsl543010 0. .0006833
rs9293488 0. .000684
rsl2711699 0. .0006843
rs2421357 0. .0006843
rsl974868 0. .0006848
rs2305317 0. .0006858
rsl2066808 0. .0006862
rsl6840486 0. .0006874
rs292209 0. .0006876
rs9376605 0. .0006901
rs756274 0. .0006926
rs7336398 0. .0006934
rs7039335 0. .0006974
rs627387 0. .0006978
rsll261299 0. .0006982
rs7534106 0. .0006986
rs493412 0. .0006989
rsl7054953 0. .0006996
rs403668 0. .0006996
rs4368235 0. .0007
rs7106157 0. .0007007
rsl862245 0. .0007025
rs986861 0. .0007037
rs7452823 0. .0007051
rsl2441919 0. .0007053
rs6688496 0. .0007057
rslll06529 0. .0007058
rs6934306 0. .000709
rs978960 0. .000709
rs598741 0. .0007093
rs622020 0. .0007093
rs7046871 0. .0007102
rs9536632 0. .0007103
rsl3243392 0. .0007121
rsl2319366 0. .0007123
rs601519 0. .0007132
rsl0790449 0. .0007143
rs4729093 0. .0007143
rs6468795 0. .0007144
rsl6831413 0. .0007156
rsl2368136 0. .0007159
rsl480639 0. .0007159
rsl0876257 0. .000718
rsl2149168 0. .0007181
rs2854516 0. .0007225
rs4236869 0. .0007253
rs7345130 0. .0007269
rs3935754 0. .0007284
rsll892222 0. .0007302
rs4803668 0. .0007322
rs4242641 0. .0007326
rs4895591 0. .0007326
rs6570456 0. .0007326
rsl0786282 0. .000733
rsl0736107 0. .0007335
rs6721161 0. .0007336
rsl2308231 0. .0007337
rsl013507 0. .0007338
rsl225740 0. .0007341
rsl0206342 0. .0007383
rs4517379 0. .0007383
Page 14
Appendi xB . txt rs632496 0. .0007383
rs7760482 0. .0007387
rsl342404 0. .0007392
rs7420862 0. .0007428
rs275737 0. .0007437
rs2588849 0. .0007438
rs7029062 0. .0007456
rsl0501696 0. .0007463
rs6686154 0. .0007466
rs7537518 0. .0007466
rs873982 0. .0007486
rsl0455430 0. .00075
rsl333201 0. .00075
rs7996728 0. .0007502
rsl949914 0. .0007516
rs2063034 0. .000753
rs2016496 0. .0007532
rs7431080 0. .0007557
rsl573515 0. .0007565
rsl945295 0. .0007565
rs226478 0. .0007591
rs438666 0. .0007592
rsl3092390 0. .0007605
rs9937891 0. .000761
rs4603646 0. .0007621
rsl925558 0. .0007634
rs7914124 0. .0007634
rsl7061059 0. .0007639
rs6560559 0. .0007642
rs440980 0. .0007662
rsl406538 0. .0007681
rs9526913 0. .0007699
rsl513681 0. .0007704
rs9952567 0. .0007704
rs7835485 0. .0007712
rsl7704557 0. .0007715
rs8036702 0. .0007715
rs8037124 0. .0007715
rsl2681932 0. .000774
rsll682773 0. .0007748
rs9399593 0. .000775
rsl393914 0. .0007753
rsll698603 0. .0007779
rsl2625034 0. .0007779
rsl2625431 0. .0007779
rsl2625628 0. .0007779
rsl2625665 0. .0007779
rsl438106 0. .0007779
rsl550266 0. .0007779
rs4254564 0. .0007779
rs4353709 0. .0007779
rs6034368 0. .0007779
rs6034370 0. .0007779
rs6043726 0. .0007779
rs7509079 0. .0007779
rs585721 0. .0007782
rs7222072 0. .0007793
rs4880981 0. .0007826
rsl2063812 0. .000783
rs4839649 0. .0007863
rsll618716 0. .0007868
rsl448822 0. .000787
rs7087620 0. .000788
rs4749914 0. .0007883
rsll245624 0. .0007902
rs3096735 0. .0007905
rs2023256 0. .0007907
rs4710440 0. .0007935
rs6936487 0. .0007936
rs7656857 0. .000794
Page 15
AppendixB.txt rs6914649 0. .0007951
rsl0876266 0. .0007952
rsl0876267 0. .0007952
rsl3121574 0. .0007987
rs7067673 0. .0007992
rs3735530 0. .0008004
rsll845831 0. .0008031
rsl7278718 0. .000804
rsl2005037 0. .0008041
rsl2454081 0. .0008046
rsl2149202 0. .000806
rsl943530 0. .0008061
rslll67538 0. .0008066
rsl2519170 0. .0008066
rs4814547 0. .0008091
rsl513679 0. .0008093
rsl3277059 0. .0008098
rsl0748673 0. .00081
rs2015439 0. .00081
rsl0027730 0. .0008101
rs268899 0. .0008104
rs2225595 0. .0008127
rs7136664 0. .0008146
rs985652 0. .0008156
rsl2510520 0. .0008166
rsl2510610 0. .0008166
rsl3338089 0. .000817
rsl7483533 0. .0008171
rs402617 0. .0008206
rs569420 0. .0008214
rs4319886 0. .0008219
rsl0818876 0. .0008236
rs2895621 0. .0008248
rs7600875 0. .0008261
rsl3123933 0. .0008268
rs7601126 0. .0008273
rsll25335 0. .0008274
rsl2297679 0. .0008288
rsl2303248 0. .0008288
rsl2309427 0. .0008288
rsl388688 0. .0008288
rsl2352641 0. .0008295
rsl889054 0. .0008314
rs2303021 0. .0008315
rs2303022 0. .0008315
