WO2021189019A1 - Activin receptor type ii chimeras and methods of use thereof - Google Patents
Activin receptor type ii chimeras and methods of use thereof Download PDFInfo
- Publication number
- WO2021189019A1 WO2021189019A1 PCT/US2021/023353 US2021023353W WO2021189019A1 WO 2021189019 A1 WO2021189019 A1 WO 2021189019A1 US 2021023353 W US2021023353 W US 2021023353W WO 2021189019 A1 WO2021189019 A1 WO 2021189019A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- polypeptide
- subject
- seq
- nucleic acid
- vector
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/50—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient the non-active ingredient being chemically bound to the active ingredient, e.g. polymer-drug conjugates
- A61K47/51—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient the non-active ingredient being chemically bound to the active ingredient, e.g. polymer-drug conjugates the non-active ingredient being a modifying agent
- A61K47/68—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient the non-active ingredient being chemically bound to the active ingredient, e.g. polymer-drug conjugates the non-active ingredient being a modifying agent the modifying agent being an antibody, an immunoglobulin or a fragment thereof, e.g. an Fc-fragment
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P11/00—Drugs for disorders of the respiratory system
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P19/00—Drugs for skeletal disorders
- A61P19/08—Drugs for skeletal disorders for bone diseases, e.g. rachitism, Paget's disease
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P19/00—Drugs for skeletal disorders
- A61P19/08—Drugs for skeletal disorders for bone diseases, e.g. rachitism, Paget's disease
- A61P19/10—Drugs for skeletal disorders for bone diseases, e.g. rachitism, Paget's disease for osteoporosis
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P21/00—Drugs for disorders of the muscular or neuromuscular system
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P3/00—Drugs for disorders of the metabolism
- A61P3/04—Anorexiants; Antiobesity agents
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P7/00—Drugs for disorders of the blood or the extracellular fluid
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P7/00—Drugs for disorders of the blood or the extracellular fluid
- A61P7/04—Antihaemorrhagics; Procoagulants; Haemostatic agents; Antifibrinolytic agents
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P7/00—Drugs for disorders of the blood or the extracellular fluid
- A61P7/06—Antianaemics
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K14/00—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- C07K14/435—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- C07K14/705—Receptors; Cell surface antigens; Cell surface determinants
- C07K14/71—Receptors; Cell surface antigens; Cell surface determinants for growth factors; for growth regulators
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K14/00—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- C07K14/435—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- C07K14/76—Albumins
- C07K14/765—Serum albumin, e.g. HSA
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K14/00—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- C07K14/435—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- C07K14/78—Connective tissue peptides, e.g. collagen, elastin, laminin, fibronectin, vitronectin or cold insoluble globulin [CIG]
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12N—MICROORGANISMS OR ENZYMES; COMPOSITIONS THEREOF; PROPAGATING, PRESERVING, OR MAINTAINING MICROORGANISMS; MUTATION OR GENETIC ENGINEERING; CULTURE MEDIA
- C12N15/00—Mutation or genetic engineering; DNA or RNA concerning genetic engineering, vectors, e.g. plasmids, or their isolation, preparation or purification; Use of hosts therefor
- C12N15/09—Recombinant DNA-technology
- C12N15/11—DNA or RNA fragments; Modified forms thereof; Non-coding nucleic acids having a biological activity
- C12N15/62—DNA sequences coding for fusion proteins
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2319/00—Fusion polypeptide
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2319/00—Fusion polypeptide
- C07K2319/30—Non-immunoglobulin-derived peptide or protein having an immunoglobulin constant or Fc region, or a fragment thereof, attached thereto
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2319/00—Fusion polypeptide
- C07K2319/31—Fusion polypeptide fusions, other than Fc, for prolonged plasma life, e.g. albumin
-
- Y—GENERAL TAGGING OF NEW TECHNOLOGICAL DEVELOPMENTS; GENERAL TAGGING OF CROSS-SECTIONAL TECHNOLOGIES SPANNING OVER SEVERAL SECTIONS OF THE IPC; TECHNICAL SUBJECTS COVERED BY FORMER USPC CROSS-REFERENCE ART COLLECTIONS [XRACs] AND DIGESTS
- Y02—TECHNOLOGIES OR APPLICATIONS FOR MITIGATION OR ADAPTATION AGAINST CLIMATE CHANGE
- Y02A—TECHNOLOGIES FOR ADAPTATION TO CLIMATE CHANGE
- Y02A50/00—TECHNOLOGIES FOR ADAPTATION TO CLIMATE CHANGE in human health protection, e.g. against extreme weather
- Y02A50/30—Against vector-borne diseases, e.g. mosquito-borne, fly-borne, tick-borne or waterborne diseases whose impact is exacerbated by climate change
Definitions
- Duchenne muscular dystrophy (DMD), facioscapulohumeral muscular dystrophy (FSHD), inclusion body myositis (IBM), and amyotrophic lateral sclerosis (ALS) are examples of muscle diseases that involve weakness and atrophy of muscles and/or motor neurons that control voluntary muscle movements.
- DMD is caused by mutations in the X-linked dystrophin gene and characterized by progressive muscle degeneration and weakness in all skeletal muscles.
- FSHD particularly affects skeletal muscles of the face, shoulders, upper arms, and lower legs.
- IBM is an inflammatory muscle disease that mainly affects muscles of the thighs and muscles of the arms that control finger and wrist flexion.
- ALS is a motor neuron disease characterized by stiff muscles, muscle twitching, and muscle atrophy throughout the body due to the degeneration of the motor neurons. Efforts to improve treatment and survival of subjects having these devastating muscle diseases have not been successful.
- Healthy bone undergoes a constant remodeling that involves both bone breakdown and bone growth. Bone growth is mediated by the osteoblast cell type whereas the osteoclasts resorb the bone. Pathology occurs when these systems fall out of balance either through downregulation of the anabolic program, upregulation of the catabolic system or a combination of both, resulting in a net bone loss. Therefore, controlling the balance in bone remodeling can be useful for promoting the healing of damage to bone as well as the treatment of disorders, such as osteoporosis, associated with loss of bone mass and bone demineralization.
- Bone damage can result from a range of root causes, including age- or cancer-related bone loss, genetic conditions, or adverse side effects of drug treatment.
- the World Health Organization estimates that osteoporosis alone affects 75 million people in the U.S., Europe, and Japan, and is a significant risk factor in bone damage. In general, the whole of bone loss represents pathological states for which there are few effective treatments. Treatment instead focuses on immobilization, exercise, and dietary modifications rather than agents that directly promote bone growth and increase bone density. With respect to osteoporosis, estrogen, calcitonin, osteocalcin with vitamin K, or high doses of dietary calcium are all used as therapeutic interventions.
- osteoporosis include bisphosphonates, parathyroid hormone, parathyroid hormone related protein, calcimimetics, statins, anabolic steroids, lanthanum and strontium salts, and sodium fluoride. Such therapeutics, however, are often associated with undesirable side effects.
- Fibrosis is the formation of excess connective tissue in an organ or tissue.
- the connective tissue which can form in response to damage (e.g., injury) or as part of an immune response (e.g., an inflammatory response), can disrupt the structure and function of the organ or tissue in which it forms, leading to an increase in tissue stiffness.
- Fibrosis can occur in many organs and tissues within the body, including the lung (e.g., pulmonary fibrosis, cystic fibrosis), liver (e.g., cirrhosis), heart (e.g., endomyocardial fibrosis or fibrosis after myocardial infarction), brain (e.g., glial scar formation), skin (e.g., formation of keloids), kidney (e.g., renal fibrosis), and eye (e.g., corneal fibrosis), among others; and is known to be associated with certain medical treatments (e.g., chemotherapy, radiation therapy, and surgery). There are limited treatment options for patients with fibrosis, and most treatments are focused on improving quality of life or temporarily slowing disease progression.
- certain medical treatments e.g., chemotherapy, radiation therapy, and surgery.
- Anemia is a global health problem with health implications that affect both morbidity and mortality. In the United States alone, the prevalence of anemia nearly doubled from 2003 to 2012. Symptoms of anemia include fatigue, weakness, shortness of breath, heart palpitations, and reduced cognitive performance, and children, pregnant women, women of reproductive age, and the elderly have been found to have the highest risk of developing anemia.
- the most common form of anemia is iron deficiency anemia, but anemia can also be caused by chronic diseases, blood loss, and red blood cell destruction. While iron deficiency anemia can be treated with iron supplements, many other forms of anemia, such as aplastic anemia, anemia of chronic disease, and hemolytic anemia may require blood transfusions.
- thrombocytopenia is a condition characterized by abnormally low levels of platelets, also called thrombocytes, in the blood, and occurs when the bone marrow makes too few platelets or when too many platelets are destroyed or accumulate within an enlarged spleen.
- Patients with thrombocytopenia may experience internal or external bleeding, bleeding under the skin, and/or bruising.
- Treatment for thrombocytopenia depends on its cause and severity and is primarily focused on preventing death or disability caused by bleeding. Certain types of thrombocytopenia (e.g., immune thrombocytopenia) may be treated using corticosteroids, but other types of thrombocytopenia may require splenectomy or platelet transfusion.
- Neutropenia is a condition characterized by an abnormally low number of neutrophils in the blood. Neutrophils typically constitute 45% to 75% of all white blood cells in the bloodstream and serve as the primary defense against infections. Reduced numbers of neutrophils can lead to difficulty in controlling infections and increase the risk of dying from an infection. In patients with severe neutropenia, infections can rapidly become severe or fatal. Antibiotics are used treat infection in patients having neutropenia, but treatments for neutropenia itself are limited, and primarily involve the use of growth factors, such as colony stimulating factors, to stimulate the production of white blood cells. Blood transfusions have not proven effective.
- MDS Myelodysplastic syndromes
- MDS-associated anemia Patients with MDS-associated anemia are generally treated with red blood cell transfusions and erythropoiesis stimulating agents (ESAs), which are not approved for such treatment.
- ESAs erythropoiesis stimulating agents
- MDS-associated thrombocytopenia is treated with platelet transfusions and platelet-stimulating agents.
- Myelofibrosis is an uncommon type of bone marrow cancer that disrupts the normal production of blood cells. It can cause extensive scarring in the bone marrow, leading to severe anemia and a low number of platelets. Symptoms of myelofibrosis include fatigue, bone pain, easy bruising, easy bleeding, and fever. Patients with aggressive or high-risk myelofibrosis may require a blood transfusion or bone marrow transplant.
- Other treatment options include therapies that have known risks, such as androgen therapy and treatment with thalidomide or related medications. For patients with intermediate-risk myelofibrosis, treatment is typically directed at symptom management
- Pulmonary hypertension is a serious condition characterized by higher than normal pressure in the blood vessels between the lungs and the heart.
- PH can be categorized into five major types: arterial (PAH), venous (PH secondary to left-sided heart disease), hypoxic (PH caused by lung disease), thromboembolic (PH caused by chronic arterial obstruction, e.g., blood clots), or miscellaneous (PH with unclear or multifactorial mechanisms), also known as WHO groups l-V.
- PAH features increased pressure in blood vessels of the lungs caused by obstruction in or narrowing of small blood vessels in the lungs due to scarring.
- PAH can be idiopathic (e.g., having no identifiable cause), heritable (e.g., familial, often due to a genetic mutation), or may be related to drug use (e.g., methamphetamine or cocaine use), infection (e.g., HIV infection or schistosomiasis), cirrhosis of the liver, congenital heart abnormalities, or connective tissue/autoimmune disorders (e.g., scleroderma or lupus).
- Treatments for PH include vasodilators, anticoagulants, and supplemental oxygen, but these treatments manage disease symptoms rather than targeting the biological mechanisms that cause the disease.
- Excess body weight is an increasing problem in large parts of the world, with about 39% of adults aged 18 years and over found to be overweight in 2016 and about 13% of the world’s adult population found to be obese. Increased visceral and subcutaneous fact causes dysfunction of various organs. Excessive body weight is a risk factor for an array of complications, including diabetes (e.g., Type 1 and Type 2 diabetes), cardiovascular disease, and several forms of cancer. Insulin resistance is also associated with obesity and results in pancreatic tissues producing an elevated amount of insulin. Once pancreatic b cells can no longer produce sufficient insulin to meet the demand, hyperglycemia occurs and Type 2 diabetes develops. Adipocytes, which are increased in obesity, are believed to play a role in this process. Despite the prevalence of obesity and metabolic diseases few therapeutic options are available.
- the present invention features polypeptides that include an extracellular activin receptor type II (ActRII) chimera.
- a polypeptide of the invention includes an extracellular ActRI I chimera fused to the N- or C-terminus of an Fc domain monomer or another moiety. Such moieties may be attached by amino acid or other covalent bonds and may increase stability of the polypeptide.
- a polypeptide including an extracellular ActRII chimera fused to an Fc domain monomer may also form a dimer (e.g., a homodimer or heterodimer) through the interaction between two Fc domain monomers.
- the polypeptides of the invention may be used to increase lean mass, muscle mass, and/or strength in a subject having or at risk of developing a disease or condition involving weakness and atrophy of muscles, e.g., a neuromuscular disease, sarcopenia, cachexia, disuse atrophy, treatment related muscle loss or atrophy, hypotonia, hypoxia, or muscle loss or atrophy associated with a burn injury.
- a disease or condition involving weakness and atrophy of muscles e.g., a neuromuscular disease, sarcopenia, cachexia, disuse atrophy, treatment related muscle loss or atrophy, hypotonia, hypoxia, or muscle loss or atrophy associated with a burn injury.
- the polypeptides of the invention may also be used to increase bone mass or bone mineral density in a subject having or at risk of developing a disease or condition involving bone damage, e.g., osteoporosis (e.g., primary osteoporosis or secondary osteoporosis), osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, osteogenesis imperfecta, neuromuscular disease-related bone loss, burn-induced bone loss (e.g., bone loss associated with a burn injury), anorexia-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity-related bone loss, or immobility.
- osteoporosis e.g., primary osteoporosis or secondary osteoporosis
- osteopenia e.g., primary osteoporosis or secondary osteoporosis
- osteopenia e.g., osteopetrosis
- the polypeptides of the invention may be used to increase red blood cell levels (e.g., increase hemoglobin levels, increase hematocrit, and/or increase red blood cell count), promote or increase the maturation and/or differentiation of erythroid progenitors, increase late-stage erythroid precursor maturation, or recruit early-stage progenitors into the erythroid lineage in a subject in need thereof, e.g., a subject having or at risk of developing anemia or blood loss, to increase platelet levels (e.g., increase platelet count) in a subject in need thereof, e.g., a subject having or at risk of developing thrombocytopenia, to increase neutrophil levels (e.g., increase neutrophil count) in a subject in need thereof, e.g., a subject having or at risk of developing neutropenia, to prevent or reduce fibrosis in a subject having or at risk of developing fibrosis, or to treat, prevent, or delay the development or progression of pulmonary hypertension
- the polypeptides of the invention may also be used to reduce body weight, reduce body fat, increase glucose clearance, increase insulin sensitivity, or reduce fasting insulin levels in a subject having or at risk of developing a metabolic disease, e.g., obesity, Type 1 diabetes, or Type 2 diabetes.
- a metabolic disease e.g., obesity, Type 1 diabetes, or Type 2 diabetes.
- polypeptides of the invention may also be used to affect myostatin, activin (e.g., activin A and/or activin B), and/or bone morphogenetic protein 9 (BMP9) signaling in a subject having a risk of developing or having a disease or condition involving weakness and atrophy of muscles, bone damage or bone demineralization, low blood cell levels (e.g., low hemoglobin levels, low hematocrit, and/or low red blood cell counts), low platelet levels (e.g., low platelet counts), low neutrophil levels (e.g., low neutrophil counts), fibrosis, pulmonary hypertension (e.g., arterial, venous, hypoxic, thromboembolic, or miscellaneous pulmonary hypertension), or a metabolic disease (e.g., obesity, Type 1 diabetes, or Type 2 diabetes).
- BMP9 bone morphogenetic protein 9
- a polypeptide containing an extracellular ActRI I chimera having a sequence of any one of
- GAILGRAETRECIYYNANWELERTNQSGLERCEGEQXiKRRHCFATWKNISGSIEIVKQGCWLD DX2X3CYDRTDCVX4X5X6X7X8PX9VYFCCCEGNMCNEKFSYFPEMEVTQPTS (SEQ ID NO: 1), GAILGRAETRECIYYNANWELERTNQSGLERCEGEQX1KRLHCFATWKNISGSIEIVKQGCWLDD X2X3CYDRTDCVX4X5X6X7X8PX9VYFCCCEGNMCNEKFSYFPEMEVTQPTS (SEQ ID NO: 2), GAILGRAETRECIYYNANWELERTNQSGLERCEGEQX1KRLHCYASWKNISGSIEIVKQGCWLDD X 2 X3CYDRTDCVX 4 X5X6X7X8PX9VYFCCCEGNMCNEKFSYFPEMEVTQPTS (SEQ
- GRGEAETRECIYYNANWELERTNQSGLERCEGEQX 1 KRLHCYASWRNSSGTIELVKKGCWLDD X 2 X3CYDRQECVX 4 X5X6X7X8PX9VYFCCCEGNMCNEKFSYFPEMEVTQPTS (SEQ ID NO: 14), in which Xi is D or R, X 2 is I, F, E, D, Y, S, N, Q, or T, X 3 is N or T, X 4 is A or E, X 5 is T or K, X 6 is E or K, X7 is E or D, Xs is N or S, and Xg is Q, E, K, R, D, or N, optionally wherein the chimera is truncated from the N-terminus by deletion of 1 , 2, 3, 4, 5, 6, 7, 8, or 9 amino acids, wherein the chimera retains the two amino acids before the first cysteine.
- a polypeptide containing an extracellular ActRI I chimera having a sequence of any one of
- E24 The polypeptide of any one of E1 -E23, wherein Xi is D.
- E25 The polypeptide of any one of E1 -E23, wherein Xi is R.
- E26 The polypeptide of any one of E1-E25, wherein X2 is I.
- E27 The polypeptide of any one of E1 -E25, wherein X2 is F.
- E28 The polypeptide of any one of E1 -E25, wherein X2 is E.
- E29 The polypeptide of any one of E1 -E25, wherein X2 is D.
- E30 The polypeptide of any one of E1 -E25, wherein X2 is Y.
- E31 The polypeptide of any one of E1 -E25, wherein X2 is S.
- E32 The polypeptide of any one of E1-E25, wherein X2 is N.
- E33 The polypeptide of any one of E1 -E25, wherein X2 is Q.
- E34 The polypeptide of any one of E1 -E25, wherein X2 is T.
- E35 The polypeptide of any one of E1-E34, wherein X3 is N.
- E36 The polypeptide of any one of E1 -E34, wherein X3 is T.
- E37 The polypeptide of any one of E1 -E36, wherein X4 is A.
- E38 The polypeptide of any one of E1 -E36, wherein X4 is E.
- E39 The polypeptide of any one of E1 -E38, wherein X5 is T.
- E40 The polypeptide of any one of E1 -E38, wherein X5 is K.
- E41 The polypeptide of any one of E1 -E40, wherein Cb is E.
- E42 The polypeptide of any one of E1 -E40, wherein Cb is K.
- E43 The polypeptide of any one of E1 -E42, wherein X7 is E.
- E44 The polypeptide of any one of E1 -E42, wherein X7 is D.
- E45 The polypeptide of any one of E1-E44, wherein Xs is N.
- E46 The polypeptide of any one of E1 -E44, wherein Xs is S.
- E47 The polypeptide of any one of E1 -E46, wherein Xg is Q.
- E48 The polypeptide of any one of E1 -E46, wherein Xg is E.
- E49 The polypeptide of any one of E1 -E46, wherein Xg is K.
- E50 The polypeptide of any one of E1 -E46, wherein Xg is R.
- E51 The polypeptide of any one of E1 -E46, wherein Xg is D.
- E52 The polypeptide of any one of E1-E46, wherein Xg is N.
- E53 The polypeptide of any one of E1-E52, wherein X5 is T, Cb is E, X7IS E, and Xsis N.
