WO2020092404A1 - Bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies - Google Patents
Bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies Download PDFInfo
- Publication number
- WO2020092404A1 WO2020092404A1 PCT/US2019/058616 US2019058616W WO2020092404A1 WO 2020092404 A1 WO2020092404 A1 WO 2020092404A1 US 2019058616 W US2019058616 W US 2019058616W WO 2020092404 A1 WO2020092404 A1 WO 2020092404A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- expression
- signature
- gene
- patient
- hematologic malignancy
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
- A61P35/02—Antineoplastic agents specific for leukemia
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P31/00—Antiinfectives, i.e. antibiotics, antiseptics, chemotherapeutics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2803—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily
- C07K16/2809—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily against the T-cell receptor (TcR)-CD3 complex
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2866—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against receptors for cytokines, lymphokines, interferons
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/68—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving nucleic acids
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/68—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving nucleic acids
- C12Q1/6876—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes
- C12Q1/6883—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for diseases caused by alterations of genetic material
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/68—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving nucleic acids
- C12Q1/6876—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes
- C12Q1/6883—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for diseases caused by alterations of genetic material
- C12Q1/6886—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for diseases caused by alterations of genetic material for cancer
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/20—Immunoglobulins specific features characterized by taxonomic origin
- C07K2317/24—Immunoglobulins specific features characterized by taxonomic origin containing regions, domains or residues from different species, e.g. chimeric, humanized or veneered
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/30—Immunoglobulins specific features characterized by aspects of specificity or valency
- C07K2317/31—Immunoglobulins specific features characterized by aspects of specificity or valency multispecific
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/60—Immunoglobulins specific features characterized by non-natural combinations of immunoglobulin fragments
- C07K2317/62—Immunoglobulins specific features characterized by non-natural combinations of immunoglobulin fragments comprising only variable region components
- C07K2317/626—Diabody or triabody
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/106—Pharmacogenomics, i.e. genetic variability in individual responses to drugs and drug metabolism
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/158—Expression markers
Definitions
- the present invention is directed to a method of treating a hematologic malignancy such as acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS), including hematologic malignancies that are refractive to chemotherapeutic and/or hypomethylating agents.
- AML acute myeloid leukemia
- MDS myelodysplastic syndrome
- the method concerns administering a CD123 x CD3 bispecific binding molecule to a patient in an amount effective to stimulate the killing of cells of said hematologic malignancy in said patient.
- the present invention is additionally directed to the embodiment of such method in which a cellular sample from the patient evidences an expression of one or more target genes that is increased relative to a baseline level of expression of such genes, for example, a baseline level of expression of such genes in a reference population of individuals who are suffering from the hematologic malignancy, or with respect to the level of expression of a reference gene.
- CD123 (interleukin 3 receptor alpha, IL-3Ra) is a 40 kDa molecule and is part of the interleukin 3 receptor complex (Stomski, F.C. et al. (1996)“ Human Interleukin-3 (IL-3) Induces Disulfide-Linked IL-3 Receptor Alpha- And Beta-Chain Heterodimerization, Which Is Required For Receptor Activation But Not High-Affinity Binding ,” Mol. Cell. Biol. l6(6):3035-3046).
- Interleukin 3 (IL-3) drives early differentiation of multipotent stem cells into cells of the erythroid, myeloid and lymphoid progenitors.
- CD123 is expressed on CD34+ committed progenitors (Taussig, D C. et al. (2005)“ Hematopoietic Stem Cells Express Multiple Myeloid Markers: Implications For The Origin And Targeted Therapy Of Acute Myeloid Leukemia ,” Blood 106:4086-4092), but not by CD34+/CD38- normal hematopoietic stem cells.
- CD123 is expressed by basophils, mast cells, plasmacytoid dendritic cells, some expression by monocytes, macrophages and eosinophils, and low or no expression by neutrophils and megakaryocytes.
- Some non-hematopoietic tissues (placenta, Leydig cells of the testis, certain brain cell elements and some endothelial cells) express CD123; however, expression is mostly cytoplasmic.
- CD123 is reported to be expressed by leukemic blasts and leukemia stem cells (LSC) (Jordan, C.T. et al. (2000)“ The Interleukin-3 Receptor Alpha Chain Is A Unique Marker For Human Acute Myelogenous Leukemia Stem Cells,” Leukemia 14: 1777-1784; Jin, W. etal. (2009)“ Regulation OfThl7 Cell Differentiation And EAE Induction By MAP3K NIK,” Blood 113:6603-6610). In human normal precursor populations, CD123 is expressed by a subset of hematopoietic progenitor cells (HPC) but not by normal hematopoietic stem cells (HSC).
- HPC hematopoietic progenitor cells
- HSC normal hematopoietic stem cells
- CD123 is also expressed by plasmacytoid dendritic cells (pDC) and basophils, and, to a lesser extent, monocytes and eosinophils (Lopez, A.F. et al. (1989)“Reciprocal Inhibition Of Binding Between Interleukin 3 And Granulocyte -Macrophage Colony-Stimulating Factor To Human Eosinophils,” Proc. Natl. Acad. Sci. (U.S.A.) 86:7022-7026; Sun, Q. et al.
- pDC plasmacytoid dendritic cells
- basophils and, to a lesser extent, monocytes and eosinophils
- CD123 has been reported to be overexpressed on malignant cells in a wide range of hematologic malignancies including acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS) (Munoz, L. et al. (2001)“Interleukin- 3 Receptor Alpha Chain (CD123) Is Widely Expressed In Hematologic Malignancies ,” Haematologica 86(12): 1261-1269). Overexpression of CD123 is associated with poorer prognosis in AML (Tettamanti, M.S. et al.
- CD3 is a T cell co-receptor composed of four distinct chains (Wucherpfennig, K.W. et al. (2010)“ Structural Biology Of The T-Cell Receptor: Insights Into Receptor Assembly, Ligand Recognition, And Initiation Of Signaling ,” Cold Spring Harb. Perspect. Biol. 2(4):a005l40; pages 1-14).
- the complex contains a CD3y chain, a CD35 chain, and two CD3e chains. These chains associate with a molecule known as the T cell receptor (TCR) in order to generate an activation signal in T lymphocytes.
- TCR T cell receptor
- TCRs do not assemble properly and are degraded (Thomas, S. et al.
- CD3 is found bound to the membranes of all mature T cells, and in virtually no other cell type (see, Janeway, C.A. et al. (2005) In: IMMUNOBIOLOGY: THE IMMUNE SYSTEM IN HEALTH AND DISEASE,” 6th Ed., Garland Science Publishing, NY, pp. 214- 216; Sun, Z. J. et al.
- AML Acute myeloid leukemia
- MDS myelodysplastic syndrome
- LSCs leukemic stem cells
- CD123 expression a normal hematopoietic stem cell population in normal human bone marrow
- CD123 is expressed in 45%-95% of AML, 85% of Hairy cell leukemia (HCL), and 40% of acute B lymphoblastic leukemia (B-ALL).
- CD123 expression is also associated with multiple other malignancies/pre-malignancies: chronic myeloid leukemia (CML) progenitor cells (including blast crisis CML); Hodgkin’s Reed Sternberg (RS) cells; transformed non-Hodgkin’s lymphoma (NHL); some chronic lymphocytic leukemia (CLL) (CD1 lc+); a subset of acute T lymphoblastic leukemia (T-ALL) (16%, most immature, mostly adult), plasmacytoid dendritic cell (pDC) DC2 malignancies and CD34+/CD38- myelodysplastic syndrome (MDS) marrow cell malignancies.
- CML chronic myeloid leukemia
- RS Reed Sternberg
- NDL transformed non-Hodgkin’s lymphoma
- CLL chronic lymphocytic leukemia
- T-ALL acute T lymphoblastic leukemia
- pDC plasmacytoid dendritic cell
- MDS myelody
- AML is a clonal disease characterized by the proliferation and accumulation of transformed myeloid progenitor cells in the bone marrow, which ultimately leads to hematopoietic failure.
- the incidence of AML increases with age, and older patients typically have worse treatment outcomes than younger patients (Robak, T. et al. (2009) “Current And Emerging Therapies For Acute Myeloid Leukemia,” Clin. Ther. 2:2349- 2370).
- Unfortunately at present, most adults with AML die from their disease.
- Treatment for AML initially focuses in the induction of remission (induction therapy). Once remission is achieved, treatment shifts to focus on securing such remission (post-remission or consolidation therapy) and, in some instances, maintenance therapy.
- the standard remission induction paradigm for AML is chemotherapy with an anthracycline/cytarabine combination, followed by either consolidation chemotherapy (usually with higher doses of the same drugs as were used during the induction period) or human stem cell transplantation, depending on the patient’s ability to tolerate intensive treatment and the likelihood of cure with chemotherapy alone (see, e.g., Roboz, G.J. (2012)“ Current Treatment Of Acute Myeloid Leukemia ,” Curr. Opin. Oncol. 24:711-719).
- Agents frequently used in induction therapy include cytarabine and the anthracy clines.
- Cytarabine also known as AraC
- AraC kills cancer cells (and other rapidly dividing normal cells) by interfering with DNA synthesis.
- Side effects associated with AraC treatment include decreased resistance to infection, a result of decreased white blood cell production; bleeding, as a result of decreased platelet production; and anemia, due to a potential reduction in red blood cells. Other side effects include nausea and vomiting.
- Anthracy clines e.g, daunorubicin, doxorubicin, and idarubicin
- have several modes of action including inhibition of DNA and RNA synthesis, disruption of higher order structures of DNA, and production of cell damaging free oxygen radicals.
- the most consequential adverse effect of anthracyclines is cardiotoxicity, which considerably limits administered life-time dose and to some extent their usefulness.
- non-monospecific molecules e.g. bispecific antibodies, bispecific diabodies, BiTE® antibodies, etc
- Bispecific molecules provide a significant advantage over monospecific molecules such as natural antibodies: the capacity to co-ligate and co localize cells that express different epitopes.
- Bispecific molecules thus have wide- ranging applications including therapy and immunodiagnosis.
- Bispecificity allows for great flexibility in the design and engineering of the diabody in various applications, providing enhanced avidity to multimeric antigens, the cross-linking of differing antigens, and directed targeting to specific cell types relying on the presence of both target antigens.
- effector cells such as cytotoxic T cells
- tumor cells Staerz et al. (1985) “Hybrid Antibodies Can Target Sites For Attack By T Cells,” Nature 314:628-631, and Holliger et al. (1996)“Specific Killing Of Lymphoma Cells By Cytotoxic T-Cells Mediated By A Bispecific Diabody, Protein Eng. 9:299-305).
- Alternative formats use linker peptides to fuse a binding protein (e.g, an scFv, VL, VH, etc.) to a dimerization domain, such as the CH2-CH3 Domain, or to alternative polypeptides (WO 2005/070966, WO 2006/107786 WO 2006/107617, WO 2007/046893) and other formats in which the CL and CH1 Domains are switched from their respective natural positions and/or the VL and VH Domains have been diversified (WO 2008/027236; WO 2010/108127) to allow them to bind to more than one antigen.
- a binding protein e.g, an scFv, VL, VH, etc.
- dimerization domain such as the CH2-CH3 Domain
- alternative polypeptides WO 2005/070966, WO 2006/107786 WO 2006/107617, WO 2007/046893
- other formats in which the CL and CH1 Domains are switched from their respective natural positions and/or the VL and VH Domain
- Such diabodies incorporate one or more cysteine residues into each of the employed polypeptide species.
- cysteine residues for example, the addition of a cysteine residue to the C-terminus of such constructs has been shown to allow disulfide bonding between the polypeptide chains, stabilizing the resulting heterodimer without interfering with the binding characteristics of the bivalent molecule.
- trivalent molecules comprising a diabody-like domain have been described (see, e.g. , WO 2015/184203; and WO 2015/184207).
- Diabody epitope binding domains may also be directed to a surface determinant of any immune effector cell such as CD3, CD16, CD32, or CD64, which are expressed on T lymphocytes, natural killer (NK) cells or other mononuclear cells.
- diabody binding to effector cell determinants e.g. , Fey receptors (FcyR) was also found to activate the effector cell (Holliger et al. (1996)“Specific Killing Of Lymphoma Cells By Cytotoxic T-Cells Mediated By A Bispecific Diabody,” Protein Eng. 9:299-305; Holliger et al.
- effector cell activation is triggered by the binding of an antigen-bound antibody to an effector cell via Fc-FcyR interaction; thus, in this regard, diabody molecules may exhibit Ig-like functionality independent of whether they comprise an Fc Domain (e.g ., as assayed in any effector function assay known in the art or exemplified herein (e.g., ADCC assay)).
- Fc Domain e.g ., as assayed in any effector function assay known in the art or exemplified herein (e.g., ADCC assay)
- the diabody By cross-linking tumor and effector cells, the diabody not only brings the effector cell within the proximity of the tumor cell, but leads to effective tumor killing (see e.g, Cao etal. (2003)“Bispecific Antibody Conjugates In Therapeutics,” Adv. Drug. Deliv. Rev. 55: 171-197).
- the present invention is directed to a method of treating a hematologic malignancy such as acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS), including hematologic malignancies that are refractive to chemotherapeutic and/or hypomethylating agents.
- AML acute myeloid leukemia
- MDS myelodysplastic syndrome
- the method concerns administering a CD123 x CD3 bispecific binding molecule to a patient in an amount effective to stimulate the killing of cells of the hematologic malignancy in the patient.
- the present invention is additionally directed to the embodiment of such method in which a cellular sample from the patient evidences an expression of one or more target genes that is increased relative to a baseline level of expression of such genes, for example, a baseline level of expression of such genes in a reference population of individuals who are suffering from the hematologic malignancy, or with respect to the level of expression of a reference gene.
- the invention provides a method of treating a chemo-refractory hematologic malignancy in a patient, wherein the method comprises administering to the patient a treatment dosage of a CD123 x CD3 bispecific molecule, the dosage being effective to stimulate the killing of cells of the hematologic malignancy in the patient and thereby treat such malignancy.
- the invention further provides the embodiment of such methods that additionally comprises evaluating the expression of one or more target and/or reference genes in a cellular sample from the patient, prior to and/or subsequent to the administration of the CD123 x CD3 bispecific molecule.
- the invention further provides, the embodiment of such methods wherein the method comprises evaluating the expression of such one or more target and/or such one or more reference genes prior to the administration of the CD123 x CD3 bispecific molecule.
- the invention also provides the embodiment of such methods wherein the method comprises evaluating the expression of such one or more target and/or such one or more reference genes subsequent to the administration of the CD123 x CD3 bispecific molecule.
- the invention further provides a method of determining whether a patient would be a suitable responder to the use of a CD123 x CD3 bispecific molecule to treat a hematologic malignancy, wherein the method comprises:
- the invention further provides the embodiment of such methods wherein the method evaluates: (i) the expression of one or more target gene; and (ii) one or more reference gene whose expression is not characteristically associated with the hematologic malignancy.
- the invention further provides the embodiment of such methods that comprises evaluating the expression of the one or more target genes relative to the baseline expression of the one or more reference genes of the patient.
- the invention further provides the embodiment of such methods that comprises evaluating the expression of the one or more target genes of a patient relative to the expression of the one or more target genes of an individual who is suffering from the hematologic malignancy or of a population of such individuals.
- the invention further provides the embodiment of such methods wherein the expression of the one or more target genes of such patient is greater than the first quartile (i.e., greater than the bottom 25%), greater than the second quartile (i.e., greater than the bottom 50%), or greater than the third quartile (i.e., greater than the bottom 75%) of the expression levels of such target gene(s) of such individual or of such population of individuals who are suffering from the hematologic malignancy.
- the invention further provides the embodiment of such methods that comprises evaluating the expression of the one or more target genes of a patient relative to the expression of the one or more target genes of an individual who had previously been unsuccessfully treated for a hematologic malignancy using the methods and compositions of the present invention (e.g., an individual who did not successfully respond to a treatment for a hematologic malignancy using a CD123 x CD3 bispecific molecule), or a population of such individuals.
- the invention further provides the embodiment of such methods wherein the expression of the one or more target genes of such patient is greater than the first quartile (i.e., greater than the bottom 25%), greater than the second quartile (i.e., greater than the bottom 50%), or greater than the third quartile (i.e., greater than the bottom 75%) of the expression levels of such target gene(s) of such individual or of such population of unsuccessfully treated individuals.
- the invention further provides the embodiment of such methods wherein the expression of the one or more target genes of such patient has a log2-fold change of at least about 0.4, at least about 0.5, at least about 0.6, or higher relative to the expression levels of such target gene(s) of such individual or such population of unsuccessfully treated individuals.
- the invention further provides the embodiment of such methods that comprises evaluating the expression of the one or more target genes of a patient relative to the expression of the one or more target genes of an individual who had previously been successfully treated for a hematologic malignancy using the methods and compositions of the present invention (e.g ., an individual who successfully responded to a treatment for a hematologic malignancy using a CD123 x CD3 bispecific molecule) or a population of such individuals.
- the invention further provides the embodiment of such methods wherein the expression of the one or more target genes of such patient is within the first quartile (i.e., within the bottom 25%) of the expression levels of such target gene(s), within the second quartile (i.e., between the bottom 25% and 50%), or within the third quartile (i.e., between the bottom 50% and 75%) of the expression levels of such target gene(s) of such individual or such population of successfully treated individuals.
- the invention further provides the embodiment of such methods wherein the relative expression level of the one or more target genes in the population is established by averaging the gene expression level in cellular samples obtained from the population of individuals.
- the invention further provides the embodiment of such methods wherein such patient exhibits an expression level of at least one of such target genes:
- the invention further provides the embodiment of such methods wherein such patient exhibits an expression level of at least one of such target genes:
- the invention further provides the embodiment of such methods wherein such patient exhibits an expression level of at least one of such target genes:
- the invention further provides a method of treating a hematologic malignancy, wherein the method comprises:
- the administration of the CD123 x CD3 bispecific molecule stimulates the killing of cells of the hematologic malignancy in the patient.
- the invention further provides the embodiment of such methods that additionally comprises evaluating the expression of such one or more target genes in a cellular sample obtained from the patient one or more times after the initiation of the treatment.
- the invention further provides the embodiment of such methods wherein the cellular sample is a bone marrow or a blood sample. Particularly, the embodiment of such methods wherein the cellular sample is a bone marrow sample.
- the invention further provides the embodiment of such methods that further comprises detecting the expression level of one or more target genes in a sample of the patient’s bone marrow.
- the invention further provides the embodiment of such methods that further comprises detecting the expression level of one or more reference genes.
- the invention further provides the embodiment of such methods that comprise detecting the expression level of such one or more target genes and/or such one or more reference genes in a sample of the patient’ s bone marrow, particularly prior to administration of a CD123 x CD3 bispecific molecule.
- the invention further provides the embodiment of such methods wherein the evaluation of expression or the determination of whether the patient would be a suitable responder to the use of a CD123 x CD3 bispecific molecule to treat a hematologic malignancy is performed by:
- the invention further provides the embodiment of such methods wherein the evaluation of expression or the determination of whether the patient would be a suitable responder to the use of a CD123 x CD3 bispecific molecule to treat a hematologic malignancy is performed by:
- the gene expression platform comprises a reference gene set of housekeeping genes
- the invention further provides the embodiment of such methods wherein the one or more target genes comprise:
- the invention further provides the embodiment of such methods wherein the one or more target genes further comprises IFNG (NM_0006l9.2).