rslll27237 0. .0008317
rsl073373 0. .000832
rs2892324 0. .000832
rslll48252 0. .0008322
rsll620062 0. .0008322
rs4886018 0. .0008322
rs7166935 0. .0008325
rsl3105679 0. .000833
rsl6836521 0. .0008337
rs4371301 0. .0008384
rs7616888 0. .0008394
rs2186392 0. .0008397
rs9946213 0. .0008399
rsl924036 0. .0008422
rsl2625207 0. .0008429
rs6043688 0. .0008429
rs4485297 0. .000843
rsl009359 0. .0008444
rsll782123 0. .0008448
rsllll886 0. .0008465
rsl497482 0. .0008473
rsl0257555 0. .0008487
rs980608 0. .0008491
rs949391 0. .0008498
rsl6940979 0. .00085
Page 16
Appendi xB . txt rs6730351 0. .0008508
rslll07218 0. .0008509
rsl7280309 0. .0008524
rs4921281 0. .0008532
rs7664389 0. .0008544
rs2123451 0. .0008552
rs4896534 0. .0008552
rs6905756 0. .0008552
rs9376601 0. .0008552
rs9403280 0. .0008552
rs7338409 0. .0008561
rsl7478082 0. .0008573
rsl2619716 0. .0008574
rsl335307 0. .0008576
rsl722545 0. .0008578
rsl722546 0. .0008578
rs6848514 0. .0008578
rsl2466324 0. .0008581
rsll07436 0. .0008615
rsl2677525 0. .0008626
rs2609115 0. .0008649
rs2301721 0. .0008656
rsll040444 0. .0008659
rs605323 0. .0008672
rs607160 0. .0008672
rsl6950049 0. .0008694
rs6557545 0. .0008695
rs9327842 0. .0008696
rs2248674 0. .0008704
rs4671750 0. .0008714
rs912507 0. .0008723
rslll88735 0. .0008737
rs317221 0. .0008738
rsl2292560 0. .0008766
rs2159106 0. .0008769
rsl557336 0. .0008787
rsl893305 0. .0008788
rsl3360698 0. .0008789
rsl037293 0. .0008799
rsl2149210 0. .00088
rsl907153 0. .00088
rsl701916 0. .0008816
rsl2472272 0. .0008822
rs7418932 0. .0008822
rsll639204 0. .0008825
rs7179938 0. .0008825
rs7179940 0. .0008825
rs6689433 0. .0008838
rs6123426 0. .0008852
rs912512 0. .0008852
rs2387616 0. .0008854
rsl2205984 0. .000886
rs450855 0. .000886
rs2081725 0. .0008887
rsl350072 0. .0008922
rs4949165 0. .0008926
rs6934166 0. .0008931
rs6911292 0. .0008934
rs9657649 0. .000894
rsl2292039 0. .0008947
rs7179747 0. .0008966
rsll668398 0. .0008968
rs4848983 0. .0008984
rsl2797590 0. .0008991
rsl0786281 0. .0009004
rs319920 0. .0009027
rs3792775 0. .000903
rs7999587 0. .0009054
rsl370500 0. .0009058
rs7164397 0. .0009065
Page 17
Appendi xB . txt rsl2643660 0. .0009071
rs6468792 0. .0009071
rs6987380 0. .0009071
rs7769835 0. .0009082
rslll90728 0. .0009084
rs906190 0. .0009101
rsl345170 0. .0009108
rs4839650 0. .0009108
rsl7764682 0. .0009125
rs2636723 0. .000916
rs3742297 0. .0009183
rsl2049174 0. .0009201
rs7829940 0. .0009232
rsl0209582 0. .0009239
rsl2052554 0. .0009239
rsl2053338 0. .0009239
rsl3419898 0. .0009239
rsl3429785 0. .0009239
rs2045041 0. .0009239
rs6746493 0. .0009239
rsl64734 0. .0009241
rsl64735 0. .0009241
rs351689 0. .0009241
rs351693 0. .0009241
rs6838150 0. .0009247
rs914804 0. .0009255
rsl971167 0. .0009265
rs2013356 0. .0009265
rs9965899 0. .0009265
rs2414594 0. .000927
rs2414597 0. .000927
rs2414598 0. .000927
rs2414599 0. .000927
rsl539948 0. .0009274
rsll46931 0. .000928
rsl0076638 0. .0009285
rs7742698 0. .0009289
rsl6962582 0. .0009298
rs7131359 0. .0009319
rs2764609 0. .0009358
rs4483986 0. .0009381
rs4591380 0. .0009382
rs6750501 0. .0009382
rs2256121 0. .0009393
rsl0091905 0. .0009414
rs9482272 0. .0009415
rs7764184 0. .0009423
rsl533172 0. .0009442
rs7096228 0. .0009443
rs4659424 0. .0009459
rs2120054 0. .0009466
rs771620 0. .0009467
rs7608301 0. .0009486
rs608539 0. .0009512
rs611671 0. .0009512
rs9388315 0. .0009517
rs3767999 0. .0009525
rsl0079948 0. .0009534
rsl2995362 0. .0009537
rs2835027 0. .0009553
rsl0876271 0. .0009555
rsl0876272 0. .0009555
rs6545476 0. .0009566
rs4769474 0. .0009571
rs4769475 0. .0009571
rs5022638 0. .0009583
rslll37756 0. .0009589
rslll37757 0. .0009589
rsl049868 0. .0009592
rsl654559 0. .0009616
Page 18
Appendi xB . txt rsl701921 0. .0009616
rs996609 0. .0009628
rs9371462 0. .0009667
rs6921058 0. .0009668
rsl0795234 0. .000967
rsl561231 0. .0009679
rs2118283 0. .0009679
rs2164715 0. .0009679
rs6723870 0. .0009679
rsl0049352 0. .0009692
rsl2476575 0. .0009699