- E54 The polypeptide of any one of E1-E52, wherein X5 is T, Cb is K, X7IS E, and Xsis N.
- E55 The polypeptide of any one of E1 -E54, wherein X2 is E and X3 is T.
- E56 The polypeptide of any one of E1-E54, wherein X2 IS I or F and X3 IS N.
- E58 The polypeptide of E56, wherein X2 is F.
- E59 The polypeptide of E1 or E2, wherein the chimera has the sequence of any one of SEQ ID NOs: 22-43.
- E60 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 22.
- E61 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 23.
- E62 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 24.
- E63 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 25.
- E64 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 40.
- E65 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 41.
- E66 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 28.
- E67 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 42.
- E68 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 43.
- E69 The polypeptide of E59, wherein the chimera has the sequence of SEQ ID NO: 37.
- E70 The polypeptide of any one of E1-E69, wherein the chimera is truncated from the N-terminus by deletion of one amino acid.
- E71 The polypeptide of any one of E1-E69, wherein the chimera is truncated from the N-terminus by deletion of two amino acids.
- E72 The polypeptide of any one of E1-E69, wherein the chimera is truncated from the N-terminus by deletion of three amino acids.
- E73 The polypeptide of any one of E1-E69, wherein the chimera is truncated from the N-terminus by deletion of four amino acids.
- E74 The polypeptide of any one of E1-E69, wherein the chimera is truncated from the N-terminus by deletion of five amino acids.
- E75 The polypeptide of any one of E1-E69, wherein the chimera is truncated from the N-terminus by deletion of six amino acids.
- E76 The polypeptide of any one of E1-E69, wherein the chimera is truncated from the N-terminus by deletion of seven amino acids.
- E77 The polypeptide of any one of E1-E69, wherein the chimera is truncated from the N-terminus by deletion of eight amino acids.
- E78 The polypeptide of any one of E1-E69, wherein the chimera is truncated from the N-terminus by deletion of nine amino acids.
- E79 The polypeptide of any one of E1 , E2, and E70-E78, wherein the chimera has the sequence of any one of SEQ ID NOs: 111-183.
- E80 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 111.
- E81 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 116.
- E82 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 117.
- E83 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 118.
- E84 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 119.
- E85 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 120.
- E86 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 121.
- E87 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 122.
- E88 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 126.
- E89 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 130.
- E90 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 142.
- E91 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 143.
- E92 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 146.
- E93 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 147.
- E94 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 150.
- E95 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 151.
- E96 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 152.
- E97 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 153.
- E98 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 154.
- E99 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 155.
- E100 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 156.
- E101 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 158.
- E102 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 159.
- E103 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 162.
- E104 The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 163.
- E105. The polypeptide of E79, wherein the chimera has the sequence of SEQ ID NO: 164.
- E106 The polypeptide of any one of E1-E105, wherein the polypeptide (e.g., the chimera) further includes a C-terminal extension of one or more amino acids (e.g., 1 , 2, 3, 4, 5, 6, or more amino acids from wild-type extracellular ActRIIA or ActRIIB).
- the polypeptide e.g., the chimera
- a C-terminal extension of one or more amino acids e.g., 1 , 2, 3, 4, 5, 6, or more amino acids from wild-type extracellular ActRIIA or ActRIIB.
- E107 The polypeptide of E106, wherein the C-terminal extension is NP.
- E108 The polypeptide of E106, wherein the C-terminal extension is NPVTPK (SEQ ID NO: 104).
- E109 The polypeptide of any one of E1-E108, wherein the polypeptide further includes an Fc domain monomer fused to the C-terminus of the polypeptide (e.g., the C-terminus of the chimera) by way of a linker.
- E110 The polypeptide of E109, wherein the Fc domain monomer has the sequence of SEQ ID NO: 48.
- E111 The polypeptide of E109 or E110, wherein the polypeptide forms a dimer.
- E112 The polypeptide of any one of E1-E108, wherein the polypeptide further includes a wild-type Fc domain fused to the C-terminus of the polypeptide (e.g., the C-terminus of the chimera) by way of a linker.
- E113 The polypeptide of E112, wherein the wild-type Fc domain has the sequence of SEQ ID NO: 100 or SEQ ID NO: 264.
- E114 The polypeptide of E112 or E113, wherein the polypeptide has the sequence of any one of SEQ ID NOs: 107-110 and SEQ ID NOs: 184-263.
- E115 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 107.
- E116 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 108.
- E117 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 109.
- E118 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 110.
- E119 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 184.
- E120 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 189.
- E121 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 190.
- E122 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 191.
- E123 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 192.
- E124 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 193.
- E125 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 194.
- E126 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 195.
- E127 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 199.
- E128 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 200.
- E129 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 213.
- E130 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 214.
- E132 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 216.
- E133 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 217.
- E134 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 218.
- E136 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 222.
- E137 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 225.
- E138. The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 226.
- E140 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 230.
- E141 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 231.
- E142 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 232.
- E143 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 233.
- E144 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 234.
- E145 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 235.
- E146 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 236.
- E147 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 237.
- E148 The polypeptide of E114, wherein the polypeptide has the sequence of SEQ ID NO: 238.
- E149 The polypeptide of any one of E1-E108, wherein the polypeptide further includes an Fc domain containing amino acid substitutions fused to the C-terminus of the polypeptide (e.g., the C- terminus of the chimera) by way of a linker.
- E150 The polypeptide of E149, wherein the Fc domain does not form a dimer.
- E151 The polypeptide of any one of E1-E108, wherein the polypeptide further includes an albuminbinding peptide fused to the C-terminus of the polypeptide (e.g., the C-terminus of the chimera) by way of a linker.
- an albuminbinding peptide fused to the C-terminus of the polypeptide (e.g., the C-terminus of the chimera) by way of a linker.
- E152 The polypeptide of E151 , wherein the albumin-binding peptide has the sequence of SEQ ID NO: 101.
- E153 The polypeptide of any one of E1-E108, wherein the polypeptide further includes a fibronectin domain fused to the C-terminus of the polypeptide (e.g., the C-terminus of the chimera) by way of a linker.
- E154 The polypeptide of E153, wherein the fibronectin domain has the sequence of SEQ ID NO: 102.
- E155 The polypeptide of any one of E1-E108, wherein the polypeptide further includes a human serum albumin fused to the C-terminus of the polypeptide (e.g., the C-terminus of the chimera) by way of a linker.
- a human serum albumin fused to the C-terminus of the polypeptide (e.g., the C-terminus of the chimera) by way of a linker.
- E156 The polypeptide of E155, wherein the human serum albumin has the sequence of SEQ ID NO: 103.
- E157 The polypeptide of any one of E109-E156, wherein the linker is an amino acid spacer.
- E158 The polypeptide of E157, wherein the amino acid spacer is GGG, GGGA (SEQ ID NO: 49),
- GGGG (SEQ ID NO: 51), GGGAG (SEQ ID NO: 81), GGGAGG (SEQ ID NO: 82), or GGGAGGG (SEQ ID NO: 83).
- E159 The polypeptide of E157, wherein the amino acid spacer is GA, GS, GG, GGA, GGS, GGGS
- SEQ ID NO: 50 GGGGA (SEQ ID NO: 52), GGGGS (SEQ ID NO: 53), GGGGG (SEQ ID NO: 54), GGAG (SEQ ID NO: 55), GGSG (SEQ ID NO: 56), AGGG (SEQ ID NO: 57), SGGG (SEQ ID NO: 58), GAGA (SEQ ID NO: 59), GSGS (SEQ ID NO: 60), GAGAGA (SEQ ID NO: 61),
- GSGSGS (SEQ ID NO: 62), GAGAGAGA (SEQ ID NO: 63), GSGSGSGS (SEQ ID NO: 64), GAGAGAGAGA (SEQ ID NO: 65), GSGSGSGSGS (SEQ ID NO: 66), GAGAGAGAGAGA (SEQ ID NO: 67), GSGSGSGSGSGS (SEQ ID NO: 68), GGAGGA (SEQ ID NO: 69), GGSGGS (SEQ ID NO: 70), GGAGGAGGA (SEQ ID NO: 71), GGSGGSGGS (SEQ ID NO: 72), GGAGGAGGAGGA (SEQ ID NO: 73), and GGSGGSGGSGGS (SEQ ID NO: 74), GGAGGGAG (SEQ ID NO: 75), GGSGGGSG (SEQ ID NO: 76), GGAGGGAGGGAG (SEQ ID NO: 77), and GGSGGGSGGGSG (SEQ ID NO: 78), GGGGAGGGGAGGGGA (SEQ
- E160 The polypeptide of any one of E1-E159, wherein the polypeptide (e.g., an ActRII chimera-Fc fusion protein) has a serum half-life of at least seven days.
- the polypeptide e.g., an ActRII chimera-Fc fusion protein
- E161 The polypeptide of any one of E1-E160, wherein the polypeptide has increased binding to one or more an ActRII ligands (e.g., activin A, activin B, myostatin, and/or GDF-11) compared to wild- type ActRIIA and/or wild-type ActRIIB (e.g., wild-type extracellular ActRIIA and/or ActRIIB).
- an ActRII ligands e.g., activin A, activin B, myostatin, and/or GDF-11
- wild-type ActRIIA and/or wild-type ActRIIB e.g., wild-type extracellular ActRIIA and/or ActRIIB.
- E162 The polypeptide of any one of E1 -E161 , wherein the polypeptide has decreased binding to bone morphogenetic protein 9 (BMP9, e.g., human BMP9) compared to wild-type ActRIIB (e.g., wild- type extracellular ActRIIB).
- BMP9 bone morphogenetic protein 9
- wild-type ActRIIB e.g., wild- type extracellular ActRIIB
- E163 The polypeptide of any one of E1-E162, wherein the polypeptide binds to activin A, activin B, and/or myostatin and has reduced or weak binding to human BMP9 (e.g., compared to wild-type extracellular ActRIIB).
- E164 The polypeptide of any one of E1-E163, wherein the polypeptide does not substantially bind to human BMP9.
- E165 The polypeptide of any one of E1-E164, wherein the polypeptide binds to human activin A with a KD of 800 pM or less.
- E166 The polypeptide of any one of E1-E165, wherein the polypeptide binds to human activin B with a KD of 800 pM or less.
- E167 The polypeptide of any one of E1-E166, wherein the polypeptide binds to human GDF-11 with a KD of 5 pM or higher.
- E168 A nucleic acid molecule encoding the polypeptide of any one of E1-E167.
- E169 A vector including the nucleic acid molecule of E168.
- E170 A host cell that expresses the polypeptide of any one of E1 -E167, wherein the host cell includes the nucleic acid molecule of E168 or the vector of E169, wherein the nucleic acid molecule or vector is expressed in the host cell.
- E171. A method of preparing the polypeptide of any one of E1-E167, wherein the method includes: a) providing a host cell containing the nucleic acid molecule of E168 or the vector of E169, and b) expressing the nucleic acid molecule or vector in the host cell under conditions that allow for the formation of the polypeptide.
- E172. A pharmaceutical composition including the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, or the vector of E169 and one or more pharmaceutically acceptable carriers or excipients.
- E173 The pharmaceutical composition of E172, wherein the polypeptide, nucleic acid molecule, or vector is in a therapeutically effective amount.
- E174 A construct including two identical polypeptides (e.g., a homodimer), each including an extracellular ActRI I chimera of any one of E1-E108 (e.g., an ActRII chimera having a sequence of any one of SEQ ID NOs: 1 -43 and 111-183) fused to the N- or C-terminus of an Fc domain monomer (e.g., the sequence of SEQ ID NO: 48).
- the two Fc domain monomers in the two polypeptides interact to form an Fc domain in the construct.
- a construct including two different polypeptides e.g., a heterodimer
- each including an extracellular ActRII chimera of any one of E1-E108 e.g., an ActRII chimera having a sequence of any one of SEQ ID NOs: 1 -43 and 111-183 fused to the N- or C-terminus of an Fc domain monomer (e.g., the sequence of SEQ ID NO: 48).
- the two Fc domain monomers in the two polypeptides interact to form an Fc domain in the construct.
- E176 A method of increasing lean mass in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of increasing muscle mass in a subject in need thereof comprising administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E178 A method of increasing muscle strength in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E179 The method of any one of E176-E178, wherein the subject has or is at risk of developing a neuromuscular disease, sarcopenia, cachexia, disuse atrophy, treatment-related muscle loss or atrophy, hypotonia, muscle loss or atrophy associated with hypoxia, or muscle loss or atrophy associated with a burn injury.
- E180 A method of treating a subject having or at risk of developing muscle disease, comprising administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E181. The method of E180, wherein the muscle disease is a neuromuscular disease, sarcopenia, cachexia, disuse atrophy, treatment-related muscle loss or atrophy, hypotonia, muscle loss or atrophy associated with hypoxia, or muscle loss or atrophy associated with a burn injury.
- the muscle disease is a neuromuscular disease, sarcopenia, cachexia, disuse atrophy, treatment-related muscle loss or atrophy, hypotonia, muscle loss or atrophy associated with hypoxia, or muscle loss or atrophy associated with a burn injury.
- a method of affecting myostatin, activin A, activin B, and/or BMP9 signaling e.g., reducing or inhibiting the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors
- method includes administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E183 The method of E182, wherein the disease or condition is a neuromuscular disease, sarcopenia, cachexia, disuse atrophy, treatment-related muscle loss or atrophy, hypotonia, muscle loss or atrophy associated with hypoxia, or muscle loss or atrophy associated with a burn injury.
- E184 A method of treating a subject having or at risk of developing a neuromuscular disease, comprising administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E185 The method of any one of E179, E181 , and E183, wherein the subject has or is at risk of developing a neuromuscular disease or wherein the disease or condition is a neuromuscular disease.
- E186 A method of treating a subject having or at risk of developing DMD by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E187 A method of treating a subject having or at risk of developing FSHD by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E188 A method of treating a subject having or at risk of developing IBM by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E189 A method of treating a subject having or at risk of developing ALS by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E190 The method of any one of E179, E181 , and E183, wherein the subject has or is at risk of developing sarcopenia or wherein the disease or condition is sarcopenia.
- a method of treating a subject having or at risk of developing sarcopenia by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E192 The method of any one of E179, E181 , and E183, wherein the subject has or is at risk of developing disuse atrophy or wherein the disease or condition is disuse atrophy.
- a method of treating a subject having or at risk of developing disuse atrophy by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E194 The method of any one of E179, E181 , and E183, wherein the subject has or is at risk of developing treatment-related muscle loss or atrophy or wherein the disease or condition is treatment-related muscle loss or atrophy.
- E195 A method of treating a subject having or at risk of developing treatment-related muscle loss or atrophy by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E196 The method of any one of E179, E181 , E183, E194, and E195, wherein the treatment is glucocorticoid treatment, FGF-21 treatment, GLP-1 treatment, treatment with an FGF-21- or GLP- 1-containing therapeutic, bariatric surgery (e.g., gastric bypass), cancer therapy (e.g., chemotherapy or radiation), or treatment for obesity or Type 2 diabetes.
- the treatment is glucocorticoid treatment, FGF-21 treatment, GLP-1 treatment, treatment with an FGF-21- or GLP- 1-containing therapeutic, bariatric surgery (e.g., gastric bypass), cancer therapy (e.g., chemotherapy or radiation), or treatment for obesity or Type 2 diabetes.
- E197 The method of any one of E179, E181 , and E183, wherein the subject has or is at risk of developing hypotonia or wherein the disease or condition is hypotonia.
- E198 A method of treating a subject having or at risk of developing hypotonia by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E199 The method of any one of E179, E181 , and E183, wherein the subject has or is at risk of developing muscle loss or atrophy associated with hypoxia or wherein the disease or condition is muscle loss or atrophy associated with hypoxia.
- E200 A method of treating a subject having or at risk of developing muscle loss or atrophy associated with hypoxia by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E201 The method of any one of E179, E181 , and E183, wherein the subject has or is at risk of developing muscle loss or atrophy associated with a burn injury or wherein the disease or condition is muscle loss or atrophy associated with a burn injury.
- E202 A method of treating a subject having or at risk of developing muscle loss or atrophy associated with a burn injury by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E203 The method of any one of E179, E181 , and E183, wherein the subject has or is at risk of developing cachexia or wherein the disease or condition is cachexia.
- E204 A method of treating a subject having or at risk of developing cachexia by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E205 The method of any one of E179, E181 , E183, E203, and E204, wherein the cachexia is cancer cachexia, HIV-related cachexia, cardiac cachexia (e.g., cachexia associated with heart failure), cachexia associated with chronic kidney disease, or pulmonary cachexia (e.g., cachexia associated with COPD).
- the cachexia is cancer cachexia, HIV-related cachexia, cardiac cachexia (e.g., cachexia associated with heart failure), cachexia associated with chronic kidney disease, or pulmonary cachexia (e.g., cachexia associated with COPD).
- E206 The method of any one of E176-E205, wherein the method increases muscle mass.
- E207 The method of any one of E176-E206, wherein the method increases lean mass.
- E208 The method of any one of E176-E207, wherein the method increases muscle strength.
- E209 A method of increasing bone mineral density in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E210 A method of reducing bone resorption in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of increasing bone formation in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E212 A method of increasing bone strength in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of reducing the risk or occurrence of bone fracture in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E214 The method of any one of E209-E213, wherein the subject has or is at risk of developing osteoporosis, osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, osteogenesis imperfecta, neuromuscular disease-related bone loss, burn-induced bone loss, anorexia-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity- related bone loss, or immobility-related bone loss.
- a method of treating a subject having or at risk of developing bone disease by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E216 The method of E215, wherein the bone disease is osteoporosis, osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, osteogenesis imperfecta, neuromuscular disease- related bone loss, burn-induced bone loss, anorexia-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity-related bone loss, or immobility- related bone loss.
- Paget’s disease is osteoporosis, osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, osteogenesis imperfecta, neuromuscular disease- related bone loss, burn-induced bone loss, anorexia-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity-related bone loss, or immobility- related bone loss.
- a method of affecting myostatin, activin A, activin B, and/or BMP9 signaling e.g., reducing or inhibiting the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors
- E218 The method of E217, wherein the disease or condition is osteoporosis, osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, osteogenesis imperfecta, neuromuscular disease- related bone loss, burn-induced bone loss, anorexia-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity-related bone loss, or immobility- related bone loss.
- the disease or condition is osteoporosis, osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, osteogenesis imperfecta, neuromuscular disease- related bone loss, burn-induced bone loss, anorexia-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity-related bone loss, or immobility- related bone loss.
- E219. The method of any one of E214, E216, or E218, wherein the subject has or is at risk of developing osteoporosis or wherein the disease or condition is osteoporosis.
- E220 A method of treating a subject having or at risk of developing osteoporosis by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E22 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing osteogenesis imperfecta or wherein the disease or condition is osteogenesis imperfecta.
- E222 A method of treating a subject having or at risk of developing osteogenesis imperfecta by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E223. The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing osteopenia or wherein the disease or condition is osteopenia.
- E224 A method of treating a subject having or at risk of developing osteopenia by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E225 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing a bone fracture or wherein the disease or condition is bone fracture.
- E226 A method of treating a subject having or at risk of developing a bone fracture by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E227 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing bone cancer or cancer metastasis-related bone loss or wherein the disease or condition is bone cancer or cancer metastasis-related bone loss.
- E228 A method of treating a subject having or at risk of developing bone cancer or cancer metastasis- related bone loss by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E229. The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing Paget’s disease or wherein the disease or condition is Paget’s disease.
- E230 A method of treating a subject having or at risk of developing Paget’s disease by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E23 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing renal osteodystrophy or wherein the disease or condition is renal osteodystrophy.
- E232 A method of treating a subject having or at risk of developing renal osteodystrophy by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E233 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing treatment-related bone loss or wherein the disease or condition is treatment-related bone loss.
- a method of treating a subject having or at risk of developing treatment-related bone loss by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E235 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing diet-related bone loss or wherein the disease or condition is diet-related bone loss.
- E236 A method of treating a subject having or at risk of developing diet-related bone loss by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E237 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing low gravity-related bone loss or wherein the disease or condition is low gravity-related bone loss.
