WO2017126549A1 - 心疾患の治療のための移植材料 - Google Patents
心疾患の治療のための移植材料 Download PDFInfo
- Publication number
- WO2017126549A1 WO2017126549A1 PCT/JP2017/001538 JP2017001538W WO2017126549A1 WO 2017126549 A1 WO2017126549 A1 WO 2017126549A1 JP 2017001538 W JP2017001538 W JP 2017001538W WO 2017126549 A1 WO2017126549 A1 WO 2017126549A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- cells
- cell
- group
- adrcs
- heart disease
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Images





































Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/38—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells
- A61L27/3804—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells characterised by specific cells or progenitors thereof, e.g. fibroblasts, connective tissue cells, kidney cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K35/00—Medicinal preparations containing materials or reaction products thereof with undetermined constitution
- A61K35/12—Materials from mammals; Compositions comprising non-specified tissues or cells; Compositions comprising non-embryonic stem cells; Genetically modified cells
- A61K35/28—Bone marrow; Haematopoietic stem cells; Mesenchymal stem cells of any origin, e.g. adipose-derived stem cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K35/00—Medicinal preparations containing materials or reaction products thereof with undetermined constitution
- A61K35/12—Materials from mammals; Compositions comprising non-specified tissues or cells; Compositions comprising non-embryonic stem cells; Genetically modified cells
- A61K35/35—Fat tissue; Adipocytes; Stromal cells; Connective tissues
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K35/00—Medicinal preparations containing materials or reaction products thereof with undetermined constitution
- A61K35/12—Materials from mammals; Compositions comprising non-specified tissues or cells; Compositions comprising non-embryonic stem cells; Genetically modified cells
- A61K35/44—Vessels; Vascular smooth muscle cells; Endothelial cells; Endothelial progenitor cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K35/00—Medicinal preparations containing materials or reaction products thereof with undetermined constitution
- A61K35/12—Materials from mammals; Compositions comprising non-specified tissues or cells; Compositions comprising non-embryonic stem cells; Genetically modified cells
- A61K35/48—Reproductive organs
- A61K35/51—Umbilical cord; Umbilical cord blood; Umbilical stem cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K35/00—Medicinal preparations containing materials or reaction products thereof with undetermined constitution
- A61K35/12—Materials from mammals; Compositions comprising non-specified tissues or cells; Compositions comprising non-embryonic stem cells; Genetically modified cells
- A61K35/48—Reproductive organs
- A61K35/54—Ovaries; Ova; Ovules; Embryos; Foetal cells; Germ cells
- A61K35/545—Embryonic stem cells; Pluripotent stem cells; Induced pluripotent stem cells; Uncharacterised stem cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L24/00—Surgical adhesives or cements; Adhesives for colostomy devices
- A61L24/04—Surgical adhesives or cements; Adhesives for colostomy devices containing macromolecular materials
- A61L24/10—Polypeptides; Proteins
- A61L24/106—Fibrin; Fibrinogen
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P9/00—Drugs for disorders of the cardiovascular system
Definitions
- the present invention relates to a transplant material for the treatment of a heart disease containing a cell cluster obtained by adhering separated cells with an adhesive, and a method for treating a heart disease using the transplant material. .
- Non-patent Document 3 Myocardial infarction is irreversible damage to cardiomyocytes.
- Ischemic heart disease accounts for 50% of all cardiovascular causes of death and is the leading cause of congestive heart failure.
- the prognosis is very poor and the 1-year mortality rate is close to 20% if treatment does not result in remission (Non-patent Document 2).
- Many of the treatments currently available to clinicians can eliminate the cause of this acute myocardial infarction, but the time from the onset of onset to reperfusion determines the degree of irreversible myocardial damage (Non-Patent Document 3) .
- Cardiomyoplasty has been proposed as a surgical method to improve left ventricular (LV) function in patients with congestive heart failure, but the effect on cardiac function and patient outcome is not satisfactory (non- Patent documents 4 to 7). None of the drugs or treatments used clinically are effective in replacing myocardial scars with functional contractile tissue, and there is a need for new therapies to regenerate normal cardiomyocytes.
- Non-Patent Documents 8 to 11 transplantation of bioengineered heart grafts using biodegradable scaffolds has shown minimal benefit in improving cardiac function due to little adherence to the myocardium (Non-Patent Documents 12, 13). ). On the other hand, whole heart transplantation is not the first-line treatment for heart failure due to donor shortage.
- Adiponectin known as a cytokine secreted from adipocytes, may protect myocardium after injury through anti-apoptosis, anti-inflammation, angiogenesis, anti-fibrosis, and anti-myocardial hypertrophy, and suppress the deterioration of cardiac function It has also been reported (Non-Patent Documents 16 and 17). Furthermore, as a means for administering adiponectin to a target heart tissue for a long period of time, research on adipocyte transplantation as a drug delivery system (DDS) has been made.
- DDS drug delivery system
- transplanted cell sheets require a lot of time and labor to produce and have problems in use in clinical settings.
- the present invention has been made in view of such circumstances, and an object of the present invention is a transplant material having an excellent effect in the treatment of heart disease, which can be easily prepared in a short time. Is to provide. A further object of the present invention is to provide a method for treating heart disease using the transplant material.
- the present inventor found that cell aggregates obtained by adhering regenerated cells separated from living adipose tissue as they were without culturing were transplanted into the heart. It has been found that it secretes adiponectin and has an excellent therapeutic effect on heart disease. In the production of this cell agglomeration, a cell agglomeration could be easily produced by using fibrinogen as a cell adhesive material. Moreover, in the production of cell clusters, the therapeutic effect could be further enhanced by using adipose tissue-derived mesenchymal progenitor cells contacted with a PPAR ⁇ agonist.
- the effect of treating heart disease is obtained by using a cell sheet containing mesenchymal stem cells derived from adipose tissue instead of mature adipocytes.
- the collected stem cells are generally cultured for a few days in a predetermined medium, and after being subcultured for several passages, a cell sheet is prepared (paragraphs 0013 to 0014).
- the mesenchymal stem cells in this cell sheet have differentiated into myocardium, vascular endothelium, and vascular smooth muscle cells after transplantation into the heart. (Paragraphs 0017-0018).
- the present invention provides a transplant material that can be easily prepared in a short time and has an excellent therapeutic effect on heart disease, and a method for treating heart disease using the transplant material. More specifically, the following invention is provided.
- a transplant material for the treatment of heart disease including cell clumps obtained by adhering separated cells with an adhesive.
- the separated cells consist of adipose tissue-derived regenerative cells, bone marrow-derived regenerative cells, umbilical cord-derived regenerative cells, smooth muscle-derived regenerative cells, pluripotent stem cells and regenerative cells derived therefrom, vascular endothelial cells, and monocytes
- a method for treating a heart disease comprising covering the heart surface of a subject suffering from a heart disease with the transplant material according to any one of [1] to [5].