rsl335304 0. .000972
rs6678949 0. .0009722
rsl7593128 0. .0009731
rsl0876270 0. .0009755
rsl7627505 0. .0009756
rs319923 0. .0009756
rs9313918 0. .0009761
rs761228 0. .0009773
rs9977734 0. .0009774
rs7993748 0. .000978
rs9946774 0. .0009786
rsl0882777 0. .0009788
rs4282632 0. .0009797
rs4744313 0. .0009797
rs7239336 0. .0009806
rs4395124 0. .0009808
rsll694900 0. .0009822
rs4799513 0. .0009828
rs6854195 0. .0009836
rsl015669 0. .0009842
rs7714352 0. .0009842
rs7714503 0. .0009842
rs2154652 0. .0009843
rs3864151 0. .0009844
rs7585690 0. .0009844
rs7586111 0. .0009844
rs4767012 0. .0009847
rsl749689 0. .0009848
rsl0765183 0. .0009851
rs7929619 0. .0009851
rs7932640 0. .0009851
rsl613720 0. .0009858
rslll01266 0. .0009871
rsl0737329 0. .0009919
rs4142492 0. .0009919
rs867541 0. .0009919
rs477424 0. .0009937
rs2788872 0. .0009947
rs667213 0. .0009953
rsll747342 0. .0009956
rsl0183953 0. .0009965
rs6545479 0. .0009965
rs6715694 0. .0009965
rs7588591 0. .0009965
rsl2189092 0. .0009975
rs7709412 0. .0009975
rsl0505012 0. .0009983
rs4777023 0. .0009993
rsl981815 0. .0009999
rs834194
rs473467
rs4085813
rs24356
rs6502586
rs4924773
rs6532675
rs4482769
rs6888545
rs420828
Page 19
Appendi xB . txt rs7116127
rs2658787
rs7383045
rs4895590
rs7475020
rs4378287
rs7475023
rs4313469
rs7475188
rs4581344
rs7481282
rs4509797
rs7482394
rs4517513
rs7504838
rs2850277
rs7509079
rs4254566
rs7926062
rs2605589
rsl0936257
rs9810082
rsll084821
rs7249031
rsll635913
rs9788669
rsl2176199
rs9371463
rsl2493604
rs9857513
Page 20
Claims
A method of treating a subject having a metabolic disorder, the method comprising:
(a) obtaining a biological sample from the subject;
(b) evaluating the sample for the presence or absence of at least one genetic indicator, wherein the at least one genetic indicator is selected from a single nucleotide polymorphism and a level of gene expression within a reference range; and
(c) performing a first metabolic procedure on the subject, if the at least one genetic indicator is absent, or (d) if the at least one genetic indicator is present, performing a second metabolic procedure on the subject, wherein the second metabolic procedure is different from the first metabolic procedure.
A method of treating a weight-related disorder in a subject comprising:
(a) obtaining a sample comprising nucleic acids from the subject;
(b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; and
(c) based on if the genetic indicator(s) is absent in (b), performing a first metabolic procedure on the subject, or if the genetic indicator(s) is present in (b), performing a second metabolic procedure on the subject, wherein the second metabolic procedure is different from the first metabolic procedure.
The method of claim 2, wherein the second metabolic procedure excludes bariatric surgery.
The method of claim 2, wherein the nucleic acids are deoxyribonucleic acids (DNA).
The method of claim 2, wherein the nucleic acids are positive for the indicator(s).
The method of claim 2, wherein the nucleic acids are negative for the indicator(s).
The method of claim 2, wherein the genetic indicator(s) is at least one single nucleotide polymorphism (SNP) selected from the SNPs shown in Appendix A (SEQ ID NOs 129- 837), Appendix B, or Appendix C.
8. The method of claim 7, wherein the at least one single nucleotide polymorphism (SNP) is selected from the SNPs shown in Appendix A. (SEQ ID NOs 129-837).
9. The method of claim 7, wherein the absence of the SNP correlates with therapeutically effective weight loss of at least 20% weight change after the metabolic procedure in the subject.
10. The method of claim 2, further comprising obtaining a clinical measurement in the
subject prior to step (c).
11. The method of claim 10, wherein the clinical measurement is at least one of a preoperative body mass index (BMI), a glucose tolerance, bile acid profile, and body composition/fat distribution of the subject.