- E238 A method of treating a subject having or at risk of developing low gravity-related bone loss by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E239. The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing immobility-related bone loss or wherein the disease or condition is immobility-related bone loss.
- E240 A method of treating a subject having or at risk of developing immobility-related bone loss by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E241 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing neuromuscular disease-related bone loss or wherein the disease or condition is neuromuscular disease-related bone loss.
- a method of treating a subject having or at risk of developing neuromuscular disease-related bone loss by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E243 The method of any one of E179, E181 , E183-E185, E214, E216, E218, E241 , and E242, wherein the neuromuscular disease is a muscular dystrophy, amyotrophic lateral sclerosis (ALS), autonomic neuropathy, botulism, Charcot-Marie-Tooth disease (CMT), chronic inflammatory demyelinating polyradiculoneuropathy, congenital myasthenic syndrome, a congenital myopathy, cramp-fasciculation syndrome, dermatomyositis, diabetic neuropathy, a distal myopathy, a dystrophinopathy, an endocrine myopathy, a focal muscular atrophy, glycogen storage disease type II, Guillain-Barre syndrome, hereditary spastic paraplegia, inclusion body myositis (IBM), Isaac’s syndrome, Kearns-Sayre syndrome, Kennedy disease, Lambert-Eaton myasthenic syndrome, a metabolic myopathy, a metabolic neuro
- E244 The method of E243, wherein the neuromuscular disease is a muscular dystrophy.
- E245. The method of E244, wherein the muscular dystrophy is Duchenne muscular dystrophy (DMD), facioscapulohumeral muscular dystrophy (FSHD), Becker muscular dystrophy (BMD), myotonic dystrophy (DM), congenital muscular dystrophy, limb-girdle muscular dystrophy (LGMD), distal muscular dystrophy (DD), oculopharyngeal muscular dystrophy (OPMD), or Emery-Dreifuss muscular dystrophy (EDMD).
- DMD Duchenne muscular dystrophy
- FSHD facioscapulohumeral muscular dystrophy
- BMD Becker muscular dystrophy
- DM myotonic dystrophy
- congenital muscular dystrophy limb-girdle muscular dystrophy
- LGMD distal muscular dystrophy
- OPMD oculopharyngeal muscular dystrophy
- EDMD Emery-Dreifuss muscular dystrophy
- E246 The method of E245, wherein the muscular dystrophy is DMD.
- E247 The method of E245, wherein the muscular dystrophy is FSHD.
- E248 The method of E245, wherein the muscular dystrophy is BMD.
- E249 The method of E245, wherein the muscular dystrophy is DM.
- E250 The method of E245, wherein the muscular dystrophy is LGMD.
- E251 The method of E245, wherein the muscular dystrophy is DD.
- E252 The method of E245, wherein the muscular dystrophy is OPMD.
- E253 The method of E245, wherein the muscular dystrophy is EDMD.
- E254 The method of E245, wherein the muscular dystrophy is a congenital muscular dystrophy.
- E255 The method of E254, wherein the congenital muscular dystrophy is congenital muscular dystrophy type 1A (MDC1A), congenital muscular dystrophy type 1C (MDC1C), congenital muscular dystrophy type 1D (MDC1D), congenital muscular dystrophy type 1B (MDC1B), Fukuyama congenital muscular dystrophy (FCMD), muscle-eye-brain disease (MEB), Walker- Warburg Syndrome (WWS), rigid spine muscular dystrophy (RSMD1), Ullrich congenital muscular dystrophy (UCMD), or muscular dystrophy associated with a mutation in integrin alpha 7, integrin alpha 9, docking protein 7, laminin A/C, SECIS binding protein 2, or choline kinase beta.
- MDC1A congenital muscular dystrophy type 1A
- MDC1C congenital muscular dystrophy type 1C
- MDC1D congenital muscular dystrophy type 1D
- MDC1B congenital muscular dystrophy type
- E256 The method of E255, wherein the congenital muscular dystrophy is MDC1 A.
- E257 The method of E255, wherein the congenital muscular dystrophy is MDC1 B.
- E258 The method of E255, wherein the congenital muscular dystrophy is MDC1 C.
- E260 The method of E255, wherein the congenital muscular dystrophy is FCMD.
- E261. The method of E255, wherein the congenital muscular dystrophy is MEB.
- E262. The method of E255, wherein the congenital muscular dystrophy is WWS.
- E263. The method of E255, wherein the congenital muscular dystrophy is RSMD1.
- E264 The method of E255, wherein the congenital muscular dystrophy is UCMD.
- E265. The method of E243, wherein the neuromuscular disease is CMT.
- E266 The method of E243, wherein the neuromuscular disease is ALS.
- E267 The method of E243, wherein the neuromuscular disease is SMA.
- E268 The method of E243, wherein the neuromuscular disease is IBM.
- E269. The method of E243, wherein the neuromuscular disease is myasthenia gravis.
- E270 The method of E243, wherein the neuromuscular disease is multiple sclerosis.
- E27 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing burn-induced bone loss or wherein the disease or condition is burn-induced bone loss.
- a method of treating a subject having or at risk of developing burn-induced bone loss by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E273 The method of any one of E214, E216, and E218, wherein the subject has or is at risk of developing anorexia-related bone loss or wherein the disease or condition is anorexia-related bone loss.
- a method of treating a subject having or at risk of developing anorexia-related bone loss by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E275 The method of any one of E214, E216, and E218-E220, wherein the osteoporosis is primary osteoporosis.
- E276 The method of E275, wherein the primary osteoporosis is age-related osteoporosis or hormone-related osteoporosis.
- E277 The method of any one of E214, E216, and E218-E220, wherein the osteoporosis is secondary osteoporosis.
- E278 The method of E277, wherein the secondary osteoporosis is immobilization-induced osteoporosis or glucocorticoid-induced osteoporosis.
- E280 The method of any one of E214, E216, E218, E233, and E234, wherein the treatment is FGF-21 treatment, GLP-1 treatment, treatment with an FGF-21- or GLP-1 -containing therapeutic, cancer therapy (e.g., chemotherapy or radiation), bariatric surgery (e.g., gastric bypass), androgen or estrogen deprivation therapy, or treatment for obesity or Type 2 diabetes.
- cancer therapy e.g., chemotherapy or radiation
- bariatric surgery e.g., gastric bypass
- androgen or estrogen deprivation therapy e.g., or treatment for obesity or Type 2 diabetes.
- E281 The method of any one of E214, E216, E218, E235, and E236, wherein the diet-related bone loss is rickets.
- E282 The method of any one of E209-E281 , wherein the subject is at risk of bone fracture.
- E283 The method of any one of E209-E282, wherein the method increases bone formation in the subject.
- E284 The method of any one of E209-E283, wherein the method decreases bone resorption in the subject.
- E285. The method of any one of E209-E284, wherein the method decreases bone loss in the subject.
- E286 The method of any one of E209-E285, wherein the method increases osteoblast activity or osteoblastogenesis.
- E287 The method of any one of E209-E286, wherein the method decreases osteoclast activity or decreases osteoclastogenesis.
- E288 The method of any one of E209-E287, wherein the method decreases the risk or occurrence of bone fracture.
- E289. The method of any one of E209-E288, wherein the method increases bone strength.
- E290 The method of any one of E209-E289, wherein the bone is cortical bone.
- a method of decreasing or preventing fibrosis in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of slowing or inhibiting the progression of fibrosis in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of reducing the risk of developing fibrosis in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E295. A method of treating a subject having or at risk of developing fibrosis by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E296. A method of reversing fibrosis in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E297 A method of affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing fibrosis or a disease or condition involving fibrosis by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E298 The method of any one of E292-E297, wherein the fibrosis or the disease or condition involving fibrosis is chemotherapeutic drug-induced fibrosis, radiation-induced fibrosis, pulmonary fibrosis, hepatic fibrosis, renal fibrosis (e.g., fibrosis related to chronic kidney disease), corneal fibrosis, heart fibrosis, bone marrow fibrosis, myelofibrosis, mediastinal fibrosis, retroperitoneal fibrosis, arthrofibrosis, osteoarticular fibrosis, tissue fibrosis, a tumor stroma, a desmoplastic tumor, a surgical adhesion, a hypertrophic scar, or a keloid.
- chemotherapeutic drug-induced fibrosis e.g., radiation-induced fibrosis, pulmonary fibrosis, hepatic fibrosis, renal fibrosis (e.g., fibro
- E299. The method of any one of E292-E297, wherein the fibrosis or the disease or condition involving fibrosis is fibrosis associated with a wound, a burn, hepatitis B or C infection, fatty liver disease, Schistosoma infection, kidney disease (e.g., chronic kidney disease), heart disease, macular degeneration, Crohn’s disease, retinal or vitreal retinopathy, systemic or local scleroderma, atherosclerosis, or restenosis.
- kidney disease e.g., chronic kidney disease
- heart disease e.g., macular degeneration, Crohn’s disease
- retinal or vitreal retinopathy e.g., systemic or local scleroderma, atherosclerosis, or restenosis.
- E300 The method of any one of E292-E298, wherein the fibrosis results from chronic kidney disease.
- E301 The method of any one of E292-E298, wherein the fibrosis is myelofibrosis.
- tissue fibrosis is fibrosis affecting a tissue selected from the group consisting of muscle tissue, skin epidermis, skin dermis, tendon, cartilage, pancreatic tissue, uterine tissue, neural tissue, testis, ovary, adrenal gland, artery, vein, bone marrow, colon, small intestine, large intestine, biliary tract, and gut.
- E303 The method of any one of E292-E302, wherein the method improves the function of a fibrotic tissue or organ.
- E304 The method of any one of E292-E303, wherein the method slows, inhibits, or reverses the development or progression of fibrosis.
- E305 The method of any one of E292-E304, wherein the method reduces (e.g., reduces the frequency or severity of) one or more symptom of fibrosis.
- a method of increasing red blood cell levels e.g., increasing hemoglobin levels, red blood cell count, or hematocrit
- a method of increasing red blood cell levels e.g., increasing hemoglobin levels, red blood cell count, or hematocrit
- administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of increasing hemoglobin levels in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of increasing red blood cell count in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E309 A method of increasing hematocrit in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E310 A method of promoting or increasing red blood cell production in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- erythroid progenitors e.g., early-stage or late- (e.g., terminal) stage erythroid progenitors, e.g., the maturation and/or differentiation of early-stage erythroid progenitors, such as colony forming unit-erythroid cells (CFU-Es) and burst forming unit-erythroid cells (BFU-Es), into proerythroblasts, reticulocytes, or red blood cells
- CFU-Es colony forming unit-erythroid cells
- BFU-Es burst forming unit-erythroid cells
- a method of promoting or increasing proerythroblasts e.g., proerythroblast numbers or proerythroblast count
- a method of promoting or increasing reticulocytes in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of promoting or increasing the recruitment of early-stage progenitors into the erythroid lineage in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of promoting or increasing late-stage erythroid precursor maturation e.g., terminal maturation, such as the maturation of reticulocytes into red blood cells or the maturation of erythroblasts into reticulocytes and/or red blood cells
- a method of promoting or increasing late-stage erythroid precursor maturation e.g., terminal maturation, such as the maturation of reticulocytes into red blood cells or the maturation of erythroblasts into reticulocytes and/or red blood cells
- E316 e.g., terminal maturation, such as the maturation of reticulocytes into red blood cells or the maturation of erythroblasts into reticulocytes and/or red blood cells
- a method of reducing the accumulation of red blood cell progenitor cells in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E317 A method of increasing the number of early-stage erythroid precursors and/or progenitors (e.g., expanding the early-stage precursor and/or progenitor population) in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E318 A method of promoting the progression of erythroid precursors and/or progenitors through erythropoiesis in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E319. The method of any one of E306-E318, wherein the subject has or is at risk of developing anemia or blood loss.
- E320 A method of affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing a disease or condition involving low red blood cell levels (e.g., low hemoglobin levels, low red blood cell count, or low hematocrit), wherein the method includes administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- the method includes administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E17
- E321. The method of E320, wherein the disease or condition is anemia or blood loss.
- a method of treating a subject having or at risk of developing anemia by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E323. The method of E319, E321 , or E322, wherein the anemia or blood loss is associated with cancer (e.g., a solid tumor, such as breast cancer, lung cancer, colon cancer; a tumor of the lymphatic system, such as chronic lymphocytic leukemia, non-Hodgkin’s lymphoma, Hodgkin’s lymphoma; or a tumor of the hematopoietic system, such as leukemia or multiple myeloma), cancer treatment (e.g., chemotherapy or radiation), myelofibrosis treatment (e.g., treatment with a JAK inhibitor, such as ruxolitinib orfedratinib), renal disease or failure (e.g., chronic kidney disease or acute renal disease or failure), a myelodysplastic syndrome, thalassemia (e.g., a- or b-thalassemia), a nutritional deficit (e.g., vitamin deficiency, such as B-12 or folate
- E324 The method of any one of E319 and E321-E323, wherein the anemia results from chronic kidney disease.
- E325. The method of any one of E319 and E321 -E323, wherein the anemia is associated with a myelodysplastic syndrome (e.g., the subject has a myelodysplastic syndrome).
- E326 The method of any one of E319 and E321 -E323, wherein the anemia is associated with myelofibrosis (e.g., the subject has myelofibrosis).
- E327 The method of any one E319 and E321-E323, wherein anemia is associated with ineffective hematopoiesis (e.g., ineffective erythropoiesis).
- anemia is associated with ineffective hematopoiesis (e.g., ineffective erythropoiesis).
- E328 The method of any one of E319 and E321 -E323, wherein the anemia is aplastic anemia, iron deficiency anemia, vitamin deficiency anemia, anemia of chronic disease (also called anemia of inflammation), anemia associated with bone marrow disease, hemolytic anemia, sickle cell anemia, microcytic anemia, hypochromic anemia, sideroblastic anemia, congenital dyserythropoietic anemia, Diamond Blackfan anemia, Fanconi anemia, or refractory anemia with excess of blasts.
- the anemia is aplastic anemia, iron deficiency anemia, vitamin deficiency anemia, anemia of chronic disease (also called anemia of inflammation), anemia associated with bone marrow disease, hemolytic anemia, sickle cell anemia, microcytic anemia, hypochromic anemia, sideroblastic anemia, congenital dyserythropoietic anemia, Diamond Blackfan anemia, Fanconi anemia, or refractory anemia
- E329. The method of E328, wherein the sideroblastic anemia is acquired sideroblastic anemia or congenital sideroblastic anemia.
- E330 The method of E329, wherein the sideroblastic anemia is congenital sideroblastic anemia.
- E331 The method of E330, wherein the congenital sideroblastic anemia is associated with a mutation in ALAS2, SLC25A38, FECH, GLRX5, HSPA9, HSCB, SLC25A38, or ABCB7.
- E332 The method of E330, wherein the congenital sideroblastic anemia is associated with a mutation in PUS1 , YARS2, LARS2, TRNT1 , MT-ATP6, NDUFB11 , or SLC19A2, or with an mtDNA mutation.
- E333 The method of any one of E306-E332, wherein the method increases red blood cell production, red blood cell count, hemoglobin levels, hematocrit, erythrocyte progenitor differentiation and/or maturation (e.g., of early and/or terminal stage erythroid progenitors), late-stage erythroid precursor maturation, recruitment of early-stage progenitors into the erythroid lineage, proerythroblast numbers, early-stage erythroid precursor and/or progenitor numbers (e.g., increases the early-stage precursor and/or progenitor populations), the progression of erythroid precursors and/or progenitors through erythropoiesis, and/or reticulocyte numbers.
- erythrocyte progenitor differentiation and/or maturation e.g., of early and/or terminal stage erythroid progenitors
- late-stage erythroid precursor maturation e.g., of early and/or terminal stage erythroid progeni
- E33 The method of any one of E306-E333, wherein the method reduces the accumulation of red blood cell progenitor cells.
- E335. The method of any one of E306-E334, wherein the subject is identified as having anemia prior to administration of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E336 The method of any one of E306-E334, wherein the method further comprises identifying the subject as having anemia prior to administration of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E337 The method of any one of E306-E336, wherein the method further comprises evaluating red blood cell, hemoglobin, hematocrit, and/or reticulocyte levels after administration of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E338 A method of increasing platelet levels (e.g., increasing platelet count) in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of increasing platelet count in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E340 A method of promoting or increasing platelet production in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of promoting or increasing megakaryocyte differentiation and/or maturation e.g., to produce platelets
- a method of promoting or increasing megakaryocyte differentiation and/or maturation e.g., to produce platelets
- administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of reducing the accumulation of platelet progenitor cells in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E343 The method of any one of E338-E342, wherein the subject has or is at risk of developing thrombocytopenia.
- a method of affecting myostatin, activin A, activin B, and/or BMP9 signaling e.g., reducing or inhibiting the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors
- the method includes administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E345. The method of E344, wherein the disease or condition is thrombocytopenia.
- E346 A method of treating a subject having or at risk of developing thrombocytopenia by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E347 A method of promoting platelet production by contacting a megakaryocyte with the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, or the construct of E174 or E175 in an amount effective to promote platelet production.
- E348 The method of E347, wherein the contacting is in vitro.
- a method of treating a subject having or at risk of developing thrombocytopenia by administering to the subject a platelet produced by the method of E347 or E348.
- E350 The method of any one of E343, E345, E346, and E349, wherein the thrombocytopenia is associated with a bone marrow defect, a myelodysplastic syndrome, bone marrow transplantation, myelofibrosis, myelofibrosis treatment (e.g., treatment with a JAK inhibitor, such as with ruxolitinib orfedratinib), ineffective hematopoiesis, Gaucher disease, aplastic anemia, Fanconi anemia, Diamond Blackfan anemia, Shwachman Diamond syndrome, heavy alcohol consumption, cirrhosis of the liver, cancer (e.g., leukemia or lymphoma), an autoimmune disease, a viral infection, a bacterial infection, an enlarged spleen, a vitamin deficiency, cancer treatment, thrombotic thrombocytopenic purpura, idiopathic thrombocytopenic purpura, disseminated intravascular coagulation, hemolytic uremic
- E351 The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with a myelodysplastic syndrome (e.g., the subject has a myelodysplastic syndrome).
- E352 The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with myelofibrosis (e.g., the subject has myelofibrosis).
- E353 The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with a bone marrow defect.
- E354 The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with bone marrow transplantation.
- E355. The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with cancer.
- E356 The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with cancer treatment (e.g., chemotherapy or radiation).
- cancer treatment e.g., chemotherapy or radiation.
- E357 The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with hematopoietic stem cell transplantation.
- E358 The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with an autoimmune disease.
- E359 The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with contraindication to transfusion.
- E360 The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with myelofibrosis treatment.
- E361. The method of any one of E343, E345, E346, E349, and E350, wherein the thrombocytopenia is associated with ineffective hematopoiesis.
- E362 The method of any one of E343, E345, E346, and E349, wherein the thrombocytopenia is familial thrombocytopenia.
- E363 The method of E362, wherein the familial thrombocytopenia is May-Hegglin anomaly, Sebastian syndrome, Fechtner syndrome, Epstein’s syndrome, Wiskott-Aldrich syndrome, congenital amegakaryocytic thrombocytopenia, platelet storage pool deficiency, Hermansky-Pudlak syndrome, Bernard-Soulier syndrome, Von Willebrand Disease Type 2B, ANKRD26-related thrombocytopenia, thrombocytopenia absent radius syndrome, familial platelet disorder with associated myeloid malignancy (FPD/AML), thrombocytopenia associated with a mutation in Filamin-A, or thrombocytopenia associated with a mutation in GATA-1.
- FPD/AML familial platelet disorder with associated myeloid malignancy
- E364 The method any one of E343, E345, E346, and E349, wherein the thrombocytopenia is immune thrombocytopenia.
- E365 The method of any one of E338-E364, wherein the method increases platelet count, platelet production and/or megakaryocyte differentiation and/or maturation.
- E366 The method of any one of E338-E365, wherein the method reduces the accumulation of platelet progenitor cells.