- the invention further provides the embodiment of such methods wherein the one or more reference genes comprise one or more of: ABCF1, G6PD, NRDE2, OAZ1, POLR2A, SDHA, STK1 HP, TBC1D10B, TBP, and UBB.
- the one or more reference genes comprise one or more of: ABCF1, G6PD, NRDE2, OAZ1, POLR2A, SDHA, STK1 HP, TBC1D10B, TBP, and UBB.
- the invention further provides the embodiment of such methods wherein a gene signature score is determined for the one or more target genes.
- a gene signature score is determined from the raw RNA levels of each target gene by a process comprising:
- the gene signature is determined using the target genes provided in Tables 6 and 12A-12G.
- the weight factors are those provided in Tables 6 and 12A-12G.
- an adjustment factor is added to each score.
- the adjustment factors are those provided in Tables 6 and 12B-12G.
- the invention particularly, provides the embodiment of such methods wherein a gene signature score is determined for one or more of:
- the invention further provides the embodiment of such methods wherein a patient gene signature score that:
- (a) is greater than the first quartile of scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who are suffering from the hematologic malignancy;
- (b) is greater than the first quartile of scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.4 relative to scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (d) is within at least the first quartile of the scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who successfully responded to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- the invention further provides the embodiment of such methods wherein a patient gene signature score that:
- (a) is greater than the second quartile for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who are suffering from the hematologic malignancy;
- (b) is greater than the second quartile for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.5 relative to scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (d) is within at least the second quartile of the scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who successfully responded to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule, is indicative of a more favorable patient response to treatment with the CD123 x CD3 bispecific molecule.
- a patient gene signature score that:
- (a) is greater than the third quartile of scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who are suffering from the hematologic malignancy;
- (b) is greater than the third quartile of scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.6 relative to scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- the gene signature is the IFN Gamma Signaling Signature, and a patient gene signature score of at least about 2.5 is indicative of a more favorable patient response to treatment with the CD123 x CD3 bispecific molecule, and/or
- the gene signature is the Tumor Inflammation Signature, and a patient gene signature score of at least about 5.5 is indicative of a more favorable patient response to treatment with the CD123 x CD3 bispecific molecule;
- the gene signature is the IFN Downstream Signaling Signature, and a patient gene signature score of at least about 4.5 is indicative of a more favorable patient response to treatment with the CD123 x CD3 bispecific molecule.
- the invention further provides the embodiment of such methods wherein the gene signature is the IFN Gamma Signaling Signature, the Tumor Inflammation Signature, or the IFN Downstream Signaling Signature, and a patient gene signature score that:
- (a) is greater than the first quartile of the scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who are suffering from a hematologic malignancy;
- (b) is greater than the first quartile of the scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.4 relative to the scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (d) is within at least the first quartile of the scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who successfully responded to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- the invention further provides the embodiment of such methods wherein the gene signature is the IFN Gamma Signaling Signature, the Tumor Inflammation Signature, or the IFN Downstream Signaling Signature, and a patient gene signature score that:
- (a) is greater than the second quartile of scores of the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who are suffering from the hematologic malignancy;
- (b) is greater than the second quartile of scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.5 relative to scores for the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who did not successfully respond to a treatment for the hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (d) is within at least the second quartile of the scores of the gene signature calculated from the expression levels of one or more of the target genes in a population of individuals who successfully responded to a treatment for a hematologic malignancy that used a CD123 x CD3 bispecific molecule is indicative of a more favorable patient response to treatment with the CD123 x CD3 bispecific molecule.
- the invention also provides the embodiment of such methods wherein a patient that exhibits a gene expression signature that is characteristic of an immune- enriched and IFN gamma-dominant tumor microenvironment is indicative of a more favorable patient response to treatment with the CD123 x CD3 bispecific molecule.
- the invention further provides the embodiment of such methods wherein the CD123 x CD3 bispecific molecule is a bispecific antibody or a bispecific molecule comprising an scFv.
- the invention further provides the embodiment of such methods wherein the CD123 x CD3 bispecific molecule is JNJ-63709178, XmAbl4045 or APV0436.
- the invention further provides the embodiment of such methods wherein the CD123 x CD3 bispecific molecule is a covalently bonded bispecific diabody having two, three, or four polypeptide chains.
- CD123 x CD3 bispecific molecule is a diabody that comprises:
- first and the second polypeptide chains are covalently bonded to one another by a disulfide bond.
- the invention further provides the embodiment of such methods wherein the hematologic malignancy of such patient is selected from the group consisting of: acute myeloid leukemia (AML), chronic myelogenous leukemia (CML), blastic crisis of CML, Abelson oncogene-associated with CML (Bcr-ABL translocation), myelodysplastic syndrome (MDS), acute B lymphoblastic leukemia (B-ALL), acute T lymphoblastic leukemia (T-ALL), chronic lymphocytic leukemia (CLL), Richter’s syndrome, Richter’s transformation of CLL, hairy cell leukemia (HCL), blastic plasmacytoid dendritic cell neoplasm (BPDCN), non-Hodgkin’s lymphoma (NHL), including mantle cell lymphoma (MCL) and small lymphocytic lymphoma (SLL), Hodgkin’s lymphoma, systemic mastocytosis, and Burkitt’s lympho
- the invention further provides the embodiments of such methods wherein the hematologic malignancy of such patient is AML, MDS, BPDCN, or T-ALL.
- the invention further provides the embodiment of such methods wherein the hematologic malignancy of such patient is refractory to chemotherapy (CTX), such as being refractory to cytarabine/anthracycline-based cytotoxic chemotherapy or refractory to hypomethylating agents (HMA) chemotherapy.
- CTX refractory to chemotherapy
- HMA hypomethylating agents
- the invention further provides the embodiment of such methods that further comprises determining the level expression of CD123 of blast cells (cancer cells) as compared to a corresponding baseline level CD 123 expressed by normal peripheral blood mononuclear cells (PBMCs).
- PBMCs peripheral blood mononuclear cells
- the invention further provides the embodiment of such methods wherein the level of expression is determined by measuring the cell surface expression of CD 123.
- the invention further provides the embodiment of such methods wherein the cell surface expression of CD123 is increased by at least about 20% relative to a baseline level of expression.
- the invention further provides the embodiment of such methods wherein the increase in CD 123 expression renders the patient more responsive to treatment with the CD123 x CD3 bispecific molecule.
- the invention further provides the embodiment of such methods wherein the effective dosage of the CD123 x CD3 bispecific molecule is selected from the group consisting of 30, 100, 300, and 500 ng/kg patient weight/day.
- the invention further provides the embodiment of all of the above-described methods wherein the treatment dosage is administered as a continuous infusion.
- the invention further provides the embodiment of such methods wherein the treatment dosage is 30 ng/kg/day administered by continuous infusion for 3 days followed by a treatment dosage of 100 ng/kg/day administered by continuous infusion for 4 days.
- the invention further provides the embodiment of such methods wherein the treatment dosage further comprises administration of 500 ng/kg/day administered by continuous infusion.
- the invention further provides the embodiment of all of the above-described methods wherein the patient is a human patient.
- Figures 1A-1C illustrate the overall structure of exemplary diabody molecules.
- Figure 1A provides the structure of the first and second polypeptide chains of a two chain CD123 x CD3 bispecific diabody (“DART-A” also known as flotetuzumab) having two epitope-binding domains, Heterodimer-Promoting Domains and a cysteine containing linker.
- Figures 1B-1C provide the overall structure of a CD123 x CD3 bispecific diabody having two epitope-binding domains composed of three polypeptide chains. Two of the polypeptide chains possess a CH2 and CH3 Domain, such that the associated chains form all or part of an Fc Domain.
- the polypeptide chains comprising the VL and VH Domain further comprise a Heterodimer-Promoting Domain and a linker.
- a cysteine residue may be present in a linker ( Figures 1A and IB) and/or in the Heterodimer-Promoting Domain ( Figure 1C).
- VL and VH Domains that recognize the same epitope are shown using the same shading or fill pattern.
- Figure 2 illustrates unsupervised hierarchical clustering of the 46 10 360 signatures or cell types generated from the baseline bone marrow biopsy obtained from patients that had had a refractory response to conventional chemotherapy (e.g patient refractory response to a regimen of treatment with cytarabine given in conjunction with daunorubicin (7+3 induction therapy (Ref CTX)) or patients that had a refractory response to a regimen of treatment with the hypomethylating agents decitabine and azacitidine (Ref HMA and including patients with secondary AML), and patients that relapsed (Relapse) all prior to flotetuzumab treatment.
- conventional chemotherapy e.g patient refractory response to a regimen of treatment with cytarabine given in conjunction with daunorubicin (7+3 induction therapy (Ref CTX)
- Ref HMA hypomethylating agents decitabine and azacitidine
- Relapse relapsed
- Figures 3A-30 show that chemo- and HMA-refractory patients have different expression of multiple gene signatures.
- the gene expression profiles of Relapsed patients display features of immune depletion while the profiles of HMA-refractory (including HMA-refractory and secondary AML) patients displayed features of immune exhaustion and adaptive immune resistance, including upregulation of TIGIT, PD-L1 and Treg gene signatures together with a trend toward increasing gene signatures associated with exhausted CD8 T cells compared to CTX-refractory patients.
- Figure 3A is a forest plot of the fold change differences between Relapsed patients change from all refractory (CTX and HMA).
- Figure 3B is a forest plot of the fold change differences between HMA-refractory patients change from Relapse
- Figure 3C is a forest plot of the fold change differences between HMA-refractory patients change from CTX-refractory patients.
- Cluster 2 Immune Exhausted (C2) and Cluster 3 Immune Enriched (C3) gene signatures are indicated in Figures 3A and 3C.
- Figure 4 shows the percent change (relative to baseline) in bone marrow blasts from 25 patients (Relapse (RL) patients, patients that were CTX-Refractory (CTx), and patients that were HMA-Refractory (HMA)) after CD123 x CD3 bispecific binding molecule therapy and their response to such therapy (CR, Complete Response; mCR, molecular CR; CRi, Complete Response with incomplete hematological improvement; MLF, Morphologic Leukemia-free state; PR, Partial Response; SD, Stable Disease; PD, Progressive Disease/Treatment Failure).
- CR Complete Response
- mCR molecular CR
- CRi Complete Response with incomplete hematological improvement
- MLF Morphologic Leukemia-free state
- PR Partial Response
- SD Stable Disease
- PD Progressive Disease/Treatment Failure
- Figures 5A-5C show that the IFN Gamma Signaling Signature is increased at baseline in Responders to flotetuzumab, and that the IFN Gamma Signaling Signature is therefore predictive of a positive response to CD123 x CD3 bispecific binding molecule therapy.
- Figure 5A is a forest plot of the baseline fold change differences between OR patients and NR patients showing that the IFN Gamma Signaling Signature was increased in baseline samples in OR patients (Immune Exhausted (C2) and Immune Enriched (C3) gene signatures are indicated). The Tumor Inflammation Signature and IFN Downstream Signature were also seen to increase.
- Figure 5B shows the distribution of IFN Gamma Signaling Signature scores in NR and OR populations of patients (2 nd AML; Ref CTX: refractory to CTX; Ref HMA: refractory to HMA, Relapse: primary relapse).
- Figure 6 shows the expression of gene signatures associated with Cytotoxic cells, or with CD8+ T cells, as examined in RNA from bone marrow samples, either pre-treatment (“Base”) or from bone marrow samples after a first cycle of treatment with flotetuzumab (“Cycle 1”).
- Figure 7 shows the expression of CD 123 in patient populations that were either refractory to chemotherapy, in relapse, refractory to HMA, or in HMA failure.
- Figure 8 shows the correlation between the level of expression of PD-L1 in patient AML blasts at baseline (BL) and whether the patients were early progressors or responders to CD123 x CD3 bispecific binding molecule therapy. Data is expressed as mean + distribution.
- Figure 9 illustrates unsupervised hierarchical clustering of 48 IO 360 signatures or cell types generated from the baseline bone marrow biopsy obtained from patients that had had a primary refractory response to conventional chemotherapy (P), and patients that relapsed (R) all prior to flotetuzumab treatment. Also indicated are the patients’ responses to CD123 x CD3 bispecific binding molecule therapy with flotetuzumab.
- Such responses were annotated as being either an anti -leukemic response (A, which included patients exhibiting a complete response (CR), a complete response with incomplete hematological improvement (CRi), a morphologic leukemia-free state (MLF), other anti-leukemic benefit (OB), or a partial response (PR)), or as non responding (N, which included progressive disease/treatment failure (PD), and stable disease (SD)).
- A which included patients exhibiting a complete response (CR), a complete response with incomplete hematological improvement (CRi), a morphologic leukemia-free state (MLF), other anti-leukemic benefit (OB), or a partial response (PR)
- N which included progressive disease/treatment failure (PD), and stable disease (SD)
- Each IO 360 signature score was rescaled within the score for this cohort to a -3 to +3 scale to facilitate comparison across signatures. Stratification into Immune-infiltrated and Immune-depleted clusters is indicated.
- Figure 10 is a forest plot of the baseline fold-change differences of relapsed and refractory patients between those exhibiting an anti-leukemic response (OR) and non-responders (NR) to CD123 x CD3 bispecific binding molecule therapy with flotetuzumab, showing that numerous signatures were increased in baseline samples from responders including: the IFN Gamma Signaling Signature, IFN Downstream Signature, and Tumor Inflammation Signature (each boxed). The gene signatures which make up the IFN Dominant Module are starred and are also increased in baseline samples from responders.
- Figures 11A-11D show the score distribution of several gene signatures and the IFN module in refractory (Refir.) and relapsed (Rel.) patients, OR patients are indicated with large open circles, NR patients are indicated with small solid dots. Comparisons were performed with the Mann-Whitney U test for paired data. **R ⁇ 0.01.
- Figure 11A shows the distribution of the IFN Gamma Signaling Signature scores.
- Figure 11B shows the distribution of the IFN Downstream Signaling Signature scores.
- Figure 11C shows the distribution of the Tumor Inflammation Signature (TIS) scores.
- Figure 11D shows the distribution of the IFN Dominant Module (IFN module) scores.
- Figures 12A-12J shows the score distribution of the scores of the nine gene signatures that make up the IFN Dominant Module and the Tumor Inflammation Signature (TIS) in non-responders (NR) and responding patients (patients having an anti-leukemic response)(OR).
- TIS Tumor Inflammation Signature
- Figure 12A shows the IFN Gamma Signaling Signature scores
- Figure 12B shows the IFN Downstream Signature scores
- Figure 12C shows the Myeloid Inflammation Signature scores
- Figure 12D the Immunoproteasome Signature scores
- Figure 12E shows the Inflammatory Chemokines Signature scores
- Figure 12F shows the MAGEs Signature scores
- Figure 12G shows the PD-L1 Signature scores
- Figure 12H the PD-L2 Signature scores
- Figure 121 the IL10 Signature scores
- Figure 12J Tumor Inflammation Signature
- Figures 13A-13K shows ROC curves showing predictive performance of the baseline scores for the nine gene signatures that make up the IFN Dominant Module, the Tumor Inflammation Signature (TIS), and the IFN Dominant Module for the group of 30 refractory/relapsed patients.
- the present invention is directed to a method of treating a hematologic malignancy such as acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS), including hematologic malignancies that are refractive to chemotherapeutic and/or hypomethylating agents.
- AML acute myeloid leukemia
- MDS myelodysplastic syndrome
- the method concerns administering a CD123 x CD3 bispecific binding molecule to a patient in an amount effective to stimulate the killing of cells of said hematologic malignancy in said patient.
- the present invention is additionally directed to the embodiment of such method in which a cellular sample from the patient evidences an expression of one or more target genes that is increased relative to a baseline level of expression of such genes, for example, a baseline level of expression of such genes in a reference population of individuals who are suffering from the hematologic malignancy, or with respect to the level of expression of a reference gene.
- the therapeutic approach in patients with acute myeloid leukemia (AML) has not changed substantially in more than 30 years.
- the standard front line therapy is a two-drug regimen of cytarabine given in conjunction with daunorubicin (the so-called 7+3 induction therapy, abbreviated herein as“CTX”).
- CTX 7+3 induction therapy
- the hypomethylating agents (abbreviated herein as“HMA”) decitabine and azacitidine are commonly administered to older patients or to those considered unfit for the CTX regimen.
- HMA hypomethylating agents
- azacitidine are commonly administered to older patients or to those considered unfit for the CTX regimen.
- Bispecific antibodies that engage T cells stimulate the release of proinflammatory cytokines.
- cytokines can increase anti-leukemia efficacy by direct cytotoxicity and by activation and recruitment of immune cells into the tumor site (Hoseini, S.S. et al. (2107)“ Acute Myeloid Leukemia Targets For Bispecific Antibodies ,” Blood Cancer Journal 7:e522, doi: l0. l038/bcj .20l7.2; pp. 1-12.
- treatment with flotetuzumab a CD123 x CD3 bispecific binding molecule, is being tested in a Phase 1/2 study of relapsed/refractory (“R/R”) AML.
- the term“gene expression signature” is intended to denote a pattern of gene expression of a group of genes that is characteristic of a particular cell type and/or biological process (see, e.g., Stenner, F. et al. (2016) “ Cancer Immunotherapy and the Immune Response in Follicular Lymphoma ,” Front. Oncol. 8:219 doi: 10.3389/fonc.2018.00219, pages 1-7; Cesano, A. et al. (2016)“ Bringing The Next Generation Of Immuno-Oncology Biomarkers To The Clinic f Biomedicines 6(14) doi: l0.3390/biomedicines60l00l4, pages 1-11; Shrestha, G. et al.
- a central aspect of the present invention relates to the recognition that the presence of IFN gamma-dominant AML tumor microenvironments (“TMEs”), in contrast to predicting resistance to standard chemotherapy, predicts a favorable response to therapy employing CD123 x CD3 bispecific binding molecules, including therapy employing the CD123 x CD3 bispecific binding molecule, flotetuzumab.
- the invention derives in part from the recognition that certain sub-populations of patients having a refractory hematologic malignancy (e.g ., an acute myeloid leukemia) are particularly amenable to treatment with the CD123 x CD3 bispecific binding molecules (e.g., flotetuzumab).
- Members of this sub-population can be readily identified by their ability to exhibit a gene expression signature that is characteristic of the presence of an immune-enriched and IFN gamma-dominant tumor microenvironment.
- RNA sample from a cellular sample obtained from a patient is evaluated to determine whether it evidences increased expression of one or more “target” genes whose expression correlates with such a signature.
- Such evaluation may make use of pre-existing detection and/or measurements of gene expression or may incorporate the step(s) of detecting and/or measuring such gene expression.
- the term“cellular sample” refers to a sample that contains cells or an extract of cells.
- Any cellular sample may be employed as a source of RNA or protein for use in determining whether a patient exhibits a gene expression signature that is characteristic of the presence of an immune-enriched and IFN gamma-dominant tumor microenvironment.
- gene expression comparisons are conducted using RNA obtained from a bone marrow (BM) sample or from a blood sample or a sample of blast cells (cancer cells) of the patient or of a population of donors.
- BM bone marrow
- blast cells blast cells
- the average of the employed expression levels may be used (e.g, a geometric mean may be employed).
- a number of different reference populations may be used for such gene expression comparisons.
