WO2018207866A1 - がん治療効果の検査方法及び免疫応答誘導用組成物 - Google Patents
がん治療効果の検査方法及び免疫応答誘導用組成物 Download PDFInfo
- Publication number
- WO2018207866A1 WO2018207866A1 PCT/JP2018/018083 JP2018018083W WO2018207866A1 WO 2018207866 A1 WO2018207866 A1 WO 2018207866A1 JP 2018018083 W JP2018018083 W JP 2018018083W WO 2018207866 A1 WO2018207866 A1 WO 2018207866A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- cancer
- antibody
- xage1
- peptide
- positive
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Images

























Classifications
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6854—Immunoglobulins
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/03—Peptides having up to 20 amino acids in an undefined or only partially defined sequence; Derivatives thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/0005—Vertebrate antigens
- A61K39/0011—Cancer antigens
- A61K39/001184—Cancer testis antigens, e.g. SSX, BAGE, GAGE or SAGE
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K14/00—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- C07K14/82—Translation products from oncogenes
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12N—MICROORGANISMS OR ENZYMES; COMPOSITIONS THEREOF; PROPAGATING, PRESERVING, OR MAINTAINING MICROORGANISMS; MUTATION OR GENETIC ENGINEERING; CULTURE MEDIA
- C12N5/00—Undifferentiated human, animal or plant cells, e.g. cell lines; Tissues; Cultivation or maintenance thereof; Culture media therefor
- C12N5/06—Animal cells or tissues; Human cells or tissues
- C12N5/0602—Vertebrate cells
- C12N5/0634—Cells from the blood or the immune system
- C12N5/0636—T lymphocytes
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/15—Medicinal preparations ; Physical properties thereof, e.g. dissolubility
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/575—Immunoassay; Biospecific binding assay; Materials therefor for cancer
- G01N33/57557—Immunoassay; Biospecific binding assay; Materials therefor for cancer of other specific parts of the body, e.g. brain
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/80—Vaccine for a specifically defined cancer
- A61K2039/892—Reproductive system [uterus, ovaries, cervix, testes]
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12N—MICROORGANISMS OR ENZYMES; COMPOSITIONS THEREOF; PROPAGATING, PRESERVING, OR MAINTAINING MICROORGANISMS; MUTATION OR GENETIC ENGINEERING; CULTURE MEDIA
- C12N2501/00—Active agents used in cell culture processes, e.g. differentation
- C12N2501/50—Cell markers; Cell surface determinants
- C12N2501/505—CD4; CD8
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/34—Genitourinary disorders
- G01N2800/344—Disorders of the penis and the scrotum and erectile dysfuncrion
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/52—Predicting or monitoring the response to treatment, e.g. for selection of therapy based on assay results in personalised medicine; Prognosis
Definitions
- the present invention relates to a test for predicting the effect or prognosis of cancer treatment and the use of an immune response-inducing peptide.
- tissue types are roughly classified into small cell lung cancer (10%) and non-small cell lung cancer (NSCLC) (90%).
- NSCLC non-small cell lung cancer
- lung adenocarcinoma accounts for 70-80%.
- Median survival (OS) is about 12 months for small cell lung cancer and about 30 months for non-small cell lung cancer.
- anti-PD-1 antibody therapy (nivolumab, pembrolizumab), which is an immune checkpoint molecule inhibitor, is the first and second-line treatment of advanced stage NSCLC. Prolonged, and anti-PD-1 antibody therapy is currently being implemented in Japan, the United States, and the European Union.
- a useful biomarker for a successful example of an immune checkpoint molecule inhibitor is a PD-L1 molecule expressed in a tumor and an immunocompetent cell in the tumor, but the response rate is 30- even in the high PD-L1 expression group. Since it is about 40% and immune checkpoint molecule inhibitors are very expensive, the identification of new biomarkers is awaited.
- XAGE1 antigen expressed in lung adenocarcinoma, the most common type of lung cancer.
- XAGE1 antigen is expressed in 40-50% of advanced stage lung adenocarcinoma, and antibody (IgG) reaction against XAGE1 is observed in about half of patients expressing XAGE1 antigen, and those who are positive for antibody against XAGE1 (prognosis) Has been clarified to be extended (Non-Patent Documents 1 and 2).
- XAGE1 antigen is one of cancer testis antigens.
- Cancer testis antigen (CT antigen) is expressed in many cancers, but is a general term for antigens expressed only in the testis in normal tissues, and many CT antigens are known (Non-patent Documents 3 and 4). .
- the response rate in the CheckMate-017 trial in the phase III clinical trial comparing nivolumab and docetaxel in previously treated lung squamous cell carcinoma was 36% in the nivolumab group and 31% in the docetaxel group.
- the response rate in the same CheckMate-057 trial comparing nivolumab and docetaxel in previously treated non-squamous non-small cell lung cancer was 19% in the nivolumab group and 12% in the docetaxel group.
- the Nivolumab group was not significant compared to the docetaxel group in the CheckMate-017 trial and the CheckMate-057 trial, whereas the Nivolumab group 33%, the docetaxel group 30%, and the CheckMate-057 in the CheckMate-017 trial, respectively. In the study, it was 44% in the nivolumab group and 29% in the docetaxel group.
- pembrolizumab Another useful anti-PD-1 antibody, pembrolizumab, was studied in the KEYNOTE-001 and KEYNOTE-010 studies for previously treated non-small cell lung cancer.
- the overall response rate was 18-20%, and 19-23% of PD-L1-positive tumors and 9-13% of PD-L1-negative tumors were successful.
- the KEYNOTE-010 trial is a phase III clinical trial comparing pembrolizumab and docetaxel in patients with tumor PD-L1 expression of 1% or higher, and the response rate is 18.0% -18.5% in the pembrolizumab group, The docetaxel group was 9.3%.
- the OS was 10.4 to 12.7 months in the pembrolizumab group and 8.5 months in the docetaxel group. Therefore, the pembrolizumab group significantly increased OS compared to the docetaxel group.
- the progression-free survival (PFS) was not significantly different from the docetaxel group.
- the response rate was 29.1% -30.2% in the pembrolizumab group, whereas 7.9% in the docetaxel group.
- the OS was 14.9 months to 17.3 months in the pembrolizumab group, and in the patient population with tumor PD-L1 expression of 50% or more, PFS was also significantly improved compared to the docetaxel group. Therefore, it was revealed that pembrolizumab prolongs the high antitumor effect and prognosis of tumors with high expression of tumor PD-L1.
- the anti-PD-L1 antibody atezolizumab is also targeted for previously treated non-small cell lung cancer in the same manner as nivolumab and pembrolizumab.
- OS showed a significant prolongation effect at 12.6 months in the atezolizumab group and 9.7 months in the docetaxel group.
- PD-L1 was expressed in tumor or tumor-infiltrating immune cells in the cancer immune microenvironment, it was shown that the OS further extended the prognosis to 15.1-15.5 months.
- the response rate of the atezolizumab group in which PD-L1 was highly expressed in the cancer immune microenvironment was 38%, and only about 15% in the docetaxel group in the cancer immune microenvironment without PD-L1 expression. Similar results to the POPLAR study have been observed in the OAK study, a Phase III study that is compared to docetaxel for previously treated non-small cell lung cancer.
- PD-L1 expression in tumors or immunocompetent cells in tumors is useful as biomarkers for successful cases of immune checkpoint molecule inhibitors at present.
- the response rate of the immune checkpoint molecule inhibitor is 30-40%, and also 10% for PD-L1 low expression or negative cases Examples of successful responses before and after.
- each immune checkpoint molecule inhibitor (nivolumab, pembrolizumab, atezolizumab) has been subjected to its own companion diagnostic method (PD-L1 expression analysis), which is causing confusion in clinical settings.
- the present inventors have found that the therapeutic effect of cancer can be predicted or confirmed by detecting an antibody against a cancer testis antigen or an anti-p53 antibody.
- an IgG type XAGE1 antibody hereinafter also referred to as XAGE1-IgG
- an IgA type XAGE1 antibody hereinafter also referred to as XAGE1-IgA
- an IgG type anti-NY-ESO- It was found that one antibody (hereinafter also referred to as NY-ESO-1-IgG) is an index for predicting the therapeutic effect and prognosis of cancer treatment.
- the novel peptide for cancer vaccines and its composition were discovered. Furthermore, they found a screening method for cancer vaccine peptides. That is, the present invention includes the following aspects.
- a method for examining a cancer therapeutic effect comprising detecting an antibody against a cancer testis antigen in a sample.
- the cancer testis antigen is at least one cancer testis antigen selected from the group consisting of XAGE1, NY-ESO-1, MAEL, BAGE, BORIS, MAGE-B3 and SSX4.
- 3. The test method according to item 1 or 2, wherein an IgG type antibody and an IgA type antibody are detected. 4).
- a method for examining a cancer therapeutic effect comprising detecting an anti-p53 antibody in a sample. 6).
- a carrier comprising at least one selected from the group consisting of a cancer testis antigen, a peptide comprising a part of a cancer testis antigen, p53 and a peptide comprising a part of p53, and an anti-human IgG antibody
- a reagent kit for testing a therapeutic effect on cancer comprising a reagent and a reagent containing an anti-human IgA antibody. 8).
- Activation comprising the step of stimulating and culturing CD4-positive T cells or CD8-positive T cells obtained from peripheral blood with SLP1 having the amino acid sequence shown in SEQ ID NO: 1 and SLP2 having the amino acid sequence shown in SEQ ID NO: 2.
- SLP1 having the amino acid sequence shown in SEQ ID NO: 1
- SLP2 having the amino acid sequence shown in SEQ ID NO: 2.
- 9. A method for inducing an immune response with at least one peptide selected from a) to c) according to item 8 and at least one peptide selected from d) to f) according to item 8. 17.
- the test method of the present invention can accurately predict the effect and prognosis of cancer treatment before cancer treatment. Moreover, the effect of cancer treatment can be confirmed after cancer treatment. More specifically, the effects of chemotherapy (effects of anticancer agents), the effects of immunotherapy, and the effects of immune checkpoint molecule inhibitors can be accurately predicted. In particular, it is possible to determine whether or not the immune checkpoint molecule inhibitor is successful regardless of PD-L1 expression. It is epoch-making that the effect can be predicted even for patients whose PD-L1 expression could not be predicted.
- immune checkpoint molecular inhibitors are very expensive, and there is currently no effective biomarker indicating the end of the treatment. Unlike conventional chemotherapy, immune checkpoint molecule inhibitors are effective in some patients, but serious adverse events such as the development of systemic autoimmune diseases are also a concern.
- the test method of the present invention can be predicted even for patients with low therapeutic effects, and the treatment can be stopped in consideration of balance with side effects. From these facts, the fact that immune checkpoint molecule inhibitors can be selected effectively by the present invention is epoch-making in terms of medical economics including treatment costs, side effects, etc.
- novel peptide of the present invention and the composition for inducing an immune response containing the novel peptide can induce an immune response against cancer by actively inducing XAGE1 immunity, thereby becoming a cancer therapeutic agent (cancer vaccine).
- cancer vaccine cancer vaccine
- the novel peptide and composition for inducing immune response of the present invention can induce XAGE1-specific antibodies, particularly IgG-type anti-XAGE1 antibodies, and can further induce antigen-specific T cells.
- novel peptide of the present invention and the composition for inducing immune response of the present invention actively induce XAGE1 immunity to ineffective cases of chemotherapy, immunotherapy and immune checkpoint molecule inhibitors, or poor prognosis groups
- XAGE1 immunity to ineffective cases of chemotherapy, immunotherapy and immune checkpoint molecule inhibitors, or poor prognosis groups
- it is possible to achieve a breakthrough treatment leading to a treatment success and a good prognosis group.
- it enables powerful cancer immunotherapy by combining existing treatments and new treatments.
- the immune response inducing composition of the present invention is also excellent in safety.
- the novel peptide of the present invention is a long-chain peptide and thus contains various epitopes, and can induce a stronger immune response than conventional epitope vaccines. Furthermore, a stronger immune response can be induced by using at least one peptide selected from a) to c) and at least one peptide selected from d) to f) in combination.
- the screening method of the present invention makes it possible to select peptides suitable for cancer vaccines.
- the activated CD4 positive T cells or activated CD8 positive T cells obtained by the method for preparing activated CD4 positive T cells or activated CD8 positive T cells of the present invention are used for cell therapy such as adoptive immunity (T cell) therapy. Can be used.
- FIG. 1 shows cancer-related antigens for sera collected from 157 patients with early or locally advanced lung adenocarcinoma (cStage I-IIIA) and 145 patients with advanced stage (cStage IIIB-IV) lung adenocarcinoma, The results of detecting antigen-specific IgG and antigen-specific IgA against XAGE1, MAGE-A3, SSX-2, NY-ESO-1 and TP53 are shown.
- FIG. 2 shows the test results of serum collected from 157 patients with early or locally advanced lung adenocarcinoma (cStage I-IIIA) and 145 patients with advanced stage (cStageIIIB-IV) lung cancer.
- FIG. 3A shows the results of examination of sera obtained from 55 lung adenocarcinoma patients positive for XAGE1 antigen for autoantibody responses to 51 types of cancer antigens.
- XAGE1-IgG and XAGE1-IgA have been shown to be surrogate markers for immune responses against autologous tumors.
- immune responses to various cancer antigens are observed.
- an anti-XAGE1 antibody of IgA type indicates that the immune response against the self-tumor is attenuated.
- XAGE1 immunonegative cases show that almost no immune response to self tumors is observed.
- FIG. 3B shows that XAGE1-IgG positive and XAGE1-IgA negative individuals have an immune response to multiple cancer antigens and a potentially high immune response against cancer (immune activated state).
- FIG. 4 shows the results of measuring immunosuppressive cytokines in the serum of 145 patients with advanced stage lung adenocarcinoma.