- the separated cells can be directly processed into a cell cluster and transplanted. Moreover, processing into a cell clump can be easily performed using fibrinogen or the like. Therefore, time, labor, and cost can be greatly reduced as compared with conventional transplantation treatment methods that utilize cell sheets.
- the method of the present invention is higher in safety than conventional transplantation treatment methods in which adipose tissue-derived mesenchymal progenitor cells are injected into the coronary artery or myocardium, and in combination with the secretion of adiponectin, improves the cardiac function. Is also excellent.
- FIG. 1 is a diagram showing the results of histological examination of cell clusters of adipose tissue-derived regenerative cells (ADRCs) (hereinafter sometimes simply referred to as “ADRCs cell clusters”).
- FIG. 1A is a micrograph (in vitro evaluation) of an ADRCs cell cluster after culture.
- FIG. 1B is a graph (in vitro evaluation) showing the results of measuring adiponectin (APN), VEGF, HGF, and IL-6 in the culture supernatant of ADRCs cell agglomerates by the enzyme immunoassay (ELISA method).
- FIG. 1C is a photomicrograph (in vitro evaluation) of ADRCs cell clusters after culture.
- FIG. 2A is a photomicrograph (in vivo evaluation) of the isolated cardiac tissue on day 5 after transplantation of ADRCs cell agglomeration in a myocardial infarction model rat.
- FIG. 2B is a micrograph (in vivo evaluation) showing the expression of new blood vessels in the epicardium side and between the myocardial infarction and the cell cluster.
- FIG. 3 is a diagram showing the results of examination of the effect of ADRCs cell agglomeration treatment on cardiac function in myocardial infarction model rats by cardiac ultrasonography.
- FIG. 3A is a graph of left ventricular ejection fraction (EF).
- FIG. EF left ventricular ejection fraction
- FIG. 3B is a graph of left ventricular end systolic diameter (LVESd).
- FIG. 3C is a graph of left ventricular end diastolic diameter (LVEDd).
- FIG. 3D is a graph of life prognosis.
- FIG. 4 is a diagram showing the results of cardiac ultrasound study on the effects of ADRCs cell agglomeration transplantation, ADRCs intramyocardial injection, or ADRCs intracoronary administration on cardiac function in chronic myocardial infarction model rats.
- FIG. 4A is a graph of left ventricular ejection fraction (EF).
- FIG. 4B is a graph of left ventricular end systolic diameter (LVESd).
- FIG. 4C is a graph of left ventricular end diastolic diameter (LVEDd).
- FIG. 5 is a view showing the results of examining the influence of ADRCs cell agglomeration treatment on myocardial tissue in myocardial infarction model rats.
- FIG. 5A is a photomicrograph showing a group S Picro-Sirius red stained macro image.
- FIG. 5B is a photomicrograph showing a Picro-Sirius red stained macro image of Group A.
- FIG. 5C is a photomicrograph showing a Picro-Sirius red stained macro image of the AP group.
- FIG. 5D is a graph showing the results of measurement of end diastolic left ventricular wall thickness (LVAWD) in S group, A group, and AP group.
- LVAWD end diastolic left ventricular wall thickness
- FIG. 5E is a graph showing the results of measuring the fibrosis rate in the left ventricular cross-sectional area of the S group, the A group, the AP group, the ic group, and the im group.
- FIG. 5F is a photomicrograph showing a von Willebrand factor stained image in the infarct-normal boundary region of group S.
- FIG. 5G is a photomicrograph showing a von Willebrand factor stained image in the infarct-normal region boundary region of Group A.
- FIG. 5H is a micrograph showing a von Willebrand factor stained image in the infarct-normal boundary region of the AP group.
- FIG. 5I is a graph showing the results of measuring capillary density in the infarct-normal boundary region of S group, A group, AP group, ic group and im group.
- FIG. 6 is a diagram showing the results of examining the effect on myocardial tissue 8 weeks after ADRCs cell agglomeration transplantation treatment for chronic myocardial infarction model rats.
- FIG. 6A is a photomicrograph showing a macro image of group S hematoxylin and eosin staining.
- FIG. 6B is a micrograph showing a macro image of group A hematoxylin and eosin staining.
- FIG. 6C is a micrograph showing a macro image of the AP group stained with hematoxylin and eosin.
- FIG. 6D is a representative histological photograph showing the result of Periodic acid-Shiff (PAS) staining of the infarct-normal part boundary region of Group S.
- FIG. 6E is a representative tissue photograph showing the result of Periodic acid-Shiff (PAS) staining of the infarct-normal boundary region of Group A.
- FIG. 6F is a representative histological photograph showing the result of Periodic acid-Shiff (PAS) staining of the infarct-normal part boundary region of the AP group.
- FIG. 6G is a graph showing the results of quantifying the myocardial cell diameter in the myocardial infarction-normal region boundary region of each experimental group.
- FIG. 7 is a diagram showing the results of examining the anti-inflammatory effect by ADRCs cell conglomerate transplantation.
- FIG. 7A is a graph showing the results of quantifying the amount of transcription of Adiponectin (APN) in the infarct region and the infarct-normal region boundary region.
- FIG. 7B is a graph showing the results of quantifying the amount of transcription of Adiponectin receptor 1 (Adipo-R1) in the infarct region and the infarct-normal region boundary region.
- FIG. 7C is a graph showing the results of quantifying the amount of transcription of Adiponectin receptor 2 (Adipo-R2) in the infarct region and the infarct-normal region boundary region.
- Adiponectin receptor 1 Adiponectin receptor 1
- Adipo-R2 Adiponectin receptor 2
- FIG. 7D is a graph showing the results of quantifying the amount of T-cadherin transcription in the infarct region and the infarct-normal region boundary region.
- FIG. 7E is a graph showing the results of quantifying the transcription amount of vascular endothelial growth factor (VEGF) in the infarct region and the infarct-normal region boundary region.
- FIG. 7F is a graph showing the results of quantifying the amount of transcription of Tumor necrosis factor alpha (TNF- ⁇ ) in the infarct region and the infarct-normal region boundary region.
- FIG. 8 is a diagram showing the ability of ADRCs to produce adiponectin continuously and engraftment in the myocardium.
- FIG. 8 is a diagram showing the ability of ADRCs to produce adiponectin continuously and engraftment in the myocardium.
- FIG. 8A is a histological photograph one week after transplanting the GFP transgenic LEW / Sea rat-derived ADRCs cell cluster into the left ventricle of the LEW / Sea rat.
- the upper region in the figure is the ADRCs cell cluster, and the lower part Is the heart
- FIG. 8B is a photomicrograph showing the results of transplanting GFP transgenic LEW / Sea rat-derived ADRCs cell clusters into the left ventricle of LEW / Sea rats and immunostaining the tissue 3 weeks later with adiponectin. The lightly colored area is adiponectin.
- FIG. 8C is a photomicrograph showing the result of intraperitoneal injection of GFP transgenic LEW / Sea rat-derived ADRCs.
- FIG. 8D is a photomicrograph showing the results of intracoronary administration of GFP transgenic LEW / Sea rat-derived ADRCs.
- the present invention provides a transplant material for the treatment of heart disease, including cell clumps obtained by adhering separated cells with an adhesive.