12. The method of claim 11, wherein the clinical measurement is the BMI of the subject.
13. The method of claim 12, wherein the nucleic acids are negative for the indicator(s) and the pre-operative BMI of the subject is greater than 23 kg/m .
14. A method of treating a subject having a metabolic disorder, the method comprising:
(a) obtaining a biological sample from the subject;
(b) evaluating expression of at least one gene in the sample, wherein the gene is differentially expressed after bariatric surgery;
(c) comparing the expression level of the gene(s) evaluated in (b) to a reference range,
if expression of the gene(s) is outside the reference range, performing a first metabolic procedure on the subject, or if expression of the gene is inside the reference range, performing a second metabolic procedure on the subject.
15. The method of claim 14, wherein the second metabolic procedure excludes bariatric surgery.
16. The method of claim 14, wherein the gene(s) are selected from SEQ ID NOs 1-128.
17. The method of claim 14, wherein the reference range of gene expression is +20% of an average determined from multiple patients having undergone bariatric surgery.
18. The method of claim 14, wherein the first metabolic procedure is a surgical procedure.
19. The method of claim 18, wherein the surgical procedure is selected from the group
consisting of gastric bypass, Roux-en-Y gastric bypass (RYGB), biliopancreatic diversion, partial gastrectomy procedures such as vertical sleeve gastrectomy, adjustable gastric banding, duodenal switch, duodenojejunal bypass, vertical banded gastroplasty, intragastric balloon therapy, greater curvature plication, gastric plication, Magenstrasse and Mill, ileal transposition or interposition, small bowel transposition, biliary diversion, procedures involving anastomotic connections of the gastrointestinal tract, gastric balloon implantation and other gastric or intestinal device implantation, gastric, duodenal or intestinal endoluminal barrier implantation, gastric electrical stimulation, small bowel electrical stimulation, vagal electrical stimulation, and vagal electrical inhibition.
20. The method of claim 15, wherein the second metabolic procedure is selected from the group consisting of (a) administering hormone, neuropeptide, receptor agonists or antagonists, (b) other pharmacological or nutritional therapies, (c) activation of brown adipose tissue, and (d) providing an alternative medical device based therapy, such as, but not limited to providing duodenal endoluminal barrier.
21. The method of claim 14, wherein the method further comprises obtaining a clinical
measurement in the subject prior to step (c).
22. The method of claim 21, wherein the clinical measurement is at least one of a preoperative body mass index (BMI), a glucose tolerance, bile acid profile, and body composition/fat distribution of the subject.
23. The method of claim 22, wherein the clinical measurement is the BMI of the subject.
24. A kit for assessing the presence of a single nucleotide polymorphism (SNP) shown in Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C in a sample
comprising:
a pair of primers that specifically hybridize to regions proximal to the SNP selected from Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C; and reagents for polymerase chain reaction (PCR).
25. The method of using the kit of claim 24 comprising:
(a) obtaining a sample comprising nucleic acids from the subject;
(b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators; and
(c) if the genetic indicator(s) is absent in (b), performing a first metabolic procedure, or if the genetic indicator(s) is present in (b), performing an alternative second metabolic procedure.
26. The method of claim 25, wherein the second metabolic procedure excludes bariatric surgery.
27. A method of treating a weight-related disorder in a subject comprising:
(a) obtaining a sample comprising nucleic acids from the subject;
(b) evaluating the nucleic acids for an absence or presence of one or more genetic indicators;
(c) predicting an outcome of performing a first metabolic procedure based on the absence or presence of the genetic indicator(s); and
(d) performing the first metabolic procedure or performing an alternative second metabolic procedure based on the predicted outcome.
28. The method of claim 27, wherein the second metabolic procedure excludes bariatric surgery.
29. The method of claim 27, wherein the genetic indicator(s) is at least one single nucleotide polymorphism (SNP) selected from Appendix A (SEQ ID NOs 129-837), Appendix B, or Appendix C.
30. The method of claim 29, wherein the outcome is a therapeutically effective weight loss and the genetic indicator(s) is absent.
31. The method of claim 29, wherein the outcome is a therapeutically effective weight loss and the metabolic procedure is performed in the absence of the genetic indicator(s).
32. The method of claim 27, wherein the outcome is therapeutically effective weight loss of at least 20% weight change.
33. The method of claim 27, wherein the alternative second metabolic procedure is
performed in the presence of the genetic indicator(s).
34. The method of claim 27, wherein the outcome is at least one of (1) amelioration of or reduction of at least one weight-related co-morbid condition and (2) an adverse metabolic event.
35. The method of claim 34, wherein the co-morbid condition is at least one of hypertension, dyslipidemia, diabetes, acid reflux, fatty liver disease, steatohepatitis, heart disease, depression, sleep apnea, asthma, osteoarthritis, compression fractures, gallstones, lymphoedema, urinary incontinence, stroke, cancer and/or other metabolic syndromes.
36. The method of claim 27, further comprising obtaining a clinical measurement in the subject prior to step (c).
37. The method of claim 36, wherein the clinical measurement is at least one of a preoperative body mass index (BMI), a glucose tolerance, bile acid profile, and body composition/fat distribution of the subject.
38. The method of claim 37, wherein the clinical measurement is the BMI of the subject.
39. The method of claim 27, wherein the step of predicting the outcome comprises inputting the subject's patient data into a metabolic procedure outcome prediction system.