- FIG. 5 shows the results of analysis of the state of B cells and T cells in the local cancer of patients with early or locally advanced lung adenocarcinoma. 5A and 5B show the accumulation state of cancer local (TIL) cells.
- FIG. 5C shows that about 30% of cases have high IgA positive B cell infiltration.
- FIG. 5D shows that the number of regulatory T cells in the tumor area is increased in cases where IgA positive B cell infiltration is high.
- FIG. 5E shows that IL-10, an immunosuppressive cytokine, was observed in tumor-infiltrating lymphocytes compared to peripheral blood, and that B cells in addition to T cells also produced IL-10.
- FIG. 5F shows that the IL-10 producing tumor infiltrating B cells shown in FIG. 5E are IgA positive.
- FIG. 6 shows the results of analysis of immune checkpoint molecules expressed in IgA + B cells of lung adenocarcinoma patients.
- FIG. 7 shows that the XAGE1-IgG positive group significantly prolongs the median survival, and this tendency is remarkable in EGFR gene mutation negative cases.
- FIG. 8 shows that the success rate of the first chemotherapy is significantly higher in the XAGE1-IgG positive and XAGE1-IgA negative group than in the XAGE1-IgG positive and XAGE1-IgA positive group and the group without immune response.
- FIG. 10 shows a group with an immune response to XAGE1 or NY-ESO-1 (XAGE1-IgG positive or NY-ESO-1-IgG positive group) and a group without an immune response (group without antibodies to XAGE1 and NY-ESO-1) Shows the response rate, progression-free survival (Progression-Free Survival) and overall survival (Overall Survival) after treatment with anti-PD-1 antibody, which is an immune checkpoint molecule inhibitor.
- FIG. 11 shows the results shown in FIG.
- FIG. 12 shows the results of monitoring anti-NY-ESO-1, anti-XAGE1 and anti-p53 antibodies in successful cases of anti-PD-1 antibody therapy.
- FIG. 13A shows the results of analysis of immune responses to 50 cancer antigens including XAGE1 and NY-ESO-1 antibodies, using sera before treatment of patients treated with anti-PD-1 antibody therapy.
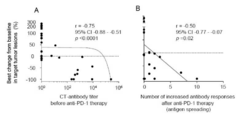
- FIG. 14A shows the relationship between the rate of change in target lesions due to anti-PD-1 antibody therapy (minus means tumor shrinkage) and the antibody titers of antibodies against CT antigens (XAGE1-IgG and NYESO-1-IgG). Yes.
- FIG. 14B shows the relationship between the rate of change of target lesions by anti-PD-1 antibody therapy and the number of immune responses (antigen spreading) to multiple antigens after treatment.
- FIG. 15A shows the difference in immune response to multiple antigens before and after anti-PD-1 antibody therapy.
- FIG. 15B shows that in the successful cases of anti-PD-1 antibody therapy, spreading of the immune response against MAGE-B3 antigen fistula and SSX4 antigen was frequently observed, and not in the non-successful cases.
- FIG. 16 shows that an immune response to the SSX4 antigen was actually observed in a completely successful case of an anti-CCR4 antibody + anti-PD-1 antibody, preoperative combination physician-initiated clinical trial case.
- FIG. 17 shows that the course of tumor shrinkage and the immune response to SSX4 were correlated.
- FIG. 18 shows that positive antibodies against CT antigen (anti-XAGE1 antibody and anti-NY-ESO-1 antibody) can clearly discriminate the effect of anti-PD-1 antibody therapy from known biomarkers.
- FIG. 19 shows that 4C34-1 which is a CD4 positive T cell clone specific for SLP2 (hereinafter also referred to as CD4 clone) and 8C34TY which is a CD8 positive T cell clone specific for SLP1 (hereinafter also referred to as CD8 clone) are recognized. The peptide to be shown is shown.
- FIG. 20 shows the results of stimulating CD4 clone (4C34-1) T cells, CD8 clone (8C34TY) T cells, and a mixture of these T cells with SLP1 alone, SLP2 alone, or a combination of SLP1 and SLP2.
- FIG. 5 shows that stimulation with a combination of SLP1 and SLP2 induces a stronger immune response.
- FIG. 21 shows the results of detection of IgG and IgA on the surface of B cells after stimulation of peripheral blood mononuclear cells with CD4 clone T cells and CD8 clone T cells with SLP1 alone, SLP2 alone, or each peptide combination. . Increased expression of IgG on the surface of B cells was observed when SLP1 and SLP2 were used in combination.
- FIG. 22 shows the detection results of XAGE1-specific antibodies in the culture supernatant after stimulation of B cells with SLP1 alone, SLP2 alone, or a combination of each peptide together with CD4 clone T cells and CD8 clone T cells.
- SLP1 and SLP2 were used in combination, XAGE1-IgG was produced and IgA production was not observed.
- FIG. 23 shows that administration of XAGE1 vaccine containing SLP1 and SLP2 showed an increase in XAGE1-IgG antibody titer in 4 of 7 cases, and that XAGE1-IgA and NY-ESO-1-IgG were not induced .
- FIG. 22 shows the detection results of XAGE1-specific antibodies in the culture supernatant after stimulation of B cells with SLP1 alone, SLP2 alone, or a combination of each peptide together with CD4 clone T cells and CD8 clone T cells.
- SLP1 and SLP2 were used in combination
- FIG. 24 shows that suppression or reduction in tumor marker elevation was observed in 4 of 7 cases by administration of XAGE1 vaccine.
- FIG. 25 shows that an immune response could be induced by low dose administration of XAGE1 vaccine.
- CD4-positive T cells obtained from patients mainly respond to SLP1, indicating that the combined use of SLP1 and SLP2 enhances the immune response.
- FIG. 26 shows that an immune response could be induced by administration of a dose in the XAGE1 vaccine.
- CD4-positive T cells obtained from patients respond to SLP1 and SLP2, indicating that the combined use of SLP1 and SLP2 enhances the immune response.
- the test method of the present invention is characterized by detecting an antibody against a cancer testis antigen or an anti-p53 antibody in a sample.
- the method for screening a peptide for cancer vaccine of the present invention is characterized by detecting an antibody against a cancer testis antigen or an anti-p53 antibody in a sample.
- the cancer testis antigen (hereinafter also referred to as CT antigen) is not particularly limited, and is an antigen that is expressed in cancer cells and expressed only in testis in normal tissues. is there.
- CT antigen is an antigen that is expressed in cancer cells and expressed only in testis in normal tissues.
- the present invention is characterized by detecting an antibody against a CT antigen, and preferred CT antigens include XAGE1, NY-ESO-1, MAEL, BAGE, BORIS, MAGE-B3 and SSX4. More preferred CT antigens include XAGE1 and NY-ESO-1.
- the test method and screening method of the present invention preferably detect an antibody against an IgG type CT antigen or an anti-p53 antibody.
- Preferred antibodies against CT antigen include XAGE1 antibody, anti-NY-ESO-1 antibody, anti-MAEL antibody, anti-BAGE antibody, anti-BORIS antibody, anti-MAGE-B3 antibody and anti-SSX4 antibody, these antibodies are of IgG type It is preferable. More preferable antibodies include IgG type anti-XAGE1 antibody and IgG type anti-NY-ESO-1 antibody.
- an antibody against an IgA type CT antigen is detected in addition to an antibody against an IgG type CT antigen.
- Suitable antibodies against IgA type CT antigens include IgA type anti-XAGE1 antibodies.
- an IgG type anti-XAGE1 antibody and an IgA type anti-XAGE1 antibody are detected.
- the “cancer vaccine” means a pharmaceutical composition capable of inducing an immune response against cancer, and the immune response induction includes humoral immunity induction and / or cellular immunity induction. included.
- test method of the present invention detects an antibody against a CT antigen or an anti-p53 antibody in a sample collected from a subject before cancer treatment. Moreover, one Embodiment of the test
- the effect and prognosis of the cancer treatment can be predicted before the cancer treatment.
- the effect of the cancer treatment can be confirmed after cancer treatment and the prognosis can be predicted. Furthermore, the effect and prognosis of subsequent treatment can be predicted.
- test method of the present invention is suitable for prediction, confirmation, and prognosis prediction of the effects of various cancer treatments, but is suitable for prediction, confirmation, and prognosis prediction of the effects of chemotherapy and immunotherapy. It is more suitable for predicting the effect of immunotherapy, and particularly suitable for predicting the effect of treatment with immune checkpoint molecule inhibitors.
- Chemotherapy includes treatment by administration of various anticancer drugs such as platinum preparations.
- Immunotherapy includes immunosuppression inhibition therapy (treatment with immune checkpoint molecule inhibitors), cytokine (IL-2 etc.) therapy, BRM therapy (immunostimulatory etc.), cancer vaccine therapy and the like.
- Treatment with an immune checkpoint inhibitor includes treatment with a PD-1 inhibitor (such as nivolumab) and treatment with a CTLA-4 inhibitor (such as ipilimumab).
- test method of the present invention uses a sample collected from a subject before cancer treatment as a test target.
- “before cancer treatment” means before cancer treatment whose effect is to be predicted is started. That is, in the "before cancer treatment” of the present invention, before starting a new cancer treatment, before administration of a drug for cancer treatment, before administration of a drug during the continuation of cancer treatment, before changing the drug for cancer treatment, Including the period before the cancer treatment policy is changed and whether or not to stop cancer treatment.
- test method of the present invention uses a sample collected from a subject after cancer treatment as a test target.
- after cancer treatment means a stage in which a specific cancer treatment drug is selected, the effect of the cancer treatment drug is confirmed after a certain period of time after starting the cancer treatment. . That is, “after cancer treatment” of the present invention, before further drug administration during the cancer treatment is continued, before the change of the drug for cancer treatment, before the change of the cancer treatment policy, and the cancer treatment is stopped. Whether or not to consider.
- sample in the screening method of the present invention, a sample collected from a B cell-containing solution cultured by stimulation with a candidate peptide for cancer vaccine is preferable.
- the supernatant of the culture solution after stimulating the mononuclear cell-containing fraction or B cell-containing fraction obtained from human blood with a candidate peptide for cancer vaccine together with CD4 positive T cells and CD8 positive T cells can be used.
- therapeutic effect is a concept including suppression of progression of cancer, reduction of cancer, disappearance of cancer, suppression of recurrence, suppression of metastasis, extension of survival time, and the like. Expressed by response rate, survival rate, survival time, etc.
- the “cancer treatment” cancer in the test method of the present invention is not particularly limited, and may be any cancer. Suitable cancers include XAGE1-positive or NY-ESO-1-positive cancers. Moreover, the cancer of the peptide for cancer vaccines obtained by the screening method of the present invention is not particularly limited and may be any cancer. Suitable cancers include XAGE1-positive cancers. Examples of the cancer in the test method of the present invention and the screening method of the present invention include lung cancer, liver cancer, prostate cancer, gastric cancer, malignant melanoma, breast cancer, esophageal cancer, renal cancer, and bladder cancer. Preferable examples include lung cancer, and particularly non-small cell lung cancer. Furthermore, the test of the present invention is suitable for predicting the effects of intractable advanced stage non-small cell lung cancer treatment and advanced stage lung adenocarcinoma treatment.
- XAGE1 (X Antigen Family, Member 1) is a known cancer testis antigen encoded by the XAGE1 gene and also known as Cancer / Testis antigen 12.1 (CT12.1). So far, five types of genes of XAGE1a-e have been identified, and the related protein is GAGED2, and it is known that there are two types of isoforms, GAGED2a and GAGED2d. To date, four alternative splice variants of XAGE 1a, b, c, d have been identified (Sato (et al., Cancer Immunity, unvol. 7, page 5 (2007)). XAGE1a and XAGE1b encode an XAGE1 (GAGED2a) protein consisting of 81 amino acids, and XAGE1d encodes an XAGE1 (GAGED2d) protein consisting of 69 amino acids.
- the amino acid sequence of XAGE1 is known for various animal species.
- the sequence of human XAGE1 (GAGED2a) is provided as NCBI Reference Sequence: NP_00109101073.2 and NP_00109101063.2
- the sequence of human XAGE1 (GAGED2d) is provided as NCBI Reference Sequence: NP_001091074.
- Human XAGE1 (GAGED2a): (SEQ ID NO: 3) mespkkknqq lkvgilhlgs rqkkiriqlr sqcatwkvic kscisqtpgi nldlgsgvkv kiipkeehck mpeageeqpq v
- the anti-XAGE1 antibody to be measured in the test method or screening method of the present invention is an antibody against XAGE1 (GAGED2a) (hereinafter simply referred to as XAGE1).
- the method for detecting the anti-XAGE1 antibody that is the detection target of the test method or screening method of the present invention is not particularly limited, and examples thereof include a method for detecting binding to an antigen.
- the antigen to be bound may be full-length XAGE1 or a partial peptide consisting of a part of the amino acid sequence. Preferably, full length XAGE1 is used.
- One embodiment of the test method or screening method of the present invention detects an IgG type anti-XAGE1 antibody.
- an IgG type anti-XAGE1 antibody XAGE1-IgG
- an IgA type anti-XAGE1 antibody XAGE1-IgA
- the labeled anti-human IgG antibody can be used.
- the method for detecting an IgA type antibody is not particularly limited.
- a labeled anti-human IgA antibody can be used.
- One embodiment of the test method or screening method of the present invention includes a step of detecting XAGE1-IgG and / or XAGE1-IgA.
- XAGE1-IgG is a biomarker indicating that the immune response against self-tumor is enhanced
- XAGE1-IgA is a biomarker indicating that the immune response against self-tumor is attenuated (suppressed) . It has been found for the first time that such a marker can be applied to predict the therapeutic effect of a cancer therapeutic agent.
- NY-ESO-1 is also one of known cancer testis antigens. It is expressed in various degrees of 5-40% in various tumors including malignant melanoma, but expression is limited only in the testis in normal tissues.
- the NY-ESO-1 protein consists of 180 amino acids and its sequence is provided as GenBank: CAA05908.1.