- the isolated cells are not particularly limited as long as they have a therapeutic effect on heart disease.
- regenerated cells derived from adipose tissue eg, subcutaneous adipose tissue, omentum, subepicardial fat
- regenerated cells derived from bone marrow examples include umbilical cord-derived regenerative cells, smooth muscle (eg, perivascular smooth muscle) -derived regenerative cells, pluripotent stem cells (eg, iPS cells, ES cells, Muse cells) and regenerative cells derived therefrom.
- differentiated cells such as vascular endothelial cells and monocytes.
- the “regenerative cell” in the present invention means a cell having an ability to restore the structure and function of an applied organ or tissue.
- the regenerative cells are a group of cells including mesenchymal stem cells and mesenchymal progenitor cells.
- the “mesenchymal stem cell” means a stem cell capable of differentiating into cells belonging to the mesenchymal system such as osteoblasts, adipocytes, muscle cells, chondrocytes, and the “mesenchymal progenitor cells” It means cells in the process of differentiation from mesenchymal stem cells to cells belonging to the mesenchymal system.
- the “stem cell” means a cell having self-renewal ability and pluripotency. Whether the separated regenerative cells are mesenchymal stem cells or mesenchymal progenitor cells can be evaluated by a predetermined cell surface marker (Lin K et al., Cytotherapy 2008; 10 (4): 417-426).
- adipose tissue-derived regenerative cells are particularly preferably used.
- Adipose tissue is a connective tissue mainly composed of adipocytes, but is not particularly limited as adipose tissue for separating regenerative cells, and includes subcutaneous adipose tissue, omentum, subepicardial fat and the like. Can be mentioned. Collection of adipose tissue from a living body can be performed, for example, by suction from a small incision or excision by surgery.
- a preferred embodiment of the cell clump obtained by adhering cells is a combination of mesenchymal progenitor cells and mesenchymal stem cells, at least 1% or more, preferably 5% or more (for example, 10% or more, 20% or more, 30% or more, 40% or more, 50% or more).
- mesenchymal progenitor cells for example, 5% or more (for example, 10% or more, 20% or more, 30% or more, 40% or more, 50% or more).
- mesenchymal progenitor cells for example, 10% or more, 20% or more, 30% or more, 40% or more, 50% or more.
- Separation of cells from the tissue can be performed by, for example, subdividing the tissue, treating with collagenase, filtering with a filter, and then centrifuging. Centrifugation for separating regenerative cells can be performed, for example, under conditions of 500 to 800 G and 5 to 10 minutes.
- the separated cells are adhered to form a cell clump.
- Fibrinogen can be used conveniently. Fibrinogen becomes a paste-like fibrin polymer when mixed with thrombin, thereby acquiring the ability to adhere cells together. Therefore, for example, as shown in this Example, cells can be easily adhered to each other by mixing a cell suspension added with fibrinogen and a solution containing thrombin. If the temperature is kept after the mixing, the adhesion can be accelerated.
- cells for forming a cell clump need not be cultured, and the separated regenerative cells can be immediately processed into a cell clump and used for transplantation into the heart. Therefore, the process from collection to preparation of a cell clump can be performed in a very short time.
- cells are adhered to each other by culturing (adhesive is used for the purpose of reinforcing the cell sheet). In general, it takes a period of several days to several weeks until the preparation of a cell.
- the time from collection of a biological tissue to the preparation of a cell agglomeration is only a few hours. It can be shortened.
- adipose tissue-derived regenerative cells in which a PPAR ⁇ agonist is allowed to act.
- the secretion of adiponectin from the cell cluster can be further enhanced after transplantation into the heart.
- the PPAR ⁇ agonist include, but are not limited to, thiazolidine drugs such as pioglitazone.
- substances that act on adipose tissue-derived cells include, for example, substances that promote differentiation into adipocytes such as insulin and steroids, angiotensin receptor antagonists (ARB) and angiotensin converting enzyme inhibitors (ACEi) And cytokines such as VEGF and HGF.
- the cell clumps When used for heart disease transplantation treatment, the cell clumps can be appropriately adjusted in size and thickness depending on the site to be transplanted, etc., but usually a disk shape or a side with a diameter of 5 mm to 5 cm. It is preferably a square of 5 mm to 5 cm, and preferably has a thickness of 0.5 to 2 mm so as to obtain sufficient strength.
- a suspension having a cell concentration of 2 ⁇ 10 5 to 2 ⁇ 10 7 cells / ml can be used.
- the transplant material of the present invention may further contain other elements useful for treating heart diseases as long as the cell aggregate is included.
- other elements include, but are not limited to, cell clumps and cell sheets made of heterogeneous cells, extracellular matrix, and adhesion factor protein.
- Examples of the “heart disease” to be treated with the transplant material of the present invention include, for example, heart failure, ischemic heart disease, myocardial infarction, cardiomyopathy, myocarditis, hypertrophic cardiomyopathy, dilated phase hypertrophic cardiomyopathy, and Examples include, but are not limited to, diseases with disorders or disorders selected from the group consisting of dilated cardiomyopathy.
- the present invention also provides a method for treating a heart disease, characterized in that the transplant material described above covers the heart surface of a subject suffering from a heart disease.
- the treatment in the present invention can be applied to humans and non-human subjects.
- the organism to be applied is not particularly limited as long as it has a heart as a therapeutic target, and examples thereof include humans, mammals other than humans, birds, reptiles, amphibians, and fish.
- mammals other than humans include, but are not limited to, primates such as chimpanzees and monkeys, and domestic animals and pets such as cows, pigs, horses, chickens, cats and dogs.
- the cells from which the transplant material of the present invention is derived may be used, but from the viewpoint of suppression of rejection, etc., preferably from the same species, particularly preferably autologous. Cells are used. Therefore, particularly preferably, the transplant material of the present invention is transplanted to a subject from which cells have been collected.
- the site where the transplant material of the present invention is transplanted is preferably the heart surface.
- the heart disease can be treated by coating the heart surface with the transplant material of the present invention.
- the transplant material is affixed to a lesion (for example, myocardial infarction focus) and is surgically fixed to the epicardium with a proline needle, or fixed to the heart surface by fibrin spray. That's fine.
- the transplant material is preferably disposed on the surface of the heart so as to sufficiently cover the boundary between the lesion site (for example, the myocardial infarction site) and the surrounding normal site.
- the heart to be transplanted When transplanting, the heart to be transplanted is preliminarily treated as necessary. For example, in the case of the first operation, it is preferable to transplant the blood surface after sufficiently wiping the blood and water on the heart surface. In the case of reoperation, the scar surface tissue on the heart surface should be removed as soon as possible. Is preferred.
- the treatment with the transplant material of the present invention may be combined with other treatments.
- chronic myocardial infarction it may be used in combination with coronary artery bypass surgery, percutaneous coronary angioplasty, or left ventricular plastic surgery.
- acute myocardial infarction coronary artery bypass surgery or percutaneous coronary angioplasty may be used in combination.
- valve replacement and pediatric heart surgery it can be used together with valve replacement and pediatric heart surgery.