40. The method of claim 39, wherein the patient data comprises the evaluation of the absence or presence of the genetic indicator(s).
41. The method of claim 40, wherein the patient data further comprises a clinical measurement of at least one of a pre-operative body mass index (BMI), a glucose tolerance, bile acid profile, and body composition/fat distribution of the subject.
42. A method of treating a metabolic disorder in a subject, the method comprising:
(a) measuring expression of the gene(s) in a sample from the subject;
(b) comparing the expression level of the gene(s) to a reference range of expression of the gene, wherein the reference range is determined from multiple patients having undergone a bariatric surgery; and
(c) administering to the subject a composition that modulates expression of the gene(s) to the mimic expression after bariatric surgery, thereby treating the metabolic disorder.
43. The method of claim 42, wherein the gene(s) are at least one of SEQ ID NOs 1-128.
44. The method of claim 42, wherein the method results in a therapeutically significant
weight loss.
45. The method of claim 44, wherein the therapeutically significant weight loss is at least a 20% body weight change or an amelioration of or reduction of at least one weight-related co-morbid condition.
46. The method of claim 45, wherein the co-morbid condition is at least one of hypertension, dyslipidemia, diabetes, acid reflux, fatty liver disease, steatohepatitis, heart disease, depression, sleep apnea, asthma, osteoarthritis, compression fractures, gallstones, lymphodema, urinary incontinence, stroke, cancer and/or other metabolic syndromes.
47. A kit for assessing genetic variation in at least one gene associated with response to a metabolic procedure in a sample comprising:
a pair of primers that specifically hybridize to an expression product of the gene(s) selected from SEQ ID NOs 1-128; and
reagents for quantitative polymerase chain reaction (qPCR).
Use of a single nucleotide polymorphism to evaluate a course of treatment for a metabolic disorder.
Use of a gene expression level to evaluate a course of treatment for a metabolic disorder.
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP13839109.9A EP2898101A4 (en) | 2012-09-21 | 2013-09-20 | CLINICAL PREDICTORS OF WEIGHT LOSS |
Applications Claiming Priority (8)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US201261704077P | 2012-09-21 | 2012-09-21 | |
| US201261704434P | 2012-09-21 | 2012-09-21 | |
| US61/704,077 | 2012-09-21 | ||
| US61/704,434 | 2012-09-21 | ||
| US201261740678P | 2012-12-21 | 2012-12-21 | |
| US61/740,678 | 2012-12-21 | ||
| US13/828,809 US20140087999A1 (en) | 2012-09-21 | 2013-03-14 | Clinical predictors of weight loss |
| US13/828,809 | 2013-03-14 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2014047432A1 true WO2014047432A1 (en) | 2014-03-27 |
Family
ID=50341966
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2013/060901 Ceased WO2014047432A1 (en) | 2012-09-21 | 2013-09-20 | Clinical predictors of weight loss |
Country Status (3)
| Country | Link |
|---|---|
| US (2) | US11236392B2 (en) |
| EP (1) | EP2898101A4 (en) |
| WO (1) | WO2014047432A1 (en) |
Families Citing this family (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10242756B2 (en) | 2012-09-21 | 2019-03-26 | Ethicon Endo-Surgery, Inc. | Systems and methods for predicting metabolic and bariatric surgery outcomes |
| CA3080932A1 (en) | 2017-11-22 | 2019-05-31 | Mayo Foundation For Medical Education And Research | Methods and materials for assessing and treating obesity |
| CN112501318B (en) * | 2020-12-30 | 2022-07-12 | 华南农业大学 | Chicken growth trait related TMEM18 gene molecular marker and application |
| WO2022246203A1 (en) * | 2021-05-21 | 2022-11-24 | Mayo Foundation For Medical Education And Research | Assessing and treating obesity |
| US20260078411A1 (en) * | 2022-09-05 | 2026-03-19 | Daewoong Pharmaceutical Co., Ltd. | Novel genomic safe harbor and use thereof |
Citations (8)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20050220710A1 (en) * | 2002-03-08 | 2005-10-06 | Seeley Randy S | Overfeeding methods for determining therapeutic strategies and/or targets for obesity therapeutics |
| US20070054278A1 (en) * | 2003-11-18 | 2007-03-08 | Applera Corporation | Polymorphisms in nucleic acid molecules encoding human enzyme proteins, methods of detection and uses thereof |
| US20090018031A1 (en) * | 2006-12-07 | 2009-01-15 | Switchgear Genomics | Transcriptional regulatory elements of biological pathways tools, and methods |
| WO2010024852A1 (en) * | 2008-08-28 | 2010-03-04 | Nestec S.A. | Gene expression profiles associated with lean phenotype and uses thereof |