- Human NY-ESO-1 (SEQ ID NO: 4) mqaegrgtgg stgdadgpgg pgipdgpggn aggpgeagat ggrgprgaga arasgpggga prgphggaas glngccrcga rgpesrllef ylampfatpm eaelarrsla qdapplpvpg vllkeftvsg niltirltaa dhrqlqlsis sclqqlsllm witqcflpvf laqppsgqrr
- the method for detecting the anti-NY-ESO-1 antibody that is a detection target in the test method or screening method of the present invention is not limited, and examples include a method for detecting binding to an antigen.
- the antigen to be bound may be full-length NY-ESO-1 or a partial peptide consisting of a part of the amino acid sequence. Preferably, full length NY-ESO-1 is used.
- an IgG type anti-NY-ESO-1 antibody is detected. Furthermore, an IgA type anti-NY-ESO-1 antibody may be detected.
- the method for detecting an IgG type antibody is not particularly limited. For example, a labeled anti-human IgG antibody can be used.
- the method for detecting an IgA type antibody is not particularly limited. For example, a labeled anti-human IgA antibody can be used.
- MAEL, BAGE, BORIS, MAGE-B3 and SSX4 are also known cancer testis antigens. It is expressed to various degrees in various tumors, but in normal tissues, expression is limited only to the testis.
- p53 is known as a tumor suppressor protein.
- anti-MAEL anti-BAGE antibody
- anti-BORIS antibody anti-MAGE-B3 antibody
- anti-SSX4 antibody anti-p53 antibody
- anti-p53 antibody detection targets in the test method or screening method of the present invention.
- a method for detecting binding is mentioned.
- the antigen to be bound may be a full length or a partial peptide consisting of a partial amino acid sequence.
- IgG type anti-MAEL, anti-BAGE antibody, anti-BORIS antibody, anti-MAGE-B3 antibody, anti-SSX4 antibody and anti-p53 antibody are detected.
- an IgA type antibody may be detected.
- the labeled anti-human IgG antibody can be used.
- the method for detecting an IgA type antibody is not particularly limited.
- a labeled anti-human IgA antibody can be used.
- the method for detecting an antibody against each CT antigen or anti-p53 antibody is not particularly limited as long as it can measure the amount, concentration or antibody titer of the antibody, and can be measured using a technique known in the art. For example, it can be measured by ELISA method, radioimmunoassay, immunoprecipitation method, affinity column method and the like.
- the “subject” in the test method of the present invention is not particularly limited and is widely used in general mammals (human, mouse, rat, monkey, dog, cat, cow, horse, pig, sheep, goat, rabbit, hamster, etc. ), But preferably a human.
- the subject is a human, not only a cancer patient or a patient suspected of having cancer, but also a healthy person can be a subject.
- the sex, age, etc. of the subject are not particularly limited.
- sample in the test method of the present invention include blood (serum, plasma, blood cells, etc.), urine, feces, sputum, chest / ascites, bronchoalveolar lavage fluid, peritoneal lavage fluid, biopsy tissue, and surgical excision. And the like.
- a preferable sample includes serum.
- At least one selected from the group consisting of the following 1) to 4) is determined to be effective for cancer treatment.
- 1) antibody against cancer testis antigen or anti-p53 antibody is positive
- 2) An antibody against an IgG type cancer testis antigen or an anti-p53 antibody is positive
- 3) Antibody against IgG type cancer testis antigen or anti-p53 antibody is positive
- antibody against IgA type cancer testis antigen or anti-p53 antibody is negative
- Antibodies against multiple cancer testis antigens are positive.
- an antibody against a CT antigen or an anti-p53 antibody when an antibody against a CT antigen or an anti-p53 antibody is positive, it is determined that there is an effect of cancer treatment.
- Preferred examples include anti-XAGE1 antibody, anti-NY-ESO-1 antibody, anti-MAEL antibody, anti-BAGE antibody, anti-BORIS antibody, anti-MAGE-B3 antibody, anti-SSX4 antibody, and anti-p53 antibody.
- the antibody against the CT antigen or the anti-p53 antibody is an IgG type antibody.
- Preferable specific examples include XAGE1-IgG or NY-ESO-1-IgG.
- an antibody against an IgG type CT antigen or an anti-p53 antibody when an antibody against an IgG type CT antigen or an anti-p53 antibody is positive and an antibody against an IgA type CT antigen or an anti-p53 antibody is negative, it is determined that there is an effect of cancer treatment. Is done.
- Preferable specific examples include a case where XAGE1-IgG or NY-ESO-1-IgG is positive and XAGE1-IgA is negative.
- XAGE1-IgG is positive, and XAGE1- The case where IgA is negative is mentioned.
- An antibody against CT antigen or anti-p53 antibody is positive when the amount, concentration or antibody titer of the antibody against CT antigen or anti-p53 antibody is greater than or equal to a cutoff value, and negative is an antibody against CT antigen Alternatively, the amount, concentration or antibody titer of the anti-p53 antibody is below the cut-off value.
- the cut-off value may be, for example, an antibody titer 10 to 1000 times that of a healthy person, an antibody titer 20 to 500 times, or an antibody titer 50 to 200 times. It may be 100 times.
- the cut-off value may be set as the average of serum of 50 or more healthy adults + 3SD.
- the amount, concentration or antibody titer of XAGE1-IgG or NY-ESO-1-IgG is equal to or higher than the cutoff value, it is determined that there is an effect of cancer treatment.
- One embodiment of the test method of the present invention includes a step of detecting an antibody against a CT antigen or an anti-p53 antibody in a sample.
- the sample is a sample collected from a subject before cancer treatment.
- antibodies against the CT antigen include anti-XAGE1 antibody and anti-NY-ESO-1 antibody. More preferable specific examples include XAGE1-IgG, a combination of XAGE1-IgG and XAGE1-IgA, a combination of NY-ESO-1-IgG and a combination of NY-ESO-1-IgG and XAGE1-IgA.
- the amount, concentration or antibody titer of XAGE1-IgA in the same sample as the step of detecting the amount, concentration or antibody titer of XAGE1-IgG in a sample collected from a subject is determined. Detecting. The presence of XAGE1-IgA indicates that immunity is suppressed, so that the amount, concentration or antibody titer of XAGE1-IgG is not less than the cutoff value, and XAGE1-IgA is not more than the cutoff value Therefore, it can be determined that there is an effect of cancer treatment.
- XAGE1-IgG is a biomarker indicating that the immune response to self-tumor is enhanced.
- IgA positive regulatory B cells were found to increase in the local cancer area, and XAGE1-IgA becomes a biomarker indicating that the immune response against self-tumor is attenuated.
- XAGE1-IgA reaction is observed in about half of patients having XAGE1-IgG.
- the screening method of the present invention includes, for example, a step of stimulating B cells isolated from human blood with a vaccine candidate peptide and a step of detecting an antibody against CT antigen or anti-p53 antibody in the culture supernatant.
- the method further includes a step of determining that the candidate peptide has an effect of cancer treatment when the antibody against the CT antigen or the anti-p53 antibody is positive.
- the method includes a step of determining that the candidate peptide has an effect of cancer treatment when XAGE1-IgA is negative and XAGE1-IgG or NY-ESO-1-IgG is positive.
- the antibody against the CT antigen to be examined is not particularly limited, but preferably an anti-XAGE1 antibody, an anti-NY-ESO-1 antibody, an anti-MAEL antibody, an anti-BAGE antibody, an anti-BORIS antibody, an anti-MAGE-B3 antibody or an anti-SSX4 antibody including.
- a patient in which antibodies against a plurality of CT antigens are detected has an immune response to multiple antigens and is in an immunostimulated state, and cancer treatment such as immunotherapy is successful.
- the plurality should just be 2 or more, Preferably it is 3 or more.
- limiting in an upper limit, 50 or less, 40 or less, 30 or less, 20 or less, 10 or less etc. are mentioned specifically from the complexity of a test
- an antibody against anti-CT antigen or anti-p53 antibody as an index (by detecting an immune response against CT antigen or p53), preferably by using anti-XAGE1 antibody or anti-NY-ESO-1 antibody as an index
- Anti-XAGE1 antibody or anti-NY-ESO-1 antibody positive clearly distinguishes the effect of anti-PD-1 antibody therapy from known biomarkers. In particular, it has become possible to clearly identify successful cases of immune checkpoint molecule inhibitors. Even if PD-L1 expression was positive, the response rate was 30%, and even if it was negative, the response rate was 10%. Therefore, it is epoch-making that these biomarkers can clearly identify the response rate. .
- a preferred vaccine is a vaccine comprising a CT antigen, more preferably at least one CT antigen selected from the group consisting of XAGE1, NY-ESO-1, MAEL, BAGE, BORIS, MAGE-B3 and SSX4 or these antigens It is a vaccine containing the peptide which consists of one part.
- the invention relating to the reagent kit includes a CT antigen, a peptide comprising a part of a CT antigen, p53, and a carrier on which at least one selected from the group consisting of a peptide comprising a part of p53 is immobilized, an anti-human IgG antibody and a reagent kit for testing a therapeutic effect on cancer comprising a reagent containing an anti-human IgA antibody.
- a preferred embodiment is a carrier in which at least one peptide selected from the group of XAGE1, a peptide comprising a part of XAGE1, NY-ESO-1 and a peptide comprising a part of NY-ESO-1 is immobilized.
- a reagent kit for testing a therapeutic effect on cancer comprising a reagent containing an anti-human IgG antibody and a reagent containing an anti-human IgA antibody. This kit is a reagent kit for examining the effects of cancer treatment.
- the peptide consisting of a part of XAGE1 is a peptide having a sequence consisting of a part of the amino acid sequence represented by SEQ ID NO: 3.
- it is a peptide containing 10 or more amino acids and contains one or more epitopes.
- the peptide consisting of a part of NY-ESO-1 is a peptide having an amino acid sequence consisting of a part of the amino acid sequence represented by SEQ ID NO: 4.
- it is a peptide containing 10 or more amino acids and contains one or more epitopes.
- the carrier on which the peptide contained in the reagent kit of the present invention is solid-phased is selected from the group consisting of CT antigen, peptide consisting of part of CT antigen, p53, and peptide consisting of part of p53. At least one is immobilized. Preferably, at least one selected from the group consisting of XAGE1, a peptide consisting of a part of XAGE1, NY-ESO-1 and a part of NY-ESO-1, is immobilized.
- the carrier is not particularly limited, and examples thereof include a plate and a stick.
- the reagent kit of the present invention includes a reagent containing an anti-human IgG antibody and a reagent containing an anti-human IgA antibody in addition to the carrier on which the peptide is immobilized. These antibodies are preferably labeled.
- the kit of the present invention may contain a reagent for reacting with a label, a diluent, a reagent, and a test instrument.
- the invention relating to the peptide of the present application is at least one peptide selected from the group consisting of the following a) to f).
- a pharmaceutically acceptable salt or solvate of the peptide d) a peptide comprising a part of XAGE1 comprising the amino acid sequence represented by SEQ ID NO: 3, and / or the N-terminal side of the amino acid sequence represented by SEQ ID NO: 2 and / or A peptide having an
- the amino acid sequence of the peptide of the present invention is designed based on the sequences of SEQ ID NO: 1, SEQ ID NO: 2 and SEQ ID NO: 3, and can be synthesized by a usual method.
- the number of amino acids of the peptide is preferably in the range of 20-30.
- the peptide of this invention is a peptide which can be selected by the screening of the said peptide for cancer vaccines.
- one amino acid is substituted with an amino acid having a similar structure or characteristic such that a hydrophobic amino acid is replaced with another hydrophobic amino acid.
- the amino acids are exchanged for identical or similar amino acids in size and chemistry so that leucine is replaced by isoleucine.
- certain amino acid substitutions are often more tolerated than other amino acid substitutions, which are of a size between the original amino acid and its substitution.
- Charge, polarity, and hydrophobicity often show similar correlations, which is the basis for the definition of “conservative substitution”.
- Conservative substitutions may be defined herein as being exchanged for one of the following five groups: Group 1—A low molecular weight aliphatic, nonpolar or slightly polar residue (Ala, Ser, Thr, Pro, Gly); Group 2-polar, negatively charged residues and their amides (Asp, Asn, Glu, Gln); Group 3-polar, positively charged residues (His, Arg, Lys); Group 4 -High molecular weight aliphatic, nonpolar residues (Met, Leu, Ile, Val, Cys); and Group 5-High molecular weight, aromatic residues (Phe, Tyr, Trp).
- Group 1 A low molecular weight aliphatic, nonpolar or slightly polar residue (Ala, Ser, Thr, Pro, Gly); Group 2-polar, negatively charged residues and their amides (Asp, Asn, Glu, Gln); Group 3-polar, positively charged residues (His, Arg, Lys); Group 4 -High molecular weight aliphatic, nonpolar residues
- the C-terminus of the peptide of the present invention may be an amide or ester.
- suitable protecting groups e.g., formyl group, C 1 such as acetyl groups - such as 6 acyl group
- glycopeptides to which sugar chains are bound are also included.
- part of the amino acids may be D amino acids.
- Examples of the salt of the peptide of the present invention include physiologically acceptable acid addition salts and the like.
- the peptide of the present invention may be in the form of a solvate.
- the solvent is not particularly limited as long as it is pharmaceutically acceptable, and examples thereof include water, ethanol, glycerol, acetic acid and the like. It may be a prodrug. Prodrugs can be designed to convert to the peptides of the invention under physiological conditions in vivo.
- the peptide of the present invention can be produced according to a known peptide synthesis method.
- a peptide synthesis method for example, either a solid phase synthesis method or a liquid phase synthesis method may be used. That is, the partial peptide or amino acid that can constitute the peptide of the present invention is condensed with the remaining portion, and when the product has a protective group, the target peptide is produced by removing the protective group if necessary. be able to.
- the number of amino acids to be extended and / or deleted is a maximum of 5, preferably 4, more preferably 3, more preferably 2. More preferably, it is 1. Most preferably 0.
- the number of conservatively substituted amino acids is 2 or 1. More preferably, it is one.