- Adipose tissue-derived regenerative cells Adipose derived regenerative cells
- Adipose tissue was collected from both inguinal regions of 9-week-old female LEW / Sea rats. The adipose tissue was minced with a scissors, suspended in 0.1% type II collagenase solution, and shaken in a 37 ° C. hot tub for 1 hour. The mixture was filtered through 100 ⁇ m and 70 ⁇ m mesh filters, and centrifuged at 1800 rpm for 10 minutes.
- a suspension obtained by suspending the precipitate in a culture medium (D-MEM containing 10% fetal bovine serum and antibiotics) was used as an adipose-derived regenerative cell group (ADRCs). These include adipose tissue-derived mesenchymal stem cells and progenitor cells.
- ADRCs cell agglomerates Immediately after ADRCs extraction from adipose tissue, cell agglomerates containing 5 ⁇ 10 6 ADRCs per piece were prepared. Add 60 ⁇ l of fibrinogen to 140 ⁇ l of ADRCs cell suspension to make solution A, and add 30 ml of thrombin to 170 ⁇ l of culture solution (10% fetal bovine serum, antibiotic-containing D-MEM) and mix well. B solution. First, add A solution onto the culture dish, add B solution to the shape, and shape it into a shape suitable for transplantation, and then incubate the cells in a humid environment at 37 ° C for 5-10 minutes in a 5% carbon dioxide atmosphere. ADRCs cell clumps were prepared by bonding them together. Immediately after preparation of the ADRCs cell cluster, it was transplanted to the infarct site.
- ADRCs cell clumps Frozen sections of ADRCs cell clumps were prepared and fixed with 4% paraformaldehyde, followed by oil red O staining and adiponectin immunostaining.
- a myocardial infarction model was prepared by ligation of the left anterior descending coronary artery using 7-week-old female LEW / Sea rats. After general anesthesia under inhalation anesthesia of isoflurane (1.5% isoflurane, ventilation volume 4 ml, 110 cycles / min), left thoracotomy was performed to expose the heart. A site 2 to 3 mm from the origin of the left coronary artery was ligated with 7-0 proline thread. Two weeks after the coronary artery ligation, the ADRCs cell cluster was placed on a precurved tweezers, slid to the infarcted region of the left ventricular anterior wall, and allowed to stand. For the untreated group, stabilized fibrin without ADRCs was transplanted with similar treatment.
- LVEDd Left ventricular end diastolic diameter
- LVESd end systolic diameter
- Left ventricular end-diastolic volume (LVEDV) ⁇ 7.0 / (2.4 + LVEDd) ⁇ xLVEDd 3
- Left ventricular end systolic volume (LVESV) ⁇ 7.0 / (2.4 + LVEDs) ⁇ xLVEDs 3 (8) Histological evaluation On the 14th and 56th days after the operation, the heart was removed under pulsation after obtaining a suppressed state by deep inhalation anesthesia with isoflurane.
- the left ventricle was sliced in the minor axis direction, embedded in a compound, and then frozen in liquid nitrogen to prepare a tissue section. Hematoxylin and eosin staining, Picro-Sirius red staining, Masson trichrome staining, oil red O staining, adiponectin immunostaining, SMA immunostaining, and von Willebrand factor immunostaining were performed. Fibrosis rate was determined by image analysis of Picro-Sirius red staining. The viable cell size at the peri-infarct border region was determined by measuring the short axis of one visual field (400 times) stained with hematoxylin and eosin, and calculating the average value of 10 visual fields per specimen. In addition, the number of capillaries per visual field (400 times) of von Willebrand factor immunostaining was measured, and the average value of 5 visual fields per specimen was calculated.
- VEGF vascular endothelial growth factor
- APN adiponectin
- Adipo-R1 adiponectin receptor-1
- Adipo-R2 adiponectin receptor-2
- CDH-13 T-cadherin
- ADRCs cell aggregates The ability of ADRCs cell aggregates to secrete cytokines and differentiate into adipocytes ADRCs cell aggregates (Fig. 1A) and pioglitazone (PGZ) -containing ADRCs cell aggregates were prepared and incubated at 37 ° C in a 5% carbon dioxide atmosphere. The cells were cultured in a humid environment for 144 hours, and the cytokine secretion ability was examined. Adiponectin (APN), VEGF, HGF, and IL-6 secretion levels of ADRCs cell aggregates and PGZ-containing cell aggregates increased with time in the culture medium.
- Adiponectin Adiponectin (APN)
- VEGF VEGF
- HGF vascular endothelial growth factor
- IL-6 secretion levels of ADRCs cell aggregates and PGZ-containing cell aggregates increased with time in the culture medium.
- the adiponectin concentrations after 144 hours of culture were 21.7 ⁇ 0.9 ng / 5x10 6 cells / day and 51 ⁇ 3.9 ng / 5x10 6 cells / day, respectively.
- the concentration was significantly higher than that of the lumps (FIG. 1B).
- the group in which ADRCs cell agglomerates were transplanted to the left ventricular anterior wall Group A
- the group in which ADRCs cell agglomerates containing pioglitazone (PGZ) were transplanted to the anterior wall of the left ventricle AP group
- no cell agglomeration transplantation The treatment group (S group), the ADRCs cell direct intramyocardial transplantation group around the left ventricular infarct (im group), and the transleft ventricular intracoronary artery transplantation group (ic group).
- the EF values of the A group and the AP group were significantly larger than those of the S group, and improvement in the left ventricular contractility was recognized. Furthermore, the AP group showed a significant improvement in EF over the A group at 8 weeks after transplantation (FIG. 3A).
- LVEDd values in group A and AP group were not significantly different from those in group S (Fig. 3C), and LVESd values were small (Fig. 3B). Admitted.
- ADRCs cells are different from the transplantation of ADRCs cell agglomeration, with direct intramyocardial transplantation group (im group) and transleft ventricular intracoronary transplantation group (ic group) around the left ventricular infarct
- im group direct intramyocardial transplantation group
- ic group transleft ventricular intracoronary transplantation group
- the EF values of the A group and the AP group were significantly larger than those of the S group, the im group, and the ic group (FIG. 4A)
- the LVESd values were compared with those of the S group, the im group, and the ip group.
- Small FIG. 4B
- no significant difference was observed in LVEDd (FIG. 4C). From the above results, it was confirmed that transplantation of ADRCs cell agglomerates had a therapeutic effect superior to the method of directly administering ADRCs cells into the myocardium or coronary artery in the treatment of myocardial infarction.
- FIG. 7 shows the examination results on the myocardial protective / anti-inflammatory effect in myocardial tissue 56 days after ADRCs cell agglomeration transplantation.
- APN adiponectin
- ADRCs cell cluster engraftment and APN production in myocardial infarction ADRCs cell cluster transplanted to the left ventricular anterior wall of myocardial infarction model rats are good in the left ventricular anterior wall scar area 28 days after transplantation (Fig. 8A), and also adiponectin positive at the transplant site (Fig. 8B). It was suggested that the engrafted cell clumps secreted adiponectin continuously.