| US20100113580A1 (en) * | 2008-10-16 | 2010-05-06 | Aronne Louis J | Combination therapies for the treatment of obesity |
| US20110263490A1 (en) | 2010-01-22 | 2011-10-27 | The General Hospital Corporation D/B/A Massachusetts General Hospital | Diagnostic Methods and Combination Therapies Involving MC4R |
| US20110270360A1 (en) | 2010-01-22 | 2011-11-03 | The General Hospital Corporation D/B/A Massachusetts General Hospital | Methods and devices for activating brown apidose tissue using electrical energy |
| US20120040342A1 (en) * | 2008-03-17 | 2012-02-16 | Geisinger Clinic | Genetic Indicators Of Weight Loss |
Family Cites Families (37)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US6582908B2 (en) | 1990-12-06 | 2003-06-24 | Affymetrix, Inc. | Oligonucleotides |
| GB9805918D0 (en) | 1998-03-19 | 1998-05-13 | Nycomed Amersham Plc | Sequencing by hybridisation |
| JP2003516111A (en) | 1999-02-22 | 2003-05-13 | バリアジェニックス インコーポレーテッド | Genetic sequence variants with utility in determining treatment for disease |
| US7194301B2 (en) | 2003-10-06 | 2007-03-20 | Transneuronic, Inc. | Method for screening and treating patients at risk of medical disorders |
| CA2574014A1 (en) | 2004-07-16 | 2006-01-26 | Oy Jurilab Ltd | Method for detecting the risk of and for treatment of type 2 diabetes |
| US20060062859A1 (en) | 2004-08-05 | 2006-03-23 | Kenneth Blum | Composition and method to optimize and customize nutritional supplement formulations by measuring genetic and metabolomic contributing factors to disease diagnosis, stratification, prognosis, metabolism, and therapeutic outcomes |
| US20070244375A1 (en) | 2004-09-30 | 2007-10-18 | Transeuronix, Inc. | Method for Screening and Treating Patients at Risk of Medical Disorders |
| US8095380B2 (en) | 2004-11-16 | 2012-01-10 | Health Dialog Services Corporation | Systems and methods for predicting healthcare related financial risk |
| FI20050011L (en) | 2005-01-05 | 2006-07-06 | Jurilab Ltd Oy | Method and test kit for detecting the risk of type 2 diabetes mellitus |
| US20060252050A1 (en) | 2005-05-06 | 2006-11-09 | Ordovas Jose M | Genetic marker for weight regulation |
| WO2007006858A2 (en) | 2005-07-12 | 2007-01-18 | Oy Jurilab Ltd | Method for treatment of cardiovascular and metabolic diseases and detecting the risk of the same |
| US20120296675A1 (en) | 2006-02-13 | 2012-11-22 | Silverman David G | Method and System for Assessing, Quantifying, Coding & Communicating a Patient's Health and Perioperative Risk |
| EP2021502A4 (en) | 2006-05-09 | 2010-08-25 | Mas Metabolic Analytical Servi | Novel genes and markers in type 2 diabetes and obesity |
| EP2136911A2 (en) | 2007-01-19 | 2009-12-30 | Biodot, Inc. | Systems and methods for high speed array printing and hybridization |
| EP1978107A1 (en) | 2007-04-03 | 2008-10-08 | Centre National De La Recherche Scientifique (Cnrs) | Fto gene polymorphisms associated to obesity and/or type II diabetes |
| US20090024144A1 (en) | 2007-07-18 | 2009-01-22 | Zeiner Mark S | Hybrid endoscopic/laparoscopic device for forming serosa to serosa plications in a gastric cavity |
| US8156166B2 (en) | 2007-08-06 | 2012-04-10 | Intuit Inc. | Method and apparatus for selecting a doctor based on an observed experience level |
| US8036912B2 (en) | 2008-04-30 | 2011-10-11 | Ethicon Endo-Surgery, Inc. | Interactive web based system in support of bariatric procedures |
| BRPI0912727A8 (en) | 2008-05-16 | 2017-10-03 | Interleulkin Genetics Inc | GENETIC MARKERS FOR WEIGHT CONTROL AND METHODS AND THEIR USE |
| US20100136561A1 (en) | 2008-05-16 | 2010-06-03 | Interleukin Genetics, Inc. | Genetic Markers for Weight Management and Methods of Use Thereof |
| US20100112570A1 (en) * | 2008-10-22 | 2010-05-06 | Interleukin Genetics, Inc. | Genetic Markers for Weight Management and Methods of Use Thereof |
| EP2192196A1 (en) | 2008-11-27 | 2010-06-02 | Helmholtz Zentrum München Deutsches Forschungszentrum für Gesundheit und Umwelt (GmbH) | Prediction of lipid-metabotype-related physiological susceptibilities |
| US20100209350A1 (en) | 2008-12-30 | 2010-08-19 | Andreas Pfuetzner | Biomarkers for Adipose Tissue Activity |
| EP2382475A2 (en) | 2009-01-07 | 2011-11-02 | IKFE GmbH | Biomarkers for appetite regulation |
| WO2011006070A2 (en) * | 2009-07-09 | 2011-01-13 | Interleukin Genetics, Inc. | Genetic association of polymorphisms in perilipin (plin) gene with resistance to weight loss |
| US20110124121A1 (en) | 2009-10-15 | 2011-05-26 | Allergan, Inc. | Methods for predicting weight loss success |