- the expression level of at least one target gene exhibited by a patient is compared to the expression level of such target gene exhibited in: a population of individuals who are suffering from a hematologic malignancy; a population of individuals who were suffering from such hematologic malignancy at the time such reference expression level was determined and who did not successfully respond to a treatment for a hematologic malignancy (i.e., a population of individuals who did not successfully respond to a treatment for a hematologic malignancy using a CD123 x CD3 bispecific molecule); and/or a population of individuals who were suffering from such hematologic malignancy at the time such reference expression level was determined and who were thereafter successfully treated for a hematologic malignancy using the methods and compositions of the present invention (i.e., a population of individuals who successfully responded to a treatment for a hematologic malignancy using a CD123 x CD3 bispecific molecule).
- the comparator population is a population of individuals who are suffering from a hematologic malignancy such population preferably includes individuals who are suffering from the same hematological malignancy as the patient. Such population may include individuals that have relapsed after prior treatment with a chemotherapeutic agent and/or that were refractory to treatment with a chemotherapeutic agent (i.e., primary refractory).
- the comparator population is a population of individuals who successfully, or unsuccessfully responded to a treatment for a hematologic malignancy CD123 x CD3 bispecific molecule such population preferably includes individuals who are suffering from the same hematological malignancy as the patient.
- the expression of a gene is said to be“increased” if, relative to a baseline or other comparator (e.g., expression of such gene in a population), its expression is at least about 10% greater, at least about 20% greater, at least about 30% greater, at least about 40% greater, at least about 50% greater, at least about 60% greater, at least about 70% greater, at least about 80% greater, at least about 90% greater, at least about 1.5-fold greater, at least about 2-fold greater, at least about 2.5- fold greater, at least about 3-fold greater, at least about 3.5-fold greater, at least about 4-fold greater, at least about 4.5-fold greater, at least about 5-fold greater, at least about 5.5-fold greater, at least about 6-fold greater, at least about 6.5-fold greater, at least about 7-fold greater, at least about 7.5-fold greater, at least about 8-fold greater, at least about 8.5-fold greater, at least about 9-fold greater, at least about lO-fold greater.
- log2-fold change of 0.4 is equivalent to about 30% greater expression
- a log2-fold change of 0.5 is equivalent to about 40% greater expression
- a log2-fold change of 0.6 is equivalent to about 50% greater expression
- a log2-fold change of 0.7 is equivalent to about 60% greater expression
- a log2-fold change of 0.8 is equivalent to about 70% greater expression
- a log2-fold change of 0.9 is equivalent to about 90% greater expression
- a log2-fold change of 1 is equivalent to a 2-fold increase
- a log2-fold change of 1.5 is equivalent to a 2.8-fold increase
- a log2-fold change of 2 is equivalent to a 4-fold increase
- a log2-fold change of 2.5 is equivalent to a 5.7-fold increase
- a log2-fold change of 3 is equivalent to an 8-fold increase
- a log2- fold change of 3.5 is equivalent to an 11.3-fold increase
- a log2-fold change of 4 is equivalent to a 16-fold increase, etc.
- a gene signature e.g ., an IFN Gamma Signaling Signature
- the expression of a gene signature is said to be“increased” if the gene signature score is at least about 2, or at least about 2.5, or at least about 3.0, or at least about 3.5, or at least about 4, or at least about 4.5, or at least about 5, or is at least about 5, or at least about 5.5, or at least about 5.5, or at least about 6, or is greater than about 6.5.
- a gene signature score of a patient is also said to be“increased” if it is greater than the first quartile of gene signature scores (i.e., greater than the bottom 25%), greater than the second quartile of gene signature scores (i.e., greater than the lower 50%), greater than the third quartile of gene signature scores (i.e., greater than the lower 75%), greater than 85%, greater than 90%, or greater than 95% of the gene signature scores calculated from the expression levels of such target genes in a population of individuals who are suffering from a hematologic malignancy.
- a gene signature score of a patient is also said to be“increased” if it is greater than the first quartile of gene signature scores (i.e., greater than the bottom 25%), greater than the second quartile of gene signature scores (i.e., greater than the lower 50%), greater than the third quartile of gene signature scores (i.e., greater than the lower 75%), greater than 85%, greater than 90%, or greater than 95% of the gene signature scores calculated from the expression levels of such target genes in a population of individuals who did not successfully respond to a treatment for a hematologic malignancy (e.g., a population of individuals who did not successfully respond to a treatment for a hematologic malignancy CD123 x CD3 bispecific molecule).
- a gene signature score of a patient is also said to be“increased” if it has a log2-fold change of at least about 0.4, or at least about 0.5, or at least about 0.6, or greater, relative to the gene signature scores calculated from the expression levels of such target genes in a population of individuals who did not successfully respond to a treatment for a hematologic malignancy (e.g, a population of individuals who did not successfully respond to a treatment for a hematologic malignancy CD123 x CD3 bispecific molecule).
- a gene signature score of a patient is also said to be“increased” if it is within at least the first quartile of gene signature scores (i.e., within the bottom 25%), and more preferably, within at least the second quartile (i.e., between the bottom 25% and 50%), within at least the third quartile (i.e., between the bottom 50% and 75%), greater than 85%, greater than 90%, or greater than 95% of the gene signature scores calculated from the expression levels of such target genes in a population of individuals who have previously been successfully treated for a hematologic malignancy using the methods and compositions of the present invention (e.g, a population of individuals who successfully responded to a treatment for a hematologic malignancy using a CD123 x CD3 bispecific molecule).
- a finding of an increased gene signature score is indicative of a more favorable patient response to treatment for hematologic malignancy with the CD123 x CD3 bispecific molecules of the present invention.
- a patient is identified as exhibiting a gene expression signature that is characteristic of the presence of an immune-enriched and IFN gamma- dominant tumor microenvironment and to thus be particularly amenable to the treatment of hematologic malignancy using the methods and compositions of the present invention by determining whether the expression of a target gene is“increased” relative to the baseline level of its expression in the patient being evaluated when such patient was healthy, or before such patient had received a diagnosis of hematologic malignancy, or relative to the expression of that gene at a time during such patient’s course of a chemotherapy treatment regimen or during such patient’s course of a treatment regimen involving a CD123 x CD3 bispecific binding molecule.
- a patient is identified as exhibiting a gene expression signature that is characteristic of the presence of an immune-enriched and IFN gamma-dominant tumor microenvironment and as thus being particularly amenable to the treatment of hematologic malignancy using the methods and compositions of the present invention by comparing the level of expression of one or more target gene(s) to the averaged or weighted baseline level of expression of such target gene(s) in a population of individuals who are suffering from a hematologic malignancy.
- a target gene whose expression is greater than such an averaged or weighted baseline level is said to exhibit an“increased” level of expression
- the methods and compositions of the present invention are particularly suitable for use in treating hematologic malignancy in such patients.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is greater than the first quartile (i.e., greater than the bottom 25%) of the expression levels of such target gene(s) in a population of individuals who are suffering from a hematologic malignancy.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is greater than the second quartile (i.e., greater than the bottom 50%) of the expression levels of such target gene(s) in a population of individuals who are suffering from a hematologic malignancy.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is greater than the third quartile ⁇ i.e., greater than the bottom 75%) of the expression levels of such target gene(s) in a population of individuals who are suffering from a hematologic malignancy.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is greater than 85%, greater than 90%, or greater than 95% of the expression levels of such target gene(s) in a population of individuals who are suffering from a hematologic malignancy.
- a patient is identified as exhibiting a gene expression signature that is characteristic of the presence of an immune-enriched and IFN gamma- dominant tumor microenvironment and as thus being particularly amenable to the treatment of hematologic malignancy using the methods and compositions of the present invention by comparing the level of expression of one or more target gene(s) to the averaged or weighted baseline level of expression of such target gene(s) in a population of individuals who have previously been unsuccessfully treated for a hematologic malignancy using the methods and compositions of the present invention ⁇ e.g ., a population of individuals who did not successfully respond to a treatment for a hematologic malignancy using a CD123 x CD3 bispecific molecule).
- a target gene whose expression is equal or greater than such an averaged or weighted baseline level is said to exhibit an“increased” level of expression
- the methods and compositions of the present invention are particularly suitable for use in treating hematologic malignancy in such patients.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is greater than the first quartile ⁇ i.e., greater than the bottom 25%) of the expression levels of such target gene(s) in such population of unsuccessfully-treated individuals.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is greater than the second quartile ⁇ i.e., greater than the bottom 50%) of the expression levels of such target gene(s) in such population of unsuccessfully-treated individuals.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is greater than the third quartile (i.e., greater than the bottom 75%) of the expression levels of such target gene(s) in such population of unsuccessfully-treated individuals.
- compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is greater than 85%, greater than 90%, or greater than 95% of the expression levels of such target gene(s) in such population of unsuccessfully -treated individuals.
- a patient is identified as exhibiting a gene expression signature that is characteristic of the presence of an immune-enriched and IFN gamma- dominant tumor microenvironment and as thus being particularly amenable to the treatment of hematologic malignancy using the methods and compositions of the present invention by comparing the level of expression of one or more target gene(s) to the averaged or weighted baseline level of expression of such target gene(s) in a population of individuals who have previously been successfully treated for a hematologic malignancy using the methods and compositions of the present invention (e.g ., a population of individuals who successfully responded to a treatment for a hematologic malignancy using a CD123 x CD3 bispecific molecule).
- a target gene whose expression is equal or greater than such an averaged or weighted baseline level is said to exhibit an“increased” level of expression
- the methods and compositions of the present invention are particularly suitable for use in treating hematologic malignancy in such patients.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is within at least the first quartile (i.e., within the bottom 25%) of the expression levels of such target gene(s) in such population of successfully-treated individuals.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is within at least the second quartile (i.e., between the bottom 25% and 50%) of the expression levels of such target gene(s) in such population of successfully-treated individuals.
- the methods and compositions of the present invention are particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is within at least the third quartile (i.e., between the bottom 50% and 75%) of the expression levels of such target gene(s) in such population of successfully-treated individuals.
- compositions of the present invention are even more particularly suitable for use in patients who exhibit an“increased” level of target gene(s) expression that is within at least the fourth quartile (i.e., above the bottom 75%) of the expression levels of such target gene(s) in such population of previously-treated individuals.
- a target gene’s expression is “increased” by comparing the level of its expression to the level of expression of one or more genes that are not associated with disease or that do not exhibit increased expression as a consequence of a disease state (“reference” genes). Because reference genes are often expressed at different levels, the geometric mean of the reference genes’ expression can be utilized to calculate scaling factors.
- a geometric mean is obtained by multiplying each gene per sample value in a data set and then taking the n th root (where n is the count of numbers in the set) of the resulting product.
- a geometric mean is similar to an arithmetic mean, in that it indicates the central tendency of a set of numbers.
- the geometric mean is less sensitive to variation in the magnitude of count levels between probes.
- the geometric mean from a set of“reference” gene(s) may be used to normalize individual samples across a data set in order for comparisons between biological genes to be made independent of differences due to technical variation such as sample mass input and sample quality.
- Preferred“reference” genes are constitutively expressed at the same level in normal and malignant cells.
- Housekeeping genes (Eisenberg, E. et al. (2003)“ Human Housekeeping Genes Are Compact ,” Trends in Genetics. l9(7):362-365; kon Butte, A.J. et al. (2001)“ Further Defining Housekeeping, Or “Maintenance, " Genes Focus On ⁇ Compendium Of Gene Expression In Normal Human Tissues’ ,” Physiol. Genomics. 7(2):95-96; Zhu, J. et al. (2008)“On The Nature Of Human Housekeeping Genes,” Trends in Genetics 24(l0):48l-484; Eisenberg, E. et al.
- a determination of whether a patient is particularly suitable for treatment with CD123 x CD3 binding molecule therapy further comprises:
- the determination of CD123 expression may be accomplished by assessing the presence of CD 123 -encoding mRNA, or by assessing the presence of CD 123 in a cellular lysate or extract. Alternatively, the determination of CD123 expression may be accomplished by assessing the presence of CD123 molecules arrayed on the cell-surface of CD 123 -expressing cells ( e.g ., blast cells).
- Increased expression e.g., at least a 10% increase in expression, at least a 15% increase in expression, at least a 20% increase in expression, at least a 25% increase in expression, at least a 30% increase in expression, or at least a 40% increase in expression
- CD123 is indicative of the patient’s suitability for receiving CD123 x CD3 binding molecule therapy for a hematologic malignancy.
- the level of PD-L1 expression is evaluated across a sample of the patient’s blast cells such that the percent of blast cells expressing PD-L1 is evaluated.
- the level of PD-L1 expression in the patients blast cells is compared to the relative to the expression of PD-L1 in such patient’s blast cells at a time during such patient’s course of a chemotherapy treatment regimen.
- the level of expression of PD-L1 in the patient’s cells may be assessed prior to any administration of a CD123 x CD3 binding molecule and/or after such administration.
- a finding of low expression of PD-L1 is indicative of the patient’s suitability for receiving CD123 x CD3 binding molecule therapy for a hematologic malignancy.
- a finding of high expression of PD-L1 is indicative of the patient’s suitability for receiving CD123 x CD3 binding molecule therapy in combination with an antagonist of the PD-1/PD-L1 axis for a hematologic malignancy.
- the determination of PD- Ll expression may be accomplished by assessing the presence of PD-L1- encoding mRNA, or by assessing the presence of PD-L1 in a cellular lysate or extract.
- the determination of PD-L1 expression may be accomplished by assessing the presence of PD-L1 molecules arrayed on the cell- surface of PD-L1 -expressing cells (e.g ., PBMCs). Increased expression (e.g. , at least 10% of blast cells express, at least 15% of blast cells express, at least 20% of blast cells express, at least 25% of blast cells express, at least 30% of blast cells express, or at least 40% of blast cells express) PD-L1 as so determined is indicative of the patient’s suitability for receiving CD123 x CD3 binding molecule therapy in combination with an antagonist of the PD-l/PD- Ll axis for a hematologic malignancy (see e.g., WO 2017/214092).
- PD-L1 -expressing cells e.g ., PBMCs.
- Increased expression e.g. , at least 10% of blast cells express, at least 15% of blast cells express, at least 20% of blast cells express, at least 25% of blast cells express, at
- CD8+ T-lymphocytes are monitored for increase in the proportion of CD8+ T-lymphocytes in the tumor microenvironment during and/or following the administration of the CD123 x CD3 bispecific molecule.
- the CD123 x CD3 binding molecule therapy of the present invention may additionally comprise the administration of an anti-human PD- Ll binding molecule, such as an anti -human PD-L1 antibody, or a diabody having a human PD-L1 binding domain.
- Anti-human PD-L1 binding molecules that may be used in accordance with this embodiment include atezolizumab, avelumab, and durvalumab (see, e.g, US Patent Nos. 9,873,740; 8,779, 108).
- the CD123 x CD3 binding molecule therapy of the present invention may additionally comprise the administration of an anti-human PD-l binding molecule, such as an anti-human PD-l antibody, or a diabody having a human PD-l binding domain.
- an anti-human PD-l binding molecule such as an anti-human PD-l antibody, or a diabody having a human PD-l binding domain.
- Anti -human PD-l binding molecules that may be used in accordance with this embodiment include: nivolumab (also known as 5C4, BMS-936558, ONO-4538, MDX-1106, and marketed as OPDIVO® by Bristol-Myers Squibb), pembrolizumab (formerly known as lambrolizumab, also known as MK- 3475, SCH-900475, and marketed as KEYTRUDA® by Merck), EH12.2H7 (commercially available from BioLegend), pidilizumab (CAS Reg.
- nivolumab also known as 5C4, BMS-936558, ONO-4538, MDX-1106, and marketed as OPDIVO® by Bristol-Myers Squibb
- pembrolizumab formerly known as lambrolizumab, also known as MK- 3475, SCH-900475, and marketed as KEYTRUDA® by Merck
- EH12.2H7 commercially available
- IFN gamma stimulates gene expression of more than 200 genes, which include primary response genes such as the IRFs, Fc-gamma receptor (FCGR), GBPs (guanylate-binding proteins), the major histocompatibility complex (MHC) class I and class II molecules, proteins involved in antigen presentation, antiviral proteins such as PKR, and OAS proteins, etc.
- primary response genes such as the IRFs, Fc-gamma receptor (FCGR), GBPs (guanylate-binding proteins), the major histocompatibility complex (MHC) class I and class II molecules, proteins involved in antigen presentation, antiviral proteins such as PKR, and OAS proteins, etc.
- Table 1 discloses exemplary target genes and a representative, non-limiting GenBank® Accession Number for each gene (see, Der, S.D. et al. (1988) “ Identification Of Genes Differentially Regulated By Interferon a, b, or g Using Oligonucleotide Arrays ,” Proc. Natl. Acad. Sci. (U.S.A.) 95: 15623-15628; Schneider, W.M. et al. (2014)“ Interferon-Stimulated Genes: A Complex Web of Host Defenses ,” Annu. Rev. Immunol. 32:513-545), and those disclosed in Schroder, K. et al.
- IFN Interferon Gamma Signaling Signature
- the genes of the IFN Gamma Signaling Signature are: CXCL9, CXCL10, CXCL11, and STAT1 (Table 6).
- the IFN Gamma Signaling Signature may further comprise IFNG (see, e.g, representative NCBI sequence accession number:NM_0006l9.2). Increased expression of the IFN Gamma Signaling Signature is particularly correlated to a patient’s suitability for CD123 x CD3 bispecific binding molecule therapy.
- Additional suitable target genes can be added. Such additional target genes may be readily identified as being downstream regulated genes of IFN gamma using the INTERFEROME Database (Samarajiwal, S.A. et al. (2009)‘‘INTERFEROME : The Database Of Interferon Regulated Genes f Nucleic Acids Research 37: D852- D857).
- PDCD1 also referred to herein by the common name PDL1
- PDCD1LG2 also referred to here by the common name PDL2
- IL10 CTLA4 (Table 13)
- IFN Interferon
- PDL1LG2 also referred to here by the common name PDL2
- IL10 CTLA4
- CTLA4 CTLA4
- the expression of multiple genes and signatures can be evaluated in the aggregate as a“module” to evaluate a patient’s suitability for CD123 x CD3 bispecific binding molecule therapy.
- One particularly preferred module which may be used to determine whether a patient exhibits an Immune-infiltrated (immune- enriched) IFN-dominant tumor microenvironment is referred to herein as an“IFN Dominant Module.”
- the target genes associated with the IFN Dominant Module include: PDL1, PDL2, IL10, CTLA4, and the genes present in each of the following gene expression signatures: the IFN Gamma Signaling Signature, the Interferon Downstream Signature, the Myeloid Inflammation Signature, the Inflammatory Chemokines Signature, the MAGES Signature, and the Immunoproteasome Signature
- the IFN Dominant Module is said to be“increased” if the module score is at least about 24, at least about 25, at least about 26, at least about 27, at least about 28, at least about 29, at least about 30, at least about 31, at least about 32, at least about 33, or at least about 35.
- the IFN Dominant Module score of a patient is also said to be“increased” if it is greater than the first quartile of IFN Dominant Module scores (i.e., greater than the bottom 25%), greater than the second quartile of IFN Dominant Module scores (i.e., greater than the lower 50%), greater than the third quartile of IFN Dominant Module scores (i.e., greater than the lower 75%), greater than 85%, greater than 90%, or greater than 95% of the IFN Dominant Module scores calculated from the expression levels of such target genes in a population of individuals who are suffering from a hematologic malignancy.