- E367 The method of any one of E338-E366, wherein the method improves blood clotting, reduces bleeding events (e.g., reduces the incidence of bleeding events), and/or reduces bleeding in the skin of the subject.
- E368 The method of any one of E338-E347 and E349-E367, wherein the subject is identified as having thrombocytopenia prior to administration of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173 or the platelets produced by the method of E347 or E348.
- E369. The method of any one of E338-E347 and E349-E367, wherein the method further comprises identifying the subject as having thrombocytopenia prior to administration of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173 or the platelets produced by the method of E347 or E348.
- E370 The method of any one of E338-E347 and E349-E369, wherein the method further comprises evaluating platelet levels after administration of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173 or the platelets produced by the method of E347 or E348.
- a method of increasing neutrophil levels e.g., increasing neutrophil count
- a method of increasing neutrophil levels by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of increasing neutrophil count in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of promoting or increasing neutrophil production in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of promoting or increasing the differentiation and/or maturation of progenitor cells e.g., myeloid progenitors, myeloblasts, and/or myelocytes
- a method of promoting or increasing the differentiation and/or maturation of progenitor cells e.g., myeloid progenitors, myeloblasts, and/or myelocytes
- E375 The method of any one of E371 -E374, wherein the subject has or is at risk of developing neutropenia.
- E376 A method of affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing a disease or condition involving low neutrophil levels, wherein method includes administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E377 The method of E376, wherein the disease or condition is neutropenia.
- E378 A method of treating a subject having or at risk of developing neutropenia by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E379. The method of E375, E377, or E378, wherein the neutropenia is associated with a bone marrow defect, a myelodysplastic syndrome, bone marrow transplantation, myelofibrosis, ineffective hematopoiesis, aplastic anemia, Fanconi anemia, Diamond Blackfan anemia, Shwachman Diamond syndrome, paroxysmal nocturnal hemoglobinuria, Pearson syndrome, dyskeratosis congenita, cancer (e.g., leukemia), a vitamin deficiency, an enlarged spleen, an autoimmune disease, a viral infection, a bacterial infection, cancer treatment, a reduction in neutrophils caused by medication (e.g., medication used to treat overactive thyroid, such as methimazole and propylthiouracil; an antibiotic, such as vancomycin, penicillin G, trimethoprim, and oxacillin; an antiviral drug, such as ganciclovir and valganciclovir
- E380 The method of any one of E375 and E377-E379, wherein the neutropenia is associated with a myelodysplastic syndrome (e.g., the subject has a myelodysplastic syndrome).
- E381. The method of any one of E375 and E377-E379, wherein the neutropenia is associated with myelofibrosis (e.g., the subject has myelofibrosis).
- E382. The method of any one of E375 and E377-E379, wherein the neutropenia is associated with a bone marrow defect.
- E383 The method of any one of E375 and E377-E379, wherein the neutropenia is associated with bone marrow transplantation.
- E384 The method of any one of E375 and E377-E379, wherein the neutropenia is associated with cancer.
- E385. The method of any one of E375 and E377-E379, wherein the neutropenia is associated with cancer treatment (e.g., chemotherapy or radiation).
- cancer treatment e.g., chemotherapy or radiation.
- E386 The method of any one of E375 and E377-E379, wherein the neutropenia is associated with hematopoietic stem cell transplantation.
- E387 The method of any one of E375 and E377-E379, wherein the neutropenia is associated with inflammation.
- E388 The method of any one of E375 and E377-E379, wherein the neutropenia is associated with contraindication to transfusion.
- E390 The method of E375, E377, or E378, wherein the neutropenia is chronic idiopathic neutropenia.
- E39. The method of E375, E377, or E378, wherein the neutropenia is familial neutropenia.
- E392 The method of E391 , wherein the familial neutropenia is cyclic neutropenia, chronic benign neutropenia, or severe congenital neutropenia (e.g., neutropenia associated with mutations in the genes ELANE (associated with SCN1), HAX1 (associated with SCN3), G6PC3 (associated with SCN4), GFI1 (associated with SCN2), CSF3R, WAS (associated with X-linked neutropenia/X- linked SCN), CXCR4, VPS45A (associated with SCN5), or JAGN1).
- ELANE associated with SCN1
- HAX1 associated with SCN3
- G6PC3 associated with SCN4
- GFI1 associated with SCN2
- CSF3R CSF3R
- WAS associated with X-linked neutropenia/X- linked SCN
- VPS45A associated with SCN5
- JAGN1 JAGN1
- E393 The method of any one of E371-E392, wherein the method increases neutrophil count, neutrophil production, and/or the differentiation and/or maturation of progenitor cells into neutrophils.
- E394 The method of any one of E371 -E393, wherein the method reduces the subject’s susceptibility to infection.
- E395. The method of any one of E371-E394, wherein the subject is identified as having neutropenia prior to administration of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E396 The method of any one of E371-E394, wherein the method further comprises identifying the subject as having neutropenia prior to administration of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E397 The method of any one of E371 -E396, wherein the method further comprises evaluating neutrophil levels after administration of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E398 A method of treating a subject having or at risk of developing a myelodysplastic syndrome by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E400 The method of any one of E323, E325, E350, E351 , E379, E380, E398, and E399, wherein the myelodysplastic syndrome is myelodysplastic syndrome with unilineage dysplasia (MDS-SLD), myelodysplastic syndrome with multilineage dysplasia (MDS-MLD), myelodysplastic syndrome with ring sideroblasts (MDS-RS, which includes single lineage dysplasia (MDS-RS-SLD) and multilineage dysplasia (MDS-RS-MLD)), myelodysplastic syndrome associated with isolated del chromosome abnormality (myelodysplastic syndrome with isolated del(5q)), myelodysplastic syndrome with excess blasts (e.g., myelodysplastic syndrome with excess blasts — type 1 (MDS- EB-1) or myelodysplastic syndrome with excess blasts — type 2 (MDS-EB-2)), myelodysplastic
- E401 The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E400, wherein the myelodysplastic syndrome is MDS-SLD.
- E402. The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E400, wherein the myelodysplastic syndrome is MDS-MLD.
- E403. The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E400, wherein the myelodysplastic syndrome is MDS-RS-SLD.
- E404 The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E400, wherein the myelodysplastic syndrome is MDS-RS-MLD.
- E405. The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E400, wherein the myelodysplastic syndrome is myelodysplastic syndrome with isolated del(5q).
- E406 The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E400, wherein the myelodysplastic syndrome is MDS-EB-1.
- E407. The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E400, wherein the myelodysplastic syndrome is MDS-EB-2.
- E408. The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E400, wherein the myelodysplastic syndrome is MDS-U.
- E409 The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E400, wherein the myelodysplastic syndrome is MDS/MPN-RS-T.
- E410 The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E409, wherein the myelodysplastic syndrome is a ring sideroblast positive myelodysplastic syndrome (RS positive MDS, e.g., the subject has ring sideroblasts).
- RS positive MDS ring sideroblast positive myelodysplastic syndrome
- E411 The method of E410, wherein the RS-positive myelodysplastic syndrome is associated with a splicing factor mutation.
- E412 The method of E411 , wherein the splicing factor mutation is a mutation in Splicing Factor 3b Subunit 1 (SF3B1).
- E413. The method of any one of E323, E325, E350, E351 , E379, E380, E398-E402, and E405-E409, wherein the myelodysplastic syndrome is a non-ring sideroblast myelodysplastic syndrome (non- RS, e.g., the subject lacks ring sideroblasts).
- non- RS non-ring sideroblast myelodysplastic syndrome
- E414 The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E413, wherein the myelodysplastic syndrome is a very low, low, or intermediate risk myelodysplastic syndrome (e.g., as determined by the Revised International Prognostic Scoring System).
- E415. The method of E414, wherein the myelodysplastic syndrome is a very low risk myelodysplastic syndrome (e.g., as determined by the Revised International Prognostic Scoring System).
- E416 The method of E414, wherein the myelodysplastic syndrome is a low risk myelodysplastic syndrome (e.g., as determined by the Revised International Prognostic Scoring System).
- E417 The method of E414, wherein the myelodysplastic syndrome is an intermediate risk myelodysplastic syndrome (e.g., as determined by the Revised International Prognostic Scoring System).
- E418 The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E417, wherein the myelodysplastic syndrome is associated with a defect in terminal maturation.
- E419. The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E417, wherein the myelodysplastic syndrome is associated with a defect in early-stage hematopoiesis (e.g., commitment or differentiation of progenitor cells).
- E420 The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E419, wherein the myelodysplastic syndrome is associated with elevated endogenous erythropoietin levels.
- E421. The method of any one of E323, E325, E350, E351 , E379, E380, and E398-E420, wherein the myelodysplastic syndrome is associated with hypocellular bone marrow (e.g., the subject has hypocellular bone marrow).
- a method of treating a subject having or at risk of developing myelofibrosis by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E424 The method of any one of E306-E423, wherein the subject does not respond well to treatment with erythropoietin (EPO), is susceptible to the adverse effects of EPO, or does not respond well to treatment with an erythroid maturation agent.
- EPO erythropoietin
- E425. The method of any one of E306-E424, wherein the subject has previously been treated with an erythropoiesis stimulating agent (ESA).
- ESA erythropoiesis stimulating agent
- E426 The method of any one of E306-E424, wherein the subject has not previously been treated with an erythropoiesis stimulating agent (ESA).
- ESA erythropoiesis stimulating agent
- E427 The method of any one of E306-E426, wherein the subject has a low transfusion burden.
- E428 The method of E427, wherein the subject has received 1-3 units of RBCs (1-3 RBC transfusions) within eight weeks prior to starting treatment with the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E429. The method of E427, wherein the subject has received 0 units of RBCs (0 RBC transfusions) within eight weeks prior to starting treatment with the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E430 The method of any one of E306-E426, wherein the subject has a high transfusion burden.
- E431. The method of any one of E306-E430, wherein the method reduces the subject’s need for a blood transfusion (e.g., reduces transfusion burden).
- a method of preventing e.g., preventing the development of) pulmonary hypertension (PH) in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of reducing the risk of developing PH in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of slowing or inhibiting the progression of PH in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of treating a subject having or at risk of developing PH by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E436 A method of affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing PH by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E437 A method of reducing vascular remodeling in a subject having or at risk of developing PH by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E438 A method of reducing right ventricular hypertrophy in a subject having or at risk of developing PH by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of reducing pulmonary vascular resistance in a subject having or at risk of developing PH by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E440 The method of any one of E432-E439, wherein the PH is pulmonary arterial hypertension (PAH).
- PAH pulmonary arterial hypertension
- E443 The method of E440, wherein the PAH is associated with HIV infection, schistosomiasis, cirrhosis of the liver, a congenital heart abnormality, portal hypertension, pulmonary veno-occlusive disease, pulmonary capillary hemangiomatosis, a connective tissue disorder, an autoimmune disorder (e.g., scleroderma or lupus), or drug use or abuse (e.g., use of cocaine or methamphetamine).
- HIV infection schistosomiasis
- cirrhosis of the liver a congenital heart abnormality
- portal hypertension pulmonary veno-occlusive disease
- pulmonary capillary hemangiomatosis a connective tissue disorder
- an autoimmune disorder e.g., scleroderma or lupus
- drug use or abuse e.g., use of cocaine or methamphetamine
- E444 The method of any one of E432-E439, wherein the PH is venous PH.
- E445. The method of E444, wherein the venous PH is associated with left ventricular systolic dysfunction, left ventricular diastolic dysfunction, valvular heart disease, congenital cardiomyopathy, or congenital or acquired pulmonary venous stenosis.
- E446 The method of any one of E432-E439, wherein the PH is hypoxic PH.
- E447 The method of E446, wherein the hypoxic PH is associated with chronic obstructive pulmonary disease (e.g., emphysema), interstitial lung disease, sleep-disordered breathing (e.g., sleep apnea), a lung disease (e.g., pulmonary fibrosis), an alveolar hypoventilation disorder, chronic exposure to high altitude, or a developmental abnormality.
- E448 The method of any one of E432-E439, wherein the PH is thromboembolic PH.
- E449. The method of E448, wherein the thromboembolic PH is associated with chronic thromboembolic pulmonary hypertension, pulmonary emboli, angiosarcoma, arteritis, congenital pulmonary artery stenosis, or parasitic infection.
- E450 The method of any one of E432-E439, wherein the PH is miscellaneous PH.
- E451 The method of E450, wherein the miscellaneous PH is associated with a hematologic disease (e.g., chronic hemolytic anemia, sickle cell disease), a systemic disease (e.g., sarcoidosis, pulmonary Langerhans cell histiocytosis, lymphangioleiomyomatosis, neurofibromatosis, or vasculitis), a metabolic disorder (e.g., glycogen storage disease, Gaucher disease, or thyroid diseases), pulmonary tumoral thrombotic microangiopathy, fibrosing mediastinitis, chronic kidney failure, or segmental pulmonary hypertension.
- a hematologic disease e.g., chronic hemolytic anemia, sickle cell disease
- a systemic disease e.g., sarcoidosis, pulmonary Langerhans cell histiocytosis, lymphangioleiomyomatosis, neurofibromatosis, or vasculitis
- a metabolic disorder e.g.,
- E452 The method of any one of E432-E451 , wherein the method reduces the frequency or severity of one or more symptoms of PH (e.g., reduces the severity or frequency of one or more of shortness of breath (dyspnea), fatigue, swelling (e.g., edema) of the legs, feet, belly (ascites), or neck, chest pain or pressure, racing pulse or heart palpitations, bluish color to lips or skin (cyanosis), dizziness, or fainting).
- dyspnea shortness of breath
- fatigue swelling
- swelling e.g., edema
- the legs feet, belly (ascites), or neck
- chest pain or pressure e.g., edema
- racing pulse or heart palpitations bluish color to lips or skin (cyanosis), dizziness, or fainting.
- E453 The method of any one of E432-E452, wherein the method reduces pulmonary vascular remodeling.
- E454 The method of any one of E432-E453, wherein the method reduces vascular remodeling in the heart.
- E455. The method of any one of E432-E454, wherein the method reduces right ventricular hypertrophy.
- E456 The method of any one of E432-E455, wherein the method reduces pulmonary vascular resistance (e.g., reduces pulmonary vascular resistance compared to measurements taken prior to treatment).
- E457 The method of any one of E432-E456, wherein the method improves performance in the 6-minute walk test (e.g., improves performance compared to measurements taken prior to treatment).
- E458 The method of any one of E432-E457, wherein the method reduces bone loss.
- E459 The method of any one of E432-E458, wherein the method reduces pulmonary arterial muscularization or pulmonary arterial wall thickening.
- E460 The method of any one of E432-E459, wherein the method reduces right ventricular compensation.
- a method of reducing body fat in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of reducing body weight in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- a method of reducing blood glucose in a subject in need thereof by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E464 A method of increasing insulin sensitivity in a subject in need thereof, by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E465. The method of any one of E461-E464, wherein the subject has or is at risk of developing a metabolic disease.
- E466 A method of affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of myostatin, activin A, activin B, and/or BMP9 to their receptors) in a subject having or at risk of developing a metabolic disease by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1 -E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E467 A method of treating and/or preventing a metabolic disease in a subject by administering to the subject a therapeutically effective amount of the polypeptide of any one of E1-E167, the nucleic acid molecule of E168, the vector of E169, the construct of E174 or E175, or the pharmaceutical composition of E172 or E173.
- E468 The method of any one of E465-E467, wherein the metabolic disease is age-related metabolic disease.
- E469. The method of any one of E465-E467, wherein the metabolic disease is treatment-related metabolic disease.
- E470 The method of E469, wherein the treatment is treatment with a glucocorticoid (e.g., a corticosteroid, such as prednisone), a selective serotonin reuptake inhibitor (SSRI, e.g., paroxetine, mirtazapine, fluoxetine, escitalopram, or sertraline), a serotonin-norepinephrine reuptake inhibitor (SNRI), a tricyclic antidepressant (e.g., amitriptyline), a mood stabilizer (e.g., valproic acid or lithium), an antipsychotic (e.g., olanzapine, chlorpromazine, or clozapine), or a diabetes medication (e.g., insulin, chlorpropamide).
- a glucocorticoid e.g., a corticosteroid, such as prednisone
- SSRI selective serotonin reup
- E471. The method of any one of E465-E470, wherein the metabolic disease is selected from the group including obesity, Type 1 diabetes, and Type 2 diabetes.
- E472 The method of E471 , wherein the metabolic disease is obesity.
- E473 The method of E471 , wherein the metabolic disease is Type 1 diabetes.
- E474 The method of E471 , wherein the metabolic disease is Type 2 diabetes.
- E475. The method of any one of E461-E474, wherein the method reduces body weight and/or percentage of body weight gain of said subject.
- E476 The method of any one of E461 -E475, wherein the method reduces amount of body fat and/or percentage of body fat of said subject.
- E477 The method of any one of E461-E476, wherein the method does not affect the appetite for food intake of said subject.
- E478 The method of any one of E461-E477, wherein the method reduces adiposity of said subject.
- E479. The method of any one of E461 -E478, wherein the method reduces the weights of epididymal and perirenal fat pads of said subject.
- E480 The method of any one of E461-E479, wherein the method reduces the amount of subcutaneous, visceral, and/or hepatic fat of said subject.
- E481 The method of any one of E461-E480, wherein the method lowers the level of fasting insulin of said subject.
- E482 The method of any one of E461-E481 , wherein the method lowers the level of blood glucose of said subject.
- E483 The method of any one of E461-E482, wherein the method increases insulin sensitivity of said subject.
- E484 The method of any one of E461 -E483, wherein the method increases the rate of glucose clearance of said subject.
- E485. The method of any one of E461-E484, wherein the method improves the serum lipid profile of said subject.
- E486 The method of any one of E461-E485, wherein the method delays, reduces, or eliminates the need for insulin treatment.
- E487 The method of any one of E461-E486, wherein the method does not reduce lean mass.
- E488 The method of any one of E176-E487, wherein the method reduces or inhibits the binding of activin A, activin B, and/or myostatin to their receptors (e.g., their endogenous receptors).
- E489. The method of any one of E176-E208, E243-E270, and E488, wherein the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to increase muscle mass and/or strength, increase lean mass, affect myostatin, activin A, activin B, and/or BMP9 signaling in the subject, or reduce or inhibit the binding of activin A, activin B and/or myostatin to their receptors (e.g., their endogenous receptors).
- their receptors e.g., their endogenous receptors.
- E490 The method of any one of E209-E291 and E488, wherein the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to increase mineral bone density, reduce bone resorption, reduce bone loss, reduce the rate of bone resorption, increase bone formation, increase the rate of bone formation, reduce osteoclast activity, increase osteoblast activity, increase bone strength, reduce the risk or occurrence of bone fracture, affect myostatin, A, activin B, and/or BMP9 signaling in the subject, or reduce or inhibit the binding of activin A, activin B and/or myostatin to their receptors (e.g., their endogenous receptors).
- their receptors e.g., their endogenous receptors
- E491 The method of any one of E292-E305 and E488, wherein the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to reduce fibrosis, prevent the development of fibrosis, reduce the risk of developing fibrosis, delay the development of fibrosis, slow or inhibit the progression of fibrosis, treat fibrosis, reduce one or more symptom of fibrosis, improve the function of a fibrotic tissue or organ, affect myostatin, activin A, activin B, and/or BMP9 signaling in the subject, or reduce or inhibit the binding of activin A, activin B, and/or myostatin to their receptors (e.g., their endogenous receptors).