| FI20096188A0 (en) | 2009-11-16 | 2009-11-16 | Mas Metabolic Analytical Servi | Nutrigenetic biomarkers for obesity and type 2 diabetes |
| FI20100211A0 (en) | 2010-05-19 | 2010-05-19 | Mas Metabolic Analytical Servi | Method for genetic diagnosis of susceptibility to atherosclerosis |
| US8990135B2 (en) | 2010-06-15 | 2015-03-24 | The Regents Of The University Of Michigan | Personalized health risk assessment for critical care |
| CA2819378A1 (en) * | 2010-12-02 | 2012-06-07 | Katholieke Universiteit Leuven, K.U.Leuven R&D | Irak-related interventions and diagnosis |
| US9610429B2 (en) | 2010-12-29 | 2017-04-04 | Ethicon Endo-Surgery, Inc. | Methods and devices for activating brown adipose tissue with targeted substance delivery |
| US9381219B2 (en) | 2010-12-29 | 2016-07-05 | Ethicon Endo-Surgery, Inc. | Brown adipocyte modification |
| US10441808B2 (en) | 2010-12-29 | 2019-10-15 | Ethicon Endo-Surgery, Inc. | Methods and devices for activating brown adipose tissue with light |
| WO2013115756A2 (en) | 2010-12-29 | 2013-08-08 | Ethicon Endo-Surgery, Inc. | Methods and devices for activating brown adipose tissue with cooling |
| US10242756B2 (en) | 2012-09-21 | 2019-03-26 | Ethicon Endo-Surgery, Inc. | Systems and methods for predicting metabolic and bariatric surgery outcomes |
| US9250172B2 (en) | 2012-09-21 | 2016-02-02 | Ethicon Endo-Surgery, Inc. | Systems and methods for predicting metabolic and bariatric surgery outcomes |
| US20140087999A1 (en) | 2012-09-21 | 2014-03-27 | The General Hospital Corporation D/B/A Massachusetts General Hospital | Clinical predictors of weight loss |
-
2013
- 2013-09-20 EP EP13839109.9A patent/EP2898101A4/en not_active Withdrawn
- 2013-09-20 WO PCT/US2013/060901 patent/WO2014047432A1/en not_active Ceased
-
2017
- 2017-10-31 US US15/799,271 patent/US11236392B2/en not_active Expired - Fee Related
-
2022
- 2022-01-21 US US17/581,335 patent/US20230096225A1/en not_active Abandoned
Patent Citations (8)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20050220710A1 (en) * | 2002-03-08 | 2005-10-06 | Seeley Randy S | Overfeeding methods for determining therapeutic strategies and/or targets for obesity therapeutics |
| US20070054278A1 (en) * | 2003-11-18 | 2007-03-08 | Applera Corporation | Polymorphisms in nucleic acid molecules encoding human enzyme proteins, methods of detection and uses thereof |
| US20090018031A1 (en) * | 2006-12-07 | 2009-01-15 | Switchgear Genomics | Transcriptional regulatory elements of biological pathways tools, and methods |
| US20120040342A1 (en) * | 2008-03-17 | 2012-02-16 | Geisinger Clinic | Genetic Indicators Of Weight Loss |
| WO2010024852A1 (en) * | 2008-08-28 | 2010-03-04 | Nestec S.A. | Gene expression profiles associated with lean phenotype and uses thereof |
| US20100113580A1 (en) * | 2008-10-16 | 2010-05-06 | Aronne Louis J | Combination therapies for the treatment of obesity |
| US20110263490A1 (en) | 2010-01-22 | 2011-10-27 | The General Hospital Corporation D/B/A Massachusetts General Hospital | Diagnostic Methods and Combination Therapies Involving MC4R |
| US20110270360A1 (en) | 2010-01-22 | 2011-11-03 | The General Hospital Corporation D/B/A Massachusetts General Hospital | Methods and devices for activating brown apidose tissue using electrical energy |
Non-Patent Citations (22)
| Title |
|---|
| CHAMBERS ET AL., GASTROENTEROLOGY, vol. 141, no. 3, 2011, pages 950 - 958 |
| DATABASE GENBANK [online] 29 June 2012 (2012-06-29), "Mus musculus adiponectin receptor 1 (Adiporl mRNA", XP055244294, accession no. NCBI Database accession no. NM_028320 * |
| DRAZEN, D. L.; WOODS, S. C., CURR. OPIN. CLIN. NUTR. METAB. CARE, vol. 6, 2003, pages 621 - 629 |
| GOMEZ-AMBROSI ET AL.: "Gene expression profile of omental adipose tissue in human-Obesity.", FASEB J, vol. 18, no. 1, January 2004 (2004-01-01), pages 215 - 217, XP055244389 * |
| HATOUM ET AL.: "Weight Loss after Gastric Bypass Is Associated with a Variant at 15q26.", AM J HUM GENET, vol. 92, no. 5, 2 May 2013 (2013-05-02), pages 827 - 34, XP055244302 * |
| HATOUM, I. J ET AL.: "Heritability Of The Weight Loss Response To Gastric Bypass Surgery", J CLIN ENDOCRINOL METAB, vol. 96, 2011, pages E1630 - 3 |
| HATOUM, I. J.; STEIN, H. K.; MERRIFIELD, B. F.; KAPLAN, L. M.: "Capacity For Physical Activity Predicts Weight Loss After Roux-En-Y Gastric Bypass", OBESITY (SILVER SPRING), vol. 17, 2009, pages 92 - 99 |
| HATOUM, I.J. ET AL., J CLIN ENDOCRINOL METAB, vol. 97, 2012, pages E1023 - E1031 |
| J.R. ROBINSON: "Sustained and Controlled Release Drug Delivery Systems", 1978, MARCEL DEKKER, INC. |
| LI, Y.; WILLER, C. J.; DING, J.; SCHEET, P.; ABECASIS, G. R., GENET. EPIDEMIOL., vol. 34, 2010, pages 816 - 834 |