- the number of amino acids to be extended and / or deleted is a maximum of 5, preferably 4, more preferably 3, more preferably 2. More preferably, it is 1. Most preferably 0.
- the number of conservatively substituted amino acids is 2 or 1. More preferably, it is one.
- Preferred peptides of the present invention include at least one peptide selected from the group consisting of the following a1) to f1).
- a1) A peptide comprising a part of XAGE1 consisting of the amino acid sequence shown in SEQ ID NO: 3, and an extension of at most 3 amino acids on the N-terminal side and / or C-terminal side of the amino acid sequence shown in SEQ ID NO: 1 and / or Or a peptide having an amino acid sequence that allows deletion b1) a peptide having an amino acid sequence in which one amino acid in the amino acid sequence of the a1) is conservatively substituted c1) a pharmaceutical of the peptide of the a1) or b1) Pharmaceutically acceptable salt or solvate d1) a peptide comprising a part of XAGE1 consisting of the amino acid sequence shown in SEQ ID NO: 3, and the N-terminal side and / or C-terminal side of the amino acid sequence shown in SEQ ID NO: 2 A peptide having an amino acid
- SLP1 and SLP2 are long peptides having 25 amino acid residues.
- SLP1 has the amino acid sequence shown in SEQ ID NO: 1
- SLP2 has the amino acid sequence shown in SEQ ID NO: 2.
- SLP1 has the 8th to 32nd amino acid sequence of XAGE1 (SEQ ID NO: 3)
- SLP2 has the 44th to 68th amino acid sequence of XAGE1.
- the invention relating to the composition for inducing an immune response against cancer of the present application contains at least one peptide selected from the above a) to c) and at least one peptide selected from the above d) to f). More preferably, it contains at least one peptide selected from a1) to c1) and at least one peptide selected from d1) to f1). More preferably, SLP1 and SLP2 are contained. The combined use of these peptides achieved an effect that could not be achieved alone.
- the invention relating to an effect enhancer of immunotherapy or chemotherapy for cancer of the present application is selected from the group consisting of at least one peptide selected from the group consisting of the above a) to c) and the above d) to f).
- composition for inducing immune response of the present invention and the effect enhancer of the present invention can also be referred to as cancer vaccines.
- composition for inducing an immune response of the present invention is used for inducing an immune response in a mammal (for example, mouse, rat, hamster, rabbit, cat, dog, cow, sheep, monkey, human, etc.).
- a mammal for example, mouse, rat, hamster, rabbit, cat, dog, cow, sheep, monkey, human, etc.
- the composition for inducing immune response of the present invention activates humoral immunity and cellular immunity, enhances immune response against cancer, and can be used for cancer treatment.
- the effect of cancer treatment by chemotherapy, immunotherapy, and immune checkpoint inhibitors can be increased.
- the composition for inducing immune response according to the present invention can be used to treat XAGE1 immunity by actively inducing chemotherapy and immunotherapy, ineffective cases of treatment with an immune checkpoint molecule inhibitor, or a poor prognosis group. Can lead to good response and good prognosis groups.
- the immune response composition of the present invention is also excellent in safety.
- the composition of the present invention can induce an immune response against a cancer expressing XAGE1, can be used for the treatment of the cancer, and can enhance the therapeutic effect of the cancer. .
- XAGE1 immunity can be actively induced in cases where the cancer treatment is ineffective or in a poor prognosis group, leading to a treatment success and good prognosis group.
- the cancer to be treated include lung cancer, liver cancer, prostate cancer, gastric cancer, malignant melanoma, breast cancer, esophageal cancer, renal cancer, or bladder cancer.
- Particularly suitable cancers include lung cancer.
- non-small cell lung cancer and lung adenocarcinoma particularly advanced non-small cell lung cancer and lung adenocarcinoma are suitable for inducing immune responses.
- the composition for inducing immune response of the present invention can induce the production of anti-XAGE1 antibody.
- the production of XAGE1-IgG can be induced. Since XAGE1-IgG positive patients and treatment subjects have good prognosis and therapeutic response, the composition for inducing immune response of the present invention has a poor prognosis even by treatment with chemotherapy, immunotherapy and immune checkpoint inhibitors, Patients who are expected to be ineffective treatment can have a good prognosis and a therapeutic response.
- the present inventors have previously prepared an epitope vaccine containing a part of 16-17 amino acids of XAGE1, but the peptide of the present invention is a long-chain peptide unlike the epitope vaccine recognized by T cells.
- a conventional epitope vaccine comprising an epitope and further using at least one peptide selected from the group consisting of a) to c) and at least one peptide selected from the group consisting of d) to f) A stronger immune response can be induced.
- composition for inducing immune response of the present invention may contain an adjuvant in order to enhance the immune response.
- a pharmacologically acceptable carrier and stabilizer may be included.
- the composition for inducing immune response according to the present invention is produced according to known means generally used in the method for producing pharmaceutical preparations, for example, as an injection, parenterally (intravenous injection, intramuscular injection, etc.). It can be safely administered.
- Examples of the pharmacologically acceptable carrier that may be used in the production of the immune response inducing composition of the present invention include various organic or inorganic carrier substances that are commonly used as pharmaceutical materials.
- excipients in solid formulations include various organic or inorganic carrier substances that are commonly used as pharmaceutical materials.
- excipients in solid formulations include various organic or inorganic carrier substances that are commonly used as pharmaceutical materials.
- excipients in solid formulations include various organic or inorganic carrier substances that are commonly used as pharmaceutical materials.
- Lubricants, binders and disintegrants include various organic or inorganic carrier substances that are commonly used as pharmaceutical materials.
- solvents in liquid preparations include solubilizers, suspending agents, tonicity agents, buffers and soothing agents.
- additives such as conventional preservatives, antioxidants, colorants, sweeteners, adsorbents, wetting agents and the like can be used in appropriate amounts.
- the prepared injection may be a liquid preparation or a solid preparation that dissolves after use.
- the solid preparation in administration, in the case of the solid preparation, it can be dissolved in a conventional aqueous diluent and used as a liquid.
- Aqueous diluents include glucose aqueous solution, physiological saline, Ringer's solution, nutritional supplement solution and the like.
- the content of the peptide of the present invention varies depending on the form of the preparation, but is usually about 0.1 to 100% by weight, preferably about 10 to 99% based on the whole preparation. It is about 9% by weight, more preferably about 20 to 90% by weight.
- the ratio of the content of at least one peptide selected from a) to c) and at least one peptide selected from d) to f) is appropriately adjusted. Examples thereof include 1: 9 to 9: 1, 3: 7 to 7: 3, and 5: 5.
- the dose of the composition for inducing immune response of the present invention varies depending on the route of administration, symptoms, patient age, etc., for example, when administered parenterally such as intravenous administration, as a peptide per kg body weight per day About 0.005 to 50 mg, preferably about 0.05 to 10 mg can be administered.
- the composition for inducing immune response which is one embodiment of the present invention can be administered before administration of other chemotherapy, immunotherapy, immune checkpoint molecule inhibitor.
- the composition for inducing an immune response of the present invention can be administered 1 day to 6 months before administration of these drugs, preferably 1 week to 3 months before, more preferably 2 weeks to 2 months. In a preferred embodiment, it can be administered 28 days to 3 months prior to administration of the immune checkpoint molecule inhibitor.
- the present invention also stimulates CD4 positive T cells or CD8 positive T cells obtained from the peripheral blood of a patient with SLP1 having the amino acid sequence shown by SEQ ID NO: 1 and SLP2 having the amino acid sequence shown by SEQ ID NO: 2.
- a method for preparing activated CD4 positive T cells or activated CD8 positive T cells, comprising a step of culturing.
- CD4-positive T cells or CD8-positive T cells are separated from peripheral blood mononuclear cells, and subjected to stimulation culture in the presence of SLP1 and SLP2 for 3 to 21 days, preferably 7 to 18 days. Thereafter, it can be obtained by restimulation with SLP1 and / or SLP2 together with antigen-presenting cells for 3 to 24 hours, preferably 6 to 18 hours.
- concentrations of SLP1 and SLP2 during stimulation culture are each 0.1 to 10 ⁇ M, preferably 0.1 to 1 ⁇ M.
- the obtained activated CD4-positive T cells and activated CD8-positive T cells can be used for cell therapy. For example, it can be administered to a patient who has provided peripheral blood and used for adoptive immunotherapy.
- the blood used in the examples was provided with informed consent from a patient before cancer treatment.
- XAGE1 protein (81 amino acids, SEQ ID NO: 3) was synthesized by GL Biochem (Shanghai, China). The synthesized XAGE1 protein is purified with an HPLC column, and it is confirmed that the purity is 90% or more.
- XAGE1 carbonate buffer, pH 9.6
- XAGE1 carbonate buffer, pH 9.6
- a washing solution PBS / 0.1% TWEEN
- FCS / PBS 5% FCS / PBS was added and blocking was performed at 37 ° C. for 1 hour.
- serum diluted 100 times, 400 times, 1600 times, and 6400 times was added and reacted at 37 ° C. for 2 hours.
- a peroxidase-conjugated goat anti-human IgG antibody (diluted 5000 times) (manufactured by Jackson) or a peroxidase-conjugated goat anti-human IgA antibody (diluted 8000 times) (manufactured by Jackson) was added, and the mixture was incubated at 37 ° C. The reaction was carried out for 1 hour. After completion of the reaction, the substrate was washed with a washing solution, and a substrate solution (a solution in which orthophenylenediamine was dissolved in 0.05 M citrate buffer (pH 5.0)) was added to cause color development.
- a substrate solution a solution in which orthophenylenediamine was dissolved in 0.05 M citrate buffer (pH 5.0)
- the antibody titer was calculated by a general method for obtaining the antibody titer (Autoantibodies against Cancer Antigen: Sacha Gnjastic, Lloyd J. Old, Yao-Tseng Chen). Both IgG and IgA were positive when the antibody titer was 100 times or more that of normal human control serum, and less than 100 times was negative.
- NY-ESO-1 180 amino acids, SEQ ID NO: 4
- NY-ESO-1-IgG was detected by the same method as that for detecting XAGE1-IgG.
- Each CT antigen or p53 was obtained from Okayama University in a state immobilized on beads (Bioconjugate Chem. 2015, 26, 2076-2084). Each CT antigen or p53 was detected by the same method as the method for detecting the XAGE1 antibody.
- XAGE1-IgG positive persons were 33 cases (22.7%), and XAGE1-IgA immune response was confirmed in about half (15.3%) of them (FIG. 1). This was much more frequent than the immune response to MAGE-A3, SSX-2, NY-ESO-1, TP53 antigens, which are said to be highly immunogenic in lung cancer (IgG response to each antigen: (4.1%, 1.4%, 6.2%, 8.3%, IgA reaction: 0.7%, 0.7%, 0.7%, 4.1%) (FIG. 2). All XAGE1-IgA positive patients were XAGE1-IgG positive.
- XAGE1-IgA immune response attenuated the immune response against self-tumor (XAGE1-IgG positive and XAGE1-IgA positive group). Furthermore, XAGE1-immune negative cases (XAGE1-IgG negative and XAGE1-IgA negative groups) showed almost no immune response against self-tumor. As shown in FIG. 3B, XAGE1-IgG-positive and XAGE1-IgA-negative individuals have an immune response to multiple cancer antigens compared to XAGE1-IgG-positive and XAGE1-IgA-positive subjects and have an immune response against cancer. Potentially high condition (immune activation state).
- XAGE1-IgG positive and XAGE1-IgA positive individuals are more immunoreactive than XAGE1-IgG negative and XAGE1-IgA negative subjects, but immunoreactivity is suppressed more than XAGE1-IgG positive and XAGE1-IgA negative subjects. It is in a state.
- TGF- ⁇ which is an immunosuppressive cytokine
- IL-6 which is a poor prognostic factor and increases during immune exhaustion, is significantly higher in XAGE1-IgG positive and XAGE1-IgA positive compared to XAGE1-IgG positive and XAGE1-IgA negative, Compared to XAGE1-IgG positive and XAGE1-IgA negative persons, XAGE1-IgG positive and XAGE1-IgA positive persons are considered to be immune exhausted.
- FIG. 5 shows that such locally accumulated IgA + B cells themselves produce IL-10, an immunosuppressive cytokine (FIG. 5F).
- IgA + B cells are thought to be involved in local immune suppression and accumulation of regulatory T cells (local IL-10 is involved in accumulation).
- immune checkpoint molecules molecules that suppress T cell function
- PD-L1 + GAL ⁇ that highly expressed immune checkpoint molecules PD-L1 and Galectin-9 were analyzed. It was confirmed that 9 + IgA + B cells were significantly accumulated locally in the cancer (FIG. 6).
- immunosuppressive cytokines (IL-6, IL-10, etc.) are produced in XAGE1-IgG + IgA + patients due to tumor genetic abnormalities, etc. It is considered that IgA + B cells (regulatory B cells) accumulate. IgA + B cells suppress their immunity indirectly by locally accumulating regulatory T cells in addition to their own IL-10 production and direct suppression of T cell functions by immune checkpoint molecules it seems to do.
- the group with no XAGE1 expression for 1 month had a median survival time of 13.6 months, and it was revealed that the XAGE1-IgG positive group significantly prolonged the median survival time.
- the prolongation of the median survival time was remarkable (FIG. 7).
- the XAGE1-IgG positive and XAGE1-IgA negative groups are XAGE1-IgG positive and It was revealed that the response rate of the initial chemotherapy was significantly higher than the XAGE1-IgA positive group and the group without immune response (FIG. 8).
- Anti-PD-1 antibody therapy which is an immune checkpoint molecule inhibitor, using immune response to highly immunogenic XAGE1 and NY-ESO-1 (with or without immune response to XAGE1 or NY-ESO-1) as an index Of 53 patients with advanced stage non-small cell lung cancer.
- Patient sera were collected approximately 28 days before starting anti-PD-1 antibody therapy.