- their receptors e.g., their endogenous receptors
- E492. The method of any one of E306-E337, E398-E431 , and E488, wherein the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to increase red blood cell levels, increase hemoglobin levels, increase red blood cell production, increase red blood cell count, increase hematocrit, reduce the need for a blood transfusion, increase the maturation and/or differentiation of erythroid progenitors (e.g., early and/or terminal stage erythroid progenitors), increase late-stage erythroid precursor maturation, recruit early- stage progenitors into the erythroid lineage, increase reticulocytes, increase proerythroblast numbers, increase reticulocyte numbers, reduce the accumulation of red blood cell progenitor cells, increase the number of early-stage erythroid precursors and/or progenitors, promote the progression of erythroid precursors and/or progenitors through erythropoiesis, treat anemia, affect myostatin
- E493. The method of any one of E338-E370, E98-E431 , and E488, wherein the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to increase platelet levels, increase platelet production, increase platelet count, increase or induce megakaryocyte differentiation and/or maturation, reduce the accumulation of platelet progenitor cells, improve blood clotting, reduce bleeding events, reduce bleeding in the skin, treat thrombocytopenia, affect myostatin, activin A, activin B, and/or BMP9 signaling in the subject, or reduce or inhibit the binding of activin A, activin B, and/or myostatin to their receptors (e.g., their endogenous receptors).
- the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to increase platelet levels, increase platelet production, increase platelet count, increase or induce megakaryocyte differentiation and/or maturation, reduce the accumulation of platelet progenitor cells, improve blood
- E494 The method of any one of E371-E431 and E488, wherein the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to increase neutrophil levels, increase neutrophil production, increase neutrophil count, increase or induce the differentiation and/or maturation of progenitor cells into neutrophils, treat neutropenia, reduce susceptibility to infection, affect myostatin, activin A, activin B, and/or BMP9 signaling in the subject, or reduce or inhibit the binding of activin A, activin B, and/or myostatin to their receptors (e.g., their endogenous receptors).
- the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to increase neutrophil levels, increase neutrophil production, increase neutrophil count, increase or induce the differentiation and/or maturation of progenitor cells into neutrophils, treat neutropenia, reduce susceptibility to infection, affect myostatin, activin A, activin B, and/or BMP
- E495. The method of any one of E432-E460 and E488, wherein the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to prevent PH, reduce the risk of developing PH, reduce the severity or frequency of one or more symptoms of PH, delay the development of PH, slow or inhibit the progression of PH, treat PH, reduce pulmonary vascular remodeling, reduce vascular remodeling in the heart, reduce right ventricular hypertrophy, reduce pulmonary vascular resistance, improve performance in the 6 minute walk test, affect myostatin, activin A, activin B, and/or BMP9 signaling in the subject, or reduce or inhibit the binding of activin A, activin B, and/or myostatin to their receptors (e.g., their endogenous receptors).
- their receptors e.g., their endogenous receptors
- E496 The method of any one of E461 -E488, wherein the polypeptide, nucleic acid, vector, construct, or pharmaceutical composition is administered in an amount sufficient to reduce body fat, reduce the amount of subcutaneous fat, reduce the amount of visceral and/or hepatic fat, reduce adiposity, reduce the weights of epididymal and perirenal fat pads, reduce body fat percentage, reduce body weight, reduce the percentage of body weight gain, reduce fasting insulin levels, reduce blood glucose levels, increase insulin sensitivity, affect myostatin, activin A, activin B, and/or BMP9 signaling in the subject, reduce the proliferation of adipose cells, reduce or inhibit the binding of activin A, activin B, and/or myostatin to their receptors (e.g., their endogenous receptors), reduce LDL, reduce triglycerides, improve the serum lipid profile, regulate insulin biosynthesis and/or secretion from b-cells, delay, postpone, or reduce the need for insulin,
- E497 The method of any one of E176-E496, wherein the method does not cause a vascular complication in the subject.
- E498 The method of E497, wherein the method does not increase vascular permeability or leakage.
- the term “about” refers to a value that is within 10% above or below the value being described.
- any values provided in a range of values include both the upper and lower bounds, and any values contained within the upper and lower bounds.
- extracellular activin receptor type II (ActRII) chimera refers to a peptide including a soluble, extracellular portion of the single transmembrane receptor ActRIIB and a soluble, extracellular portion of the single transmembrane receptor ActRII A.
- the ActRII chimeras described herein result from joining an N-terminal portion of extracellular ActRIIB to a C-terminal portion of extracellular ActRIIA such that the sequences are contiguous (e.g., the ActRIIA sequence continues where the ActRIIB sequence left off, starting with the next the amino acid located in the corresponding position of ActRIIA).
- the extracellular ActRII chimera may also include one or more amino acid substitutions in the portion of the chimera that corresponds to the sequence of ActRIIB compared to a wild-type extracellular ActRIIB (e.g., bold portion of the sequence of SEQ ID NO: 46 shown below), and one or more amino acid substitutions in the portion of the chimera that corresponds to the sequence of ActRIIA compared to a wild-type extracellular ActRIIA (e.g., bold portion of the sequence of SEQ ID NO: 47 shown below).
- the extracellular ActRII chimera may also have an N-terminal truncation of 1-9 amino acids relative to the extracellular portion of ActRIIB or ActRIIA.
- An extracellular ActRI I chimera may have the sequence of any one of SEQ ID NOs: 1-43.
- an extracellular ActRI I chimera has the sequence of any one of SEQ ID NOs: 22- 43 (Table 2).
- N-terminal truncation refers to a deletion of 1-9 amino acids (e.g., 1 , 2, 3, 4, 5, 6, 7, 8, or 9 amino acids) from the N-terminus of an extracellular ActRI I chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the N-terminal truncation can remove amino acids up two to amino acids before the first cysteine (e.g., the two amino acids before the first cysteine (RE or QE) are retained in the N-terminally truncated ActRII chimeras).
- linker refers to a linkage between two elements, e.g., peptides or protein domains.
- a polypeptide described herein may include an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)), fused to a moiety.
- the moiety may increase stability or improve pharmacokinetic properties of the polypeptide.
- the moiety may be fused to the polypeptide by way of a linker.
- a linker can be a covalent bond or a spacer.
- the term “bond” refers to a chemical bond, e.g., an amide bond or a disulfide bond, or any kind of bond created from a chemical reaction, e.g., chemical conjugation.
- spacer refers to a moiety (e.g., a polyethylene glycol (PEG) polymer) or an amino acid sequence (e.g., a 1-200 amino acid sequence) occurring between two elements, e.g., peptides or protein domains, to provide space and/or flexibility between the two elements.
- An amino acid spacer is part of the primary sequence of a polypeptide (e.g., fused to the spaced peptides via the polypeptide backbone).
- the formation of disulfide bonds, e.g., between two hinge regions that form an Fc domain is not considered a linker.
- Fc domain refers to a dimer of two Fc domain monomers.
- An Fc domain has at least 80% sequence identity (e.g., at least 85%, 90%, 95%, 97%, or 100% sequence identity) to a human Fc domain that includes at least a CH2 domain and a CH3 domain.
- An Fc domain monomer includes second and third antibody constant domains (CH2 and CH3).
- the Fc domain monomer also includes a hinge domain.
- An Fc domain does not include any portion of an immunoglobulin that is capable of acting as an antigen-recognition region, e.g., a variable domain or a complementarity determining region (CDR).
- CDR complementarity determining region
- each of the Fc domain monomers in an Fc domain includes amino acid substitutions in the CH2 antibody constant domain to reduce the interaction or binding between the Fc domain and an Fey receptor.
- the Fc domain contains one or more amino acid substitutions that reduce or inhibit Fc domain dimerization.
- An Fc domain can be any immunoglobulin antibody isotype, including IgG, IgE, IgM, IgA, or IgD. Additionally, an Fc domain can be an IgG subtype (e.g., lgG1 , lgG2a, lgG2b, lgG3, or lgG4). The Fc domain can also be a non-naturally occurring Fc domain, e.g., a recombinant Fc domain.
- albumin-binding peptide refers to an amino acid sequence of 12 to 16 amino acids that has affinity for and functions to bind serum albumin.
- An albumin-binding peptide can be of different origins, e.g., human, mouse, or rat.
- an albumin-binding peptide has the sequence DICLPRWGCLW (SEQ ID NO: 101).
- the term “endogenous” describes a molecule (e.g., a polypeptide, nucleic acid, or cofactor) that is found naturally in a particular organism (e.g., a human) or in a particular location within an organism (e.g., an organ, a tissue, or a cell, such as a human cell, e.g., a human red blood cell, platelet, neutrophil, or muscle cell).
- a molecule e.g., a polypeptide, nucleic acid, or cofactor
- fibronectin domain refers to a high molecular weight glycoprotein of the extracellular matrix, or a fragment thereof, that binds to, e.g., membrane-spanning receptor proteins such as integrins and extracellular matrix components such as collagens and fibrins.
- a fibronectin domain is a fibronectin type III domain (SEQ ID NO: 102) having amino acids 610-702 of the sequence of UniProt ID NO: P02751.
- a fibronectin domain is an adnectin protein.
- human serum albumin refers to the albumin protein present in human blood plasma. Human serum albumin is the most abundant protein in the blood. It constitutes about half of the blood serum protein. In some embodiments, a human serum albumin has the sequence of UniProt ID NO: P02768 (SEQ ID NO: 103).
- fused is used to describe the combination or attachment of two or more elements, components, or protein domains, e.g., peptides or polypeptides, by means including chemical conjugation, recombinant means, and chemical bonds, e.g., amide bonds.
- two single peptides in tandem series can be fused to form one contiguous protein structure, e.g., a polypeptide, through chemical conjugation, a chemical bond, a peptide linker, or any other means of covalent linkage.
- an extracellular ActRI I chimera may be fused in tandem series to the N- or C-terminus of a moiety (e.g., Fc domain monomer (e.g., the sequence of SEQ ID NO: 48) a wild-type Fc domain (e.g., the sequence of SEQ ID NO: 100 or SEQ ID NO: 264), an Fc domain with amino acid substitutions (e.g., one or more substitutions that reduce dimerization), an albumin-binding peptide (e.g., the sequence of SEQ ID NO: 101), a fibronectin domain (e.g., the sequence of SEQ ID NO: 102), or a human serum albumin (e.g., the sequence of SEQ ID NO: 103)) by way of a linker
- Fc domain monomer e.g., the sequence of SEQ ID NO: 48
- a wild-type Fc domain e.g., the sequence of SEQ ID NO: 100 or SEQ ID NO: 264
- an extracellular ActRII chimera is fused to a moiety (e.g., an Fc domain monomer, a wild-type Fc domain, an Fc domain with amino acid substitutions (e.g., one or more substitutions that reduce dimerization), an albumin-binding peptide, a fibronectin domain, or a human serum albumin) by way of a peptide linker, in which the N-terminus of the peptide linker is fused to the C-terminus of the extracellular ActRII chimera through a chemical bond, e.g., a peptide bond, and the C-terminus of the peptide linker is fused to the N-terminus of the moiety (e.g., Fc domain monomer, wild-type Fc domain, Fc domain with amino acid substitutions (e.g., one or more substitutions that reduce dimerization), albumin-binding peptide, fibronectin domain, or human serum albumin) through a chemical bond,
- bone mineral density (BMD),” “bone density,” and “bone mass” refer to a measure of the amount of bone mineral (e.g., calcium) in bone tissue.
- BMD may be measured by well- established clinical techniques known to one of skill in the art (e.g., by single-1 or dual-energy photon or X-ray absorptiometry).
- the concept of BMD relates to the mass of mineral per volume of bone, although clinically it is measured by proxy according to optical density per square centimeter of bone surface upon imaging. BMD measurement is used in clinical medicine as an indirect indicator of osteoporosis and fracture risk.
- BMD test results are provided as a T-score, where the T-score represents the BMD of a subject compared to the ideal or peak bone mineral density of a healthy 30-year- old adult.
- a score of 0 indicates that the BMD is equal to the normal reference value for a healthy young adult.
- Differences between the measured BMD of subject and that of the reference value for a healthy young adult are measured in standard deviations units (SDs).
- SDs standard deviations units
- a T-score of between +1 SD and -1 SD may indicate a normal BMD
- a T-score of between -1 SD and -2.5 SD may indicate low bone mass (e.g., osteopenia)
- a T-score lower than -2.5 SD may indicate osteoporosis or severe osteoporosis.
- a polypeptide of the invention including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid encoding such a polypeptide, or a vector containing such a nucleic acid molecule is administered to a subject in need thereof, wherein the patient has low bone mass (e.g., a T-Score of between -1 SD and -2.5 SD).
- a polypeptide of the invention including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid encoding such a polypeptide, or a vector containing such a nucleic acid molecule is administered to a subject in need thereof, wherein the patient has osteoporosis (e.g., a T-Score of less than -2.5 SD).
- administration of a polypeptide of the invention including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid encoding such a polypeptide or a vector containing such a nucleic acid molecule treats the subject by increasing their BMD.
- administration of a polypeptide of the invention including an extracellular ActRI I chimera e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid encoding such a polypeptide, or a vector containing such a nucleic acid molecule increases the BMD of a subject resulting in an increase in the T- Score of the subject (e.g., resulting in an increase in the T-Score of the subject of 0.1 or more, 0.2 or more, 0.3 or more, 0.4 or more, 0.5 or more, 1 .0 or more, or 2.0 or more).
- bone strength refers to a measurement of bone that is determined by bone quality in addition to bone mineral density. Bone quality is influenced by bone geometry, microarchitecture, and the properties of constituent tissues. Bone strength can be used to assess the bone’s risk of fracture.
- bone disease refers to a condition characterized by bone damage (e.g., decreased bone mineral density, decreased bone strength, and/or bone loss). Such diseases or conditions may be caused by an imbalance in osteoblast and/or osteoclast activity (e.g., increased bone resorption or reduced bone formation).
- Bone diseases include primary osteoporosis, secondary osteoporosis, osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis-related bone loss (e.g., bone loss associated with multiple myeloma), Paget’s disease, renal osteodystrophy, osteogenesis imperfecta, neuromuscular disease-related bone loss, burn-induced bone loss (e.g., bone loss associated with a burn injury), anorexia-related bone loss, treatment-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity-related bone loss, and immobility-related bone loss.
- bone loss associated with multiple myeloma e.g., Paget’s disease, renal osteodystrophy, osteogenesis imperfecta, neuromuscular disease-related bone loss, burn-induced bone loss (e.g., bone loss associated with a burn injury), anorexia-related bone loss, treatment-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity-
- the term “neuromuscular disease-related bone loss” refers to bone loss that occurs in a subject having a neuromuscular disease. Poor bone health is often a significant problem for patients with neuromuscular disease. Deficiency of bone mineral density and increased incidence of bone fractures, for example, are a we 11- re cognized clinical consequence of diseases such as DMD, ALS, and SMA.
- bone remodeling or “bone metabolism” refer to the process for maintaining bone strength and ion homeostasis by replacing discrete parts of old bone with newly synthesized packets of proteinaceous matrix. Bone is resorbed by osteoclasts and is deposited by osteoblasts in a process called ossification. Osteocyte activity plays a key role in this process.
- Conditions that result in a decrease in bone mass can either be caused by an increase in resorption, or a decrease in ossification.
- bone formation exceeds resorption.
- resorption exceeds formation.
- Bone resorption rates are also typically much higher in post-menopausal older women due to estrogen deficiency related to menopause.
- bone resorption or “bone catabolic activity” refer to a process by which osteoclasts break down the tissue in bones and release the minerals, resulting in a transfer of the mineral (e.g., calcium) from bone tissue to the blood.
- Increased rates of bone resorption are associated with aging, including in post-menopausal women.
- High rates of bone resorption, or rates of bone resorption that exceed the rate of ossification, are associated with bone disorders, such as decreased bone mineral density, including osteopenia and osteoporosis, and can result in bone loss.
- a polypeptide of the invention including an extracellular ActRI I chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid encoding such a polypeptide, or a vector containing such a nucleic acid molecule is administered to a subject in need thereof to decrease bone resorption (e.g., decrease bone loss) in the subject (e.g., the amount or rate of bone resorption in the subject).
- a polypeptide of the invention including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid encoding such a polypeptide, or a vector containing such a nucleic acid molecule is administered to a subject in need thereof, to increase bone formation (e.g., increase the amount or rate of bone formation or osteogenesis in the subject).
- Reduced rates of bone formation, or rates of bone formation that are exceeded by the rate of bone resorption, can result in bone loss.
- the terms “increasing” and “decreasing” refer to modulating resulting in, respectively, greater or lesser amounts, of function, expression, or activity of a metric relative to a reference.
- the amount of a marker of a metric e.g., lean mass
- the metric is measured subsequent to administration at a time that the administration has had the recited effect, e.g., at least one week, one month, 3 months, or 6 months, after a treatment regimen has begun.
- fibrosis refers to the pathological process of excess formation of fibrous connective tissue. Fibrosis is characterized by fibroblast accumulation and collagen deposition in excess of normal deposition in any particular tissue. In response to inflammation or an injury to a tissue, nearby fibroblasts can migrate into the wound, proliferate, and produce large amounts of collagenous extracellular matrix. When fibrosis occurs in response to injury, the term “scarring” can be used as synonym.
- Fibrosis may occur in many tissues of the body, including, e.g., lungs, skin, liver, kidney, heart, eye, tendon, cartilage, pancreatic tissue, uterine tissue, neural tissue, testis, ovary, adrenal gland, artery, vein, bone marrow, colon, small and large intestine, biliary tract, and gut.
- pulmonary hypertension refers to a disease characterized by an increase in blood pressure between the heart and lungs, which can include an increase in blood pressure in pulmonary arteries (pulmonary arterial hypertension), pulmonary veins, or pulmonary capillaries.
- Pulmonary hypertension can have a number of symptoms, shortness of breath (dyspnea), fatigue, swelling (e.g., edema) of the legs, feet, belly (ascites), or neck, chest pain or pressure, racing pulse or heart palpitations, bluish color to lips or skin (cyanosis), dizziness, or fainting.
- PH also features reduce exercise tolerance and may lead to heart failure.
- PAH pulmonary arterial hypertension
- PAH refers to a form of pulmonary hypertension characterized by a narrowing or obstruction in the small pulmonary arteries, often caused by scarring, and an increase in pulmonary arterial blood pressure.
- PAH is also known as WHO Group I PH.
- PAH can be diagnosed based on an increase in blood pressure in the pulmonary artery mean pulmonary arterial pressure above 25 mmHg at rest, with a normal pulmonary artery capillary wedge pressure. PAH can lead to shortness of breath, dizziness, fainting, and other symptoms, all of which are exacerbated by exertion.
- PAH can be a severe disease with a markedly decreased exercise tolerance and heart failure.
- PAH PAH in which no predisposing factor is identified
- heritable PAH e.g., PAH associated with a mutation in BMPR2, ALK1 , SMAD9, caveolin 1 , KCNK3, or EIF2AK4
- mutations are located in the BMPR2 gene.
- Risk factors for the development of PAH include family history of PAH, drug use (e.g., methamphetamine or cocaine use), infection (e.g., HIV infection or schistosomiasis), cirrhosis of the liver, congenital heart abnormalities, portal hypertension, pulmonary veno-occlusive disease, pulmonary capillary hemangiomatosis, or connective tissue/autoimmune disorders (e.g., scleroderma or lupus).
- drug use e.g., methamphetamine or cocaine use
- infection e.g., HIV infection or schistosomiasis
- cirrhosis of the liver congenital heart abnormalities
- portal hypertension e.g., portal hypertension
- pulmonary veno-occlusive disease e.g., pulmonary capillary hemangiomatosis
- connective tissue/autoimmune disorders e.g., scleroderma or lupus
- venous pulmonary hypertension and “venous PH” refer to a form of pulmonary hypertension that is secondary to left heart disease.
- Venous PH is also known as WHO Group II PH.
- Venous PH may be associated with or caused by left ventricular systolic dysfunction (e.g., failure of the left ventricle), left ventricular diastolic dysfunction, valvular heart disease (e.g., mitral valve or aortic valve disease), congenital cardiomyopathy, or congenital/acquired pulmonary venous stenosis.
- left ventricular systolic dysfunction e.g., failure of the left ventricle
- left ventricular diastolic dysfunction e.g., valvular heart disease (e.g., mitral valve or aortic valve disease)
- congenital cardiomyopathy e.g., congenital cardiomyopathy
- congenital/acquired pulmonary venous stenosis e.g
- hypooxic pulmonary hypertension and “hypoxic PH” refer to a form of pulmonary hypertension that is due to lung disease or chronic hypoxia. This form of PH is also known as WHO Group III PH. Hypoxic PH may be associated with or caused by chronic obstructive pulmonary disease (e.g., emphysema), interstitial lung disease, sleep-disordered breathing (e.g., sleep apnea), lung disease (e.g., pulmonary fibrosis), alveolar hypoventilation disorders, chronic exposure to high altitude, or developmental abnormalities.