- the IFN Dominant Module score of a patient is also said to be“increased” if it is greater than the first quartile of IFN Dominant Module scores (i.e., greater than the bottom 25%), greater than the second quartile of IFN Dominant Module scores (i.e., greater than the lower 50%), greater than the third quartile of IFN Dominant Module scores (i.e., greater than the lower 75%), greater than 85%, greater than 90%, or greater than 95% of the IFN Dominant Module scores calculated from the expression levels of such target genes in a population of individuals who did not successfully respond to a treatment for a hematologic malignancy (e.g., a population of individuals who did not successfully respond to a treatment for a hematologic malignancy CD123 x CD3 bispecific molecule).
- a hematologic malignancy e.g., a population of individuals who did not successfully respond to a treatment for a hematologic malignancy CD123 x CD3 bi
- the IFN Dominant Module score of a patient is also said to be“increased” if it is within at least the first quartile of IFN Dominant Module scores (i.e., within the bottom 25%), and more preferably, within at least the second quartile (i.e., between the bottom 25% and 50%), within at least the third quartile (i.e., between the bottom 50% and 75%), greater than 85%, greater than 90%, or greater than 95% of IFN Dominant Module scores calculated from the expression levels of such target genes in a population of individuals who have previously been successfully treated for a hematologic malignancy using the methods and compositions of the present invention (e.g ., a population of individuals who successfully responded to a treatment for a hematologic malignancy using a CD123 x CD3 bispecific molecule).
- the gene signatures associated with the IFN Dominant Module can be individually evaluated to evaluate a patient’s suitability for CD123 x CD3 bispecific binding molecule therapy.
- TIS Tumor Inflammation Signature
- CCL5 CD27, CD274 , CD276, CD8A, CMKLR1, CXCL9, CXCR6, HLA-DQA1, HLA-DRB1, HLA-E, IDOl, LAG3, NKG7, PDCD1LG2, P SMB 10, STAT1, and/or TIGIT (Table 12A).
- Increased expression of the Tumor Inflammation Signature is particularly correlated to a patient’s suitability for CD123 x CD3 bispecific binding molecule therapy.
- Housekeeping genes that are constitutively expressed at the same level in normal and malignant cells comprise a preferred class of reference genes.
- Housekeeping genes include genes involved in general gene expression (such as genes encoding transcription factors, repressors, RNA splicing factors, translation factors, tRNA synthetases, RNA binding proteins, ribosomal proteins, mitochondrial ribosomal proteins, RNA polymerases, protein processing factors, heat shock proteins, histones, cell cycle regulators, apoptosis, oncogenes, DNA repair/replication, etc), metabolism (such as genes encoding enzymes of: carbohydrate metabolism, the citric acid cycle, lipid metabolism, amino acid metabolism, NADH dehydrogenases, cytochrome C oxidase, ATPases, lysosomal enzymes, proteasome proteins, ribonucleases, thioreductases, etc), cellular structural integrity (such as genes encoding cytoskeletal proteins, proteins involved in organelle synthesis,
- sterol regulatory element binding proteins e.g ., ATF1, ATF2, ATF4, ATF6, ATF7, ATF7, BTF3, E2F4, ERH, HMGB1, ILF2, IER2, JUND, TCEB2, etc.
- repressors e.g., PEIF60, etc
- RNA splicing proteins e.g., BAT1, HNRPD, HNRPK, PABPN1, SRSF3, etc.
- translation factors e.g, EIF1, EIF1 D, EIF1B, EIF2A, EIF2AK1, EIF2AK3, EIF2AK4, EIF2AK1, EIF2B2, EIF2B3, EIF2B4, EIF2S2, EIF3A, EIF3B, EIF3D, EIF3G, EIF3I, EIF3H, EIF3J, EIF3K, EIF3L, EIF3M, EIF3S5, EIF3S8, EIF4A1, EIF4A2, EIF4A3, EIF4E2, EIF4G1, EIF4G2, EIF4G3, EIF4H, EIF5, EIF5, EIF5A, EIF5AL1, EIF5B, EIF6, TUFM, etc);
- tRNA synthetases e.g, AARS, AARS2, AARSD1434, CARS, CARS2, DARS, DARS2, EARS2614, FARS2, FARSA, FARSB, GARS, HARS, HARS2, IARS, IARS2, KARS, LARS2, MARS, MARS2, NARS, NARS2, QARS, RARS, RARS2, SARS, TARS, VARS2, WARS2, YARS, YARS2436, etc);
- RNA binding proteins e.g, ELAVL1, etc
- ribosomal proteins e.g, RPL5, RPL8, RPL9, RPL10A, RPL11, RPL14, RPL25, RPL26L1, RPL27, RPL30, RPL32, RPL34, RPL35, RPL35A, RPL36AL, RPS5, RPS6, RPS6KA3, RPS6KB1, RPS6KB2, RPS13, RPS19BP1, RPS20, RPS23, RPS24, RPS27, RPN1, etc);
- mitochondrial ribosomal proteins e.g, MRPL9, MRPL1, MRPL10,
- MRPL24 MRPL27, MRPL28, MRPL3, MRPL30, MRPL32, MRPL33,
- RNA polymerases e.g, POLR1C, POLR1D, POLR1E, POLR2A, POLR2B, POLR2C, POLR2D, POLR2E, POLR2F, POLR2G, POLR2H, POLR2I, POLR2J, POLR2K, POLR2L, POLR3C, POLR3E, POLR3GL, POLR3K, etc);
- protein processing proteins e.g., PPID, PPIE, PPIF, PPIG, PPIH, CANX, CAPN1, CAPN7, CAPNS1, NACA, NACA2, PFDN2, PFDN4, PFDN5, PFDN6, SNX2, SNX3, SNX4, SNX5, SNX6, SNX9, SNX12, SNX13, SNX17, SNX18, SNX19, SNX25, SSR1, SSR2, SSR3, SUMOl, SUM03, etc);
- protein processing proteins e.g., PPID, PPIE, PPIF, PPIG, PPIH, CANX, CAPN1, CAPN7, CAPNS1, NACA, NACA2, PFDN2, PFDN4, PFDN5, PFDN6, SNX2, SNX3, SNX4, SNX5, SNX6, SNX9, SNX12, SNX13, SNX17, SNX18,
- heat shock proteins e.g, HSPA4, HSPA5, HSPA8, HSPA9, HSPA14, HSBP1, etc
- histones e.g, HIST1H2BC, H1FX, H2AFV, H2AFX, H2AFY, H2AFZ, etc);
- cell cycle proteins e.g, ARHGAP35, ARHGAP5, ARHGDIA, ARHGEF10L, ARHGEF11, ARHGEF40, ARHGEF7, RAB10, RAB11A, RAB11B, RAB 14, RAB 18, RAB 1A, RAB 1B, RAB21, RAB22A, RAB2A, RAB2B380, RAB3GAP1, RAB3GAP2, RAB40C, RAB4A, RAB5A, RAB5B, RAB5C, RAB6A, RAB7A, RAB9A, RABEP1, RABEPK, RABGEF1, RABGGTA, RABGGTB, CENPB, CTBP1, CCNB1IP1, CCNDBP1, CCNG1, CCNH, CCNK402, CCNL1, CCNL2, CCNY, PPP1CA, PPP1CC, PPP1R10, PPP1R11, PPP1R15B, PPP1R37, PPP1R7, PPP
- apoptosis proteins e.g, DAD1, DAP3, DAXX, etc.
- oncogene proteins e.g, ARAF, MAZ, MYC, etc.
- DNA repair/replication proteins e.g, MCM3AP, XRCC5, XRCC6, etc
- metabolism proteins e.g, PRKAG1, PRKAA1, PRKAB 1, PRKACA, PRKAG1, PRKAR1A, PRKRIP1, etc
- carbohydrate metabolism proteins e.g ., ALDOA, B3GALT6, B4GALT3, B4GALT5, B4GALT7, GSK3A, GSK3B, TPI1, PGK1, PGAM5, ENOPH1, LDHA, TALDOl, TSTA3;
- citric acid cycle proteins e.g., SDHA, SDHAF2, SDHB, SDHC, SDHD, etc.
- lipid metabolism proteins e.g, HADHA, etc
- amino acid metabolism proteins e.g, COMT, etc
- NADH dehydrogenases e.g, NDUFA2, NDUFA3, NDUFA4, NDUFA5, NDUFA6, NDUFA7, NDUFA8, NDUFA9, NDUFA10, NDUFA 1 1 , NDUFA 12, NDUFA 13, NDUFAF2, NDUFAF3, NDUFAF4, NDUFB2, NDUFB3, NDUFB4, NDUFB5, NDUFB6, NDUFB7, NDUFB 10, NDUFB 1 1 , NDUFB8, NDUFB9, NDUFC 1 , NDUFC2, NDUFC2, NDUFS5, NDUFV2, NDUFS2, NDUFS3, NDUFS4, NDUFS5, NDUFS6, NDUFS7, NDUFS8, NDUFV1, NDUFV2, etc);
- cytochrome C oxidases e.g, COX4I1, COX5B, COX6B1, COX6C, COX7A2, COX7A2L, COX7C, COX8, COX8A, COX11, COX14, COX15, COX16, COX19617, COX20, CYC1, UQCC, UQCR10, UQCR11, UQCRB, UQCRC1, UQCRC2, UQCRHL591, UQCRQ, ATPase, ATP2C1, ATP5A1, ATP5B, ATP5C1, ATP5D, ATP5F1, ATP5G2, ATP5G3, ATP5H, ATP5J, ATP5J2, ATP5J2, ATP5L, ATP50, ATP5S, ATP5SL, ATP6AP1, ATP6V0A2, ATP6V0B, ATP6V0C, ATP6V0D1, ATP6V0E1, ATP6V
- lysosomal proteins e.g, CTSD, CSTB, LAMP1, LAMP2, M6PR, etc
- proteasomal proteins e.g, PSMA1, PSMA2, PSMA3, PSMA4, PSMA5, PSMA6, PSMA7, PSMB1, PSMB2, PSMB3, PSMB4, PSMB5, PSMB6, PSMB7, PSMC2, PSMC3, PSMC4, PSMC5, PSMC6, PSMD1, PSMD10, PSMD11, PSMD12, PSMD13, PSMD14, PSMD2, PSMD3, PSMD4, PSMD5, PSMD6, PSMD7, PSMD8, PSMD9, PSME2, PSME3, PSMF1, PSMG2, PSMG3, PSMG4591, UBA1, UBA2, UBA3, UBA5, UBA52, UBAC2, UBALD 1 , UBAP1, UBAP2L, UBB, UBC, UBE2A, UBE2B, UBE2D2, UBE2D3, UBE2D4, UBE2E1, UBE2E2, UBE2E3, UBE2F, UBE2G2, UBE2H, UBE2I, UBE2J1, UBE2J2, UBE2K,
- ribonucleases e.g ., RNH, etc ;
- • thioreductases e.g., TXN2, TXNDCl l, TXNDC12, TXNDC15, TXNDC17, TXNDC9, TXNL1, TXNL4A, TXNL4B, TXNRD1, Cytoskeletal, ANXA6, ANXA7, ARPC1A, ARPC2, ARPC5L, CAPZA2, CAPZB, RHOB, RHOT1, RHOT2, TUBB, WDR1, etc);
- proteins involved in organelle synthesis e.g, BLOC1 S1, BLOC1 S2, BLOC1 S3, BLOC1 S4, BLOC1 S6, AP1G1, AP1M1, AP2A1, AP2A2, AP2M1, AP2S1, AP3B1, AP3D1, AP3M1, AP3S1, AP3S2, AP4B1, AP5M1, ANXA6, ANXA7, AP1B 1, CLTA, CLTB, CLTC, etc);
- mitochondrial proteins e.g, MTX2, etc
- cell surface proteins e.g., AP2S1, CD81, GPAA1, LGALS9, MGAT2, MGAT4B, VAMP3, etc;
- cell adhesion proteins e.g, CTNNA1, CTNNB1, CTNNBIP1, CTNNBL1, CTNND1458, etc.
- ion channels and transporter proteins e.g, ABCB 10, ABCB7, ABCD3,
- HLA/immunoglobulin/cell recognition proteins e.g, BAT1, BSG, MIF, TAPBP, etc.
- kinases/signaling proteins e.g, ADRBK1, AGPAT1, ARF1, ARF3, ARF4, ARF5, ARL2, CSF1, CSK, DCT, EFNA3, FKBP1A, GDI1, GNAS1, GNAI2, HAX1, ILK, MAPKAPK2, MAP2K2, MAP3K11, PITPNM, RAC1, RAP1B, RAGA, STK19, STK24, STK25, YWFLAB, YWHAH, YWHAQ, YWHAZ, etc); • growth factors (e.g., AIF1, HDGF, HGS, LTBP4, VEGFB, ZFP36L1, tissue necrosis factor, CD40, casein kinase, CSNK1E, CSNK2B, etc.); and
- miscellaneous proteins e.g, ALAS1, ARHGEF2, ARMET, AES, BECN1, BUD31, CKB, CPNE1, ENSA, FTH1, GDI2, GUK1, HPRT, IFITM1, JTB, MMPL2, NME2, NONO, P4HB, PRDX1, PTMA, RPA2, SULT1A3, SYNGR2, TTC1, Cl lOrfl3, Cl4orf2, C2lorf33, SPAG7, SRM, TEGT, DAZAP2, MEA1, etc ).
- miscellaneous proteins e.g, ALAS1, ARHGEF2, ARMET, AES, BECN1, BUD31, CKB, CPNE1, ENSA, FTH1, GDI2, GUK1, HPRT, IFITM1, JTB, MMPL2, NME2, NONO, P4HB, PRDX1, PTMA, RPA2, SULT1A3, SYNGR2, TTC1, Cl lOrfl3, Cl4orf2, C2lor
- Preferred housekeeping genes include those listed in Table 2.
- Table 2 also provides a representative, non-limiting NCBI Accession Number for each gene. Any combination or sub-combination of such genes (and/or splice variants of the same) may be employed.
- the amount of mRNA in a cellular sample corresponding to each assessed target gene is determined and normalized to the expression of mRNA corresponding to the baseline or reference gene(s). Any suitable method may be employed to accomplish such an analysis.
- a preferred method employs the nCOUNTER® Analysis System (NanoString Technologies, Inc.). In the nCOUNTER® Analysis System, RNA of a sample is incubated in the presence of sets of gene-specific Reporter Probes and Capture Probes under conditions sufficient to permit the sample RNA to hybridize to the probes.
- Each Reporter Probe carries a fluorescent barcode and each Capture Probe contains a biotin moiety capable of immobilizing the hybridized complex to a solid support for data collection. After hybridization, excess probe is removed, and the support is scanned by an automated fluorescence microscope. Barcodes are counted for each target molecule.
- Data analysis is preferably conducted using nSolver® 4.0 Analysis Software (NanoString Technologies, Inc.). The data presented in Example 1 was obtained using PanCancer IO 360TM Gene Expression Panel kits (NanoString Technologies, Inc.) which contain a set of probes for 770 different genes (750 genes cover the key pathways at the interface of the tumor, tumor microenvironment, and immune response, and 20 internal reference genes that may be used for data normalization (Table 5). Gene signature scores are calculated as follows:
- Raw data counts for each gene are normalized to the geometric mean of the selected housekeeping (HK) genes (e.g., ABCF1, NRDE2, G6PD, OAZ1, POLR2A, SDHA, STK1 HP, TBC1D10B, TBP, UBB) for each sample.
- HK housekeeping
- HK normalized data is then normalized to IO 360 panel standards, preferably to those run on the same cartridges as the test samples.
- each gene is multiplied by a weight value.
- Each of these weighted counts is summed to generate a single score.
- An adjustment factor that is a constant is added to the final calculated score (e.g. + 7).
- the adjustment factor may be derived from the lowest observed score (from TCGA and/or cell line analysis), in order for the score range to be above 0.
- the genes are categorized as follows: Column 1: Gene Name; Column 2: Internal Reference Gene; Column 3: Cell Type (B: B cells; CD8: CD8 T cells; Cyto: Cytotoxic cells; CD45: CD45-expressing cells; CD56d: NK CD56 dim cells; DC: dendritic cells; exhausted CD8 cells; M: macrophages; MC: Mast cells; N: Neutrophils; NK: NK cells; T: T cells; Thl : Thl cells; Treg: Treg cells); Column 4: Release of Cancer Antigens; Column 5: Cancer Antigen Presentation; Column 6: T Cell Priming and Activation; Column 7: Immune Cell Localization to Tumors; Column 8: Stromal Factors; Column 9: Recognition of Cancer Cells by T-cells; Column 10: Killing of Cancer Cells; Column 11: Myeloid Cell Activity; Column 12: NK Cell Activity; Column 13: Cell Cycle and Proliferation; Column 14: Tumor Intrinsic Factors; Column 15: Immuno
- BM bone marrow
- HMA-refractory including secondary AML
- Relapsed patients into 3 cluster groups within an immunological continuum: patients exhibiting an immune-depleted gene expression signature, patients exhibiting an immune-exhausted gene expression signature, and patients exhibiting an immune- enriched gene expression signature.
- patients with primary-refractory disease refractory to >2 induction attempts, first CR of ⁇ 6 months, or failure after >4 cycles of hypomethylating agents, HMA
- HMA hypomethylating agents
- the chemotherapy-refractory patients and the HMA- refractory patients further stratify into a first sub-population that exhibits gene signatures of an immune-exhausted tumor microenvironment (see, Figure 2, boxed signatures indicated for Cluster 2) and a second sub-population that exhibits gene signatures of an immune-enriched tumor microenvironment including the Interferon Gamma (also referred to herein as“IFN gamma”) Signaling Signature (see, Figure 2, boxed signatures indicated for Cluster 3).
- IFN gamma Interferon Gamma
- JNJ-63709178 is a humanized IgG4 bispecific antibody with silenced Fc function.
- the antibody was produced using Genmab DuoBody® technology and is able to bind both CD123 on tumor cells and CD3 on T cells.
- JNJ- 63709178 is disclosed in WO 2016/036937, Gaudet, F. et al.
- amino acid sequences of the heavy and light chains of JNJ-63709178 and/or related antibodies 13RB179, 13RB 180, 13RB 181, 13RB 182, 13RB 183, 13RB 186, 13RB 187, 13RB 188, 13RB 189, CD3B19, 7959, 3978, 7955, 9958, 8747, 8876, 4435 and 5466 are disclosed in WO 2016/036937.
- XmAb 14045 (also known as vibecotamab) is a tumor-targeted antibody that contains both a CD123 binding domain and a cytotoxic T-cell binding domain (CD3).
- An XmAb Bispecific Fc domain serves as the scaffold for these two antigen binding domains and confers long circulating half-life, stability and ease of manufacture on XmAbl4045.
- Engagement of CD3 by XmAbl4045 activates T cells for highly potent and targeted killing of CD 123 -expressing tumor cells (US Patent Publication 2017/0349660; Chu, S.Y. et al.
- APV0436 is an ADAPTIRTM CD123 x CD3 bispecific binding molecule that possesses an anti-CD 123 scFv portion and an anti-CD3 scFv portion. Each of the scFv portions are bound to an Fc Domain that has been modified to abolish ADCC/CDC effector function.
- APV0436 is disclosed to bind human CD123 and CD3 -expressing cells with EC so values in the low nM range and to demonstrate potent target-specific activity against CD 123 -expressing tumor cell lines at low effector to target ratios.
- APV0436 is disclosed to be capable of potently inducing endogenous T-cell activation and proliferation accompanied by depletion of CD 123 expressing cells in experiments with primary AML subject samples and normal donor samples.