- immune response to XAGE1 (XAGE1-IgG positive) or immune response to NY-ESO-1 (NY-ESO-1-IgG positive) group 16 cases
- No immune response group (no antibody to XAGE1 and NY-ESO-1) Group) 37 cases
- Fig. 9 shows the maximum change rate of the target lesion.
- CR complete response
- PR partial response
- SD stable
- PD pathological progression
- progression-free survival (OverallOverSurvival) and overall survival (Overall Survival) in the group with and without immune response to XAGE1 or NY-ESO-1. Progression-free survival and overall survival were found to be significantly different between groups with and without immune response.
- FIG. 11 shows the results shown in FIG. 3A for the immunity against each cancer antigen in the XAGE1-IgG positive and XAGE1-IgA negative group, the XAGE1-IgG positive and XAGE1-IgA positive group, the XAGE1-IgG negative and the XAGE1-IgA negative group.
- the result of analyzing the reaction is shown.
- FIG. 11 shows, an immune reaction against MAEL antigen and p53 antigen is specifically observed in XAGE1-IgG positive and XAGE1-IgA negative persons. Therefore, those who are positive for anti-MAEL antibody and those who are positive for anti-p53 antibody are XAGE1-IgG positive and XAGE1-IgA negative, and are immunostimulated.
- FIG. 12 is a successful example of anti-PD-1 antibody therapy, and anti-NY-ESO-1 antibody, anti-XAGE1 antibody and anti-p53 antibody were monitored. As a result, in the successful cases, an enhanced immune response to the p53 antigen was observed, and the fluctuation of the anti-p53 antibody is useful for determining the therapeutic effect of the anti-PD-1 antibody therapy.
- ⁇ Anti-NY-ESO-1 antibody, anti-BAGE antibody and anti-BORIS antibody> The immune response to 50 cancer antigens including XAGE1 and NY-ESO-1 antibodies was analyzed using the serum before treatment of patients treated with anti-PD-1 antibody therapy.
- XAGE1-IgG and NY-ESO-1-IgG positive individuals have an immune response against multiple antigens as shown in FIG. Further, as shown in FIG. 13B, in 3 cases out of 8 cases that succeeded in anti-PD-1 antibody, the immune response to BAGE antigen or BORIS antigen was significantly positive (0 out of 12 cases in non-response cases)
- the effect of anti-PD-1 therapy can be predicted by detection of anti-BAGE antibody or anti-BORIS antibody.
- FIG. 14A shows the relationship between the rate of change of target lesions due to anti-PD-1 antibody therapy (minus means tumor shrinkage) and the antibody titers of antibodies against CT antigen (XAGE1-IgG and NY-ESO-1-IgG).
- FIG. 14B shows the relationship between the rate of change of target lesions by anti-PD-1 antibody therapy and the number of immune responses (antigen spreading) to multiple antigens after treatment.
- the effects of anti-PD-1 therapy can be predicted by detecting antibodies against multiple CT antigens.
- FIG. 15A shows the difference in immune response to multiple antigens before and after anti-PD-1 antibody therapy.
- FIG. 15B shows that in the successful case of the anti-PD-1 antibody therapy, spreading of the immune response against the MAGE-B3 antigen and the SSX4 antigen was frequently observed and not in the non-successful case. Therefore, anti-MAGE-B3 antibody, actually anti-SSX4 antibody, is a factor that significantly affects the effect of anti-PD-1 antibody therapy, and is useful for predicting therapeutic effects.
- FIG. 16 and FIG. 17 are complete successful cases of clinical trials led by anti-CCR4 antibody + anti-PD-1 antibody, preoperative combination doctors, and show the images and immune responses of the same patients.
- FIG. 16 shows that an immune response to the SSX4 antigen was observed.
- the image in FIG. 17 is a chest CT image, and the baseline images are CT images after administration of the study drug and before surgery for 3 weeks and 7 weeks before administration of anti-CCR4 antibody + anti-PD-1 antibody.
- Anti-CCR4 antibody was administered 4 times before surgery, anti-PD-1 antibody was administered 3 times before surgery, and surgery was performed at 8 weeks.
- the CT image shows that the tumor is shrinking due to immunotherapy. This patient is an example of positive anti-SSX4 antibody, and immunotherapy was effective.
- measurement of anti-SSX4 antibody is useful as a method for predicting the effect of immunotherapy.
- Example 2 ⁇ Synthesis of XAGE1 long chain peptide and preparation of composition for inducing immune response (vaccine)>
- SLP1 is a peptide consisting of positions 8-32 of XAGE1 (a protein consisting of 81 amino acids)
- SLP2 is a peptide consisting of positions 44-68. It has been confirmed that the purity of each of SLP1 and SLP2 is 99% or more.
- SLP1 amino acid sequence SEQ ID NO: 1: NQQLKVGILHLGSRQKKIRIQLRSQ SLP2 amino acid sequence (SEQ ID NO: 2): ISQTPGINLDLGSGVKVKIIPKEEH SLP1 and SLP2 obtained above were mixed to obtain a composition for inducing immune response (vaccine).
- XAGE1 antibody positive patients XAGE1-IgG positive and XAGE1-IgA negative patients
- a magnetic cell separation method manufactured by Militenny Biotech
- CD4 positive T cells 1 ⁇ 10 6 and 40 Gy irradiated CD4 negative CD8 negative cells 1 ⁇ 10 6 in 96 ⁇ l U bottom culture plate with 200 ⁇ l of AIM culture medium containing 2% serum (including IL-2 and IL-7) SLP1 and SLP2 were each stimulated for 14 days in the presence of 1 ⁇ M.
- 200 ⁇ l of AIM culture medium containing 2% serum (including IL-2 and IL-7) was used unless otherwise specified.
- T-APC cells In order to use as antigen-presenting cells, a part of patient CD4-positive T cells obtained in a was stimulated with PHA to prepare T-APC cells.
- T-APC 1 ⁇ 10 4 (30 ⁇ l) prepared as antigen-presenting cells was collected from the 96-well plate after 14 days of stimulation culture with b1 above in a new 96-well plate for 30 ⁇ l each for SLP1 and SLP2 restimulation and non-stimulation. ) was added to each well. Furthermore, SLP1 and SLP2 were added to SLP1 and SLP2 restimulation wells so that each amount was 1 ⁇ M and restimulated for 12 hours.
- IFN ⁇ in the 96-well culture supernatant was detected by ELISA.
- the IFN ⁇ activity of the culture supernatant stimulated with SLP1 and SLP2 is compared with that of the unstimulated culture supernatant, and antigen-specific T cells exist in wells with strong activity. Cloned.
- the cloned cells were screened again by the method b3 to b5, and SLP1 or SLP2-specific CD4 positive T cell clones (hereinafter also referred to as CD4 clones) were selected to obtain a plurality of T cell clones.
- the obtained clone T cells were proliferated by PHA stimulation and cryopreserved.
- One of the CD4 clones obtained is 4C34-1.
- CD8 clones SLP1 or SLP2 specific CD8 positive T cell clones (hereinafter also referred to as CD8 clones) were prepared in the same manner as b above. One of the resulting CD8 clones is 8C34TY.
- T cells 2 ⁇ 10 4 of CD4 clone or CD8 clone were stimulated and cultured with the same number of T-APC for 12 hours so that each peptide was 1 ⁇ M, and IFN ⁇ in the supernatant was detected by ELISA.
- the results are shown in FIG.
- the CD4 clone 4C34-1 recognized amino acids 52-68 among SLP2 (44-68).
- CD8 clone 8C34TY recognizes SLP1 (8-32) and amino acids at positions 19-33, and an epitope is considered to exist in this.
- SLP1 and SLP2 succeeded in detecting a plurality of CD4 T cells and CD8 T cells that recognize SLP1 and SLP2 by stimulating and culturing peripheral blood mononuclear cells of anti-XAGE1 antibody-positive patients. This indicates that SLP1 and SLP2 vaccines are multi-antigenic cancer vaccines containing various epitopes, unlike epitope vaccines recognized by T cells.
- CD4 clone (4C34-1) T cells 1 ⁇ 10 4 were stimulated with SLP1 alone (1 ⁇ M), SLP2 alone (1 ⁇ M) or a combination of each peptide (1 ⁇ M each) together with the same number of T-APCs.
- CD4 clone T cells recognized SLP2.
- CD8 clone (8C34TY) T cells 1 ⁇ 10 4 were stimulated and cultured with SLP1 alone (1 ⁇ M), SLP2 alone (1 ⁇ M), or each peptide combination (1 ⁇ M each) together with the same number of T-APCs.
- CD8 clone T cells recognized SLP1.
- Peripheral blood mononuclear cells 1 ⁇ 10 5 obtained in (a) above were present (500-fold dilution) in the presence of CD4 clone 4C34-1T cells 2 ⁇ 10 4 , CD8 clone C34TYT cells 2 ⁇ 10 4 and Protein Transport Inhibitor Cocktail (eBioscienc, USA).
- SLP1 alone (1 ⁇ M), SLP2 alone (1 ⁇ M), or each peptide combination (1 ⁇ M each) was stimulated for 12 hours.
- B cells were gated by flow cytometry, and IgG or IgA on the surface of B cells was detected under the stimulation of each peptide (FIG. 21). Increased expression of IgG on the surface of B cells was observed when SLP1 and SLP2 were used in combination. On the other hand, there was no change in the expression level of IgA.
- XAGE1-specific antibody present in the culture supernatant When an XAGE1-specific antibody present in the culture supernatant was detected, XAGE1-IgG was detected when SLP1 and SLP2 were used in combination, and IgA was not observed (FIG. 22).
- the composition containing SLP1 and SLP2 is a cancer vaccine that can induce the production of XAGE1-IgG and induce an immune response against cancer. Since XAGE1-IgG positivity is a treatment success group and a good prognosis group, the composition containing SLP1 and SLP2 can lead a patient to a treatment success and a good prognosis.
- the dosage of the test substance was 2 mg / kg (SLP1: 0.2 mg / kg + SLP2: 0.2 mg / kg) and 2 mg / kg (SLP1: 2 mg / kg + SLP2: 2 mg / kg).
- SLP1 and SLP2 dissolved in water for injection and picibanil were mixed with an equal amount of oil adjuvant MONTANIDE ISA 51 VG (ISA51) to form an emulsion and administered subcutaneously in the back at a dose volume of 1 mL / kg.
- ISA51 oil adjuvant MONTANIDE ISA 51 VG
- a vehicle control group for administering water for injection and an emulsion of picibanil and ISA51 and a physiological saline control group for administering physiological saline were provided.
- SLP1 and SLP2 were emulsified with Montanide (ISA51, manufactured by SEPPIC) together with adjuvant OK432 picibanil to obtain a composition for inducing immune response (hereinafter also referred to as XAGE1 vaccine). More specifically, a mixed peptide consisting of two kinds of long-chain peptides prepared in GMP grade was prepared in three stages.
- the test was conducted on the advanced stage or postoperative recurrent lung adenocarcinoma using the above three doses of XAGE1 vaccine. Each time the XAGE1 vaccine was administered to two different sites on the limb. Administration was performed 4 times at intervals of 2 weeks. Three doses were administered for each dose.
- Adverse events are graded using the Common Terminology Criteria for Adverse Events (CTCAE) v4.0 Japanese translation JCOG version. Adverse events were determined according to CTCAE v4.0. The observation period for adverse events was from the first day of study drug administration to 6 weeks after the last administration (end of individual study).
- CTCAE Common Terminology Criteria for Adverse Events
- the safety evaluation was completed in 7 cases, 3 cases in the low dose group, 3 cases in the medium dose group, and 1 case in the high dose group. As shown in Table 1, all adverse events caused by XAGE1 vaccine were minor and no serious adverse events were observed.
- XAGE1-IgG antibody titer was increased by administration of XAGE1 vaccine, and XAGE1-IgA and NY-ESO-1-IgG were not induced (FIG. 23).
- XAGE1-IgA was positive (KMX-01) in 1 of 7 cases before treatment, but negative in the other cases.
- the XAGE1 vaccine did not increase the XAGE1-IgA antibody titer. From the above, the specific induction of XAGE1-IgG immunity by SLP1 and SLP2 observed in vitro was also observed in vivo.
- Tumor Marker As shown in FIG. 24, inhibition or decrease in tumor marker elevation was observed in 4 of 7 cases. a. In 2 out of 3 cases of the XAGE1 vaccine low-dose group, inhibition of tumor marker elevation was observed. b. A decrease in tumor marker was observed in 2 out of 3 patients in the XAGE1 vaccine medium dose group. c. In 3 of 4 cases in which the XAGE1-IgG antibody titer increased, tumor marker elevation was suppressed or decreased. On the other hand, an increase in tumor marker was observed in 2 out of 3 cases in which no increase in XAGE1-IgG antibody titer was observed. From the above, it was observed that tumor marker elevation was suppressed or decreased by the XAGE1 vaccine.
- CD4-positive T cells were isolated from the peripheral blood of low-dose and medium-dose patients and examined for induction of antigen-specific T cells by XAGE1 vaccine administration. In both low-dose and medium-dose patients, it was demonstrated that IFN- ⁇ was produced by the combined stimulation of SLP1 and SLP2, and T cells reactive to SLP1 and SLP2 antigens were induced ( FIG. 25, FIG. 26).
- the XAGE1 vaccine containing SLP1 and SLP2 is a vaccine that can induce antigen-specific T cells in cancer patients, and is also a multi-antigenic vaccine containing multiple epitopes, and mixes SLP1 and SLP2. Thus, it was proved in vivo that the vaccine can induce a stronger immune response.
- the experimental protocol is as follows. a) A mononuclear cell fraction was obtained from peripheral blood 12 weeks after the start of vaccine administration by specific gravity centrifugation. Subsequently, using an anti-CD4 antibody-bound bead, an anti-CD8 antibody-bound bead, and an anti-CD19 antibody-bound bead (manufactured by Miltenyi Biotech), a CD8 positive fraction is sequentially obtained by magnetic cell separation (MACS, Miltenyi Biotech). CD4 positive fraction, CD19 positive fraction and CD4 ⁇ CD8 ⁇ CD19 ⁇ fraction were separated.