- engraftment was observed in the myocardium 3 days after transplantation.
- Example 2 Cell surface antigens were analyzed using flow cytometry (FACS) to analyze the constituent cells of ADRCs.
- FACS flow cytometry
- Fresh ADRCs extracted from adipose tissue were suspended in FACS staining solution (phosphate buffered saline supplemented with 5% fetal bovine serum) by the method shown in Example 1.
- Mouse antibodies against CD11b, CD31, CD45, CD73, and CD90 as surface antigen markers and the corresponding mouse IgG1 isotype were used as negative markers.
- Cells were stained for 30 minutes at room temperature, washed, and then analyzed using flow cytometry (BD FACS cant II instrument (BD Biosciences, San Jose, Calif.)).
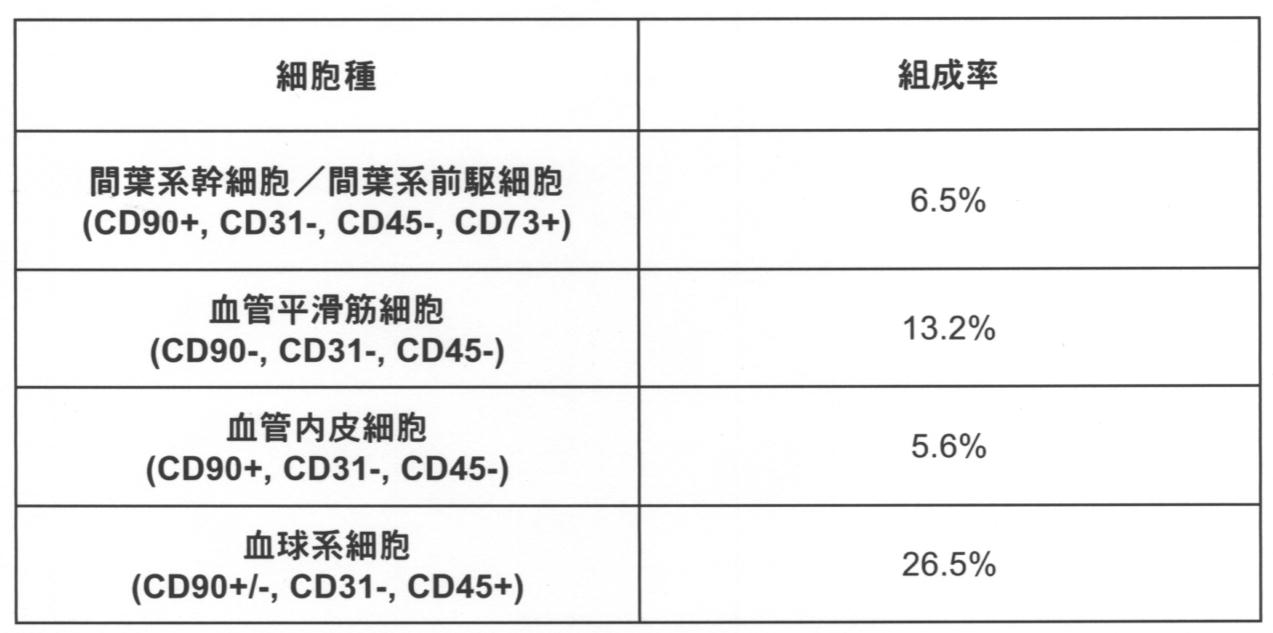
- the constituent cells of ADRC are mainly mesenchymal stem cells / mesenchymal progenitor cells (CD90 +, CD31-, CD45-, CD73 +), endothelial cells (CD90 +, CD31 +, CD45-), vascular smooth muscle (CD90-, It was composed of CD31-, CD45-) and blood cells (CD90 +/-, CD31-, CD45 +).
- the approximate composition ratio is as shown in Table 1.
- adipose tissue-derived mesenchymal stem cells contained 6.5%.
- the transplant material of the present invention includes a cell clump to which separated cells are adhered, and can be produced easily and in a short time.
- adiponectin is secreted and has an excellent therapeutic effect on heart disease. Therefore, the present invention can greatly contribute to the development of transplantation medicine centering on heart disease.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Cell Biology (AREA)
- Developmental Biology & Embryology (AREA)
- Engineering & Computer Science (AREA)
- Biomedical Technology (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Chemical & Material Sciences (AREA)
- General Health & Medical Sciences (AREA)
- Animal Behavior & Ethology (AREA)
- Immunology (AREA)
- Epidemiology (AREA)
- Medicinal Chemistry (AREA)
- Pharmacology & Pharmacy (AREA)
- Zoology (AREA)
- Virology (AREA)
- Biotechnology (AREA)
- Reproductive Health (AREA)
- Hematology (AREA)
- Gynecology & Obstetrics (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Vascular Medicine (AREA)
- Organic Chemistry (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- General Chemical & Material Sciences (AREA)
- Urology & Nephrology (AREA)
- Botany (AREA)
- Dermatology (AREA)
- Oral & Maxillofacial Surgery (AREA)
- Transplantation (AREA)
- Surgery (AREA)
- Heart & Thoracic Surgery (AREA)
- Cardiology (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Medicines Containing Material From Animals Or Micro-Organisms (AREA)
- Materials For Medical Uses (AREA)
- Medicinal Preparation (AREA)
Abstract
Description
[材料と方法]
(1)脂肪組織由来再生細胞(ADRCs=Adipose derived regenerative cells)の調製
9週齢雌性LEW/Seaラットの両鼡径部から脂肪組織を採取した。脂肪組織を鋏で細かく刻み、0.1%のタイプIIコラゲナーゼ溶液中に懸濁し、37℃温浴槽で1時間震盪した。100μmおよび70μmのメッシュフィルターで濾過し、毎分1800回転10分間遠心分離した。沈査を培養培地(10%ウシ胎児血清、および抗生物質含有D-MEM)に懸濁したものを脂肪組織由来再生(間葉系前駆)細胞群(Adipose-derived Regenerative Cells: ADRCs)とした。これらは脂肪組織由来間葉系幹細胞および前駆細胞群を含んでいる。
脂肪組織からのADRCs抽出に引き続き、即座に、1片あたり5x106個のADRCsを含む細胞集塊を作製した。ADRCs細胞懸濁液140μlに対し、フィブリノーゲン60μlを添加してA液とし、また、培養液(10%ウシ胎児血清、抗生物質含有D-MEM)170μLに対し、トロンビン30mlを添加し充分に混和してB液とした。まず培養皿上にA液を滴下し、そこにB液を加え、移植に好適な形状に成形した後に、5%二酸化炭素雰囲気下、37℃の湿潤環境で5~10分程保温して細胞同士を接着させることでADRCs細胞集塊を作製した。ADRCs細胞集塊の作製後、速やかに梗塞部位に移植した。
ADRCs細胞集塊を24、48、72、96、120、144時間培養した上澄液を採取し、酵素免疫抗体法(ELISA法)により上澄液中のアディポネクチン、VEGF、HGF、IL-6の分泌量をそれぞれ測定した。
ADRCs細胞集塊の凍結切片を作成し、4%パラホルムアルデヒドで固定後、オイルレッドO染色およびアディポネクチン免疫染色を施行した。
心筋梗塞モデルは、7週齢雌性LEW/Seaラットを用い、左冠動脈前下行枝結紮術により作製した。イソフルランの吸入麻酔人工呼吸下(1.5%イソフルラン、換気量4ml、110サイクル/分)に全身麻酔をした後、左開胸を行い、心臓を露出した。左冠動脈起始部から2~3mmの部位を7-0プロリン糸で結紮した。冠動脈結紮術2週間後、ADRCs細胞集塊を先曲ピンセット上に載せて左室前壁の梗塞部位に滑らせ、静置した。無治療群に対しては、ADRCsを含まない安定化フィブリンを同様な処置で移植した。