- APV0436 see, Comeau, M.R. et al. (2016) “ APV0436 , a Bispecific anti-CD 123 x anti-CD 3 ADAPIIRTM Molecule for Redirected T-cell Cytotoxicity, Induces Potent T-cell Activation, Proliferation and Cytotoxicity with Limited Cytokine Release ,” AACR Annual Meeting April 2018, Abstract 1786; Godwin, C.D. et al.
- DART-A (also known as flotetuzumab, CAS number: 1664355-28-5) is the preferred CD123 x CD3 bispecific binding molecule of the present invention.
- DART- A is a sequence-optimized bispecific diabody capable of simultaneously and specifically binding to an epitope of CD123 and to an epitope of CD3 (a“CD123 x CD3” bispecific diabody) (US Patent Publn. No. US 2016-0200827, in PCT Publn. WO 2015/026892, in Al-Hussaini, M. et al.
- DART-A was found to exhibit enhanced functional activity relative to other non-sequence-optimized CD123 x CD3 bispecific diabodies of similar composition, and is thus termed a“sequence-optimized” CD123 x CD3 bispecific diabody.
- PCT Application PCT/US2017/050471 describes preferred dosing regimens for administering DART-A to patients, and is herein incorporated by reference in its entirety.
- DART-A comprises a first polypeptide chain and a second polypeptide chain ( Figure 1).
- the first polypeptide chain of the bispecific diabody will comprise, in the N-terminal to C-terminal direction, an N-terminus, a Light Chain Variable Domain (VL Domain) of a monoclonal antibody capable of binding to CD3 (VLCD3), an intervening linker peptide (Linker 1), a Heavy Chain Variable Domain (VH Domain) of a monoclonal antibody capable of binding to CD123 (VHcDm), and a C-terminus.
- VL Domain Light Chain Variable Domain
- Linker 1 an intervening linker peptide
- VH Domain Heavy Chain Variable Domain
- VHcDm a monoclonal antibody capable of binding to CD123
- a preferred sequence for such a VLCD3 Domain is SEQ ID NO:l:
- the Antigen Binding Domain of VLCD3 comprises:
- CDRL2 (SEQ ID NO:3): GTNKRAP
- CDRL3 (SEQ ID NO: 4): ALWYSNLWV
- a preferred sequence for such Linker 1 is SEQ ID NO:5: GGGSGGGG.
- a preferred sequence for such a VHCDI23 Domain is SEQ ID NO:6:
- the Antigen Binding Domain of VHCDI23 comprises:
- CDRH2 (SEQ ID NO: 8): DI I PSNGAT FYNQKFKG
- the second polypeptide chain will comprise, in the N-terminal to C-terminal direction, an N-terminus, a VL domain of a monoclonal antibody capable of binding to
- VLCDI23 CD123
- intervening linker peptide e.g, Linker 1
- VHCD3 a VH domain of a monoclonal antibody capable of binding to CD3
- C-terminus a preferred sequence for such a VLCDI23 Domain is SEQ ID NO:10:
- the Antigen Binding Domain of VLCDI23 comprises:
- CDRL2 (SEQ ID NO: 12): WAS TRES
- CDRL3 (SEQ ID NO: 13): QNDYSYPYT
- VHCD3 Domain A preferred sequence for such a VHCD3 Domain is SEQ ID NO:14:
- the Antigen Binding Domain of VHCD3 comprises:
- CDRH2 (SEQ ID NO: 16): RIRSKYNNYATYYADSVKD
- CDRH3 (SEQ ID NO: 17): HGNFGNSYVS WFAY
- the sequence-optimized CD123 x CD3 bispecific diabodies of the present invention are engineered so that such first and second polypeptides covalently bond to one another via cysteine residues along their length.
- Such cysteine residues may be introduced into the intervening linker (e.g ., Linker 1) that separates the VL and VH domains of the polypeptides.
- Linker 2 e.g ., Linker 1
- Linker 2 e.g a second peptide
- a preferred sequence for such Linker 2 is SEQ ID NO:18: GGCGGG.
- heterodimers can be driven by further engineering such polypeptide chains to contain polypeptide coils of opposing charge.
- one of the polypeptide chains will be engineered to contain an“E-coil” domain (SEQ ID NO:19: EVAALEKEVAALEKEVAALEKEVAALEK) whose residues will form a negative charge at pH 7, while the other of the two polypeptide chains will be engineered to contain an “K-coil” domain (SEQ ID NO:20: KVAALKEKVAALKEKVAALKEKVAALKEKVAALKE) whose residues will form a positive charge at pH 7.
- K-coil domain SEQ ID NO:20: KVAALKEKVAALKEKVAALKEKVAALKE
- DART-A a preferred sequence-optimized CD123 x CD3 bispecific diabody of the present invention
- DART-A Chain 1 is composed of: SEQ ID NO:l - SEQ ID NO:5 - SEQ ID NO:6— SEQ ID NO:18— SEQ ID NO:19.
- a polynucleotide that encodes the first polypeptide chain of DART-A is SEQ ID NO:22:
- the second polypeptide chain of DART-A has the sequence (SEQ ID NO:23):
- DART-A Chain 2 is composed of: SEQ ID NO: 10 - SEQ ID NO:5 - SEQ ID NO: 14— SEQ ID NO: 18— SEQ ID NO:20.
- a polynucleotide that encodes the second polypeptide chain of DART-A is
- DART-A has the ability to simultaneously bind CD 123 and CD3 as arrayed by human and cynomolgus monkey cells. Provision of DART-A was found to cause T cell activation, to mediate blast reduction, to drive T cell expansion, to induce T cell activation and to cause the redirected killing of target cancer cells (Table 4).
- DART-A-redirected killing was also observed with multiple target cell lines with T cells from different donors and no redirected killing activity was observed in cell lines that do not express CD123. Results are summarized in Table 5.
- DART-A is active against primary AML specimens (bone marrow mononucleocytes (BMNC) and peripheral blood mononucleocytes (PBMC)) from AML patients.
- primary AML specimens bone marrow mononucleocytes (BMNC) and peripheral blood mononucleocytes (PBMC)
- BMNC bone marrow mononucleocytes
- PBMC peripheral blood mononucleocytes
- DART-A is active against primary AML specimens (bone marrow mononucleocytes (BMNC) and peripheral blood mononucleocytes (PBMC)) from AML patients.
- BMNC bone marrow mononucleocytes
- PBMC peripheral blood mononucleocytes
- DART-A Incubation of primary AML bone marrow samples with DART-A resulted in depletion of the leukemic cell population over time compared to untreated control or Control DART.
- T cells were counted (CD8 and CD4 staining) and activation (CD25 staining) were assayed, the T cells expanded and were activated in the DART-A sample compared to untreated or Control DART samples.
- DART-A was also found to be capable of mediating the depletion of pDCs cells in both human and cynomolgus monkey PBMCs, with cynomolgus monkey pDCs being depleted as early as 4 days post infusion with as little as 10 ng/kg DART-A.
- DART-A is an antibody-based molecule engaging the CD3e subunit of the TCR to redirect T lymphocytes against cells expressing CD 123, an antigen up- regulated in several hematologic malignancies.
- DART-A binds to both human and cynomolgus monkey’s antigens with similar affinities and redirects T cells from both species to kill CD123+ cells.
- Monkeys infused 4 or 7 days a week with weekly escalating doses of DART-A showed depletion of circulating CD123+ cells 72h after treatment initiation that persisted throughout the 4 weeks of treatment, irrespective of dosing schedules.
- a decrease in circulating T cells also occurred, but recovered to baseline before the subsequent infusion in monkeys on the 4-day dose schedule, consistent with DART-A-mediated mobilization.
- DART-A administration increased circulating PD1+, but not TIM-3+, T cells; furthermore, ex vivo analysis of T cells from treated monkeys exhibited unaltered redirected target cell lysis, indicating no exhaustion.
- Toxicity was limited to a minimal transient release of cytokines following the DART-A first infusion, but not after subsequent administrations even when the dose was escalated, and a minimal reversible decrease in red cell mass with concomitant reduction in CD123+ bone marrow progenitors.
- DART-A comprising an Fc Region and having the general structure shown in Figure 1B is described in US 2016-0200827.
- Preferred polypeptides that contains the CH2 and CH3 Domains of an Fc Domain have the sequence (SEQ ID NO:25) (“Knob-Bearing” Fc Domain):
- the first polypeptide of an exemplary DART-A w/Fc construct comprises, in the N-terminal to C-terminal direction, an N-terminus, a VL domain of a monoclonal antibody capable of binding to CD123 (VLcDm), an intervening linker peptide (Linker 1), a VH domain of a monoclonal antibody capable of binding to CD3 (VHCD3), a Linker 2, an E-coil Domain, a Linker 5, Peptide 1, a polypeptide that contains the CH2 and CH3 Domains of an Fc Domain and a C-terminus.
- a preferred Linker 5 has the sequence: GGG.
- a preferred Peptide 1 has the sequence: DKTHTCPPCP (SEQ ID NO:29).
- the first polypeptide of such a DART-A w/Fc version 1 construct is composed of: SEQ ID NO: 10 - SEQ ID NO:5 - SEQ ID NO: 14 - SEQ ID NO: 18 - SEQ ID NO: 19 - GGG - SEQ ID NO:29 - SEQ ID NO:25 (wherein X is K) [001501
- a preferred sequence of the first polypeptide of such a DART- A w/Fc version 1 construct has the sequence (SEQ ID NO:27):
- the second chain of such a DART-A w/Fc version 1 construct will comprise, in the N-terminal to C-terminal direction, an N-terminus, a VL domain of a monoclonal antibody capable of binding to CD3 (VLCD3), an intervening linker peptide (Linker 1), a VH domain of a monoclonal antibody capable of binding to CD123 (VHCD123), a Linker 2, a K-coil Domain, and a C-terminus.
- VLCD3 VL domain of a monoclonal antibody capable of binding to CD3
- Linker 1 an intervening linker peptide
- VHCD123 VH domain of a monoclonal antibody capable of binding to CD123
- Linker 2 a K-coil Domain
- the second polypeptide of such a DART-A w/Fc version 1 construct is composed of: SEQ ID NO:l— SEQ ID NO:5— SEQ ID NO:6 - SEQ ID NO: 18 - SEQ ID NO:20.
- Such a polypeptide has the sequence (SEQ ID NO:28):
- the third polypeptide chain of such a DART-A w/Fc version 1 will comprise the CH2 and CH3 Domains of an IgG Fc Domain.
- compositions of the invention include bulk drug compositions useful in the manufacture of pharmaceutical compositions (e.g ., impure or non-sterile compositions) and pharmaceutical compositions (i.e., compositions that are suitable for administration to a subject or patient) which can be used in the preparation of unit dosage forms.
- Such compositions comprise a prophylactically or therapeutically effective amount of a CD123 x CD3 bispecific binding molecule and a pharmaceutically acceptable carrier.
- Preferred pharmaceutical formulations comprise a CD123 x CD3 bispecific binding molecule and an aqueous stabilizer and, optionally, a pharmaceutically acceptable carrier.
- the term“pharmaceutically acceptable carrier” is intended to refer to a diluent, adjuvant (e.g., Freund’s adjuvant (complete and incomplete)), excipient, or vehicle that is approved by a regulatory agency or listed in the U.S. Pharmacopeia or in another generally recognized pharmacopeia as being suitable for delivery into animals, and more particularly, humans.
- Such pharmaceutical carriers can be sterile liquids, such as water and oils, including those of petroleum, animal, vegetable or synthetic origin, such as peanut oil, soybean oil, mineral oil, sesame oil and the like. Water is a preferred carrier when the pharmaceutical composition is administered intravenously.
- Saline solutions and aqueous dextrose and glycerol solutions can also be employed as liquid carriers, particularly for injectable solutions.
- suitable pharmaceutical excipients include starch, glucose, lactose, sucrose, gelatin, malt, rice, flour, chalk, silica gel, sodium stearate, glycerol monostearate, talc, sodium chloride, dried skim milk, glycerol, propylene, glycol, water, ethanol and the like.
- the composition if desired, can also contain minor amounts of wetting or emulsifying agents, or pH buffering agents. These compositions can take the form of solutions, suspensions, emulsion, tablets, pills, capsules, powders, sustained-release formulations and the like.
- compositions of the invention are supplied either separately or mixed together in unit dosage form, for example, as a liquid formulation, as a dry lyophilized powder or water free concentrate in a hermetically sealed container such as a vial, an ampoule or sachette indicating the quantity of active agent.
- a liquid formulation such as a dry lyophilized powder or water free concentrate
- a hermetically sealed container such as a vial, an ampoule or sachette indicating the quantity of active agent.
- the composition is to be administered by infusion, it can be dispensed with an infusion bottle containing sterile pharmaceutical grade water or saline.
- an ampoule of sterile water for injection or saline can be provided so that the ingredients may be mixed prior to administration.
- the invention also provides a pharmaceutical pack or kit comprising one or more containers containing a CD123 x CD3 bispecific binding molecule alone or with a stabilizer and/or a pharmaceutically acceptable carrier. Additionally, one or more other prophylactic or therapeutic agents useful for the treatment of a disease can also be included in the pharmaceutical pack or kit.
- the invention also provides a pharmaceutical pack or kit comprising one or more containers filled with one or more of the ingredients of the pharmaceutical compositions of the invention.
- Optionally associated with such container(s) can be a notice in the form prescribed by a governmental agency regulating the manufacture, use or sale of pharmaceuticals or biological products, which notice reflects approval by the agency of manufacture, use or sale for human administration.
- kits that comprise a CD123 x CD3 bispecific binding molecule, instructional material (for example, relating to storage, dosage, indications, side effects, counter-indications, etc), and optionally a stabilizer and/or carrier that can be used in the above methods.
- the CD123 x CD3 bispecific binding molecule is preferably packaged in a hermetically sealed container such as an ampoule, a vial, a sachette, etc. that preferably indicates the quantity of the molecule contained therein.
- the container may be formed of any pharmaceutically acceptable material, such as glass, resin, plastic, etc.
- the CD123 x CD3 bispecific binding molecule of such kit is preferably supplied as a liquid solution, a dry sterilized lyophilized powder or a water-free concentrate in a hermetically sealed container that can be reconstituted, e.g ., with water or saline to the appropriate concentration for administration to a subject.
- a liquid or lyophilized material should be stored at between 2 and 8°C in its original container and the material should be administered within 12 hours, preferably within 6 hours, within 5 hours, within 3 hours, or within 1 hour after being reconstituted.
- the kit can further comprise one or more other prophylactic and/or therapeutic agents useful for the treatment of cancer, in one or more containers; and/or the kit can further comprise one or more cytotoxic antibodies that bind one or more cancer antigens associated with cancer.
- the other prophylactic or therapeutic agent is a chemotherapeutic.
- the prophylactic or therapeutic agent is a biological or hormonal therapeutic.
- the kit can further comprise instructions for use, or other printed information.
- one or more other prophylactic or therapeutic agents useful for the treatment of a disease can also be included in the pharmaceutical pack or kit.
- the invention also provides a pharmaceutical pack or kit comprising one or more containers filled with one or more of the ingredients of the pharmaceutical compositions of the invention.
- Optionally associated with such container(s) can be a notice in the form prescribed by a governmental agency regulating the manufacture, use or sale of pharmaceuticals or biological products, which notice reflects approval by the agency of manufacture, use or sale for human administration.
- the CD123 x CD3 bispecific binding molecule pharmaceutical formulations of the present invention may be provided for the treatment, prophylaxis, and amelioration of one or more symptoms associated with a disease, disorder or infection by administering to a subject an effective amount of a molecule of the invention, or a pharmaceutical composition comprising a fusion protein or a conjugated molecule of the invention.
- such compositions are substantially purified (i.e., substantially free from substances that limit its effect or produce undesired side effects).
- the subject is an animal, preferably a mammal such as non- primate (e.g., bovine, equine, feline, canine, rodent, etc.) or a primate (e.g, monkey such as, a cynomolgus monkey, human, etc.).
- non- primate e.g., bovine, equine, feline, canine, rodent, etc.
- a primate e.g, monkey such as, a cynomolgus monkey, human, etc.
- the subject or patient is a human.
- Methods of administering a CD123 x CD3 bispecific binding molecule pharmaceutical formulation of the invention include, but are not limited to, parenteral administration (e.g, intradermal, intramuscular, intraperitoneal, intravenous and subcutaneous).
- parenteral administration e.g, intradermal, intramuscular, intraperitoneal, intravenous and subcutaneous.
- the CD123 x CD3 bispecific binding molecules are administered intravenously.
- the compositions may be administered by any convenient route, for example, by infusion, and may be administered together with other biologically active agents.
- Infusion pumps are medical device that deliver fluids into a patient’s body in a controlled manner, especially at a defined rate and for a prolonged period of time. Infusion pumps may be powered mechanically, but are more preferably electrically powered. Some infusion pumps are“stationary” infusion pumps, and are designed to be used at a patient’s bedside. Others, called“ambulatory” infusion pumps, are designed to be portable or wearable.
- A“syringe” pump is an infusion pump in which the fluid to be delivered is held in the reservoir of a chamber ( e.g ., a syringe), and a moveable piston is used to control the chamber’s volume and thus the delivery of the fluid.
- A“elastomeric” infusion pump fluid is held in a stretchable balloon reservoir, and pressure from the elastic walls of the balloon drives fluid delivery.
- a “peristaltic” infusion pump a set of rollers pinches down on a length of flexible tubing, pushing fluid forward.
- a“multi-channel” infusion pump fluids can be delivered from multiple reservoirs at multiple rates.
- A“smart pump” is an infusion pump that is equipped a computer-controlled fluid delivery system so as to be capable of alerting in response to a risk of an adverse drug interaction, or when the pump's parameters have been set beyond specified limits.
- infusion pumps are well-known, and are provided in, for example, [Anonymous] 2002“ General-Purpose Infusion Pumps,” Health Devices 3 l(l0):353-387; and in US Patents No. 10,029,051, 10,029,047, 10,029,045, 10,022,495, 10,022,494, 10,016,559, 10,006,454, 10,004,846, 9,993,600, 9,981,082, 9,974,901, 9,968,729, 9,931,463, 9,927,943, etc.
- a 7-day continuous infusion regimen comprises a treatment dosage of about 30 ng/kg patient weight/day for 3 days followed by a treatment dosage of about 100 ng/kg/day for 4 days (for example, a treatment dosage of 30 ng/kg patient weight/day for 3 days followed by a treatment dosage of 100 ng/kg/day for 4 days; etc).
- such 7-day continuous infusion regiment is followed by a 21 -day continuous infusion regiment in which a treatment dosage of 500 ng/kg/day is administered during days 1-4 of each week of such 21 -day regiment and during days 5-7 of each week no treatment dosage is administered.
- such 7-day continuous infusion regiment is followed by a 21 -day continuous infusion regiment in which a treatment dosage of 500 ng/kg/day is administered every day for 21 days.
- the proportion of CD8+ T-lymphocytes in the tumor microenvironment may additionally be monitored. Such monitoring may occur prior to the administration of the CD123 x CD3 bispecific binding molecule, during the course of CD123 x CD3 binding molecule therapy, and/or after the conclusion of a cycle of CD123 x CD3 binding molecule therapy.
- the CD123 x CD3 bispecific binding molecules of the invention may be used to treat any disease or condition associated with or characterized by the expression of CD123.
- the CD123 x CD3 bispecific binding molecules of the invention may be used to treat hematologic malignancies.