- Detection of IFN- ⁇ producing cells The cell population containing antigen-specific T cells proliferated in the stimulation culture was subjected to secondary stimulation as described below to detect production of antigen-specific cytokines.
- the same number of autologous EBV-B cells (Epstein-Barr virus-infected B cells: used as antigen-presenting cells) and peptides (SLP1, SLP2 or SLP1 + SLP2) are added to the cells after stimulation culture at 37 ° C. Secondary stimulation was performed in a CO 2 incubator for 4 hours. As a control, secondary stimulation was performed in a CO 2 incubator at 37 ° C. for 4 hours without adding a peptide.
- the cultured cells are suspended in 10 ml of AIM-V medium, and a rotator (Maxmix, manufactured by Millitney Biotech). ) And suspended in a CO 2 incubator at 37 ° C. for 45 minutes.
- the detection method of the present invention can predict the effect of cancer treatment and expands the possibility of cancer treatment. It also contributes to the medical economy.
- the composition for inducing immune response according to the present invention can be directly used for cancer treatment, enhances the effect of treatment with chemotherapy, immunotherapy, immune checkpoint inhibitor, and treats treatment invalidity effectively. Can lead to.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Engineering & Computer Science (AREA)
- Immunology (AREA)
- General Health & Medical Sciences (AREA)
- Biomedical Technology (AREA)
- Medicinal Chemistry (AREA)
- Molecular Biology (AREA)
- Hematology (AREA)
- Microbiology (AREA)
- Organic Chemistry (AREA)
- Biochemistry (AREA)
- Urology & Nephrology (AREA)
- Biotechnology (AREA)
- Pharmacology & Pharmacy (AREA)
- Veterinary Medicine (AREA)
- Public Health (AREA)
- Animal Behavior & Ethology (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Cell Biology (AREA)
- Genetics & Genomics (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- General Physics & Mathematics (AREA)
- Pathology (AREA)
- Analytical Chemistry (AREA)
- Physics & Mathematics (AREA)
- Food Science & Technology (AREA)
- Epidemiology (AREA)
- Oncology (AREA)
- Zoology (AREA)
- Wood Science & Technology (AREA)
- Mycology (AREA)
- Biophysics (AREA)
- Gastroenterology & Hepatology (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- General Chemical & Material Sciences (AREA)
- General Engineering & Computer Science (AREA)
- Medicines Containing Antibodies Or Antigens For Use As Internal Diagnostic Agents (AREA)
Abstract
Description
2.前記がん精巣抗原が、XAGE1、NY-ESO-1、MAEL、BAGE、BORIS、MAGE-B3及びSSX4からなる群から選択される少なくとも1つのがん精巣抗原である、前項1に記載の方法。
3.IgGタイプの抗体とIgAタイプの抗体を検出する、前項1または2に記載の検査方法。
4.前記試料ががん治療前の被験体から採取された試料であり、該がん治療の効果を予測するための検査である、前項1~3のいずれか1に記載方法。
5.試料中の抗p53抗体を検出することを特徴とする、がん治療効果の検査方法。
6.以下の1)~4)からなる群から選択される少なくとも1の場合に、がん治療の効果があると判定される、前項1~5のいずれか一に記載の方法;
1)がん精巣抗原に対する抗体若しくは抗p53抗体が陽性である、
2)IgGタイプのがん精巣抗原に対する抗体若しくは抗p53抗体が陽性である、
3)IgGタイプのがん精巣抗原に対する抗体若しくは抗p53抗体が陽性であり、IgAタイプのがん精巣抗原に対する抗体若しくは抗p53抗体が陰性である、
4)複数のがん精巣抗原に対する抗体が陽性である。
7.がん精巣抗原、がん精巣抗原の一部からなるペプチド、p53、及びp53の一部からなるペプチドからなる群から選択される少なくとも1が固相化された担体、抗ヒトIgG抗体を含有する試薬、及び抗ヒトIgA抗体を含有する試薬を含むがん治療効果検査用の試薬キット。
8.以下のa)~f)からなる群から選択される少なくとも1つのペプチド;
a)配列番号3に示されるアミノ酸配列からなるXAGE1の一部からなるペプチドであり、配列番号1に示されるアミノ酸配列のN末側及び/又はC末側に最大5個のアミノ酸の伸長及び/又は欠失を許容するアミノ酸配列を有するペプチド
b)前記a)のペプチドのアミノ酸配列中の1個又は2個のアミノ酸が保存的置換されたアミノ酸配列を有するペプチド
c)前記a)又はb)のペプチドの薬学的に認容可能な塩若しくは溶媒和物
d)配列番号3に示されるアミノ酸配列からなるXAGE1の一部からなるペプチドであり、配列番号2に示されるアミノ酸配列のN末側及び/又はC末側に最大5個のアミノ酸の伸長及び/又は欠失を許容するアミノ酸配列を有するペプチド
e)前記d)のペプチドのアミノ酸配列中の1個又は2個のアミノ酸が保存的置換されたアミノ酸配列を有するペプチド
f)前記d)又はe)のペプチドの薬学的に認容可能な塩若しくは溶媒和物。
9.前項8に記載のa)~c)からなる群から選択される少なくとも1つのペプチドと前項8に記載のd)~f)からなる群から選択される少なくとも1つのペプチドを含有するがんに対する免疫応答誘導用組成物。
10.前記がんが、XAGE1陽性の肺癌、肝癌、前立腺癌、胃癌、悪性黒色腫、乳癌、食道癌、腎癌、又は、膀胱癌である前項9に記載の組成物。
11.免疫療法前又は化学療法前に投与される、前項9または10に記載の組成物。
12.前項8に記載のa)~c)からなる群から選択される少なくとも1つのペプチドと前項8に記載のd)~f)からなる群から選択される少なくとも1つのペプチドを含有するがんに対する免疫療法若しくは化学療法の効果増強剤。
13.試料中のがん精巣抗原に対する抗体若しくは抗p53抗体を検出することを特徴とする、がんワクチン用ペプチドのスクリーニング方法。
14.前記試料が、がんワクチン用候補ペプチドによって刺激培養されたB細胞含有液から採取された試料である、前項13に記載の方法。
15.末梢血から得られたCD4陽性T細胞又はCD8陽性T細胞を、配列番号1に示されるアミノ酸配列を有するSLP1及び配列番号2に示されるアミノ酸配列を有するSLP2で刺激培養する工程を含む、活性化CD4陽性T細胞又は活性化CD8陽性T細胞の調製方法。
16.前項8に記載のa)~c)から選択される少なくとも1つのペプチドと前項8に記載のd)~f)から選択される少なくとも1つのペプチドによる、免疫応答を誘導する方法。
17.免疫療法または化学療法を開始する前に、前項8に記載のa)~c)から選択される少なくとも1つのペプチドと前項8に記載のd)~f)から選択される少なくとも1つのペプチドを投与することによる、該免疫療法または該化学療法の効果を増大する方法。
18.請求項1に記載の検査方法により、がん治療の効果があると判定されなかった場合に、抗体価を上昇させて、免疫療法を有効症例に導く方法。
本発明の検査方法の一実施形態は、がん治療後の被験体から採取された試料を検査対象とする。本明細書において「がん治療後」とは、特定のがん治療薬を選定し、がん治療を開始後、一定期間を経て、当該がん治療薬の効果を確認する段階という意味である。すなわち、本発明の「がん治療後」には、がん治療の継続中におけるさらなる薬剤投与前、がん治療用薬剤の変更前、がん治療方針の変更前、及びがん治療を中止するか否かの検討段階を含む。
ヒトXAGE1(GAGED2a):(配列番号3)
mespkkknqq lkvgilhlgs rqkkiriqlr sqcatwkvic kscisqtpgi nldlgsgvkv kiipkeehck mpeageeqpq v
ヒトNY-ESO-1:(配列番号4)
mqaegrgtgg stgdadgpgg pgipdgpggn aggpgeagat ggrgprgaga arasgpggga
prgphggaas glngccrcga rgpesrllef ylampfatpm eaelarrsla qdapplpvpg
vllkeftvsg niltirltaa dhrqlqlsis sclqqlsllm witqcflpvf laqppsgqrr
1)がん精巣抗原に対する抗体若しくは抗p53抗体が陽性である、
2)IgGタイプのがん精巣抗原に対する抗体若しくは抗p53抗体が陽性である、
3)IgGタイプのがん精巣抗原に対する抗体若しくは抗p53抗体が陽性であり、IgAタイプのがん精巣抗原に対する抗体若しくは抗p53抗体が陰性である、
4)複数のがん精巣抗原に対する抗体が陽性である。
a)配列番号3に示されるアミノ酸配列からなるXAGE1の一部からなるペプチドであり、配列番号1に示されるアミノ酸配列のN末側及び/又はC末側に最大5個のアミノ酸の伸長及び/又は欠失を許容するアミノ酸配列を有するペプチド
b)前記a)のペプチドのアミノ酸配列中の1個又は2個のアミノ酸が保存的置換されたアミノ酸配列を有するペプチド
c)前記a)又はb)のペプチドの薬学的に認容可能な塩若しくは溶媒和物
d)配列番号3に示されるアミノ酸配列からなるXAGE1の一部からなるペプチドであり、配列番号2に示されるアミノ酸配列のN末側及び/又はC末側に最大5個のアミノ酸の伸長及び/又は欠失を許容するアミノ酸配列を有するペプチド
e)前記d)のペプチドのアミノ酸配列中の1個又は2個のアミノ酸が保存的置換されたアミノ酸配列を有するペプチド
f)前記d)又はe)のペプチドの薬学的に認容可能な塩若しくは溶媒和物
a1)配列番号3に示されるアミノ酸配列からなるXAGE1の一部からなるペプチドであり、配列番号1に示されるアミノ酸配列のN末側及び/又はC末側に最大3個のアミノ酸の伸長及び/又は欠失を許容するアミノ酸配列を有するペプチド
b1)前記a1)のペプチドのアミノ酸配列中の1個のアミノ酸が保存的置換されたアミノ酸配列を有するペプチド
c1)前記a1)又はb1)のペプチドの薬学的に認容可能な塩若しくは溶媒和物
d1)配列番号3に示されるアミノ酸配列からなるXAGE1の一部からなるペプチドであり、配列番号2に示されるアミノ酸配列のN末側及び/又はC末側に最大3個のアミノ酸の伸長及び/又は欠失を許容するアミノ酸配列を有するペプチド
e1)前記d)のペプチドのアミノ酸配列中の1個のアミノ酸が保存的置換されたアミノ酸配列を有するペプチド
f1)前記d)又はe)のペプチドの薬学的に認容可能な塩若しくは溶媒和物
SLP1:(配列番号1)NQQLKVGILHLGSRQKKIRIQLRSQ
SLP2:(配列番号2)ISQTPGINLDLGSGVKVKIIPKEEH
SLP1はXAGE1(配列番号3)の8番目から32番目のアミノ酸配列を有し、SLP2は、XAGE1の44番目から68番目のアミノ酸配列を有する。
<XAGE1-IgG及びXAGE1-IgAの検出>
XAGE1タンパク質(81個のアミノ酸、配列番号3)は、GLバイオケム社(上海、中国)で合成されたものを使用した。合成したXAGE1タンパク質は、HPLCカラムで精製を行い、純度が90%以上であることを確認している。
NY-ESO-1(180個のアミノ酸、配列番号4)は、通常の方法により大腸菌を用いて作成した。NY-ESO-1-IgGは上記XAGE1-IgGの検出方法と同様の方法で検出した。