冠動脈結紮術2週間後、ラットを5群に分けて以下の処置を行った。すなわちADRCs細胞集塊を左室前壁に移植した群(A群;n=26)、ピオグリタゾン(PGZ, 50mM)含有ADRCs細胞集塊を移植した群(AP群;n=26)、細胞集塊移植を行わない未治療群(S群;n=26)、ADRCsの左室前壁梗塞周囲への直接心筋内移植群(im群;n=6)および経左室冠動脈内移植群(ic群;n=6)である。手術後12日および56日後に組織学的評価、分子学的評価を行った。手術後1週間毎に心臓超音波検査にて心機能評価を行った。
イソフルランの吸入麻酔により抑制状態を得た後、14MHzトランスジューサーを備えた心臓超音波システムを用いて、乳頭筋レベルの左室短軸像を得た。左室の拡張末期径(LVEDd)および収縮末期径(LVESd)を測定した。測定は3回以上繰り返し、平均値を求めた。左室駆出率(EF%)は以下の式から算出した。
左室駆出率(EF)={(LVEDV-LVESV)/LVEDV}x100=(SV/LVEDV)x100
左室拡張末期容積(LVEDV)={7.0/(2.4+LVEDd)}xLVEDd3
左室収縮終末期容積(LVESV)={7.0/(2.4+LVEDs)}xLVEDs3
(8)組織学的評価
手術後14日目および56日目において、イソフルランの吸入深麻酔により抑制状態を得た後、拍動下に心臓を摘出した。左室を短軸方向にスライスしてコンパウンドに包理後、液体窒素中で凍結し、組織切片を作製した。ヘマトキシリン・エオジン染色、Picro-Sirius red染色、マッソン・トリクロム染色、オイルレッドO染色、アディポネクチン免疫染色、SMA免疫染色、von Willebrand factor免疫染色を施行した。線維化率をPicro-Sirius red染色の画像解析により求めた。梗塞周囲境界部位の生細胞サイズはヘマトキシリン・エオジン染色の1視野(400倍)の細胞短径を計測し、検体あたり10視野の平均値を算出した。また、von Willebrand factor免疫染色の1視野(400倍)あたりの毛細血管数を計測し、検体あたり5視野の平均値を算出した。
移植後14日目および56日目において、摘出した心臓サンプルを梗塞部(scar)、梗塞と正常部位の境界部(border)、非梗塞部(remote)に分けて、それぞれmRNA抽出をした。mRNAから逆転写反応によりcDNAを合成した。定量PCR法により血管内皮細胞増殖因子(VEGF)、アディポネクチン(APN)、アディポネクチン受容体-1(Adipo-R1)、アディポネクチン受容体-2(Adipo-R2)、T-カドヘリン(CDH-13)、および腫瘍壊死因子(TNF-α)の転写量を定量し、内在性コントロールであるグリセルアルデヒド3リン酸脱水素酵素(GAPDH)の転写量で除算した値を、各検体の正常値との比で表した。
データは平均値±標準誤差で表した。群間の比較はt検定にて行い、P値が0.05未満を有意差ありとした。生存率解析は、カプラン・マイヤー法により生存率を算出し、各実験群について、ログランク検定で有意差を求めた。
(1)ADRCs細胞集塊のサイトカイン分泌能および脂肪細胞への分化能
ADRCs細胞集塊(図1A)およびピオグリタゾン(PGZ)含有ADRCs細胞集塊を作製し、5%二酸化炭素雰囲気下、37℃の湿潤環境でそれぞれ144時間培養し、サイトカイン分泌能を検討した。ADRCs細胞集塊およびPGZ含有細胞集塊のアディポネクチン(APN)、VEGF、HGF、IL-6の分泌量は培養液においてそれぞれ経時的に増加した。特に144時間培養後のアディポネクチン濃度は、それぞれ21.7±0.9ng/5x106cells/dayおよび51±3.9ng/5x106cells/dayとなり、PGZ含有のADRCs細胞集塊培養液は、ADRCsのみの細胞集塊と比較して有意に高濃度であった(図1B)。
ADRCs細胞集塊の心筋への生着を検討するため、細胞集塊の作製後速やかにラット心筋への移植を行ったところ、数日から1週間後の細胞集塊は心表面に密着していた(図2A)。毛細血管で心筋との連絡が認められた(図2B)ことから、移植した細胞集塊は心筋へ生着することが確認できた。
慢性心筋梗塞モデルラットに対するADRCs細胞集塊移植後28日の心機能評価結果を図2に示した。心臓超音波検査における左室駆出率(EF)、左室収縮末期径(LVESd)、左室拡張期径(LVEDd)、拡張末期左室壁厚(LVAWD)を心機能の評価指標とした。モデルラットは冠動脈結紮術2週間後、5群に分けて以下の処置後に、試験を行った。すなわちADRCs細胞集塊を左室前壁に移植した群(A群)、ピオグリタゾン(PGZ)含有ADRCs細胞集塊を左室前壁に移植した群(AP群)、細胞集塊移植を行わない未治療群(S群)、ADRCs細胞の左室前壁梗塞周囲への直接心筋内移植群(im群)、および経左室冠動脈内移植群(ic群)である。
心筋梗塞モデルラットに対するADRCs細胞集塊移植後、14日目および56日目に、組織学的解析を施行した。未治療であるS群は強度の左室前壁菲薄化を認めた(図5A)が、A群(図5B)およびAP群(図5C)はS群、im群、ic群とに比して左室前壁が厚く、左室前壁組織が維持されていることを認めた(図5D)。梗塞サイズを定量したところ、統計学的有意差はないもののA群およびAP群における梗塞サイズはS群、im群、ic群と比して小さい傾向を示した(図5E)。さらに、梗塞部周縁の毛細血管密度を測定したところA群(図5G)およびAP群(図5H)ではS群(図5F)、im群、ic群と比して有意に高い毛細血管密度を示した(図5I)。
心筋梗塞モデルラットに対するADRCs細胞集塊移植14日および56日後、組織学的解析を施行した。各群の心筋梗塞部周縁における細胞径をヘマトキシリン・エオジン染色(図6A~C)およびPAS染色(図6D~F)により検出したところ、A群およびAP群における細胞短径はS群、im群、ic群と比して有意に低値であった(図6G)。以上の結果より、ADRCs細胞集塊移植は、残存心筋細胞に対し抗アポトーシスなどの保護作用を有する可能性が示唆された。
ADRCs細胞集塊移植後56日の心筋組織における心筋保護・抗炎症効果に関する検討結果を図7に示す。各群の梗塞部周縁の血管再生および心筋保護サイトカイン転写程度を評価したところ、AP群では他群と比して梗塞部周縁におけるアディポネクチン(APN)の転写量は有意に高かった(図7A)。またA群においても、S群よりも、APNの転写量は有意に高かった(図7A)。その他のAdipo-R1、Adipo-R2、CDH-13、VEGF、およびTNF-αの転写量には有意差を認められなかった(図7B~F)。以上より、ADRCs細胞集塊にPGZを添加することにより、心筋梗塞後の心機能改善効果がさらに増強されている可能性が示唆された。
心筋梗塞モデルラットの左室前壁に移植されたADRCs細胞集塊は、移植後28日の左室前壁瘢痕領域に良好に生着しており(図8A)、移植部位でもアディポネクチン陽性であった(図8B)。生着した細胞集塊は持続的にアディポネクチンを分泌していたことが示唆された。また、比較対象とした、ADRCsの心筋内(図8C)および冠動脈内(図8D)移植を行った群においても移植後3日で心筋内に生着を認めた。
ADRCsの構成細胞を分析するためにフローサイトメトリー(FACS)を用いて細胞表面抗原を解析した。実施例1に示す方法によって、脂肪組織から抽出した新鮮なADRCsをFACS用染色液(5%ウシ胎児血清で補完したリン酸緩衝整理食塩水)に懸濁した。表面抗原マーカーとしてのCD11b、CD31、CD45、CD73、CD90に対するマウス抗体およびそれに対応するマウスIgG1アイソタイプを陰性マーカーとして用いた。細胞を室温にて30分間染色し、洗浄した後にフローサイトメトリー(BD FACS cant II instrument(BD Biosciences, San Jose, CA))を用いて解析した。
Claims (7)
- 分離された細胞を接着剤により接着させることにより得られる細胞集塊を含む、心疾患の治療のための移植材料。
- 分離された細胞が脂肪組織由来再生細胞、骨髄由来再生細胞、臍帯由来再生細胞、平滑筋由来再生細胞、多能性幹細胞およびそれに由来する再生細胞、血管内皮細胞、ならびに単球からなる群より選択される、請求項1に記載の移植材料。
- 分離された細胞が、PPARγアゴニストを作用させた脂肪組織由来再生細胞である、請求項1に記載の移植材料。
- 分離された細胞が培養されていないものである、請求項1から3のいずれかに記載の移植材料。
- 接着剤がフィブリノーゲンを含む、請求項1から4のいずれかに記載の移植材料。
- 請求項1から5のいずれかに記載の移植材料で、心疾患を罹患している対象の心表面を被覆することを特徴とする、心疾患の治療方法。
- 心疾患を罹患している対象が、移植材料が由来する細胞を採取した対象である、請求項6に記載の治療方法。