- chronic obstructive pulmonary disease e.g., emphysema
- interstitial lung disease e.g., sleep-disordered breathing
- sleep-disordered breathing e.g., sleep apnea
- lung disease e.g., pulmonary fibrosis
- alveolar hypoventilation disorders chronic exposure to high altitude, or
- thromboembolic pulmonary hypertension and “thromboembolic PH” refer to a form of pulmonary hypertension that is related to chronic arterial obstruction (e.g., blood clots). Thromboembolic PH is also known as WHO Group IV PH. Thromboembolic PH may be associated with or caused by chronic thromboembolic pulmonary hypertension, or other pulmonary artery obstructions (e.g., pulmonary emboli, angiosarcoma, arteritis, congenital pulmonary artery stenosis, or parasitic infection).
- pulmonary emboli e.g., pulmonary emboli, angiosarcoma, arteritis, congenital pulmonary artery stenosis, or parasitic infection.
- miscellaneous pulmonary hypertension and “miscellaneous PH” refer to a form of pulmonary hypertension with unclear or multifactorial mechanisms. This form of PH is categorized as WHO Group V PH.
- Miscellaneous PH may be associated with or caused by a hematologic disease (e.g., chronic hemolytic anemia, sickle cell disease), a systemic disease (e.g., sarcoidosis, pulmonary Langerhans cell histiocytosis, lymphangioleiomyomatosis, neurofibromatosis, or vasculitis), a metabolic disorder (e.g., glycogen storage disease, Gaucher disease, or thyroid diseases), pulmonary tumoral thrombotic microangiopathy, fibrosing mediastinitis, chronic kidney failure, or segmental pulmonary hypertension.
- a hematologic disease e.g., chronic hemolytic anemia, sickle cell disease
- a systemic disease e.g., sarcoidosis, pulmonary Langer
- the terms “increase red blood cell levels” and “promote red blood cell formation” refer to clinically observable metrics, such as hematocrit, red blood cell counts, and hemoglobin measurements, and are intended to be neutral as to the mechanism by which such changes occur.
- the term “low red blood cell levels” as used herein refers to red blood cell counts, hematocrit, and hemoglobin measurements that are below the range of values that is considered normal for the subject’s age and gender.
- the terms “red blood cell formation” and “red blood cell production” refer to the generation of red blood cells, such as the process of erythropoiesis in which red blood cells are produced in the bone marrow.
- the terms “increase platelet levels” and “promote platelet formation” refer to clinically observable metrics, such as platelet counts, and are intended to be neutral as to the mechanism by which such changes occur.
- the term “low platelet levels” as used herein refers to platelet counts that are below the range of values that is considered normal for the subject’s age and gender.
- the terms “platelet formation” and “platelet production” refer to the generation of platelets, such as the process in which platelets are produced from megakaryocytes.
- the terms “increase neutrophil levels” and “promote neutrophil formation” refer to clinically observable metrics, such as neutrophil counts, and are intended to be neutral as to the mechanism by which such changes occur.
- the term “low neutrophil levels” as used herein refers to neutrophil counts that are below the range of values that is considered normal for the subject’s age and gender.
- the terms “neutrophil formation” and “neutrophil production” refer to the generation of neutrophils such as the process in which neutrophils are produced in the bone marrow.
- anemia refers to any abnormality in hemoglobin or red blood cells that leads to reduced oxygen levels in the blood.
- Anemia can be associated with abnormal production, processing, or performance of erythrocytes and/or hemoglobin.
- the term anemia refers to any reduction in the number of red blood cells and/or level of hemoglobin in blood relative to normal blood levels.
- thrombocytopenia refers to a condition in which the blood contains a lower than normal number of platelets, which may be due to a deficiency in platelet production, accumulation of platelets within an enlarged spleen, or the destruction of platelets.
- Normal blood platelet levels range from about 150,000 to 450,000 per microliter blood in humans.
- a platelet count of less than 150,000 platelets per microliter is lower than normal. Bleeding can occur after a relatively minor injury if the platelet count falls below 50,000 platelets per microliter of blood, and serious bleeding may occur without any recognized injury if the platelet count falls below 10,000 to 20,000 platelets per microliter of blood.
- immune thrombocytopenia is used herein to refer to any type of thrombocytopenia arising from an autoimmune response directed against an individual's own platelets.
- Immune thrombocytopenia includes primary immune thrombocytopenia, in which autoimmune response is the original cause for the decrease in the platelet counts, such as idiopathic thrombocytopenic purpura.
- Immune thrombocytopenia also includes secondary immune thrombocytopenia, in which the decrease in platelet counts is associated with one or more other diseases that cause an individual's body to generate an autoimmune response against its own platelets, such as systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS), Evans syndrome, immune thyroid disease, leukemia (e.g., chronic lymphocytic leukemia or large granular T-lymphocyte lymphocytic leukemia), or chronic infection (e.g., with Helicobacter pylori, human immunodeficiency virus (HIV), or Hepatitis C).
- SLE systemic lupus erythematosus
- APS antiphospholipid syndrome
- Evans syndrome immune thyroid disease
- leukemia e.g., chronic lymphocytic leukemia or large granular T-lymphocyte lymphocytic leukemia
- chronic infection e.g., with Helicobacter pylori, human immunode
- neutrophils refers to a condition in which the blood contains an abnormally low number of neutrophils.
- the typical lower limit of the neutrophil count is about 1500 cells per microliter of blood. Below this level, the risk of infection increases. Neutropenia severity is classified as: mild (1000 to 1500 neutrophils per microliter of blood), moderate (500 to 1000 neutrophils per microliter of blood), and severe (below 500 neutrophils per microliter of blood). Neutropenia has many causes, but they typically fall into two main categories: destruction or depletion of neutrophils faster than the bone marrow can produce new neutrophils, or reduced production of neutrophils in the bone marrow.
- the term “low transfusion burden” refers to a condition of a subject that has received less than four units of red blood cells (RBCs) within eight weeks (e.g., 3, 2, 1 , or 0 units of RBCs within eight weeks) prior to treatment with an ActRII chimera described herein.
- RBCs red blood cells
- a subject with a low transfusion burden can be identified as having anemia based on measurements of mean hemoglobin concentration.
- a subject with a low transfusion burden and a mean hemoglobin concentration of less than 10.0 g/dL of two measurements performed at least one week apart prior to treatment with an ActRII chimera described herein is defined as having anemia.
- a subject with a low transfusion burden receives 1-3 units of RBCs (1-3 RBC transfusions) within eight weeks prior to treatment with an ActRII chimera described herein.
- a subject with a low transfusion burden does not receive any units of RBCs (0 RBC transfusions) within eight weeks prior to treatment with an ActRII chimera described herein.
- high transfusion burden refers to a condition of a subject requiring greater than or equal to four units of RBCs (e.g., 4, 5, 6, 7, 8, or more units) within eight weeks prior to treatment with an ActRII chimera described herein.
- a subject with a high transfusion burden can be identified as having anemia based on measurements of mean hemoglobin concentration.
- a subject with a high transfusion burden and a mean hemoglobin concentration of less than or equal to 9.0 g/dL is defined as having anemia.
- ineffective hematopoiesis refers to the failure to produce fully mature hematopoietic cells (e.g., the failure to produce red blood cells, platelets, and neutrophils). Ineffective hematopoiesis may be due to single or multiple defects, such as abnormal proliferation and/or differentiation of progenitor cells (e.g., an excessive production of progenitors that are unable to complete differentiation), that can lead to a hyperproliferation or a shortage of progenitor cells.
- erythropoiesis stimulating agent and “ESA” refer to a class of drugs that act on the proliferation stage of red blood cell development by expanding the pool of early-stage progenitor cells.
- erythropoiesis-stimulating agents are epoetin alfa and darbepoetin alfa.
- metabolic disease refers to a disease, disorder, or syndrome that is related to a subject’s metabolism, such as breaking down carbohydrates, proteins, and fats in food to release energy, and converting chemicals into other substances and transporting them inside cells for energy utilization and/or storage.
- Some symptoms of a metabolic disease include high serum triglycerides, high low-density cholesterol (LDL), low high-density cholesterol (HDL), and/or high fasting insulin levels, elevated fasting plasma glucose, abdominal (central) obesity, and elevated blood pressure.
- Metabolic diseases increase the risk of developing other diseases, such as cardiovascular disease.
- metabolic diseases include, but are not limited to, obesity, Type 1 diabetes, and Type 2 diabetes.
- treatment-related metabolic disease refers to a metabolic disease (e.g., obesity, Type 1 diabetes, or Type 2 diabetes) associated with a medication taken by the subject (e.g., a metabolic disease developed during treatment with the medication).
- the medication can be one that the subject continues to take, or one taken previously that led to the development of metabolic disease.
- glucocorticoids e.g., corticosteroids, such as prednisone
- SSRIs selective serotonin reuptake inhibitors
- SSRIs selective serotonin reuptake inhibitors
- SSRIs selective serotonin reuptake inhibitors
- mirtazapine mirtazapine
- fluoxetine e.g., escitalopram, sertraline
- tricyclic antidepressants e.g., amitriptyline
- mood stabilizers e.g., valproic acid, lithium
- antipsychotics e.g., olanzapine, chlorpromazine, clozapine
- diabetes medication e.g., insulin, chlorpropamide
- Medications associated with the development of diabetes include glucocorticoids (e.g., corticosteroids, which may cause glucocorticoid-induced diabetes mellitus), SSRIs, serotonin-norepinephrine reuptake inhibitors (SNRIs), mood stabilizers (e.g., lithium and valproic acid), and antipsychotics (e.g., olanzapine and clozapine).
- glucocorticoids e.g., corticosteroids, which may cause glucocorticoid-induced diabetes mellitus
- SSRIs serotonin-norepinephrine reuptake inhibitors (SNRIs)
- mood stabilizers e.g., lithium and valproic acid
- antipsychotics e.g., olanzapine and clozapine.
- the development of obesity may lead to the development of diabetes.
- the term “age-related metabolic disease” refers to a metabolic disease (e.g., obesity, Type 1 diabetes, or Type 2 diabetes) that develops with age. For example, the risk of diabetes increases with age and is more common in older adults, with approximately 25% of adults over 60 having diabetes. Adults can develop Type 2 diabetes or new-onset Type 1 diabetes. Rates of obesity also increase with age, with the highest rates of obesity in the United States occurring in adults aged 40-59 (with a prevalence of obesity of 45%). Aging also reduces the body’s ability to burn fat, leading to increased fat surrounding internal organs.
- a metabolic disease e.g., obesity, Type 1 diabetes, or Type 2 diabetes
- percentage of body weight gain refers to the percentage of gained body weight compared to a prior body weight of a subject at a prior time.
- the percentage of body weight gain can be calculated as follows:
- administration of a polypeptide including an extracellular ActRI I chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid molecule encoding a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- vector containing such a nucleic acid molecule to a subject can reduce the percentage of body weight gain of the subject.
- appetite for food intake refers to a subject’s natural desire or need for food.
- the appetite for food intake of a subject can be monitored by measuring the amount of food consumed after the polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) is administered.
- an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid molecule encoding a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- vector containing such a nucleic acid molecule to a subject does not affect the subject’s appetite for food intake.
- the term “adiposity” refers to the fat stored in the adipose tissue of a subject.
- administration of a polypeptide including extracellular ActRI I chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid molecule encoding a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- vector containing such a nucleic acid molecule to a subject can reduce the subject’s adiposity without affecting lean mass.
- the term “epididymal and perirenal fat pads” refers to the tightly packed fat cells in the epididymis and around the kidney.
- administration of a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid molecule encoding a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- vector containing such a nucleic acid molecule to a subject can reduce the weights of epididymal and perirenal fat pads of the subject.
- fasting insulin refers to a subject’s level of insulin while the subject has not had any food intake for a length of time (i.e. , 12-24 hours).
- Fasting insulin level is used in diagnosing metabolic diseases.
- Fasting insulin level is also used as an indication of whether a subject is at the risk of developing a metabolic disease. Normally, in a subject suffering from Type 1 diabetes, the subject’s fasting insulin level is low compared to that of a healthy subject. In a subject suffering from insulin resistance (i.e., Type 2 diabetes), the subject’s fasting insulin level is high compared to that of a healthy subject.
- a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid molecule encoding a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- vector containing such a nucleic acid molecule to a subject can modulate the subject’s fasting insulin level.
- the term “rate of glucose clearance” refers to the rate at which glucose is being cleared from the blood.
- the rate of glucose clearance can be measured in a glucose tolerance test (GTT).
- GTT glucose tolerance test
- a subject is given a certain amount of glucose and blood samples are taken afterward to determine how quickly it is cleared from the blood.
- the rate of glucose clearance can be used as a parameter in diagnosing and/or determining the risk of developing metabolic diseases such as obesity, diabetes, and insulin resistance.
- the term “serum lipid profile” refers to the measurement of the distribution of different types of lipids and lipoproteins in a subject’s serum. Such measurement can be accomplished by a panel of blood tests.
- the types of lipids and lipoproteins in a subject’s serum include, but are not limited to, cholesterol (e.g., high-density lipoprotein (HDL) and low-density lipoprotein (LDL)), triglyceride, and free fatty acid (FFA).
- the distribution of the different types of lipids and lipoproteins can be used as a parameter in diagnosing and/or determining the risk of developing metabolic diseases such as obesity, diabetes, and insulin resistance.
- High levels of cholesterol, especially low-density lipoprotein, is generally regarded as an indication or risk factor for developing certain metabolic diseases, or in some severe medical cases, cardiovascular diseases.
- administration of a polypeptide including an extracellular ActRI I chimera e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a nucleic acid molecule encoding a polypeptide including an extracellular ActRI I chimera e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- vector containing such a nucleic acid molecule to a subject improves the subject’s serum lipid profile such that the levels of cholesterol (especially low-density lipoprotein) and triglyceride are lowered.
- C-terminal extension refers to the addition of one or more amino acids to the C-terminus of a an extracellular ActRI I chimera (e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the C-terminal extension can be one or more amino acids, such as 1-6 amino acids (e.g., 1 , 2, 3, 4, 5, 6 or more amino acids).
- the C- terminal extension may include amino acids from the corresponding position of wild-type ActRIIA or ActRIIB.
- Exemplary C-terminal extensions are the amino acid sequence NP (a two amino acid C-terminal extension) and the amino acid sequence NPVTPK (SEQ ID NO: 104) (a six amino acid C-terminal extension). Any amino acid sequence that does not disrupt the activity of the polypeptide can be used.
- percent (%) identity refers to the percentage of amino acid (or nucleic acid) residues of a candidate sequence that are identical to the amino acid (or nucleic acid) residues of a reference sequence after aligning the sequences and introducing gaps, if necessary, to achieve the maximum percent identity (i.e. , gaps can be introduced in one or both of the candidate and reference sequences for optimal alignment and non-homologous sequences can be disregarded for comparison purposes). Alignment for purposes of determining percent identity can be achieved in various ways that are within the skill in the art, for instance, using publicly available computer software such as BLAST, ALIGN, or Megalign (DNASTAR) software.
- the percent amino acid (or nucleic acid) sequence identity of a given candidate sequence to, with, or against a given reference sequence is calculated as follows:
- A is the number of amino acid (or nucleic acid) residues scored as identical in the alignment of the candidate sequence and the reference sequence
- B is the total number of amino acid (or nucleic acid) residues in the reference sequence.
- the percent amino acid (or nucleic acid) sequence identity of the candidate sequence to the reference sequence would not equal to the percent amino acid (or nucleic acid) sequence identity of the reference sequence to the candidate sequence.
- a reference sequence aligned for comparison with a candidate sequence may show that the candidate sequence exhibits from 50% to 100% identity across the full length of the candidate sequence or a selected portion of contiguous amino acid (or nucleic acid) residues of the candidate sequence.
- the length of the candidate sequence aligned for comparison purpose is at least 30%, e.g., at least 40%, e.g., at least 50%, 60%, 70%, 80%, 90%, or 100% of the length of the reference sequence.
- serum half-life refers to, in the context of administering a therapeutic protein to a subject, the time required for plasma concentration of the protein in the subject to be reduced by half.
- the protein can be redistributed or cleared from the bloodstream, or degraded, e.g., by proteolysis. Serum half-life comparisons can be made by comparing the serum half-life of Fc fusion proteins.
- lean mass refers to a component of body composition which includes, e.g., lean mass, body fat, and body fluid. Normally lean mass is calculated by subtracting the weights of body fat and body fluid from total body weight. Typically, a subject’s lean mass is between 60% and 90% of totally body weight.
- a polypeptide including an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 e.g., SEQ ID NOs: 22-43
- a nucleic acid molecule encoding a polypeptide including an extracellular ActRII chimera e.g., extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- vector containing such a nucleic acid molecule to a subject increases the subject’s lean mass.
- binding affinity refers to the strength of the binding interaction between two molecules.
- binding affinity refers to the strength of the sum total of non-covalent interactions between a molecule and its binding partner, such as an extracellular ActRII chimera and BMP9 or activin A.
- binding affinity refers to intrinsic binding affinity, which reflects a 1 :1 interaction between members of a binding pair.
- the binding affinity between two molecules is commonly described by the dissociation constant (KD) or the affinity constant (KA). TWO molecules that have low binding affinity for each other generally bind slowly, tend to dissociate easily, and exhibit a large KD.
- TWO molecules that have high affinity for each other generally bind readily, tend to remain bound longer, and exhibit a small KD.
- the KD of two interacting molecules may be determined using methods and techniques well known in the art, e.g., surface plasmon resonance. KD is calculated as the ratio of kon/kon .
- muscle mass refers to the primary component of lean mass. Muscle mass can be measured experimentally by measuring muscle weight.
- neuromuscular disease refers to a disease that affects voluntary or involuntary muscle function due to problems in the nerves and muscles, typically leading to muscle weakness.
- exemplary neuromuscular diseases include amyotrophic lateral sclerosis (ALS), autonomic neuropathy, botulism, Charcot-Marie-Tooth disease (CMT), chronic inflammatory demyelinating polyradiculoneuropathy, congenital myasthenic syndrome, congenital myopathies, cramp-fasciculation syndrome, dermatomyositis, diabetic neuropathy, distal myopathies, dystrophinopathies, endocrine myopathies, focal muscular atrophies, glycogen storage disease type II, Guillain-Barre syndrome, hereditary spastic paraplegia, inclusion body myositis (IBM), Isaac’s syndrome, Kearns-Sayre syndrome, Kennedy disease, Lambert-Eaton myasthenic syndrome, metabolic myopathies, metabolic neuropathies, mitochondrial myopathies
- DMD Duchenne
- BMD Becker
- DM myotonic
- FSHD limb-girdle
- LGMD distal
- DD oculopharyngeal
- EDMD Emery-Dreifuss
- congenital e.g., MDC1A, MDC1B, MDC1C, FCMD, WWS, RSMD1 , MEB, and UCMD
- myasthenia gravis myotonic dystrophy, necrotizing myopathies, neuromyotonia, neuropathy of Friedreich’s Ataxia, nutritional neuropathy, peripheral neuropathy, polymyositis, primary lateral sclerosis, Schwartz-Jampel Syndrome, small fiber neuropathy, spinal and bulbar muscular atrophy, spinal muscular atrophy, spinal muscular atrophy with respiratory distress type 1 , spinocerebellar ataxia, stiff person syndrome, toxic neuropathy, and Troyer syndrome.
- a neuromuscular disease may be inherited in an autosomal dominant
- the phrase “affecting myostatin, activin A, activin B, and/or BMP9 signaling” means changing the binding of myostatin, activin A, activin B, and/or BMP9 to their receptors, e.g., ActRIIA, ActRIIB, and BMPRII (e.g., endogenous receptors).