各CT抗原若しくはp53は、ビーズに固定化された状態で岡山大学より入手した(Bioconjugate Chem. 2015, 26, 2076-2084)。各CT抗原若しくはp53は、上記XAGE1抗体の検出方法と同様の方法で検出した。
<XAGE1-IgG及び XAGE1-IgA反応>
145例の進行期(cStageIIIB-IV)の肺腺癌患者から採取した血清について、がん抗原、XAGE1、MAGE-A3、SSX-2、NY-ESO-1及びTP53に対する特異的IgG及びIgAを検査した。
MAGE-A3は、ATgen社(韓国)より入手し、SSX-2は、ATgen社(韓国)より入手し、TP53は、RayBiotech(アメリカ)より入手した。NY-ESO-1(180個のアミノ酸、配列番号4)は、通常の方法により大腸菌を用いて作成した。それぞれの抗原に対する特異的IgG及びIgAの検出は、上記XAGE1-IgG及びXAGE1-IgAの検出方法と同様の方法で検出した。
<サロゲートマーカーとしてのXAGE1-IgG、XAGE1-IgA反応>
XAGE1抗原が陽性の55例の肺腺癌患者から得られた血清について51種類のがん抗原への自己抗体反応を検査した結果(図3A)、XAGE1-IgG陽性かつXAGE1-IgA陰性群には、種々のがん抗原に対する免疫応答が観察され、XAGE1-IgG及びXAGE1-IgAが自己腫瘍に対する免疫応答のサロゲートマーカーになっていることが明らかになった。一方でXAGE1-IgA免疫応答の出現は、自己腫瘍に対する免疫応答が減弱していた(XAGE1-IgG陽性かつXAGE1-IgA陽性群)。さらに、XAGE1免疫陰性例(XAGE1-IgG陰性かつXAGE1-IgA陰性群)は、自己腫瘍に対する免疫応答はほとんど観察されなかった。
図3Bで示すように、XAGE1-IgG陽性かつXAGE1-IgA陰性者は、XAGE1-IgG陽性かつXAGE1-IgA陽性者に比べ、複数のがん抗原に免疫反応を有し、がんに対する免疫応答が潜在的に高い状態(免疫活性化状態)である。一方、XAGE1-IgG陽性かつXAGE1-IgA陽性者は、XAGE1-IgG陰性かつXAGE1-IgA陰性者より免疫活性が高い状態であるが、XAGE1-IgG陽性かつXAGE1-IgA陰性者より免疫活性が抑制されている状態である。
<XAGE1免疫による化学療法の奏効率及び予後予測>
進行期肺腺癌145例の検討で、XAGE1-IgG、XAGE1-IgA、免疫応答なし、XAGE1発現なしを指標として生存曲線を解析した結果、XAGE1-IgG陽性かつXAGE1-IgA陰性群は、中央生存期間33.8ヶ月、XAGE1-IgG陽性かつXAGE1-IgA陽性群は、中央生存期間19.7ヶ月、免疫応答なし群(XAGE1-IgG陰性かつXAGE1-IgA陰性群)は、中央生存期間11.9ヶ月、XAGE1発現無し群は、中央生存期間13.6ヶ月であり、XAGE1-IgG陽性群が有意に中央生存期間を延長することが明らかになった。特に、XAGE1-IgG陽性かつXAGE1-IgA陰性群は中央生存期間の延長が顕著であった(図7)。
<免疫チェックポイント分子阻害薬の奏功例に対するバイオマーカーとしてのXAGE1及びNY-ESO-1免疫>
高免疫原性のXAGE1及びNY-ESO-1に対する免疫応答(XAGE1若しくはNY-ESO-1に対する免疫応答あり、免疫応答なし)を指標として、免疫チェックポイント分子阻害薬である抗PD-1抗体療法の効果について、53例の進行期非小細胞肺癌患者で検討した。患者の血清は抗PD-1抗体療法を始める概ね28日前に採血した。
XAGE1に対する免疫応答あり(XAGE1-IgG陽性)又はNY-ESO-1に対する免疫応答あり(NY-ESO-1-IgG陽性)群:16例
免疫応答なし群(XAGE1及びNY-ESO-1に対する抗体なし群):37例
現在の指針では、免疫チェックポイント阻害薬は、EGFR遺伝子変異、EML-4/ALK融合遺伝子異常といったドライバー遺伝子変異を有する肺癌では、免疫療法の効果が少ないということで免疫療法は慎重に適応を決めるよう(控えるよう)に通達が来ている。しかしながら、EGFR遺伝子変異1名、EML-4/ALK融合遺伝子異常1名のXAGE1-IgG陽性かつXAGE1-IgA陰性の患者2名に免疫療法(免疫チェックポイント分子阻害薬である抗PD-1抗体療法)を施行した結果、EGFR遺伝子変異1名はSD、EML-4/ALK融合遺伝子異常1名は著効にて90%以上腫瘍が縮小した。現在の指針では見逃してしまう免疫療法(免疫チェックポイント分子阻害薬である抗PD-1抗体療法)著効症例を、XAGE1-IgGとXAGE1-IgAを指標とすることで、見逃すことなく治療することができる。
抗PD-1抗体療法を実施した患者の治療前の血清を用いて、XAGE1およびNY-ESO-1抗体を含むがん抗原50種に対する免疫応答を解析した。XAGE1-IgGおよびNY-ESO-1-IgG陽性者は図13Aで示すように多抗原に対する免疫応答を有し免疫活性化状態である。また、図13Bで示すように、抗PD-1抗体に奏功した8例中3例で、BAGE抗原または、BORIS抗原に対する免疫反応が有意に陽性であり(非奏功例12例中0例)、抗BAGE抗体または、抗BORIS抗体の検出により抗PD-1療法の効果を予測し得る。
図14Aは、抗PD-1抗体療法による標的病変の変化率(マイナスは腫瘍縮小を意味する)とCT抗原に対する抗体(XAGE1-IgG及びNY-ESO-1-IgG)の抗体価との関係を示している。図14Bは、抗PD-1抗体療法による標的病変の変化率と治療後の多抗原に対する免疫反応の増強(抗原スプレディング)数との関係を示している。CT抗原に対する抗体価が高いほど抗PD-1療法の腫瘍の縮小率が高く、また様々なCT抗原に対する免疫反応の数が多い(抗原スプレディングが多い)ほど、抗PD-1療法の腫瘍の縮小率が高いことが明かになった。よって、複数のCT抗原に対する抗体を検出することにより、抗PD-1療法の効果を予測し得る。
図15Aは、抗PD-1抗体療法の前後における多抗原に対する免疫応答の差を示す。図15Bは、抗PD-1抗体療法の奏功例では、MAGE-B3抗原 及びSSX4抗原に対する免疫応答のスプレディングが高頻度に認められ、非奏功例には認められなかったことを示す。よって、抗MAGE-B3抗体、実際に抗SSX4抗体は、抗PD-1抗体療法の効果に重大な影響を及ぼす因子であり、治療効果予測に有用である。
<XAGE1長鎖ペプチドの合成及び免疫応答誘導用組成物(ワクチン)の作製>
XAGE1の部分ペプチドである25アミノ酸残基を有する長鎖ペプチドSLP1及びSLP2を通常の方法でGMPグレードで株式会社ペプチド研究所にて合成した。SLP1は、XAGE1(81アミノ酸からなるタンパク質)の8位-32位からなるペプチドであり、SLP2は、44位-68位からなるペプチドである。SLP1及びSLP2の各々の純度は99%以上であることを確認している。
SLP1アミノ酸配列(配列番号1):NQQLKVGILHLGSRQKKIRIQLRSQ
SLP2アミノ酸配列(配列番号2):ISQTPGINLDLGSGVKVKIIPKEEH
上記で得られたSLP1及びSLP2を混合し、免疫応答誘導用組成物(ワクチン)を得た。
a.細胞の分離
XAGE1抗体陽性患者(XAGE1-IgG陽性かつXAGE1-IgA陰性患者)の末梢血から比重遠心法によって単核球を得た。次いで、抗CD4抗体結合ビーズ及び抗CD8抗体結合ビーズ(ミリテニーバイオテク社製)を用いて、磁気細胞分離法(MACS、ミリテニーバイオテク社製)によって、順次CD8陽性細胞、CD4陽性細胞、及びCD4陰性CD8陰性細胞を分離した。
b1.CD4陽性T細胞1x106と40Gyの放射線照射済みのCD4陰性CD8陰性細胞1x106を、96穴Uボトムカルチャープレートで、2%血清入りAIM培養メディウム200μl(IL-2、IL-7を含む)で、SLP1及びSLP2各々1μM存在下で14日間刺激培養した。
以下の実験における培養においても、特に記載の無い限り、2%血清入りAIM培養メディウム200μl(IL-2、IL-7を含む)を用いた。
SLP1若しくはSLP2特異的CD8陽性T細胞クローン(以下、CD8クローンともいう)を上記bと同様に調製した。得られたCD8クローンの1つが8C34TYである。
上記bで得られたCD4クローン4C34-1、及び上記cで得れたCD8クローン8C34TYについて解析した。
XAGE1のアミノ酸配列の一部からなる20のペプチドを合成した。各々のアミノ酸配列は配列番号5~24に示す。また、各ペプチドのXAGE1のアミノ酸配列上の位置については、配列表と図19に示すとおりである。ペプチド合成は通常の合成法によりPHジャパン(日本)において合成した。純度は各々95%以上である。
CD4クローン若しくはCD8クローンのT細胞2x104を、同数のT-APCと共に、各々のペプチドが1μMになるように12時間刺激培養し、上清のIFNγをELISA法にて検出した。
結果を図19に示す。CD4クローンである4C34-1はSLP2(44-68)の中でも、52-68位のアミノ酸を認識していた。また、CD8クローンである8C34TYはSLP1(8-32)と19-33位のアミノ酸を認識し、この中にエピトープが存在すると考えられる。
CD4クローン(4C34-1)T細胞1x104を、同数のT-APCと共に、SLP1単独(1μM)、SLP2単独(1μM)、又は各のペプチド併用(各1μM)で12時間刺激培養し、上清のIFNγをELISA法にて検出した(図20)。CD4クローンのT細胞はSLP2を認識した。
同様にCD8クローン(8C34TY)T細胞1x104を、同数のT-APCと共に、SLP1単独(1μM)、SLP2単独(1μM)、又は各のペプチド併用(各1μM)で12時間刺激培養し、上清のIFNγをELISA法にて検出した(図20)。CD8クローンのT細胞はSLP1を認識していた。
ヒトの末梢血には、CD4陽性T細胞のみ、CD8陽性T細胞のみ存在するということはないので、SLP1単独、SLP2単独ではなく、SLP1とSLP2の併用がより強い免疫応答を誘導することが可能である。
上記aで得られた末梢血単核球1x105を、CD4クローン4C34-1T細胞2x104、CD8クローンC34TYT細胞2x104及びProtein Transport Inhibitor Cocktail(eBioscienc社、アメリカ)存在下(500倍希釈)で、SLP1単独(1μM)、SLP2単独(1μM)、又は各ペプチド併用(各1μM)で12時間刺激培養した。
フローサイトメトリー法にてB細胞にゲートし、それぞれのペプチド刺激下でのB細胞表面上のIgG若しくはIgAを検出した(図21)。B細胞表面上のIgGは、SLP1及びSLP2を併用することで発現の上昇を認めた。一方でIgAの発現量には変化はなかった。
SLP1およびSLP2の混合物をアジュバントとともにSprague-Dawley系ラット(Crl:CD(SD)、投与開始時6週齢、1群雌雄各10匹)の背部皮下に10週間反復投与(14日おきに5回間歇投与)し、毒性試験を行った。
被験物質投与に起因する死亡はみられず、いずれの検査においても被験物質投与による変化はみられなかった。
SLP1およびSLP2をアジュバントOK432ピシバニールと共にモンタナイド(ISA51、SEPPIC製)でエマルジョン化して、免疫応答誘導用組成物を得た(以下、XAGE1ワクチンともいう)。より具体的には、GMPグレードで作成した二種の長鎖ペプチドからなる混合ペプチドを3段階の用量で用意した。
低用量:500μg(SLP1:250μg+SLP2:250μg)
中用量:1mg(SLP1:500μg+SLP2:500μg)
高用量:2mg(SLP1:1mg+SLP2:1mg)
これら混合ペプチドをOK432(中外製薬)0.2KEと共に1.25mlの生食に混和し、モンタナイド1.25mlによりエマルジョン化した。
上記XAGE1ワクチンを進行期肺腺がん患者に対して投与した。本試験は、主目的として安全性を確認し、副次目的として試験薬の投与に伴うXAGE1抗体価の変動を検討する第I相臨床試験である。本臨床試験は、「ヘルシンキ宣言」、「人を対象とする医学系研究に関する倫理指針」およびXAGE1ワクチン臨床試験実施計画書に則り実施したが、ICH E6(R1)-GCP(Guideline for Good Clinical Practice)に可能な限り準拠した。

1.XAGE1-IgGの誘導
XAGE1ワクチンの投与により、7例中4例でXAGE1-IgG抗体価の上昇を認め、XAGE1-IgAおよびNY-ESO-1-IgGは誘導されなかった(図23)。
a.XAGE1ワクチン低用量群3例中2例でXAGE1-IgG抗体価の上昇を認めた。
b.XAGE1ワクチン中用量群3例中2例でXAGE1-IgG抗体価の上昇を認めた。
c.XAGE1-IgAは治療前より7例中1例で陽性(KMX-01)であったが、その他は陰性であった。XAGE1ワクチンによって、XAGE1-IgA抗体価の上昇は認められなかった。
以上より、in vitroで観察された、SLP1およびSLP2によるXAGE1-IgG免疫の特異的な誘導が、in vivoでも観察された。
図24で示すように、腫瘍マーカーの上昇抑制または低下が、7例中4例で観察された。
a.XAGE1ワクチン低用量群3例中2例で腫瘍マーカーの上昇抑制を認めた。
b.XAGE1ワクチン中用量群3例中2例で腫瘍マーカーの低下を認めた。
c.XAGE1-IgG抗体価が上昇した4例中3例で、腫瘍マーカーの上昇抑制もしくは低下が認められた。一方、XAGE1-IgG抗体価の上昇が認められなかった3例中2例で腫瘍マーカーの上昇が観察された。
以上より、XAGE1ワクチンによって腫瘍マーカーの上昇抑制もしくは低下が観察された。
低用量投与の患者及び中用量投与の患者の末梢血よりCD4陽性T細胞を分離し、XAGE1ワクチン投与による抗原特異的T細胞の誘導について調べた。低用量投与の患者及び中用量投与の患者とも、SLP1とSLP2の併用刺激により、IFN-γが産生され、SLP1抗原及びSLP2抗原に反応性のT細胞が誘導されていることが証明された(図25、図26)。
a)ワクチン投与開始後12週目の末梢血から比重遠心法によって単核球分画を得た。次いで、抗CD4抗体結合ビーズ、抗CD8抗体結合ビーズおよび抗CD19抗体結合ビーズ(ミリテニーバイオテク社製)を用いて、磁気細胞分離法(MACS、ミリテニーバイオテク社製)によって、順次CD8陽性分画、CD4陽性分画、CD19陽性分画およびCD4-CD8-CD19-分画を分離した.