Priority Applications (5)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US16/071,123 US12226436B2 (en) | 2016-01-19 | 2017-01-18 | Transplant material for treatment of heart disease |
| JP2017562848A JP6854519B2 (ja) | 2016-01-19 | 2017-01-18 | 心疾患の治療のための移植材料 |
| EP17741426.5A EP3406255B1 (en) | 2016-01-19 | 2017-01-18 | Transplant material for therapy for heart disease |
| SG11201806177QA SG11201806177QA (en) | 2016-01-19 | 2017-01-18 | Transplant material for treatment of heart disease |
| CN201780006848.7A CN108472319B (zh) | 2016-01-19 | 2017-01-18 | 用于治疗心脏病的移植材料 |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2016-008096 | 2016-01-19 | ||
| JP2016008096 | 2016-01-19 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2017126549A1 true WO2017126549A1 (ja) | 2017-07-27 |
Family
ID=59362376
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2017/001538 Ceased WO2017126549A1 (ja) | 2016-01-19 | 2017-01-18 | 心疾患の治療のための移植材料 |
Country Status (6)
| Country | Link |
|---|---|
| US (1) | US12226436B2 (ja) |
| EP (1) | EP3406255B1 (ja) |
| JP (1) | JP6854519B2 (ja) |
| CN (1) | CN108472319B (ja) |
| SG (1) | SG11201806177QA (ja) |
| WO (1) | WO2017126549A1 (ja) |
Cited By (7)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2019132026A1 (ja) | 2017-12-28 | 2019-07-04 | 株式会社カネカ | 接着性幹細胞を含む細胞集団とその製造方法、及び医薬組成物 |
| WO2019132025A1 (ja) | 2017-12-28 | 2019-07-04 | 株式会社カネカ | 接着性幹細胞を含む細胞集団とその製造方法、及び医薬組成物 |
| JPWO2018074381A1 (ja) * | 2016-10-18 | 2019-08-08 | 国立大学法人大阪大学 | 疾患治療剤調製用キット、疾患治療剤及び疾患治療剤の調製方法 |
| WO2019187918A1 (ja) * | 2018-03-29 | 2019-10-03 | 国立大学法人 琉球大学 | 分化コントロール化合物を用いて造腫瘍性をもつおそれのある未分化iPS細胞等の混入を除去する方法 |
| WO2020184350A1 (ja) | 2019-03-08 | 2020-09-17 | 株式会社カネカ | 多能性幹細胞の大量培養 |
| WO2021045190A1 (ja) * | 2019-09-05 | 2021-03-11 | 国立大学法人東北大学 | 心筋炎の治療剤 |
| JP2021102571A (ja) * | 2019-12-25 | 2021-07-15 | ロート製薬株式会社 | 高血圧性心疾患治療剤 |
Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2005047491A2 (en) * | 2003-11-10 | 2005-05-26 | Amgen Inc. | Methods of using g-csf mobilized c-kit+cells in the production of embryoid body-like cell clusters for tissue repair and in the treatment of cardiac myopathy |
| WO2008153179A1 (ja) * | 2007-06-14 | 2008-12-18 | Akifumi Matsuyama | 脂肪組織由来多系統前駆細胞 |
| JP2009542237A (ja) * | 2006-07-13 | 2009-12-03 | セルアーティス アーベー | ヒト胚盤胞由来幹細胞に由来する多能性心臓前駆細胞の新規の集団 |
| WO2013162057A1 (ja) * | 2012-04-25 | 2013-10-31 | 独立行政法人理化学研究所 | 心筋指向性細胞を含む細胞製剤 |
Family Cites Families (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP5103626B2 (ja) | 2005-01-27 | 2012-12-19 | 財団法人ヒューマンサイエンス振興財団 | 間葉系幹細胞を含む細胞シート |
| DE602005026724D1 (de) | 2005-05-25 | 2011-04-14 | Cytori Therapeutics Inc | Verfahren zur verwendung von aus fettgewebe stammenden zellen bei der behandlung von herz-kreislauf-leiden |
| CN101517069A (zh) | 2006-07-13 | 2009-08-26 | 塞拉帝思股份公司 | 由人类胚泡来源的干细胞衍生的多能心脏前体细胞新种群 |
| US20120308533A1 (en) | 2009-12-03 | 2012-12-06 | Osaka University | Adipocyte sheet, three-dimensional structure thereof, and method for producing the same |
| SG11201405257WA (en) | 2012-03-12 | 2014-09-26 | Univ Singapore | Generation of brown adipose tissue (bat) from mesenchymal cells |
-
2017
- 2017-01-18 JP JP2017562848A patent/JP6854519B2/ja active Active
- 2017-01-18 CN CN201780006848.7A patent/CN108472319B/zh active Active
- 2017-01-18 EP EP17741426.5A patent/EP3406255B1/en active Active
- 2017-01-18 WO PCT/JP2017/001538 patent/WO2017126549A1/ja not_active Ceased
- 2017-01-18 US US16/071,123 patent/US12226436B2/en active Active
- 2017-01-18 SG SG11201806177QA patent/SG11201806177QA/en unknown
Patent Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2005047491A2 (en) * | 2003-11-10 | 2005-05-26 | Amgen Inc. | Methods of using g-csf mobilized c-kit+cells in the production of embryoid body-like cell clusters for tissue repair and in the treatment of cardiac myopathy |
| JP2009542237A (ja) * | 2006-07-13 | 2009-12-03 | セルアーティス アーベー | ヒト胚盤胞由来幹細胞に由来する多能性心臓前駆細胞の新規の集団 |