- a polypeptide including an extracellular ActRI I chimera described herein reduces or inhibits the binding of myostatin, activin A, activin B, and/or BMP9 to their receptors, e.g., ActRIIA, ActRIIB, and BMPRII (e.g., endogenous ActRIIA and/or ActRIIB).
- vascular complication refers to a vascular disorder or any damage to the blood vessels, such as damage to the blood vessel walls. Damage to the blood vessel walls may cause an increase in vascular permeability or leakage.
- vascular permeability or leakage refers to the capacity of the blood vessel walls to allow the flow of small molecules, proteins, and cells in and out of blood vessels.
- An increase in vascular permeability or leakage may be caused by an increase in the gaps (e.g., an increase in the size and/or number of the gaps) between endothelial cells that line the blood vessel walls and/or thinning of the blood vessel walls.
- polypeptide describes a single polymer in which the monomers are amino acid residues which are covalently conjugated together through amide bonds.
- a polypeptide is intended to encompass any amino acid sequence, either naturally occurring, recombinant, or synthetically produced.
- the term “homodimer” refers to a molecular construct formed by two identical macromolecules, such as proteins or nucleic acids.
- the two identical monomers may form a homodimer by covalent bonds or non-covalent bonds.
- an Fc domain may be a homodimer of two Fc domain monomers if the two Fc domain monomers contain the same sequence.
- a polypeptide described herein including an extracellular ActRI I chimera fused to an Fc domain monomer may form a homodimer through the interaction of two Fc domain monomers, which form an Fc domain in the homodimer.
- heterodimer refers to a molecular construct formed by two different macromolecules, such as proteins or nucleic acids.
- the two monomers may form a heterodimer by covalent bonds or non-covalent bonds.
- a polypeptide described herein including an extracellular ActRII chimera fused to an Fc domain monomer may form a heterodimer through the interaction of two Fc domain monomers, each fused to a different ActRII chimera, which form an Fc domain in the heterodimer.
- the term “host cell” refers to a vehicle that includes the necessary cellular components, e.g., organelles, needed to express proteins from their corresponding nucleic acids.
- the nucleic acids are typically included in nucleic acid vectors that can be introduced into the host cell by conventional techniques known in the art (transformation, transfection, electroporation, calcium phosphate precipitation, direct microinjection, etc.).
- a host cell may be a prokaryotic cell, e.g., a bacterial cell, or a eukaryotic cell, e.g., a mammalian cell (e.g., a CHO cell or a HEK293 cell).
- the term “therapeutically effective amount” refers an amount of a polypeptide, nucleic acid, or vector of the invention or a pharmaceutical composition containing a polypeptide, nucleic acid, or vector of the invention effective in achieving the desired therapeutic effect in treating a patient having a or at risk of developing a disease, such as a muscle disease, a condition involving weakness and atrophy of muscles (e.g., a neuromuscular disease, such as a muscular dystrophy, IBM, ALS, SMA, CMT, myasthenia gravis, or multiple sclerosis; sarcopenia; or cachexia), a disease or condition involving bone damage (e.g., osteoporosis, or a condition involving bone damage, e.g., primary osteoporosis, secondary osteoporosis, osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis- related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, osteogenesis
- the term “pharmaceutical composition” refers to a medicinal or pharmaceutical formulation that includes an active ingredient as well as excipients and diluents to enable the active ingredient suitable for the method of administration.
- the pharmaceutical composition of the present invention includes pharmaceutically acceptable components that are compatible with the polypeptide, nucleic acid, or vector.
- the pharmaceutical composition may be in tablet or capsule form for oral administration or in aqueous form for intravenous or subcutaneous administration.
- the term “pharmaceutically acceptable carrier or excipient” refers to an excipient or diluent in a pharmaceutical composition.
- the pharmaceutically acceptable carrier must be compatible with the other ingredients of the formulation and not deleterious to the recipient.
- the pharmaceutically acceptable carrier or excipient must provide adequate pharmaceutical stability to the polypeptide including an extracellular ActRI I chimera, the nucleic acid molecule(s) encoding the polypeptide, or a vector containing such nucleic acid molecule(s).
- the nature of the carrier or excipient differs with the mode of administration. For example, for intravenous administration, an aqueous solution carrier is generally used; for oral administration, a solid carrier is preferred.
- the term “treating and/or preventing” refers to the treatment and/or prevention of a disease, e.g., a muscle disease (e.g., a neuromuscular disease, such as a muscular dystrophy, IBM, SMA, CMT, ALS, myasthenia gravis, or multiple sclerosis; sarcopenia; or cachexia), a bone disease (e.g., a disease or condition involving bone damage, e.g., osteoporosis, osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, osteogenesis imperfecta, neuromuscular disease-related bone loss, burn- induced bone loss, anorexia-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity-related bone loss, or immobility-related bone loss), a disease involving low blood cell levels (e.g., anemia or blood
- treating a muscle, bone, low blood cell, low platelet, low neutrophil, metabolic, or fibrotic disease, or PH occurs after a subject has developed the muscle, bone, low blood cell, low platelet, low neutrophil, metabolic, or fibrotic disease, or PH and/or is already diagnosed with the muscle, bone, low blood cell, low platelet, low neutrophil, metabolic, or fibrotic disease, or PH.
- Preventing a muscle, bone, low blood cell, low platelet, low neutrophil, metabolic, or fibrotic disease, or PH refers to steps or procedures taken when a subject is at risk of developing the muscle, bone, low blood cell, low platelet, low neutrophil, metabolic, or fibrotic disease, or PH (.
- the subject may show signs or mild symptoms that are judged by a physician to be indications or risk factors for developing the muscle, bone, low blood cell, low platelet, low neutrophil, metabolic, or fibrotic disease, or PH, have another disease or condition associated with the development of the muscle, bone, low blood cell, low platelet, low neutrophil, metabolic, or fibrotic disease, or PH, be undergoing treatment that may cause anemia, thrombocytopenia, neutropenia, fibrosis, obesity or diabetes, or loss of bone density (e.g., surgery, chemotherapy, or radiation), or have a family history or genetic predisposition to developing the muscle, bone, low blood cell, low platelet, low neutrophil, metabolic or fibrotic disease, or PH , but has not yet developed the disease.
- a physician may show signs or mild symptoms that are judged by a physician to be indications or risk factors for developing the muscle, bone, low blood cell, low platelet, low neutrophil, metabolic, or fibrotic disease, or PH, have another disease or
- the term “subject” refers to a mammal, e.g., preferably a human. Mammals include, but are not limited to, humans and domestic and farm animals, such as monkeys (e.g., a cynomolgus monkey), mice, rats, dogs, cats, horses, sheep, goats, rabbits, and cows, etc.
- monkeys e.g., a cynomolgus monkey
- mice e.g., a cynomolgus monkey
- mice e.g., a cynomolgus monkey
- FIG. 1 is a schematic showing the amino acid sequence of exemplary extracellular ActRII chimeras. Sequence corresponding to wild-type extracellular ActRII A is shown in bold and sequence corresponding to wild-type extracellular ActRIIB is shown in italics. Amino acid substitutions that are not derived from the sequence of ActRIIA or ActRIIB are shown in bold italics.
- FIG. 2 is a bar graph showing the effects of extracellular ActRII chimeras on body weight. Mice received a single hydrodynamic injection of a plasmid construct encoding the indicated ActRII chimera or vehicle.
- FIG. 3 is a bar graph showing the effects of extracellular ActRII chimeras on lean mass. Mice received a single hydrodynamic injection of a plasmid construct encoding the indicated ActRII chimera or vehicle.
- FIG. 4 is a bar graph showing the effects of extracellular ActRII chimeras on body weight. Mice received an intraperitoneal injection of the indicated recombinant ActRII chimera or a vehicle control twice weekly for four weeks.
- FIG. 5 is a bar graph showing the effects of extracellular ActRII chimeras on lean mass. Mice received an intraperitoneal injection of the indicated recombinant ActRII chimera or a vehicle control twice weekly for four weeks.
- FIGS. 6A-6D are a series of bar graphs showing the effects of extracellular ActRI I chimeras on hematology parameters.
- HDI hydrodynamic tail vain injection
- EDTA was used as an anticoagulant and blood was analyzed using a Heska HT5 veterinary blood analyzer.
- FIGS. 6A-6D The effect of extracellular ActRI I chimeras on red blood cell, hemoglobin, and hematocrit levels and absolute reticulocytes is shown in FIGS. 6A-6D. Data are shown as average ⁇ SEM. Statistics are shown relative to vehicle treatment using a 1-way ANOVA with a Fisher’s LSD post test. *** P ⁇ 0.001 , **** P ⁇ 0.0001 .
- FIG. 7 is a bar graph showing the effect of ActRII chimeras on lean mass.
- HDI hydrodynamic tail vain injection
- mice were weight and lean mass determined using a small rodent nuclear magnetic resonance (NMR) analyzer (Bruker, Minispec LF50). The study was terminated after 28 days and terminal body and lean mass were determined.
- FIG. 7 shows the effect of the extracellular ActRII chimeras on lean mass. Data are shown as average ⁇ SEM. Statistics are shown relative to vehicle treatment using a 1-way ANOVA with a Fisher’s LSD post test. * P ⁇ 0.05 and **** P ⁇ 0.0001.
- FIGS. 8A-8D are a series of bar graphs showing the effects of extracellular ActRII chimeras on bone density and structure.
- HDI hydrodynamic tail vain injection
- FIGS. 8A-8D The effect of the extracellular ActRII chimeras on tibial bone mineral density, trabecular bone volume fraction of the proximal end of the tibia, trabecular spacing within the proximal end of the tibia, and trabecular number of the proximal end of the tibia are shown in FIGS. 8A-8D. Data are shown as average ⁇ SEM. Statistics are shown relative to vehicle treatment using a 1- way ANOVA with a Fisher’s LSD post test. * P ⁇ 0.05, ** P ⁇ 0.01 , *** P ⁇ 0.001 , **** P ⁇ 0.0001.
- a polypeptide of the invention includes an extracellular activin receptortype II (ActRII) chimera.
- a polypeptide of the invention includes an extracellular ActRII chimera fused to a moiety (e.g., Fc domain monomer, a wild-type Fc domain, an Fc domain with amino acid substitutions (e.g., one or more substitutions that reduce dimerization), an albumin-binding peptide, a fibronectin domain, or a human serum albumin).
- a polypeptide including an extracellular ActRII chimera fused to an Fc domain monomer may also form a dimer (e.g., homodimer or heterodimer) through the interaction between two Fc domain monomers.
- the ActRII chimeras described herein may have reduced binding to bone morphogenetic protein 9 (BMP9) relative to the wild-type extracellular ActRIIB, or have weak binding affinity or no binding affinity to BMP9 compared to binding affinity to activins (e.g., activin A and/or activin B) and myostatin.
- BMP9 bone morphogenetic protein 9
- the invention also includes methods of treating diseases and conditions involving weakness and atrophy of muscles by increasing muscle mass, lean mass, and/or muscle strength, methods of treating or preventing bone damage by increasing bone mineral density, increasing bone formation, or decreasing bone resorption, methods of treating or preventing fibrosis, methods of treating or preventing low blood cell levels (e.g., anemia or blood loss) by increasing red blood cell levels (e.g., red blood cell count, hemoglobin levels, or hematocrit), red blood cell production, or erythroid progenitor maturation and/or differentiation (e.g., the maturation and/or differentiation of early-stage or late- (e.g., terminal) stage erythroid progenitors into proerythroblasts, reticulocytes, or red blood cells), late-stage precursor (erythroid precursor) maturation (e.g., terminal maturation, such as the maturation of reticulocytes into red blood cells or the maturation of erythroblasts into reticulocytes and/or red blood cells
- Activin type II receptors are single transmembrane domain receptors that modulate signals for ligands in the transforming growth factor b (TGF-b) superfamily.
- Ligands in the TGF-b superfamily are involved in a host of physiological processes, such as muscle growth, vascular growth, cell differentiation, homeostasis, hematopoiesis, and osteogenesis.
- Examples of ligands in the TGF-b superfamily include, e.g., activin (e.g., activin A and activin B), inhibin, growth differentiation factors (GDFs) (e.g., GDF8, also known as myostatin, and GDF11), and bone morphogenetic proteins (BMPs) (e.g., BMP9).
- GDFs growth differentiation factors
- BMPs bone morphogenetic proteins
- Myostatin and activins are known to play a role in the regulation of skeletal muscle growth. For example, mice without myostatin show a large increase in skeletal muscle mass. Myostatin has also been implicated in promoting fibrosis. Mice lacking myostatin show a reduction in muscle fibrosis, and injection of myostatin-coated beads induces muscle fibrosis in mice. Mice overexpressing an activin subunit that leads to the production of diffusible activin A also exhibit fibrosis. In addition, activins are expressed abundantly in bone tissues and regulate bone formation by controlling both osteoblast and osteoclast functions. Activin A has been reported to be upregulated in bone disease and inhibits osteoblast activity.
- Myostatin is also implicated in bone homeostasis through increasing osteogenesis and inhibiting osteoblast activity.
- TGF-b signaling pathways also regulate hematopoiesis, with signaling pathways involving activins preventing the differentiation of red blood cell, platelet, and neutrophil progenitor cells in order to maintain progenitor cells in a quiescent state, and signaling pathways involving BMPs promoting differentiation of progenitor cells.
- Homeostasis of this process is essential to ensure that all cell types, including red cells, white cells, and platelets, are properly replenished in the blood.
- activin receptor ligand GDF11 has been found to be overexpressed in a mouse model of hemolytic anemia and associated with defects in red blood cell production.
- Elevated activin A has also been observed in clinical and experimental pulmonary hypertension. Furthermore, activins are highly expressed in adipose tissue, and increased myostatin levels and activin receptor levels have been observed in subcutaneous and visceral fat of obese mice. Additionally, myostatin has been shown to be elevated in skeletal muscle and plasma of obese and insulin resistant women, and both type I and type II activin receptors have been linked to pancreatic function and diabetes.
- activin receptor ligands e.g., activin A, activin B, myostatin
- increased expression of activin receptors themselves could contribute to a variety of diseases and conditions, including muscle atrophy or weakness, fibrosis, bone disease, anemia, thrombocytopenia, neutropenia, pulmonary hypertension, and metabolic disease.
- Methods that reduce or inhibit activin A, activin B, or myostatin signaling could, therefore, be used in the treatment of diseases and conditions involving muscle atrophy or weakness, fibrosis, bone damage, low red blood cell levels (e.g., anemia), low platelet levels (e.g., thrombocytopenia), low neutrophil levels (e.g., neutropenia), pulmonary hypertension (e.g., PAH, venous PH, hypoxic PH, thromboembolic PH, or miscellaneous PH), or metabolic disorders (e.g., obesity, Type 1 diabetes, or Type 2 diabetes).
- low red blood cell levels e.g., anemia
- low platelet levels e.g., thrombocytopenia
- neutrophil levels e.g., neutropenia
- pulmonary hypertension e.g., PAH, venous PH, hypoxic PH, thromboembolic PH, or miscellaneous PH
- metabolic disorders
- ActRIIA activin type II receptors
- ActRIIB activin type II receptors
- Studies have shown that BMP9 binds ActRIIB with about 300-fold higher binding affinity than ActRIIA (see, e.g., Townson et al., J. Biol. Chem. 287:27313, 2012).
- ActRIIA-Fc is known to have a longer half-life compared to ActRIIB-Fc.
- the present invention describes extracellular ActRI I chimeras that are constructed by combining portions of extracellular ActRIIA and ActRIIB with the goal of generating proteins that bind to ActRII ligands (e.g., activin A, activin B, myostatin, and GDF11) and retain the function of wild-type extracellular ActRII proteins (e.g., the ability to increase muscle mass and/or lean mass or red blood cell levels).
- the ActRII chimeras exhibit reduced BMP9 binding relative to wild-type extracellular ActRIIB, which can prevent or reduce disruption of endogenous BMP9 signaling.
- the chimeras have properties of both ActRIIA (e.g., low binding affinity to BMP9, the ability to increase red blood cell levels, and/or longer serum half-life as an Fc fusion protein) and ActRIIB (e.g., the ability to increase muscle mass).
- ActRIIA e.g., low binding affinity to BMP9, the ability to increase red blood cell levels, and/or longer serum half-life as an Fc fusion protein
- ActRIIB e.g., the ability to increase muscle mass
- the ActRII chimeras have reduced binding affinity for BMP9 compared to wild-type extracellular ActRIIB, and confer increases in lean mass, muscle mass, bone mineral density, and/or red blood cell levels (e.g., increase red blood cell production and/or red cell mass or volume), decreases in body weight and/or body fat, and/or treat muscle disease (e.g., a neuromuscular disease, such as a muscular dystrophy, IBM, SMA, CMT, ALS, myasthenia gravis, or multiple sclerosis; sarcopenia; or cachexia), bone disease (e.g., a disease or condition involving bone damage, e.g., osteoporosis, osteopenia, osteopetrosis, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, osteogenesis imperfecta, neuromuscular disease-related bone loss, burn-induced bone loss, anorexia-related bone loss, diet
- the ActRII chimeras may exhibit similar or improved binding to activins (e.g., activin A and/or activin B) and/or myostatin compared to wild-type extracellular ActRIIA and/or ActRIIB, allowing them to compete with endogenous activin receptors for ligand binding and reduce or inhibit endogenous activin receptor signaling.
- activins e.g., activin A and/or activin B
- myostatin compared to wild-type extracellular ActRIIA and/or ActRIIB, allowing them to compete with endogenous activin receptors for ligand binding and reduce or inhibit endogenous activin receptor signaling.
- the chimeras can be used to treat disorders in which activin receptor signaling is elevated, such as bone disease, muscle disease, fibrosis, PH, metabolic disease, thrombocytopenia, neutropenia, and/or anemia, leading to a reduction in bone resorption or osteoclast activity, an increase in bone formation or bone mineral density, an increase in muscle mass, lean mass, or muscle strength, a reduction in fibrosis (e.g., reduced fibrosis or a slowing or stopping of the progression of fibrosis), an increase red blood cell levels (e.g., an increase in hemoglobin levels, hematocrit, or red blood cell counts, e.g., an increase in red blood cell production and/or red cell mass or volume), an increase in the maturation and/or differentiation of erythroid progenitors (e.g., early-stage or late- (e.g., terminal) stage erythroid progenitors, e.g., maturation and/or differentiation of early-stage
- Polypeptides described herein include an extracellular ActRI I chimera containing sequence from both the extracellular portion of ActRIIB and the extracellular portion of ActRIIA.
- the ActRII chimeras described herein result from joining an N-terminal portion of extracellular ActRIIB (SEQ ID NO: 45 shown above) to a C-terminal portion of extracellular ActRIIA (SEQ ID NO: 44 shown above) such that the sequences are contiguous (e.g., the ActRIIA sequence continues where the ActRIIB sequence left off, starting with the next the amino acid located in the corresponding position of ActRIIA).
- the N-terminus of the ActRII chimera includes the six amino acids found at the N-terminus of extracellular ActRIIA joined to the fifth amino acid of extracellular ActRIIB. In some embodiments, the N-terminus of the ActRII chimera begins with the first amino acid located at the N-terminus of extracellular ActRIIB.
- the N-terminal portion of ActRIIB begins with the amino acid in the fifth position of SEQ ID NO: 45 (A), while in other embodiments (e.g., in embodiments in which the six amino acids found at the N-terminus of extracellular ActRIIA are not included in the chimera), the N- terminal portion of ActRIIB begins with the amino acid in the first position of SEQ ID NO: 45 (G).
- the N-terminus of the ActRII chimera includes the first ten amino acids found at the N- terminus of extracellular ActRIIA joined to the ninth amino acid of extracellular ActRIIB, in which case the N-terminal portion of ActRIIB begins with the amino acid in the ninth position of SEQ ID NO: 45 (E).
- the extracellular ActRII chimera may also include one or more amino acid substitutions in the portion of the chimera that corresponds to the sequence of ActRIIB compared to wild-type extracellular ActRIIB (e.g., SEQ ID NO: 45 shown above), and one or more amino acid substitutions in the portion of the chimera that corresponds to the sequence of ActRIIA compared to wild-type extracellular ActRIIA (e.g., SEQ ID NO: 44 shown above). Amino acid substitutions at 9 different positions may be introduced into an extracellular ActRII chimera (Table 1).