- the CD123 x CD3 bispecific binding molecules of the invention are particularly suitable for use in the treatment of hematologic malignancies, including chemo-refractory hematologic malignancies.
- a chemo-refractory hematologic malignancy is a hematologic malignancy that is refractory to two or more induction attempts, a first CR of less than 6 months, or a failure after two or more cycles of treatment with a hypomethylating agent).
- such molecules may be employed in the diagnosis or treatment of acute myeloid leukemia (AML) (including primary chemo-refractory AML), chronic myelogenous leukemia (CML), including blastic crisis of CML and Abelson oncogene-associated with CML (Bcr-ABL translocation), myelodysplastic syndrome (MDS), acute B lymphoblastic leukemia (B-ALL), acute T lymphoblastic leukemia (T-ALL), chronic lymphocytic leukemia (CLL), including Richter’s syndrome or Richter’s transformation of call, hairy cell leukemia (HCL), blastic plasmacytoid dendritic cell neoplasm (BPDCN), non-Hodgkin’s lymphoma (NHL), including mantle cell lymphoma (MCL) and small lymphocytic lymphoma (SLL), Hodgkin’s lymphoma, systemic mastocytosis, and Burkitt’s lymphom
- AML acute myeloid
- the CD123 x CD3 bispecific binding molecules of the invention are particularly suitable for use in the treatment of acute myeloid leukemia (AML, including primary chemo-refractory acute myeloid leukemia), hematologic myelodysplastic syndrome (MDS), blastic plasmacytoid dendritic cell neoplasm (BPDCN), non-Hodgkin’s lymphoma (NHL), or acute T lymphoblastic leukemia (T- ALL)
- AML acute myeloid leukemia
- MDS hematologic myelodysplastic syndrome
- BPDCN blastic plasmacytoid dendritic cell neoplasm
- NHL non-Hodgkin’s lymphoma
- T- ALL acute T lymphoblastic leukemia
- a method of treating a chemo-refractory hematologic malignancy in a patient comprising administering to said patient a treatment dosage of a CD123 x CD3 bispecific molecule, said dosage being effective to stimulate the killing of cells of said hematologic malignancy in said patient and thereby treat said malignancy.
- said method additionally comprises evaluating the expression of one or more target and/or reference genes in a cellular sample from said patient, prior to and/or subsequent to said administration of said CD123 x CD3 bispecific molecule.
- E3 The method of E2, wherein said method comprises evaluating the expression of said one or more target and/or said one or more reference genes prior to said administration of said CD123 x CD3 bispecific molecule.
- E4 The method of E2, wherein said method comprises evaluating the expression of said one or more target and/or said one or more reference genes subsequent to said administration of said CD123 x CD3 bispecific molecule.
- a method of determining whether a patient would be a suitable responder to the use of a CD123 x CD3 bispecific molecule to treat a hematologic malignancy comprising:
- E7 The method of any one of E2-E6, wherein said method comprises evaluating the expression of said one or more target genes relative to the baseline expression of said one or more reference genes of said patient.
- E8 The method of any one of E2-E7, wherein said method comprises evaluating the expression of said one or more target genes of said patient relative to the expression of said one or more target genes of an individual who is suffering from said hematologic malignancy, or of a population of such individuals.
- said method comprises evaluating the expression of said one or more target genes of said patient relative to the expression of said one or more target genes of an individual who did not successfully respond to the use of a CD123 x CD3 bispecific molecule to treat said hematologic malignancy, or of a population of such individuals.
- E10 The method of any one of E2-E7, wherein said method comprises evaluating the expression of said one or more target genes of said patient relative to the expression of said one or more target genes of an individual who successfully responded to the use of a CD123 x CD3 bispecific molecule to treat said hematologic malignancy, or of a population of such individuals.
- E16 The method of E15, wherein said method additionally comprises evaluating the expression of said one or more target genes of said patient one or more times after the initiation of said treatment.
- a method of treating a hematologic malignancy comprising:
- E19 The method of any one of E2-E17, wherein said cellular sample is a bone marrow sample.
- E20 The method of any one of E2-E17, comprising detecting the expression level of said one or more target genes and/or said one or more reference genes in a sample of the patient’s bone marrow.
- E21 The method of any one of E2-E20, wherein said evaluation of expression or said determination of whether said patient would be a suitable responder to the use of a CD123 x CD3 bispecific molecule to treat a hematologic malignancy is performed by:
- E22 The method of any one of E2-E21, wherein said evaluation of expression or said determination of whether said patient would be a suitable responder to the use of a CD123 x CD3 bispecific molecule to treat a hematologic malignancy is performed by:
- E25 The method of any one of E2-E24, wherein said one or more reference genes comprise one or more of: ABCF1, G6PD, NRDE2, OAZ1, POLR2A, SDH A, STK11IP, TBC1D10B, TBP, and UBB.
- E26 The method of any one of E2-E25, wherein a gene signature score is determined for said one or more target genes.
- E27 The method of E26, wherein said gene signature score is determined by a process comprising:
- E28 The method of E26 or E27, wherein said gene signature score is determined using the target gene(s), the scoring weights and optionally the adjustment factors provided in Tables 6 and 12A-12G.
- E29 The method of any one of E26-E28, wherein said gene signature score is a gene signature score determined for one or more of:
- E30 The method of any one of E26-E29, wherein a patient gene signature score that:
- (a) is greater than the first quartile of scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who are suffering from said hematologic malignancy;
- (b) is greater than the first quartile of scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.4 relative to scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or (d) is within at least the first quartile of the scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who successfully responded to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- E31 The method of any one of E26-E29, wherein a patient gene signature score that:
- (a) is greater than the second quartile for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who are suffering from said hematologic malignancy;
- (b) is greater than the second quartile for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.5 relative to scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (d) is within at least the second quartile of the scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who successfully responded to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- (a) is greater than the third quartile of scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who are suffering from said hematologic malignancy;
- (b) is greater than the third quartile of scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.6 relative to scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- said gene signature is the IFN Gamma Signaling Signature, and a patient gene signature score of at least about 2.5 is indicative of a more favorable patient response to treatment with said CD123 x CD3 bispecific molecule, and/or
- said gene signature is the Tumor Inflammation Signature, and a patient gene signature score of at least about 5.5 is indicative of a more favorable patient response to treatment with said CD123 x CD3 bispecific molecule;
- said gene signature is the IFN Downstream Signaling Signature, and a patient gene signature score of at least about 4.5 is indicative of a more favorable patient response to treatment with said CD123 x CD3 bispecific molecule.
- (a) is greater than the first quartile of scores of said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who are suffering from said hematologic malignancy;
- (b) is greater than the first quartile of scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.4 relative to scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule;
- (d) is within at least the first quartile of the scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who successfully responded to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- (a) is greater than the second quartile of scores of said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who are suffering from said hematologic malignancy;
- (b) is greater than the second quartile of scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or (c) has a log2-fold change of at least about 0.5 relative to scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (d) is within at least the second quartile of the scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who successfully responded to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- E36 The method of any one of E28-E29, wherein said gene signature is the IFN Gamma Signaling Signature, the Tumor Inflammation Signature, or the IFN Downstream Signaling Signature, and a patient gene signature score that:
- (a) is greater than the third quartile of scores of said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who are suffering from said hematologic malignancy;
- (b) is greater than the third quartile of scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) has a log2-fold change of at least about 0.6 relative to scores for said gene signature calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- E37 The method of E29, wherein an IFN Dominant Module score is determined, and wherein a patient IFN Dominant Module score of at least about 25 is indicative of a more favorable patient response to treatment with said CD123 x CD3 bispecific molecule.
- E38 The method of E29, wherein an IFN Dominant Module score is determined, and wherein a patient IFN Dominant Module score that:
- (a) is greater than the first quartile of scores of said IFN Dominant Module calculated from the expression levels of one or more of said target genes in a population of individuals who are suffering from said hematologic malignancy;
- (b) is greater than the first quartile of scores for IFN Dominant Module calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) is within at least the first quartile of the scores for said IFN Dominant Module calculated from the expression levels of one or more of said target genes in a population of individuals who successfully responded to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- E39 The method of E29, wherein an IFN Dominant Module score is determined, and wherein a patient IFN Dominant Module score that:
- (a) is greater than the second quartile of scores of said IFN Dominant Module calculated from the expression levels of one or more of said target genes in a population of individuals who are suffering from said hematologic malignancy;
- (b) is greater than the second quartile of scores for IFN Dominant Module calculated from the expression levels of one or more of said target genes in a population of individuals who did not successfully respond to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule; or
- (c) is within at least the second quartile of the scores for said IFN Dominant Module calculated from the expression levels of one or more of said target genes in a population of individuals who successfully responded to a treatment for said hematologic malignancy that used a CD123 x CD3 bispecific molecule,
- E40 The method of any one of E26-E39, wherein a patient that exhibits a gene expression signature that is characteristic of an immune-enriched and IFN gamma-dominant tumor microenvironment is indicative of a more favorable patient response to treatment with said CD123 x CD3 bispecific molecule.
- E41 The method of any one of E1-E40, wherein said CD123 x CD3 bispecific molecule is a bispecific antibody or bispecific molecule comprising an scFv.
- E42 The method of E41, wherein said CD123 x CD3 bispecific molecule is JNJ- 63709178, XmAbl4045 or APV0436.
- E43 The method of any one of E1-E40, wherein said CD123 x CD3 bispecific molecule is a covalently bonded bispecific diabody having two, three, or four polypeptide chains.
- CD123 x CD3 bispecific molecule is a diabody that comprises:
- first and said second polypeptide chains are covalently bonded to one another by a disulfide bond.
- E45 The method of any one of E1-E44, wherein said hematologic malignancy of said patient is selected from the group consisting of: acute myeloid leukemia (AML), chronic myelogenous leukemia (CML), blastic crisis of CML, Abelson oncogene-associated with CML (Bcr-ABL translocation), myelodysplastic syndrome (MDS), acute B lymphoblastic leukemia (B-ALL), acute T lymphoblastic leukemia (T-ALL), chronic lymphocytic leukemia (CLL), Richter’s syndrome, Richter’s transformation of CLL, hairy cell leukemia (HCL), blastic plasmacytoid dendritic cell neoplasm (BPDCN), non-Hodgkin’s lymphoma (NHL), including mantle cell lymphoma (MCL) and small lymphocytic lymphoma (SLL), Hodgkin’s lymphoma, systemic mastocytosis, and Burkitt’s
- E46 The method of E45, wherein said hematologic malignancy of said patient is AML.
- E48 The method of E45, wherein said hematologic malignancy of said patient is BPDCN.
- E49 The method of E45, wherein said hematologic malignancy of said patient is T- ALL.
- E50 The method of any one of E2-E49, wherein said hematologic malignancy of said patient is refractory to chemotherapy.
- E53 The method of any one of E2-E52, further comprising determining the level expression of CD123 of blast cells (cancer cells) as compared to a corresponding baseline level CD 123 expressed by normal PBMCs.
- E54 The method of E56, wherein said level of expression is measured by cell surface expression of CD 123.
- E55 The method of E54, wherein said surface expression of CD 123 is increased by at least about 20% relative to a baseline level of expression.
- E56 The method of E55, wherein said increase in CD 123 expression renders the patient more responsive to treatment with said CD123 x CD3 bispecific molecule.
- E57. The method of any one of E1-E4, or E6-E56, wherein said treatment dosage of said CD123 x CD3 bispecific molecule includes at least one dose selected from the group consisting of 30, 100, 300, and 500ng/kg patient weight/day.
- E58 The method of E57, wherein said treatment dosage includes a dose of 30 ng/kg/day.
- E59 The method of E57, wherein said treatment dosage includes a dose of 100 ng/kg patient weight /day.
- E60 The method of E57, wherein said treatment dosage includes a dose of 300 ng/kg patient weight /day.
- E61 The method of E57, wherein said treatment dosage includes a dose of 500 ng/kg patient weight /day.
- E62 The method of any one of E1-E4, or E6-E561, wherein said treatment dosage is administered by continuous infusion.
- BM bone marrow
- NanoString PanCancer IO 360TM assay (NanoString Technologies, Inc.) compared the expression profiles of 750 genes that cover the key pathways at the interface of the tumor, tumor microenvironment, and immune response, including the levels of 14 immune cell types and 32 immuno-oncology signatures.
- the NanoString PanCancer IO 360TM assay also compared the expression profiles of control and internal reference genes for data normalization as provided below.
- the expression profile included gene signatures of the following pathways or cells: Proliferation, JAKSTAT loss, endothelial cells, B7-H3, APM loss, glycolytic activity, mast cells, cytotoxicity, cytotoxic cells, CD8 T cells, lymphoid cells, T cells, Treg cells, CTLA4, TIS, Thl cells, TIGIT, NK O ⁇ 56 ⁇ h cells, NK cells, apoptosis, hypoxia, ARG1, IL-10, IFN gamma, macrophages, myeloid cells, neutrophils, PD-L2, stroma, dendritic cells (DC), MAGEs, IDOl, B cells, PD-l, NOS2, inflammatory chemokines, PD-L1, CD45, exhausted CD8 T cells, immunoproteasome, APM, IFN downstream regulated genes, myeloid inflammatory genes, MHC2 genes, TGF beta, MMR loss.
- Interferon (IFN) Gamma Signaling Signature genes including a representative, non-limiting NCBI accession number for each gene, and weight factors are shown in Table 6 below.
- Raw data counts for each gene are normalized to the geometric mean of 10 housekeeping (HK) genes (ABCF1, NRDE2, G6PD, OAZ1, POLR2A, SDHA, STK11IP, TBC1D10B, TBP, UBB) for each sample.
- HK housekeeping
- IFN Gamma Signaling Signature scores is 0 to 10.
- the range is 1 to 5.
- the score is calculated for each baseline (screen day -14) sample.
- Baseline expression of the profiled genes was correlated with whether the patient had a refractory response to conventional chemotherapy (i.e., patient refractory response to a regimen of treatment with cytarabine given in conjunction with daunorubicin (e.g. , 7+3 induction therapy, (abbreviated as Ref CTX or CTX- refractory)) or patient refractory response to a regimen of treatment with the hypom ethylating agents (e.g, decitabine and azacitidine, (abbreviated as Ref HMA or HMA-refractory)) or to patient relapse (Relapse).
- conventional chemotherapy i.e., patient refractory response to a regimen of treatment with cytarabine given in conjunction with daunorubicin (e.g. , 7+3 induction therapy, (abbreviated as Ref CTX or CTX- refractory)) or patient refractory response to a regimen of treatment with the hypom
- FIG. 4 provides a waterfall plot of 25 evaluable patients treated at the target dose. Such responses were scored as being either an objective response (OR) or as non-responding (NR).
- OR included all patients that exhibited a molecular complete response (mCR), a complete response with incomplete hematological improvement (CRi), a morphologic leukemia-free state (MLF), and a partial response (PR).
- NR included all patients that exhibited progressive disease/ treatment failure (PD), and stable disease (SD).
- Figure 2 provides an unsupervised hierarchical clustering the 46 IO 360 signatures or cell types generated from the results.
- the results show the baseline levels of expression of the 36 bone marrow samples (each in a separate column) relative to the gene signature evaluated (each in a separate row).
- Each IO 360 signature score was rescaled within the score for this cohort to a -3 to +3 scale to facilitate comparison across signatures.
- chemotherapy-refractory and HMA-refractory patients further stratify into immune-enriched and immune-exhausted phenotypes, respectively.
- the gene signatures associated with immune-exhausted and immune enriched phenotypes are listed in Table 7 below and indicted on the forest plots shown in Figures 3A, 3B, and 4A.
- FIG. 3D-30 Plotted in Figures 3D-30 are several gene signature scores associated with the Immune Enriched (Cluster 2, Figure 3D-3I) or the Immune Exhausted (Cluster 3, Figure 3J-30) profiles.
- Figure 4 shows the change (relative to baseline) in blast cells present in bone marrow samples from 25 patients (categorized as being either relapse (RL) patients or patients that were Chemo-Refractory (CTX) or HMA- Refractory (HMA)) as a measure of their response to the CD123 x CD3 bispecific binding molecule flotetuzumab at the target dose of 500 ng/kg/day.
- the objective response (OR) rate to the therapy for Primary Refractory patients was 50% (7/14).
- the complete response (CR) rate for Primary Refractory patients was 35.7% (5/14).
- Figure 5A presents a forest plot of the baseline fold change differences between OR patients and NR patients (including PD, SD, TF, NE) showing that expression of the IFN Gamma Signaling Signature was increased in baseline samples in OR patients (boxed in Figure 5A, showing change from NR).
- the TIS and IFN Downstream Signatures were substantially increased in OR patients.
- Figure 5B shows that the distribution of IFN Gamma Signaling Signature scores is increased in OR patients.
- the sensitivity and specificity of the IFN Gamma Signaling Signature score was measured to predict response diagnostic capability. Bootstrapping over all samples is performed using different threshold cutoffs for the range of data in this cohort.
- the confidence intervals (CIs) of the thresholds or the sensitivity and specificity values are computed with bootstrap resampling and the averaging methods. In all bootstrap CIs, patients are resampled and the modified curve is built before the statistics of interest is computed. As in the bootstrap comparison test, the resampling is done in a stratified manner by default.
- ROC area under receiver operating characteristic
- Flotetuzumab-induced tumor microenvironment (TME) gene activation was therefore indicative of an immune-enrichment signature rather than an immune-exhaustion signature.
- TEE tumor microenvironment
- AML blast samples collected during screening were analyzed for PD-L1 expression by flow cytometry.
- patients that progressed early ( ⁇ 15 days) on flotetuzumab treatment had higher baseline levels of PD-L1 on AML cells than other patients, and had evidence of response (SD, OB, PR, CR).
- SD, OB, PR, CR evidence of response
- the results of this investigation indicate that PD-L1 expression is associated with decreased activity in vivo and support the combinatorial use of a PD-1/PD-L1 antagonist in combination with a CD123 x CD3 bispecific binding molecule therapy (see, e.g ., WO 2017/214092).
- CD123 x CD3 bispecific binding molecule therapy may invigorate an immune exhausted tumor microenvironment as noted by 25% anti-leukemic activity in this population.
- treatment with the CD123 x CD3 bispecific binding molecule, DART-A was seen to enhance immune activation, antigen processing/presenting and IFN Gamma Signaling Signatures scores.
- the gene signatures associated with the three signature modules are listed in Table 10 below.
- the module score is the sum of the individual gene signature scores in each sample (each gene signature score was calculated as provided above).
- Figure 9 provides an unsupervised hierarchical clustering (Euclidean distance, complete linkage) of immune and biological activity signatures in the bone marrow (BM) microenvironment of patients with relapsed/refractory AML prior to receiving flotetuzumab immunotherapy in the CP-MGD006-01 clinical trial (NCT#02152956).
- Responders were individuals exhibiting an anti -leukemic response defined as either complete remission (CR), CR with incomplete hematologic recovery (CRi), CR with partial hematologic recovery (CRh) partial remission (PR) or“other benefit” (OB; >30% decrease in BM blasts).
- Non-responders were individuals with either treatment failure (TF), stable disease (SD) or progressive disease (PD).
- Chemotherapy refractoriness was defined as >2 induction attempts or lst CR with initial CR duration ⁇ 6 months.
- Each IO 360 signature score was rescaled within the score for this cohort to a -3 to +3 scale to facilitate comparison across signatures.