刺激培養で増殖した抗原特異的なT細胞が含まれる細胞集団に、以下のように二次刺激を行い、抗原特異的なサイトカインの産生を検出した。
刺激培養した後の細胞に、これと同数の自己のEBV-B細胞(エプスタイン・バール・ウイルス感染B細胞:抗原提示細胞として利用)及び、ペプチド(SLP1、SLP2若しくはSLP1+SLP2)を加え、37℃で4時間、CO2インキュベーター内で二次刺激を行った。コントロールは、ペプチドを加えずに、37℃で4時間、CO2インキュベーター内で二次刺激を行った。
染色後、FACS buffer(1%FCS/PBS,0.02%アジ化ナトリウム)を加えて細胞を洗浄し、FACS Calibur(BD社製)を用いてフローサイトメトリーを行い、IFN-γ産生細胞を検出した。IFN-γ産生細胞の頻度は、データ解析ソフト(FlowJo,Tree Star社製)を用いて解析した。結果を図25及び図26に示す。
Claims (15)
- 試料中のがん精巣抗原に対する抗体を検出することを特徴とする、がん治療効果の検査方法。
- 前記がん精巣抗原が、XAGE1、NY-ESO-1、MAEL、BAGE、BORIS、MAGE-B3及びSSX4からなる群から選択される少なくとも1つのがん精巣抗原である、請求項1に記載の方法。
- IgGタイプの抗体とIgAタイプの抗体を検出する、請求項1または2に記載の検査方法。
- 前記試料ががん治療前の被験体から採取された試料であり、該がん治療の効果を予測するための検査である、請求項1~3のいずれか1に記載方法。
- 試料中の抗p53抗体を検出することを特徴とする、がん治療効果の検査方法。
- 以下の1)~4)からなる群から選択される少なくとも1の場合に、がん治療の効果があると判定される、請求項1~5のいずれか一に記載の方法;
1)がん精巣抗原に対する抗体若しくは抗p53抗体が陽性である、
2)IgGタイプのがん精巣抗原に対する抗体若しくは抗p53抗体が陽性である、
3)IgGタイプのがん精巣抗原に対する抗体若しくは抗p53抗体が陽性であり、IgAタイプのがん精巣抗原に対する抗体若しくは抗p53抗体が陰性である、
4)複数のがん精巣抗原に対する抗体が陽性である。 - がん精巣抗原、がん精巣抗原の一部からなるペプチド、p53、及びp53の一部からなるペプチドからなる群から選択される少なくとも1が固相化された担体、抗ヒトIgG抗体を含有する試薬、及び抗ヒトIgA抗体を含有する試薬を含むがん治療効果検査用の試薬キット。
- 以下のa)~f)からなる群から選択される少なくとも1つのペプチド;
a)配列番号3に示されるアミノ酸配列からなるXAGE1の一部からなるペプチドであり、配列番号1に示されるアミノ酸配列のN末側及び/又はC末側に最大5個のアミノ酸の伸長及び/又は欠失を許容するアミノ酸配列を有するペプチド
b)前記a)のペプチドのアミノ酸配列中の1個又は2個のアミノ酸が保存的置換されたアミノ酸配列を有するペプチド
c)前記a)又はb)のペプチドの薬学的に認容可能な塩若しくは溶媒和物
d)配列番号3に示されるアミノ酸配列からなるXAGE1の一部からなるペプチドであり、配列番号2に示されるアミノ酸配列のN末側及び/又はC末側に最大5個のアミノ酸の伸長及び/又は欠失を許容するアミノ酸配列を有するペプチド
e)前記d)のペプチドのアミノ酸配列中の1個又は2個のアミノ酸が保存的置換されたアミノ酸配列を有するペプチド
f)前記d)又はe)のペプチドの薬学的に認容可能な塩若しくは溶媒和物。 - 請求項8に記載のa)~c)からなる群から選択される少なくとも1つのペプチドと請求項8に記載のd)~f)からなる群から選択される少なくとも1つのペプチドを含有するがんに対する免疫応答誘導用組成物。
- 前記がんが、XAGE1陽性の肺癌、肝癌、前立腺癌、胃癌、悪性黒色腫、乳癌、食道癌、腎癌、又は、膀胱癌である請求項9に記載の組成物。
- 免疫療法前又は化学療法前に投与される、請求項9または10に記載の組成物。
- 請求項8に記載のa)~c)からなる群から選択される少なくとも1つのペプチドと請求項8に記載のd)~f)からなる群から選択される少なくとも1つのペプチドを含有するがんに対する免疫療法若しくは化学療法の効果増強剤。
- 試料中のがん精巣抗原に対する抗体若しくは抗p53抗体を検出することを特徴とする、がんワクチン用ペプチドのスクリーニング方法。
- 前記試料が、がんワクチン用候補ペプチドによって刺激培養されたB細胞含有液から採取された試料である、請求項13に記載の方法。
- 末梢血から得られたCD4陽性T細胞又はCD8陽性T細胞を、配列番号1に示されるアミノ酸配列を有するSLP1及び配列番号2に示されるアミノ酸配列を有するSLP2で刺激培養する工程を含む、活性化CD4陽性T細胞又は活性化CD8陽性T細胞の調製方法。
Priority Applications (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP18797663.4A EP3640641B1 (en) | 2017-05-11 | 2018-05-10 | Method for examining therapeutic effect on cancer and composition for inducing immune response |
| JP2019517688A JP7216420B2 (ja) | 2017-05-11 | 2018-05-10 | がん治療効果の検査方法及び免疫応答誘導用組成物 |
| CN201880028524.8A CN110582701A (zh) | 2017-05-11 | 2018-05-10 | 检查癌症治疗效果的方法和用于诱导免疫应答的组合物 |
| US16/611,947 US11709165B2 (en) | 2017-05-11 | 2018-05-10 | Examination method for prediction of effect of treatment of cancer based on detection of cancer/testis antibodies |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2017-094986 | 2017-05-11 | ||
| JP2017094986 | 2017-05-11 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2018207866A1 true WO2018207866A1 (ja) | 2018-11-15 |
Family
ID=64105321
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2018/018083 Ceased WO2018207866A1 (ja) | 2017-05-11 | 2018-05-10 | がん治療効果の検査方法及び免疫応答誘導用組成物 |
Country Status (5)
| Country | Link |
|---|---|
| US (1) | US11709165B2 (ja) |
| EP (1) | EP3640641B1 (ja) |
| JP (1) | JP7216420B2 (ja) |
| CN (1) | CN110582701A (ja) |
| WO (1) | WO2018207866A1 (ja) |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN110687281A (zh) * | 2019-08-26 | 2020-01-14 | 中国医学科学院肿瘤医院 | Pd-l1自身抗体在肿瘤预后评估中的应用 |
| CN110687282A (zh) * | 2019-08-26 | 2020-01-14 | 中国医学科学院肿瘤医院 | PD-1和/或p53自身抗体作为肿瘤疗效预测或预后评估的标志物 |
| JP2024541350A (ja) * | 2021-11-11 | 2024-11-08 | オムニシーク, インコーポレイテッド | がん精巣抗原負荷を分析及び利用するための方法及びシステム |
| WO2026060295A1 (en) * | 2024-09-12 | 2026-03-19 | Omniseq, Inc. | Cancer testis antigen burden (ctab) as a biomarker of tumor-associated antigens |
Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPS579108B2 (ja) | 1977-09-10 | 1982-02-19 | ||
| WO2013147233A1 (ja) * | 2012-03-30 | 2013-10-03 | 国立大学法人岡山大学 | 抗体検出用試薬の製造方法、及びその用途 |
| JP5709108B2 (ja) * | 2009-05-22 | 2015-04-30 | 国立大学法人 岡山大学 | XAGE−1b特異的免疫反応を誘導するペプチドおよびその利用 |
| WO2016181912A1 (ja) | 2015-05-08 | 2016-11-17 | 学校法人 川崎学園 | 免疫因子を指標とした肺腺癌の予後演算式作成方法と予後推定方法 |
Family Cites Families (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPS579108U (ja) | 1980-06-14 | 1982-01-18 | ||
| WO2005000870A2 (en) * | 2003-05-30 | 2005-01-06 | Ludwig Institute Of Cancer Research | Isolated ny-eso-1 peptides which bind to hla class ii molecules and uses thereof |
| WO2013169971A1 (en) * | 2012-05-10 | 2013-11-14 | Bristol-Myers Squibb Company | Anti-tumor antibodies as predictive or prognostic biomarkers of efficacy and survival in ipilimumab-treated patients |
| RU2522231C1 (ru) * | 2012-11-14 | 2014-07-10 | Евгений Иосифович Гоуфман | Способ диагностики онкологических заболеваний и иммуноферментный набор для его осуществления |
| WO2015172843A1 (en) * | 2014-05-16 | 2015-11-19 | Biontech Diagnostics Gmbh | Methods and kits for the diagnosis of cancer |
-
2018
- 2018-05-10 CN CN201880028524.8A patent/CN110582701A/zh active Pending
- 2018-05-10 US US16/611,947 patent/US11709165B2/en active Active
- 2018-05-10 JP JP2019517688A patent/JP7216420B2/ja active Active
- 2018-05-10 EP EP18797663.4A patent/EP3640641B1/en active Active
- 2018-05-10 WO PCT/JP2018/018083 patent/WO2018207866A1/ja not_active Ceased
Patent Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPS579108B2 (ja) | 1977-09-10 | 1982-02-19 | ||
| JP5709108B2 (ja) * | 2009-05-22 | 2015-04-30 | 国立大学法人 岡山大学 | XAGE−1b特異的免疫反応を誘導するペプチドおよびその利用 |
| WO2013147233A1 (ja) * | 2012-03-30 | 2013-10-03 | 国立大学法人岡山大学 | 抗体検出用試薬の製造方法、及びその用途 |
| WO2016181912A1 (ja) | 2015-05-08 | 2016-11-17 | 学校法人 川崎学園 | 免疫因子を指標とした肺腺癌の予後演算式作成方法と予後推定方法 |
Non-Patent Citations (12)
| Title |
|---|
| "GenBank", Database accession no. CAA05908.1 |
| BEETON-KEMPEN, N. ET AL.: "Development of a novel, quantitative protein microarray platform for the multiplexed serological analyasis of autoantibodies to cancer-testis antigens", INT J CANCER, vol. 135, 2014, pages 1842 - 1851, XP055562611 * |
| BIOCONJUGATE CHEM., vol. 26, 2015, pages 2076 - 2084 |
| HOFMANN 0 ET AL., PROC NATL ACAD SCI USA, vol. 105, no. 51, 23 December 2008 (2008-12-23), pages 20422 - 7 |
| OHUE Y ET AL., CANCER IMMUNOL RES., vol. 4, no. 12, 2016, pages 1049 - 1060 |
| OHUE Y ET AL., CLIN CANCER RES., vol. 20, no. 19, 2014, pages 5052 - 5063 |
| OHUE, Y. ET AL.: "Prolongation of overall survival in advanced lung adenocarcinoma patients with the XAGE1 (GAGED2a) antibody", CLIN CANCER RES, vol. 20, no. 19, 1 October 2014 (2014-10-01), pages 5052 - 5063, XP055562608 * |
| SACHA GNJATICLLOYD J. OLDYAO-TSENG CHEN, AUTOANTIBODIES AGAINST CANCER ANTIGENS |
| SATO ET AL., CANCER IMMUNITY, vol. 7, 2007, pages 5 |
| See also references of EP3640641A4 |
| SHIMADA, HIDEAKI: "Development and Clinical Significance of Serum p53 Antibodies", MODERN MEDIA, vol. 54, no. 8, 2008, pages 233 - 237, XP055645948 * |
| WANG C ET AL., NAT COMMUN., vol. 7, 27 January 2016 (2016-01-27), pages 10499 |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN110687281A (zh) * | 2019-08-26 | 2020-01-14 | 中国医学科学院肿瘤医院 | Pd-l1自身抗体在肿瘤预后评估中的应用 |
| CN110687282A (zh) * | 2019-08-26 | 2020-01-14 | 中国医学科学院肿瘤医院 | PD-1和/或p53自身抗体作为肿瘤疗效预测或预后评估的标志物 |
| JP2024541350A (ja) * | 2021-11-11 | 2024-11-08 | オムニシーク, インコーポレイテッド | がん精巣抗原負荷を分析及び利用するための方法及びシステム |
| WO2026060295A1 (en) * | 2024-09-12 | 2026-03-19 | Omniseq, Inc. | Cancer testis antigen burden (ctab) as a biomarker of tumor-associated antigens |
Also Published As
| Publication number | Publication date |
|---|---|
| EP3640641A4 (en) | 2021-04-07 |
| US20210148927A1 (en) | 2021-05-20 |
| US11709165B2 (en) | 2023-07-25 |
| CN110582701A (zh) | 2019-12-17 |
| EP3640641A1 (en) | 2020-04-22 |
| JPWO2018207866A1 (ja) | 2020-05-28 |
| JP7216420B2 (ja) | 2023-02-01 |
| EP3640641B1 (en) | 2025-07-09 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| AU2020213294B2 (en) | Novel peptides and combination of peptides for use in immunotherapy against hepatocellular carcinoma (hcc) and other cancers | |
| US11033613B2 (en) | Methods and compositions for treating cancer | |
| US9404925B2 (en) | Cancer antigen and use thereof | |
| JP2020014460A (ja) | 数種の血液腫瘍、特に慢性リンパ性白血病(cll)に対する新規免疫療法 | |
| JP2018519825A (ja) | 食道がんおよびその他のがんに対する免疫療法において使用するための新規ペプチドおよびペプチドの組み合わせ | |
| JP7216420B2 (ja) | がん治療効果の検査方法及び免疫応答誘導用組成物 | |
| US11559573B2 (en) | Method of eliciting a CD8+ cytotoxic response in hepatocellular carcinoma patients with a population of activated T cells | |
| KR102215578B1 (ko) | 인간 백혈구 항원에 특이적으로 결합하는 펩타이드 및 이의 용도 | |
| US20240408197A1 (en) | Methods and compositions for treating cancer | |
| KR20220010712A (ko) | Wt1-양성 암을 치료하기 위한 다가 면역요법 조성물 및 사용 방법 | |
| US20220313817A1 (en) | Methods and compositions for treating cancer | |
| HK40028447A (en) | Novel peptides and combination of peptides for use in immunotherapy against hepatocellular carcinoma (hcc) and other cancers | |
| HK40016906A (en) | Novel peptides and combination of peptides for use in immunotherapy against hepatocellular carcinoma (hcc) and other cancers | |
| JP2003500072A (ja) | 癌関連薬剤およびその使用 | |
| NZ791721A (en) | Novel peptides and scaffolds for use in immunotherapy against head and neck squamous cell carcinoma and other cancers |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 18797663 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 2019517688 Country of ref document: JP Kind code of ref document: A |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2018797663 Country of ref document: EP Effective date: 20191211 |
|
| WWG | Wipo information: grant in national office |
Ref document number: 2018797663 Country of ref document: EP |