| MCAULEY, E. Z ET AL.: "Identification Of Sialyltransferase 8B As A Generalized Susceptibility Gene For Psychotic And Mood Disorders On Chromosome 15q25-26", PLOS ONE, vol. 7, 2012, pages E38172 |
| MCMINN, J. E.; BASKIN, D. G.; SCHWARTZ, M. W., OBES. REV, vol. 1, 2000, pages 37 - 46 |
| MOSCHEN ET AL.: "Effects of weight loss induced by bariatric surgery on hepatic adipocytokine expression.", J HEPATOL, vol. 51, no. 4, October 2009 (2009-10-01), pages 765 - 77, XP026686859 * |
| OCHNER, C. N ET AL.: "Selective Reduction In Neural Responses To High Calorie Foods Following Gastric Bypass Surgery", ANN. SURG., vol. 253, 2011, pages 502 - 507 |
| PETERLI ET AL., ANN SURG, vol. 250, no. 2, 2009, pages 234 - 41 |
| PRICE, A. L. ET AL., NAT. GENET., vol. 38, 2006, pages 904 - 909 |
| PURCELL, S. ET AL.: "PLINK: a tool set for whole-genome association and population-based linkage analyses", AM. J. HUM. GENET., vol. 81, 2007, pages 559 - 575 |
| RANKINEN ET AL.: "The Human Obesity Gene Map: The 2005 Update.", OBESITY, vol. 14, no. 4, April 2006 (2006-04-01), pages 529 - 644, XP055244370 * |
| See also references of EP2898101A4 |
| SHIN, A. C.; ZHENG, H.; PISTELL, P. J.; BERTHOUD, H.-R.: "Roux-En-Y Gastric Bypass Surgery Changes Food Reward In Rats", INT J OBES (LOND, vol. 35, 2011, pages 642 - 651 |
| SPELIOTES, E.K. ET AL., NAT GENET, vol. 42, 2010, pages 937 - 48 |
| STILL ET AL.: "High Allelic Burden of Four Obesity SNPs Is Associated With Poorer Weight Loss Outcomes Following Gastric Bypass", SURGERY., vol. 19, no. 8, August 2011 (2011-08-01), pages 1676 - 83, XP055244384 * |
Also Published As
| Publication number | Publication date |
|---|---|
| US20180066315A1 (en) | 2018-03-08 |
| US11236392B2 (en) | 2022-02-01 |
| EP2898101A4 (en) | 2016-08-03 |
| EP2898101A1 (en) | 2015-07-29 |
| US20230096225A1 (en) | 2023-03-30 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US20140087999A1 (en) | Clinical predictors of weight loss | |
| US20230096225A1 (en) | Clinical predictors of weight loss | |
| KR102622309B1 (en) | Detection of chromosomal interactions | |
| Yuan et al. | Plasma extracellular RNA profiles in healthy and cancer patients | |
| Jeffries | Osteoarthritis year in review 2018: genetics and epigenetics | |
| Powell et al. | Endometriosis risk alleles at 1p36. 12 act through inverse regulation of CDC42 and LINC00339 | |
| Jobard et al. | Identification of mutations in a new gene encoding a FERM family protein with a pleckstrin homology domain in Kindler syndrome | |
| Callahan et al. | Axis inhibition protein 2 (AXIN2) polymorphisms and tooth agenesis | |
| Hatoum et al. | Weight loss after gastric bypass is associated with a variant at 15q26. 1 | |
| Knevel et al. | Identification of a genetic variant for joint damage progression in autoantibody-positive rheumatoid arthritis | |
| Benson et al. | Natural human genetic variation determines basal and inducible expression of PM20D1, an obesity-associated gene | |
| EP1978107A1 (en) | Fto gene polymorphisms associated to obesity and/or type II diabetes | |
| WO2009117415A2 (en) | Genetic indicators of weight loss | |
| CN104508149A (en) | Prediction of treatment response to JAK/STAT inhibitor | |
| TW201726140A (en) | Novel biomarkers and methods of treating cancer | |
| Marko et al. | The molecular biology of WHO grade I astrocytomas | |
| CN105659085B (en) | Predict subject to the gene expression mark and its application method of the reaction of multi-kinase inhibitor | |
| Esfandi et al. | Expression assessment of a panel of long non-coding RNAs in gastric malignancy | |
| Ünal et al. | Polymorphisms in transcription factor binding sites and enhancer regions and pancreatic ductal adenocarcinoma risk | |
| Di Meglio et al. | Immunopathogenesis of psoriasis | |
| Singh et al. | Annotation of androgen dependence to human prostate cancer-associated genes by microarray analysis of mouse prostate | |
| Poorhosseini et al. | New gene profiling in determination of breast cancer recurrence and prognosis in Iranian women | |
| Pu et al. | Exome-wide association analysis suggests LRP2BP as a susceptibility gene for endothelial injury in systemic sclerosis in the Han Chinese population | |
| Müller et al. | SNP dependent modulation of circulating miRNAs from the miR25/93/106 cluster in patients undergoing weight loss | |
| Kim et al. | Polymorphisms of ADIPOR1 and ADIPOR2 are associated with phenotypes of type 2 diabetes in Koreans |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 13839109 Country of ref document: EP Kind code of ref document: A1 |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2013839109 Country of ref document: EP |