- Figure 10 presents a forest plot of the baseline fold change differences between responders (CR, CRi, CRh, PR, and OB) and non-responders (PD, SD, TF) from the analysis of the 30 chemotherapy-refractory or relapsed AML patients. Consistent with the analysis provided in Example 1 above, the expression of the IFN Gamma Signaling Signature, IFN Downstream Signature, and Tumor Inflammation Signature (boxed in Figure 10) were increased in baseline samples in responders vs non-responders. In addition, most of the gene signatures that make up the IFN Dominant Module were increased in baseline samples in responders vs non-responders (starred in Figure 10).
- the distribution of scores for these gene signatures are increased in responding patients.
- the responders showed significantly higher IFN Gamma Signaling Signature, IFN Downstream Signature, TIS, and IFN Dominant Module scores at baseline compared to non-responders. Comparisons were performed with the Mann Whitney U test for unpaired determinations.
- IO 360 gene counts were generated using the nCounter® system (NanoString Technologies, Inc.) essentially as follows: RNA (-100 ng per sample) was purified from bone marrow aspirates, and was incubated with report and capture probe mix for hybridization. Transcript counts were analyzed on the nCounter FLEX analysis system using the high-resolution setting. Reporter code count (RCC) output files are used to calculate gene signature scores using pre-defmed linear combinations (weighted averages) of biologically relevant gene sets essentially as previously described, as detailed herein.
- RCC Reporter code count
- IFN Gamma Signaling Signature is described in detail above. Immune cell type abundance signatures were defined in Danaher, P., el al, 2017,“ Gene Expression Markers of Tumor Infiltrating Leukocytes ,” J Immunother Cancer 5, 18); Tumor Inflammation Signature is as described in Danaher, P., etal ., 2018 (“ Pan-cancer Adaptive Immune Resistance as Defined by the Tumor Inflammation Signature (TlS : Results From The Cancer Genome Atlas (TCGA)f J Immunother Cancer. 6(l):63) (also see T cell-inflamed GEP described in Ayers. M., el al.
- TIS Tumor Inflammation Signature
- Interferon (IFN) Downstream Signature Genes including a representative, non-limiting NCBI accession number for each gene, and weight factors are shown in Table 12B below.
- the adjustment factor for this signature is: 5.342598.
- MAGEs Signature genes including a representative, non-limiting NCBI accession number for each gene, and weight factors are shown in Table 12D below.
- the adjustment factor for this signature is: 3.965625.
- Myeloid Inflammation (Myeloid Inflam) Signature genes including a representative, non-limiting NCBI accession number for each gene, and weight factors are shown in Table 12E below.
- the adjustment factor for this signature is: 5.41931.
- the Immunoproteasome Signature genes (including a representative, non limiting NCBI accession number for each gene), and weight factors are shown in Table 12F below.
- the adjustment factor for this signature is: 6.096812.
- the single gene signature genes (including a representative, non-limiting NCBI accession number for each gene) and adjustment factors are shown in Table 12G below.
- the signatures scores are calculated essentially as described above except that once normalized and log transformed, each gene is multiplied to the weight provided in Tables 12A-12F, and the indicated adjustment factor is added. For single gene signatures (e.g ., PDL1) no weight is used, the log2 normalized gene expression values are added to the adjustment factors are provided in Table 12G.
Landscapes
- Health & Medical Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Organic Chemistry (AREA)
- Immunology (AREA)
- Life Sciences & Earth Sciences (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- General Health & Medical Sciences (AREA)
- Genetics & Genomics (AREA)
- Medicinal Chemistry (AREA)
- Molecular Biology (AREA)
- Biochemistry (AREA)
- Biophysics (AREA)
- Engineering & Computer Science (AREA)
- Wood Science & Technology (AREA)
- Zoology (AREA)
- Analytical Chemistry (AREA)
- Oncology (AREA)
- Animal Behavior & Ethology (AREA)
- General Chemical & Material Sciences (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Pharmacology & Pharmacy (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Physics & Mathematics (AREA)
- Biotechnology (AREA)
- Microbiology (AREA)
- General Engineering & Computer Science (AREA)
- Pathology (AREA)
- Hematology (AREA)
- Communicable Diseases (AREA)
- Hospice & Palliative Care (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
- Pharmaceuticals Containing Other Organic And Inorganic Compounds (AREA)
- Measuring Or Testing Involving Enzymes Or Micro-Organisms (AREA)
- Peptides Or Proteins (AREA)
- Medicines Containing Antibodies Or Antigens For Use As Internal Diagnostic Agents (AREA)
- Medicinal Preparation (AREA)
Abstract
Description



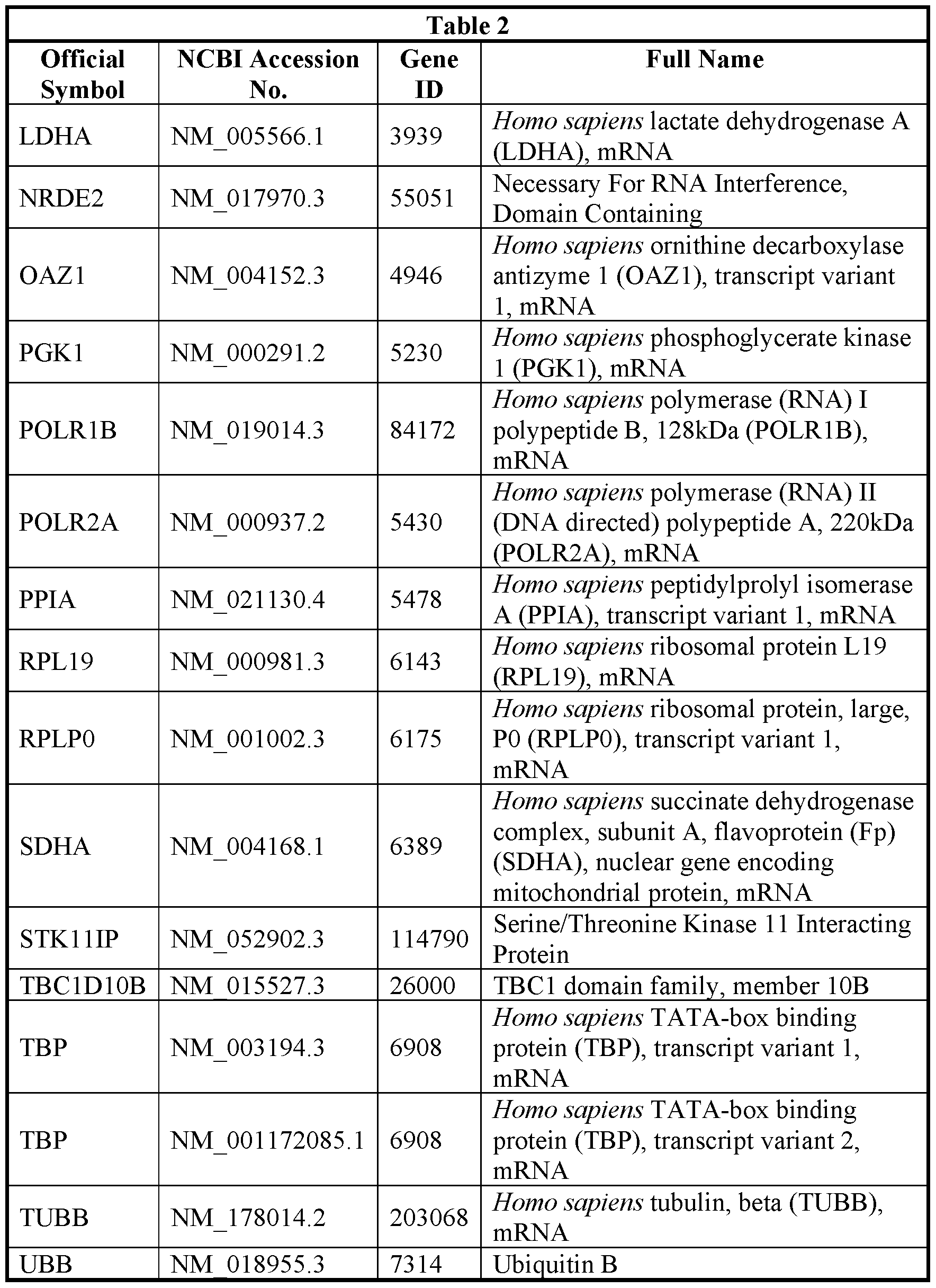
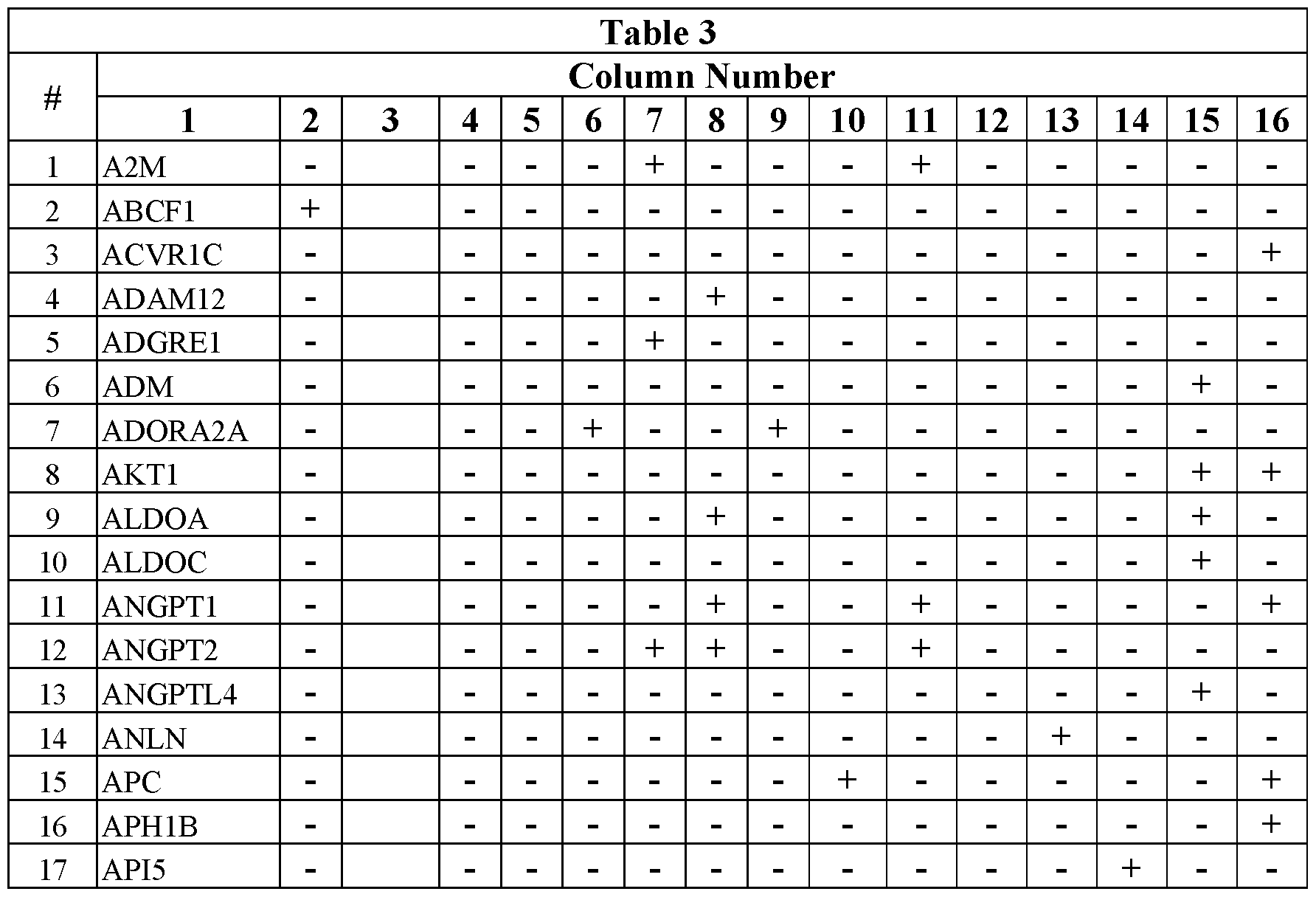























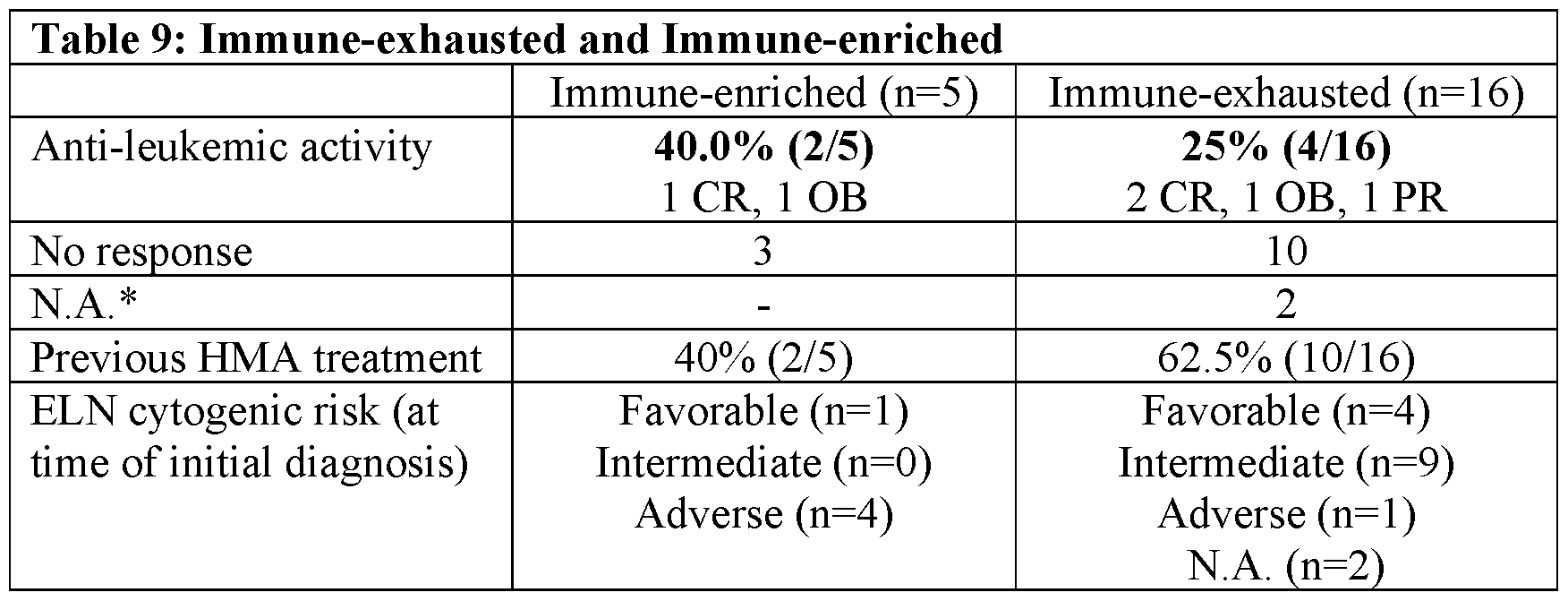




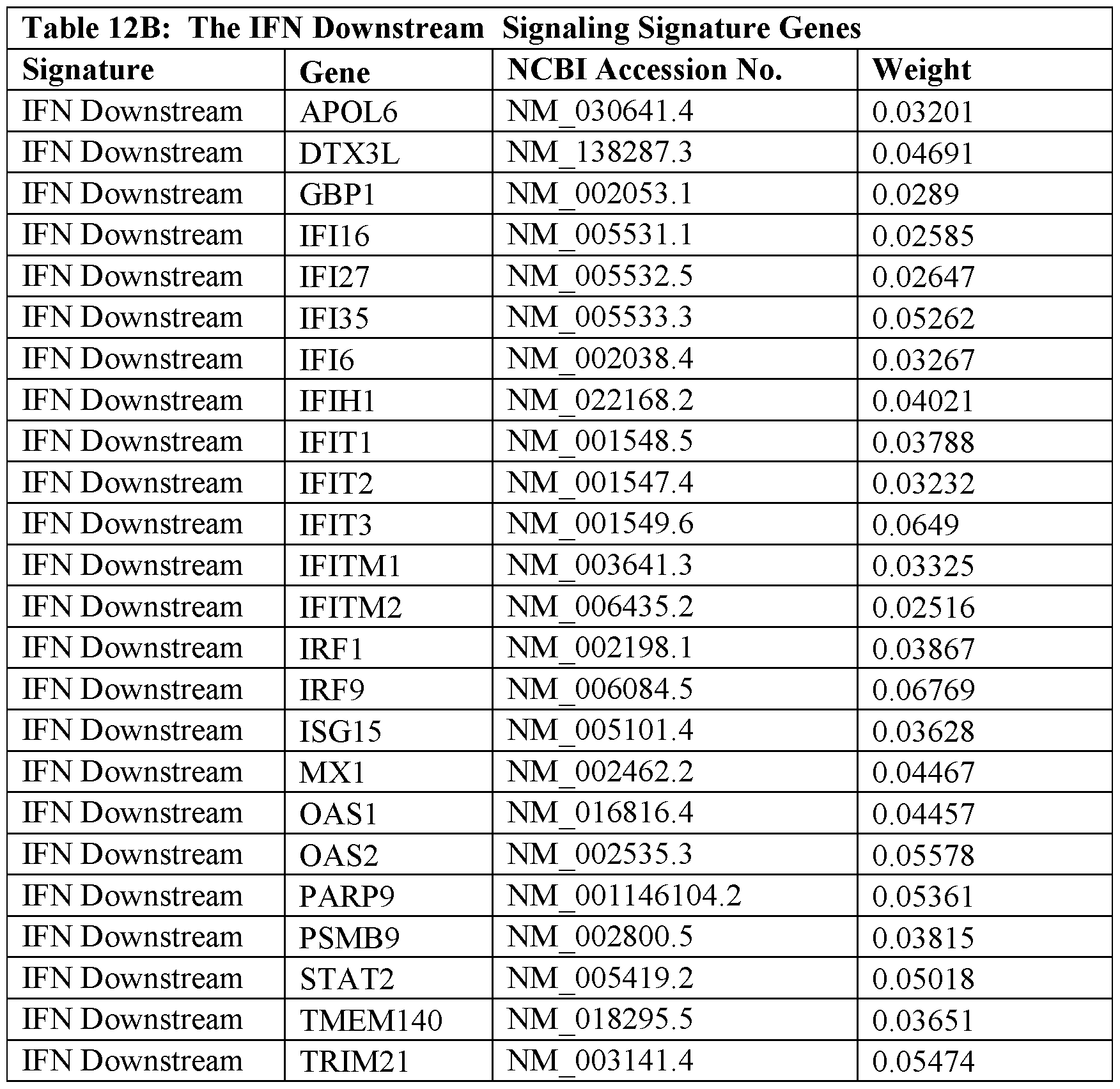


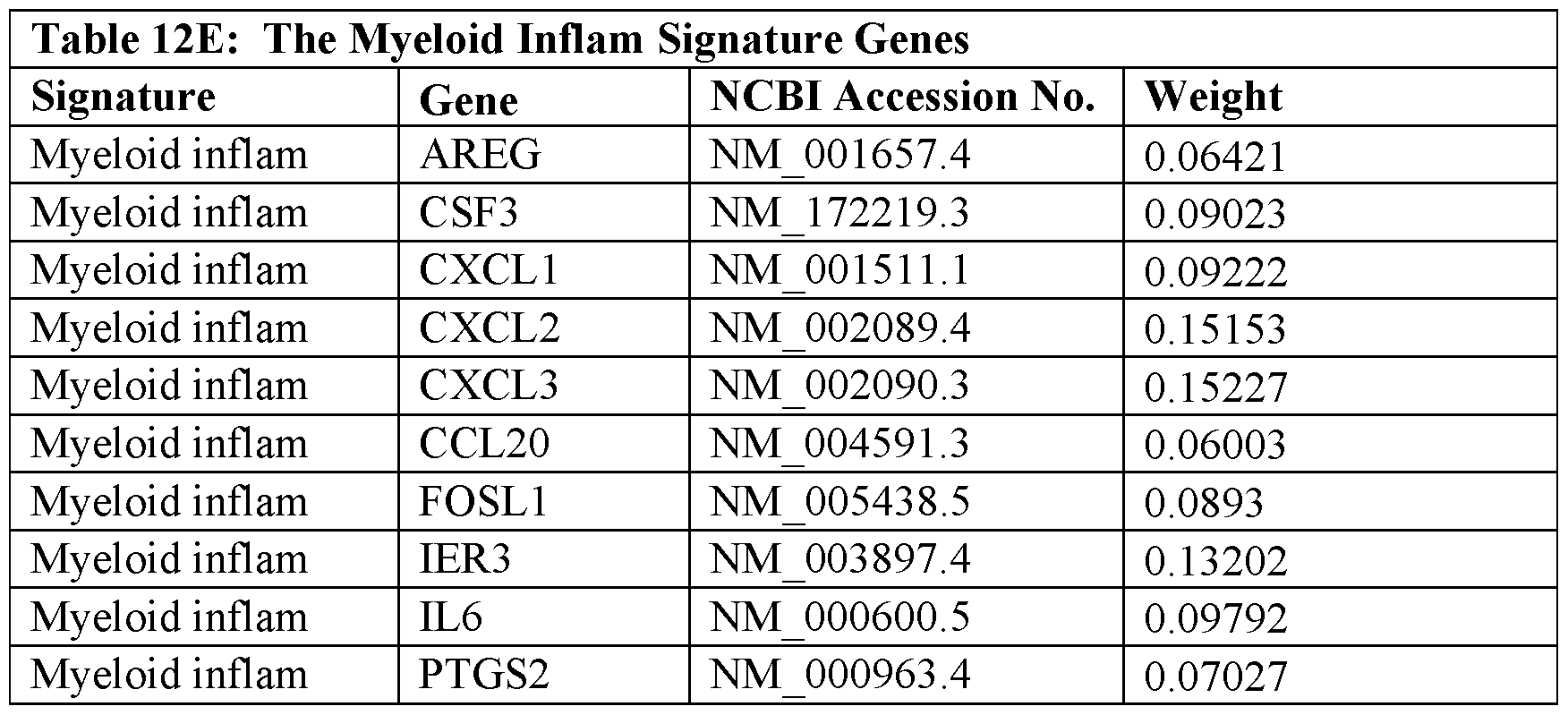


Claims
Priority Applications (15)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US17/290,061 US20210395374A1 (en) | 2018-10-30 | 2019-10-29 | Bispecific CD123 x CD3 Diabodies for the Treatment of Hematologic Malignancies |
| SG11202104367RA SG11202104367RA (en) | 2018-10-30 | 2019-10-29 | Bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies |
| EP19878838.2A EP3873606A4 (en) | 2018-10-30 | 2019-10-29 | BISPECIFIC CD123 X CD3 DIABODIES FOR THE TREATMENT OF HEMATOLOGICAL MALIGNOS |
| KR1020217014961A KR102943465B1 (en) | 2018-10-30 | 2019-10-29 | Bispecific CD123 x CD3 Diabodies for the Treatment of Blood Cancer |
| CN201980087139.5A CN113286633A (en) | 2018-10-30 | 2019-10-29 | Bispecific CD123x CD3 diabodies for the treatment of hematological malignancies |
| CN202411135807.6A CN119280393A (en) | 2018-10-30 | 2019-10-29 | Bispecific CD123 x CD3 diabody for the treatment of hematological malignancies |
| MX2021004868A MX2021004868A (en) | 2018-10-30 | 2019-10-29 | Bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies. |
| CN202411135769.4A CN119236065A (en) | 2018-10-30 | 2019-10-29 | Bispecific CD123 x CD3 diabody for the treatment of hematological malignancies |
| AU2019371243A AU2019371243A1 (en) | 2018-10-30 | 2019-10-29 | Bispecific CD123 x CD3 diabodies for the treatment of hematologic malignancies |
| BR112021008283-2A BR112021008283A2 (en) | 2018-10-30 | 2019-10-29 | METHOD OF TREATMENT OF A CHEMOREFRACTORY HEMATOLOGICAL MALIGNITY IN A PATIENT, AND METHOD FOR DETERMINING WHETHER A PATIENT WOULD BE AN ADEQUATE RESPONDER TO USE A CD123 X CD3 BSPECIFIC MOLECULE TO TREAT A HEMATOLOGICAL MALIGNITY |
| JP2021548536A JP7551066B2 (en) | 2018-10-30 | 2019-10-29 | Bispecific CD123xCD3 Diabodies for the Treatment of Hematological Malignancies - Patent application |
| CA3118081A CA3118081A1 (en) | 2018-10-30 | 2019-10-29 | Bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies |
| ZA2021/02775A ZA202102775B (en) | 2018-10-30 | 2021-04-26 | Bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies |
| IL282827A IL282827A (en) | 2018-10-30 | 2021-04-29 | "Diabodi" antibodies with double specificity 123cd x 3cd for the treatment of blood diseases |
| JP2024139452A JP2024178163A (en) | 2018-10-30 | 2024-08-21 | Bispecific CD123xCD3 Diabodies for the Treatment of Hematological Malignancies - Patent application |
Applications Claiming Priority (6)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US201862752659P | 2018-10-30 | 2018-10-30 | |
| US62/752,659 | 2018-10-30 | ||
| US201862769078P | 2018-11-19 | 2018-11-19 | |
| US62/769,078 | 2018-11-19 | ||
| US201962878368P | 2019-07-25 | 2019-07-25 | |
| US62/878,368 | 2019-07-25 |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| WO2020092404A1 true WO2020092404A1 (en) | 2020-05-07 |
| WO2020092404A8 WO2020092404A8 (en) | 2021-05-20 |
Family
ID=70464448
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2019/058616 Ceased WO2020092404A1 (en) | 2018-10-30 | 2019-10-29 | Bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies |
Country Status (13)
| Country | Link |
|---|---|
| US (1) | US20210395374A1 (en) |
| EP (1) | EP3873606A4 (en) |
| JP (2) | JP7551066B2 (en) |
| KR (1) | KR102943465B1 (en) |
| CN (3) | CN119280393A (en) |
| AU (1) | AU2019371243A1 (en) |
| BR (1) | BR112021008283A2 (en) |
| CA (1) | CA3118081A1 (en) |
| IL (1) | IL282827A (en) |
| MX (1) | MX2021004868A (en) |
| SG (1) | SG11202104367RA (en) |
| WO (1) | WO2020092404A1 (en) |
| ZA (1) | ZA202102775B (en) |
Cited By (7)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2021257334A1 (en) * | 2020-06-18 | 2021-12-23 | Macrogenics, Inc. | Use of bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies |
| WO2022165171A1 (en) | 2021-01-28 | 2022-08-04 | Regeneron Pharmaceuticals, Inc. | Compositions and methods for treating cytokine release syndrome |
| WO2022178243A1 (en) * | 2021-02-20 | 2022-08-25 | Kite Pharma, Inc. | Gene markers for sellecting immunotherapies |
| WO2023092119A3 (en) * | 2021-11-22 | 2023-06-29 | Ludwig Institute For Cancer Research Ltd | Methods for predicting responsiveness to a cancer therapy |
| WO2023192850A1 (en) * | 2022-03-29 | 2023-10-05 | Ngm Biopharmaceuticals, Inc. | Ilt3 and cd3 binding agents and methods of use thereof |
| WO2023201226A1 (en) | 2022-04-11 | 2023-10-19 | Regeneron Pharmaceuticals, Inc. | Compositions and methods for universal tumor cell killing |
| WO2024173830A2 (en) | 2023-02-17 | 2024-08-22 | Regeneron Pharmaceuticals, Inc. | Induced nk cells responsive to cd3/taa bispecific antibodies |