| WO2008153179A1 (ja) * | 2007-06-14 | 2008-12-18 | Akifumi Matsuyama | 脂肪組織由来多系統前駆細胞 |
| WO2013162057A1 (ja) * | 2012-04-25 | 2013-10-31 | 独立行政法人理化学研究所 | 心筋指向性細胞を含む細胞製剤 |
Non-Patent Citations (2)
| Title |
|---|
| FUKUSHIMA, S. ET AL.: "Choice of cell -delivery route for successful cell transplantation therapy for the heart", FUTURE CARDIO L, vol. 9, no. 2, 2013, pages 215 - 227, XP055400668, ISSN: 1479-6678 * |
| See also references of EP3406255A4 * |
Cited By (11)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPWO2018074381A1 (ja) * | 2016-10-18 | 2019-08-08 | 国立大学法人大阪大学 | 疾患治療剤調製用キット、疾患治療剤及び疾患治療剤の調製方法 |
| JP7108541B2 (ja) | 2016-10-18 | 2022-07-28 | ロート製薬株式会社 | 疾患治療剤調製用キット、疾患治療剤及び疾患治療剤の調製方法 |
| WO2019132026A1 (ja) | 2017-12-28 | 2019-07-04 | 株式会社カネカ | 接着性幹細胞を含む細胞集団とその製造方法、及び医薬組成物 |
| WO2019132025A1 (ja) | 2017-12-28 | 2019-07-04 | 株式会社カネカ | 接着性幹細胞を含む細胞集団とその製造方法、及び医薬組成物 |
| WO2019187918A1 (ja) * | 2018-03-29 | 2019-10-03 | 国立大学法人 琉球大学 | 分化コントロール化合物を用いて造腫瘍性をもつおそれのある未分化iPS細胞等の混入を除去する方法 |
| JPWO2019187918A1 (ja) * | 2018-03-29 | 2021-03-25 | 国立大学法人 琉球大学 | 分化コントロール化合物を用いて造腫瘍性をもつおそれのある未分化iPS細胞等の混入を除去する方法 |
| JP7217542B2 (ja) | 2018-03-29 | 2023-02-03 | 国立大学法人 琉球大学 | 分化コントロール化合物を用いて造腫瘍性をもつおそれのある未分化iPS細胞等の混入を除去する方法 |
| WO2020184350A1 (ja) | 2019-03-08 | 2020-09-17 | 株式会社カネカ | 多能性幹細胞の大量培養 |
| WO2021045190A1 (ja) * | 2019-09-05 | 2021-03-11 | 国立大学法人東北大学 | 心筋炎の治療剤 |
| JP2021102571A (ja) * | 2019-12-25 | 2021-07-15 | ロート製薬株式会社 | 高血圧性心疾患治療剤 |
| JP7495075B2 (ja) | 2019-12-25 | 2024-06-04 | ロート製薬株式会社 | 高血圧性心疾患治療剤 |
Also Published As
| Publication number | Publication date |
|---|---|
| EP3406255C0 (en) | 2023-06-07 |
| CN108472319B (zh) | 2021-12-28 |
| JPWO2017126549A1 (ja) | 2018-11-08 |
| EP3406255A4 (en) | 2019-08-14 |
| JP6854519B2 (ja) | 2021-04-07 |
| SG11201806177QA (en) | 2018-08-30 |
| US12226436B2 (en) | 2025-02-18 |
| EP3406255B1 (en) | 2023-06-07 |
| EP3406255A1 (en) | 2018-11-28 |
| US20210187031A1 (en) | 2021-06-24 |
| CN108472319A (zh) | 2018-08-31 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| JP6854519B2 (ja) | 心疾患の治療のための移植材料 | |
| JP4971787B2 (ja) | 心臓血管疾患の治療における脂肪組織由来細胞の使用方法 | |
| AU2011293144B2 (en) | Bone marrow derived CD271 precursor cells for cardiac repair | |
| US11660317B2 (en) | Compositions comprising cardiosphere-derived cells for use in cell therapy | |
| JP6781973B2 (ja) | 腎臓病進行抑制細胞シート組成物、その製造方法、及び、それを用いた腎臓病進行抑制方法 | |
| JP7072135B2 (ja) | 線維芽細胞を含む心臓疾患を治療するための注射用組成物、及び治療用線維芽細胞の製造方法 | |
| US20250073278A1 (en) | Methods and compositions for treatment of penile defects | |
| JP5894071B2 (ja) | 心臓組織由来細胞 | |
| US11963983B2 (en) | Methods of cardiac repair | |
| HK1256653A1 (en) | Transplant material for therapy for heart disease | |
| HK1256653B (en) | Transplant material for therapy for heart disease | |
| WO2019104466A1 (en) | Methods of producing populations of mesenchymal stem cells from peripheral blood and uses thereof | |
| WO2022123958A1 (en) | Pharmaceutical composition for use in prevention and treatment of liver fibrosis and/or liver cirrhosis, comprising adipose-derived regenerative cells (adrcs) | |
| TWI656215B (zh) | 自周邊血液製備間質幹細胞群的方法及其用途 | |
| EP4671364A1 (en) | CELL POPULATION CONTAINING CARDIAC STEM CELLS | |
| Martens | Novel Platforms for Cardiovascular Repair | |
| WO2016127153A1 (en) | Methods and compositions for treatment of penile defects |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 17741426 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2017562848 Country of ref document: JP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 11201806177Q Country of ref document: SG |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2017741426 Country of ref document: EP |
|
| ENP | Entry into the national phase |
Ref document number: 2017741426 Country of ref document: EP Effective date: 20180820 |