Families Citing this family (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| KR20250134857A (en) * | 2024-03-05 | 2025-09-12 | 사회복지법인 삼성생명공익재단 | Method, device, and computer program for predicting responsiveness of a non-small cell lung cancer patient to an immun checkpoint inhibitor |
| CN120866362B (en) * | 2025-07-15 | 2026-03-31 | 郑州大学第一附属医院 | CAR-T cells overexpressing the IFITM2 gene, their construction methods, and their application in immunocellular therapy. |
Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20110123442A1 (en) * | 2009-10-08 | 2011-05-26 | Pinku Mukherjee | Tumor specific antibodies and uses therefor |
| WO2015069935A1 (en) * | 2013-11-06 | 2015-05-14 | Memorial Sloan-Kettering Cancer Center | Compositions and methods for the treatment of acute myeloid leukemias and myelodysplastic syndromes |
| US20170183413A1 (en) * | 2014-03-19 | 2017-06-29 | Cellectis | Cd123 specific chimeric antigen receptors for cancer immunotherapy |
| WO2017214092A1 (en) * | 2016-06-07 | 2017-12-14 | Macrogenics, Inc. | Combination therapy |
Family Cites Families (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2005333987A (en) | 2004-05-06 | 2005-12-08 | Veridex Llc | Prognosis of malignant blood disease |
| EP2839842A1 (en) | 2013-08-23 | 2015-02-25 | MacroGenics, Inc. | Bi-specific monovalent diabodies that are capable of binding CD123 and CD3 and uses thereof |
| TW201722428A (en) | 2015-10-23 | 2017-07-01 | 第一三共股份有限公司 | Medicinal composition for treating acute myeloid leukemia (AML) and method for treating acute myeloid leukemia for those in need thereof |
| TWI790206B (en) | 2016-07-18 | 2023-01-21 | 法商賽諾菲公司 | Bispecific antibody-like binding proteins specifically binding to cd3 and cd123 |
| WO2019050521A1 (en) * | 2017-09-07 | 2019-03-14 | Macrogenics, Inc. | Dosing regimens of bi-specific cd123 x cd3 diabodies in the treatment of hematologic malignancies |
-
2019
- 2019-10-29 CN CN202411135807.6A patent/CN119280393A/en active Pending
- 2019-10-29 EP EP19878838.2A patent/EP3873606A4/en active Pending
- 2019-10-29 BR BR112021008283-2A patent/BR112021008283A2/en unknown
- 2019-10-29 AU AU2019371243A patent/AU2019371243A1/en active Pending
- 2019-10-29 WO PCT/US2019/058616 patent/WO2020092404A1/en not_active Ceased
- 2019-10-29 CA CA3118081A patent/CA3118081A1/en active Pending
- 2019-10-29 CN CN202411135769.4A patent/CN119236065A/en active Pending
- 2019-10-29 MX MX2021004868A patent/MX2021004868A/en unknown
- 2019-10-29 CN CN201980087139.5A patent/CN113286633A/en active Pending
- 2019-10-29 US US17/290,061 patent/US20210395374A1/en active Pending
- 2019-10-29 KR KR1020217014961A patent/KR102943465B1/en active Active
- 2019-10-29 SG SG11202104367RA patent/SG11202104367RA/en unknown
- 2019-10-29 JP JP2021548536A patent/JP7551066B2/en active Active
-
2021
- 2021-04-26 ZA ZA2021/02775A patent/ZA202102775B/en unknown
- 2021-04-29 IL IL282827A patent/IL282827A/en unknown
-
2024
- 2024-08-21 JP JP2024139452A patent/JP2024178163A/en active Pending
Patent Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20110123442A1 (en) * | 2009-10-08 | 2011-05-26 | Pinku Mukherjee | Tumor specific antibodies and uses therefor |
| WO2015069935A1 (en) * | 2013-11-06 | 2015-05-14 | Memorial Sloan-Kettering Cancer Center | Compositions and methods for the treatment of acute myeloid leukemias and myelodysplastic syndromes |
| US20170183413A1 (en) * | 2014-03-19 | 2017-06-29 | Cellectis | Cd123 specific chimeric antigen receptors for cancer immunotherapy |
| WO2017214092A1 (en) * | 2016-06-07 | 2017-12-14 | Macrogenics, Inc. | Combination therapy |
Non-Patent Citations (3)
| Title |
|---|
| "NCBI", Database accession no. NM_000619.2 |
| SAMARAJIWAL, S.A. ET AL.: "INTERFEROME: The Database Of Interferon Regulated Genes", NUCLEIC ACIDS RESEARCH, vol. 37, 2009, pages D852 - D857 |
| See also references of EP3873606A4 |
Cited By (13)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN116209773A (en) * | 2020-06-18 | 2023-06-02 | 宏观基因有限公司 | Use of bispecific CD123x CD3 diabodies for the treatment of hematological malignancies |
| JP2023531201A (en) * | 2020-06-18 | 2023-07-21 | マクロジェニクス,インコーポレーテッド | Use of bispecific CD123xCD3 diabodies for the treatment of hematologic malignancies |
| WO2021257334A1 (en) * | 2020-06-18 | 2021-12-23 | Macrogenics, Inc. | Use of bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies |
| US12274747B2 (en) | 2021-01-28 | 2025-04-15 | Regeneron Pharmaceuticals, Inc. | Compositions and methods for treating cytokine release syndrome |
| WO2022165171A1 (en) | 2021-01-28 | 2022-08-04 | Regeneron Pharmaceuticals, Inc. | Compositions and methods for treating cytokine release syndrome |
| EP4538292A2 (en) | 2021-01-28 | 2025-04-16 | Regeneron Pharmaceuticals, Inc. | Compositions and methods for treating cytokine release syndrome |
| WO2022178243A1 (en) * | 2021-02-20 | 2022-08-25 | Kite Pharma, Inc. | Gene markers for sellecting immunotherapies |
| AU2022223981B2 (en) * | 2021-02-20 | 2025-06-26 | Kite Pharma, Inc. | Gene markers for selecting immunotherapies |
| JP2024507199A (en) * | 2021-02-20 | 2024-02-16 | カイト ファーマ インコーポレイテッド | Genetic markers for choosing immunotherapy |
| WO2023092119A3 (en) * | 2021-11-22 | 2023-06-29 | Ludwig Institute For Cancer Research Ltd | Methods for predicting responsiveness to a cancer therapy |
| WO2023192850A1 (en) * | 2022-03-29 | 2023-10-05 | Ngm Biopharmaceuticals, Inc. | Ilt3 and cd3 binding agents and methods of use thereof |
| WO2023201226A1 (en) | 2022-04-11 | 2023-10-19 | Regeneron Pharmaceuticals, Inc. | Compositions and methods for universal tumor cell killing |
| WO2024173830A2 (en) | 2023-02-17 | 2024-08-22 | Regeneron Pharmaceuticals, Inc. | Induced nk cells responsive to cd3/taa bispecific antibodies |
Also Published As
| Publication number | Publication date |
|---|---|
| CN113286633A (en) | 2021-08-20 |
| BR112021008283A2 (en) | 2021-09-14 |
| JP7551066B2 (en) | 2024-09-17 |
| IL282827A (en) | 2021-06-30 |
| SG11202104367RA (en) | 2021-05-28 |
| AU2019371243A1 (en) | 2021-05-27 |
| ZA202102775B (en) | 2022-03-30 |
| CN119280393A (en) | 2025-01-10 |
| CN119236065A (en) | 2025-01-03 |
| CA3118081A1 (en) | 2020-05-07 |
| KR20210110567A (en) | 2021-09-08 |
| WO2020092404A8 (en) | 2021-05-20 |
| EP3873606A1 (en) | 2021-09-08 |
| EP3873606A4 (en) | 2022-10-26 |
| KR102943465B1 (en) | 2026-03-25 |
| MX2021004868A (en) | 2021-09-08 |
| JP2022513402A (en) | 2022-02-07 |
| JP2024178163A (en) | 2024-12-24 |
| US20210395374A1 (en) | 2021-12-23 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| JP7551066B2 (en) | Bispecific CD123xCD3 Diabodies for the Treatment of Hematological Malignancies - Patent application | |
| AU2023201367B2 (en) | Chimeric receptor T cell treatment using characteristics of the tumor microenvironment | |
| US20090087404A1 (en) | Methods of treating cancer using il-21 and monoclonal antibody therapy | |
| AU2022205653B2 (en) | T cell therapy | |
| Besla et al. | T cell–dependent bispecific therapy enhances innate immune activation and antibody-mediated killing | |
| RU2837616C2 (en) | Bispecific diabodies cd123 x cd3 for treating haematological malignancies | |
| US20230220087A1 (en) | Use of Bispecific CD123 x CD3 Diabodies for the Treatment of Hematologic Malignancies | |
| HK40095144A (en) | Use of bispecific cd123 x cd3 diabodies for the treatment of hematologic malignancies | |
| HK40123134A (en) | Chimeric receptor t cell treatment using characteristics of the tumor microenvironment | |
| HK40011995A (en) | Treatment using chimeric receptor t cells incorporating optimized polyfunctional t cells | |
| HK40044133A (en) | Chimeric receptor t cell treatment using characteristics of the tumor microenvironment | |
| HK1167337A (en) | Methods of treating cancer using il-21 and monoclonal antibody therapy |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 19878838 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: MX/A/2021/004868 Country of ref document: MX |
|
| ENP | Entry into the national phase |
Ref document number: 2021548536 Country of ref document: JP Kind code of ref document: A Ref document number: 3118081 Country of ref document: CA |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| REG | Reference to national code |
Ref country code: BR Ref legal event code: B01A Ref document number: 112021008283 Country of ref document: BR |
|
| ENP | Entry into the national phase |
Ref document number: 20217014961 Country of ref document: KR Kind code of ref document: A |
|
| ENP | Entry into the national phase |
Ref document number: 2019371243 Country of ref document: AU Date of ref document: 20191029 Kind code of ref document: A |
|
| ENP | Entry into the national phase |
Ref document number: 2019878838 Country of ref document: EP Effective date: 20210531 |
|
| REG | Reference to national code |
Ref country code: BR Ref legal event code: B01E Ref document number: 112021008283 Country of ref document: BR Free format text: COM BASE NA PORTARIA 405 DE 21/12/2020, SOLICITA-SE QUE SEJA APRESENTADO, EM ATE 60 (SESSENTA) DIAS, NOVO CONTEUDO DE LISTAGEM DE SEQUENCIA POIS O CONTEUDO APRESENTADO NA PETICAO NO 870210057659 DE 25/06/2021 POSSUI INFORMACOES DIVERGENTES AO PEDIDO EM QUESTAO (DIVERGENCIA DE INVENTOR) |
|
| ENP | Entry into the national phase |
Ref document number: 112021008283 Country of ref document: BR Kind code of ref document: A2 Effective date: 20210429 |
|
| WWG | Wipo information: grant in national office |
Ref document number: 2021114463 Country of ref document: RU |
|
| WWG | Wipo information: grant in national office |
Ref document number: MX/A/2021/004868 Country of ref document: MX |