- An extracellular ActRII chimera may have one or more (e.g., 1 , 2, 3, 4, 5, 6, 7, 8, or 9) amino acid substitutions relative the sequence of a wild-type sequence (e.g., relative to the sequence of wild-type extracellular ActRIIB (SEQ ID NO: 45) if the portion of the chimera corresponds to a region of wild-type extracellular ActRIIB, or relative to the sequence of wild-type extracellular ActRIIA (SEQ ID NO: 44) if the portion of the chimera corresponds to a region of wild-type extracellular ActRIIA).
- the positions at which amino acid substitutions may be made, as well as the amino acids that may be substituted at these positions, are listed in Table 1.
- Amino acid substitutions can alter the activity and/or binding affinity of the extracellular ActRII chimeras of the invention.
- the extracellular ActRII chimeras bind to activin A, activin B, myostatin, and/or GDF11 with sufficient affinity to compete with endogenous activin receptors for binding to one or more of these ligands.
- the extracellular ActRII chimeras of the invention have reduced, weak, or no substantial binding to BMP9 (e.g., compared to wild-type ActRIIB). BMP9 binding may be reduced in extracellular ActRII chimeras containing the amino acid sequence TEEN orTKEN at positions X3, X4, Xs, and Cb.
- a polypeptide of the invention including an extracellular ActRII chimera e.g., any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) with the sequence TEEN at positions X3, X4, Xs, and Cb can have a substitution of the amino acid K for the amino acid E at position X4.
- a polypeptide of the invention including an extracellular ActRII chimera e.g., any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) with the sequence TKEN at positions X3, X4, Xs, and Cb can have a substitution of the amino acid E for the amino acid K at position X 4 .
- the sequences TEEN and TKEN can be used interchangeably in the extracellular ActRII chimeras (e.g., the chimeras in Tables 1 and 2, e.g., SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22- 43)) of the invention.
- the extracellular ActRII chimeras of the invention may further include a C-terminal extension (e.g., additional amino acids at the C-terminus).
- the C-terminal extension can add one or more additional amino acids at the C-terminus (e.g., 1 , 2, 3, 4, 5, 6 or more additional amino acids) to any of the chimeras shown in Tables 1 and 2 (e.g., SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the C- terminal extension may correspond to sequence from the same position in wild-type ActRIIA or ActRIIB.
- C-terminal extensions that can be included in the extracellular ActRII chimeras of the invention are the amino acid sequence NP and the amino acid sequence NPVTPK (SEQ ID NO: 104), which correspond to sequence found in the same position in wild-type ActRIIA.
- Xi is D
- X 2 is I, F, or E
- X 3 is N or T
- X 4 is A or E
- X 5 is T or K
- X 6 is E or K
- X 7 is E or D
- X 8 is N or S
- Xg is E or Q.
- Xi is D
- X 2 is I or F
- X 3 is N
- X 4 is A or E
- X 5 is T or K
- X 6 is E or K
- X 7 is E or D
- X 8 is N or S
- X 9 is E or Q.
- a polypeptide described herein includes an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 22-43 (Table 2).
- the extracellular ActRII chimeras described herein have an N-terminal truncation of 1-9 amino acids (e.g., 1 , 2, 3, 4, 5, 6, 7, 8, or 9 amino acids).
- the N-terminal truncation can involve the removal of 1-9 amino acids from the N-terminus of any of the chimeras shown in Tables 1 and 2 (e.g., SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the N-terminal truncation can remove amino acids up two to amino acids before the first cysteine (e.g., the two amino acids before the first cysteine (RE or QE) are retained in the N-terminally truncated ActRII chimeras).
- Exemplary ActRII chimeras having N-terminal truncations are provided in Table 3, below. Table 3. Extracellular ActRII chimeras having N-terminal truncations
- a polypeptide of the invention including an extracellular ActRII chimera may further include a moiety (e.g., Fc domain monomer, a wild-type Fc domain, an Fc domain with amino acid substitutions (e.g., one or more substitutions that reduce dimerization), an albumin-binding peptide, a fibronectin domain, or a human serum albumin), which may be fused to the N- or C-terminus (e.g., C- terminus) of the extracellular ActRII chimera by way of a linker or other covalent bonds.
- a moiety e.g., Fc domain monomer, a wild-type Fc domain, an Fc domain with amino acid substitutions (e.g., one or more substitutions that reduce dimerization), an albumin-binding peptide, a fibronectin domain, or a human serum albumin
- a polypeptide including an extracellular ActRII chimera fused to an Fc domain monomer may form a dimer (e.g., homodimer or heterodimer) through the interaction between two Fc domain monomers, which combine to form an Fc domain in the dimer.
- a dimer e.g., homodimer or heterodimer
- Exemplary polypeptides containing an ActRII chimera, an Fc domain, and a linker are provided in Table 4, below.
- the terminal lysine is absent from the Fc domain amino acid sequence.
- a polypeptide described herein has a serum half-life of at least 7 days in humans.
- the polypeptide may bind to activin A with a KD of 10 pM or higher.
- the polypeptide binds to activin A, activin B, and/or myostatin and exhibits reduced (e.g., weak) binding to BMP9 (e.g., compared to wild-type extracellular ActRIIB).
- the polypeptide that has reduced or weak binding to BMP9 has the sequence TEEN orTKEN at positions X3, X4, Xs, and Cb.
- the polypeptide that has reduced or weak binding to BMP9 has the sequence KKDS or TKDS at positions X3, X4, Xs, and Xe. In some embodiments, the polypeptide does not substantially bind to human BMP9.
- the polypeptide may bind to human activin A with a KD of about 800 pM or less (e.g., a K D of about 800, 700, 600, 500, 400, 300, 200, 100, 90, 80, 70, 60, 50, 40, 30, 20, 10, 9, 8, 7, 6, 5, 4, 3, 2, or 1 pM or less, e.g., a KD of between about 800 pM and about 30 pM).
- a KD of about 800 pM or less e.g., a K D of about 800, 700, 600, 500, 400, 300, 200, 100, 90, 80, 70, 60, 50, 40, 30, 20, 10, 9, 8, 7, 6, 5, 4, 3, 2, or 1 pM or less, e.g., a KD of between about 800 pM and about 30 pM.
- the polypeptide may bind to human activin B with a KD of 800 pM or less (e.g., a KD of about 800, 700, 600, 500, 400, 300, 200, 100, 90, 80, 70, 60, 50, 40, 30, 20, 10, 9, 8, 7, 6, 5, 4, 3, 2, or 1 pM or less, e.g., a KD of between about 800 pM and about 5 pM)
- the polypeptide may also bind to growth and differentiation factor 11 (GDF-11) with a KD of approximately 5 pM or higher (e.g., a KD of about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 55, 60, 65, 70, 75, 80, 85, 90, 95, 100, 105, 110, 115, 120,
- GDF-11 growth and differentiation factor 11
- a polypeptide described herein may include an extracellular ActRII chimera fused to an Fc domain monomer of an immunoglobulin or a fragment of an Fc domain to increase the serum half-life of the polypeptide.
- a polypeptide including an extracellular ActRII chimera fused to an Fc domain monomer may form a dimer (e.g., homodimer or heterodimer) through the interaction between two Fc domain monomers, which form an Fc domain in the dimer.
- an Fc domain is the protein structure that is found at the C-terminus of an immunoglobulin.
- An Fc domain includes two Fc domain monomers that are dimerized by the interaction between the CH3 antibody constant domains.
- a wild-type Fc domain forms the minimum structure that binds to an Fc receptor, e.g., FcyRI, FcyRIla, FcyRIIb, FcyRIIIa, FcyRIIIb, FcyRIV.
- an Fc domain may be mutated to lack effector functions, typical of a “dead” Fc domain.
- an Fc domain may include specific amino acid substitutions that are known to minimize the interaction between the Fc domain and an Fey receptor.
- an Fc domain is from an lgG1 antibody and includes amino acid substitutions L234A, L235A, and G237A.
- an Fc domain is from an lgG1 antibody and includes amino acid substitutions D265A, K322A, and N434A.
- the aforementioned amino acid positions are defined according to Kabat (Sequences of Proteins of Immunological Interest, 5th Ed. Public Health Service, National Institutes of Health, Bethesda, MD. (1991)).
- an Fc domain does not induce any immune system-related response.
- the Fc domain in a dimer of a polypeptide including an extracellular ActRII chimera fused to an Fc domain monomer may be modified to reduce the interaction or binding between the Fc domain and an Fey receptor.
- the sequence of an Fc domain monomer that may be fused to an extracellular ActRII chimera is shown below (SEQ ID NO: 48):
- an Fc domain is from an lgG1 antibody and includes amino acid substitutions L12A, L13A, and G15A, relative to the sequence of SEQ ID NO: 48. In some embodiments, an Fc domain is from an lgG1 antibody and includes amino acid substitutions D43A, K100A, and N212A, relative to the sequence of SEQ ID NO: 48. In some embodiments, the terminal lysine is absent from the Fc domain monomer having the sequence of SEQ ID NO: 48.
- an extracellular ActRII chimera described herein may be fused to the N- or C-terminus of an Fc domain monomer (e.g., SEQ ID NO: 48) through conventional genetic or chemical means, e.g., chemical conjugation.
- a linker e.g., a spacer
- the Fc domain monomer can be fused to the N- or C-terminus (e.g., C- terminus) of the extracellular ActRII chimera.
- a polypeptide described herein may include an extracellular ActRII chimera fused to an Fc domain.
- the Fc domain contains one or more amino acid substitutions that reduce or inhibit Fc domain dimerization.
- the Fc domain contains a hinge domain.
- the Fc domain can be of immunoglobulin antibody isotype IgG, IgE, IgM, IgA, or IgD. Additionally, the Fc domain can be an IgG subtype (e.g., lgG1 , lgG2a, lgG2b, lgG3, or lgG4).
- the Fc domain can also be a non-naturally occurring Fc domain, e.g., a recombinant Fc domain.
- one or more amino acids with large side-chains may be introduced to the CH3-CH3 dimer interface to hinder dimer formation due to steric clash.
- one or more amino acids with small side-chains e.g., alanine, valine, or threonine
- Methods of introducing amino acids with large or small side-chains in the CH3 domain are described in, e.g., Ying et al. ( J Biol Chem.
- one or more amino acid residues in the CH3 domain that make up the CH3-CH3 interface between two Fc domains are replaced with positively-charged amino acid residues (e.g., lysine, arginine, or histidine) or negatively-charged amino acid residues (e.g., aspartic acid or glutamic acid) such that the interaction becomes electrostatically unfavorable depending on the specific charged amino acids introduced.
- positively-charged amino acid residues e.g., lysine, arginine, or histidine
- negatively-charged amino acid residues e.g., aspartic acid or glutamic acid
- an Fc domain includes one or more of the following amino acid substitutions: T366W, T366Y, T394W, F405W, Y349T, Y349E, Y349V, L351T, L351H, L351N, L352K, P353S, S354D, D356K, D356R, D356S, E357K, E357R, E357Q, S364A, T366E, L368T, L368Y, L368E, K370E, K370D, K370Q, K392E, K392D, T394N, P395N, P396T, V397T, V397Q, L398T, D399K, D399R, D399N, F405T, F405H, F405R, Y407T, Y407H, Y407I, K409E, K409
- the terminal lysine is absent from the Fc domain amino acid sequence.
- an Fc domain includes the amino acid substitution T366W, relative to the sequence of human lgG1. The sequence of a wild-type Fc domain is shown below in SEQ ID NO: 100:
- a polypeptide described herein may include an extracellular ActRII chimera fused to a serum protein-binding peptide. Binding to serum protein-binding peptides can improve the pharmacokinetics of protein pharmaceuticals.
- albumin-binding peptides that can be used in the methods and compositions described herein are generally known in the art.
- the albumin binding peptide includes the sequence DICLPRWGCLW (SEQ ID NO: 101).
- albumin-binding peptides may be joined to the N- or C-terminus (e.g., C- terminus) of an extracellular ActRII chimera described herein (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) to increase the serum half-life of the extracellular ActRII chimera.
- an albumin-binding peptide is joined, either directly or through a linker, to the N- or C-terminus of an extracellular ActRII chimera.
- an extracellular ActRII chimera described herein may be fused to the N- or C-terminus of albumin-binding peptide (e.g., SEQ ID NO: 101) through conventional genetic or chemical means, e.g., chemical conjugation.
- a linker e.g., a spacer
- inclusion of an albumin-binding peptide in an extracellular ActRII chimera described herein may lead to prolonged retention of the therapeutic protein through its binding to serum albumin.
- a polypeptide described herein may include an extracellular ActRII chimera fused to fibronectin domains. Binding to fibronectin domains can improve the pharmacokinetics of protein pharmaceuticals.
- Fibronectin domain is a high molecular weight glycoprotein of the extracellular matrix, or a fragment thereof, that binds to, e.g., membrane-spanning receptor proteins such as integrins and extracellular matrix components such as collagens and fibrins.
- a fibronectin domain is joined to the N- or C-terminus (e.g., C-terminus) of an extracellular ActRII chimera described herein (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) to increase the serum half-life of the extracellular ActRII chimera.
- an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a fibronectin domain can be joined, either directly or through a linker, to the N- or C-terminus of an extracellular ActRII chimera.
- fibronectin domains that can be used in the methods and compositions described here are generally known in the art.
- the fibronectin domain is a fibronectin type III domain having amino acids 610-702 of the sequence of UniProt ID NO: P02751 (SEQ ID NO: 102, shown below):
- the fibronectin domain is an adnectin protein.
- an extracellular ActRII chimera described herein may be fused to the N- or C-terminus of a fibronectin domain (e.g., SEQ ID NO: 102) through conventional genetic or chemical means, e.g., chemical conjugation.
- a linker e.g., a spacer
- a linker can be inserted between the extracellular ActRII chimera and the fibronectin domain.
- fibronectin domain in an extracellular ActRII chimera described herein may lead to prolonged retention of the therapeutic protein through its binding to integrins and extracellular matrix components such as collagens and fibrins.
- a polypeptide described herein may include an extracellular ActRII chimera fused to serum albumin. Binding to serum albumins can improve the pharmacokinetics of protein pharmaceuticals.
- Serum albumin is a globular protein that is the most abundant blood protein in mammals. Serum albumin is produced in the liver and constitutes about half of the blood serum proteins. It is monomeric and soluble in the blood. Some of the most crucial functions of serum albumin include transporting hormones, fatty acids, and other proteins in the body, buffering pH, and maintaining osmotic pressure needed for proper distribution of bodily fluids between blood vessels and body tissues. In preferred embodiments, serum albumin is human serum albumin.
- a human serum albumin is joined to the N- or C-terminus (e.g., C-terminus) of an extracellular ActRII chimera described herein (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) to increase the serum half-life of the extracellular ActRII chimera.
- a human serum albumin can be joined, either directly or through a linker, to the N- or C- terminus of an extracellular ActRII chimera.
- serum albumins that can be used in the methods and compositions described herein are generally known in the art.
- the serum albumin includes the sequence of UniProt ID NO: P02768 (SEQ ID NO: 103, shown below):
- an extracellular ActRI I chimera described herein may be fused to the N- or C-terminus of a human serum albumin (e.g., SEQ ID NO: 103) through conventional genetic or chemical means, e.g., chemical conjugation.
- a linker e.g., a spacer
- inclusion of a human serum albumin in an extracellular ActRII chimera described herein may lead to prolonged retention of the therapeutic protein.
- a polypeptide described herein may include an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having a sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) fused to a moiety by way of a linker.
- the moiety increases stability of the polypeptide.
- exemplary moieties include an Fc domain monomer, a wild-type Fc domain, an Fc domain with amino acid substitutions (e.g., one or more substitutions that reduce dimerization), an albumin-binding peptide, a fibronectin domain, or a human serum albumin.
- a linker between a moiety e.g., an Fc domain monomer (e.g., the sequence of SEQ ID NO: 48), a wild-type Fc domain (e.g., SEQ ID NO:
- an Fc domain with amino acid substitutions e.g., one or more substitutions that reduce dimerization
- an albumin-binding peptide e.g., SEQ ID NO: 101
- a fibronectin domain e.g., SEQ ID NO: 102
- a human serum albumin e.g., SEQ ID NO: 103
- an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- Suitable peptide spacers are known in the art, and include, for example, peptide linkers containing flexible amino acid residues such as glycine, alanine, and serine.
- a spacer can contain motifs, e.g., multiple or repeating motifs, of GA, GS, GG, GGA, GGS, GGG, GGGA (SEQ ID NO: 49), GGGS (SEQ ID NO: 50), GGGG (SEQ ID NO: 51), GGGGA (SEQ ID NO: 52), GGGGS (SEQ ID NO: 53), GGGGG (SEQ ID NO: 54), GGAG (SEQ ID NO: 55), GGSG (SEQ ID NO: 56), AGGG (SEQ ID NO: 57), or SGGG (SEQ ID NO: 58).
- motifs e.g., multiple or repeating motifs, of GA, GS, GG, GGA, GGS, GGG, GGGA (SEQ ID NO: 49), GGGS (SEQ
- a spacer can contain 2 to 12 amino acids including motifs of GA or GS, e.g., GA, GS, GAGA (SEQ ID NO: 59), GSGS (SEQ ID NO: 60), GAGAGA (SEQ ID NO: 61), GSGSGS (SEQ ID NO: 62), GAGAGAGA (SEQ ID NO: 63), GSGSGSGS (SEQ ID NO: 64), GAGAGAGAGA (SEQ ID NO: 65), GSGSGSGSGS (SEQ ID NO: 66), GAGAGAGAGAGA (SEQ ID NO: 67), and GSGSGSGSGSGSGS (SEQ ID NO: 68).
- a spacer can contain 3 to 12 amino acids including motifs of GGA or GGS, e.g., GGA, GGS, GGAGGA (SEQ ID NO: 69), GGSGGS (SEQ ID NO: 70), GGAGGAGGA (SEQ ID NO: 71), GGSGGSGGS (SEQ ID NO: 72), GGAGGAGGAGGA (SEQ ID NO: 73), and GGSGGSGGSGGS (SEQ ID NO: 74).
- GGA, GGS, GGAGGA SEQ ID NO: 69
- GGSGGS SEQ ID NO: 70
- GGAGGAGGA SEQ ID NO: 71
- GGSGGSGGS SEQ ID NO: 72
- GGAGGAGGAGGA SEQ ID NO: 73
- GGSGGSGGSGGS SEQ ID NO: 74
- a spacer can contain 4 to 12 amino acids including motifs of GGAG (SEQ ID NO: 55), GGSG (SEQ ID NO: 56), e.g., GGAG (SEQ ID NO: 55), GGSG (SEQ ID NO: 56), GGAGGGAG (SEQ ID NO: 75), GGSGGGSG (SEQ ID NO: 76), GGAGGGAGGGAG (SEQ ID NO: 77), and GGSGGGSGGGSG (SEQ ID NO: 78).
- a spacer can contain motifs of GGGGA (SEQ ID NO: 52) or GGGGS (SEQ ID NO: 53), e.g., GGGGAGGGGAGGGGA (SEQ ID NO: 79) and GGGGSGGGGSGGGGS (SEQ ID NO: 80).
- an amino acid spacer between a moiety e.g., an Fc domain monomer, a wild-type Fc domain, an Fc domain with amino acid substitutions (e.g., one or more substitutions that reduce dimerization), an albumin-binding peptide, a fibronectin domain, or a human serum albumin
- an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a spacer can also contain amino acids other than glycine, alanine, and serine, e.g., AAAL (SEQ ID NO: 84), AAAK (SEQ ID NO: 85), AAAR (SEQ ID NO: 86), EGKSSGSGSESKST (SEQ ID NO: 87), GSAGSAAGSGEF (SEQ ID NO: 88), AEAAAKEAAAKA (SEQ ID NO: 89), KESGSVSSEQLAQFRSLD (SEQ ID NO: 90), GENLYFQSGG (SEQ ID NO: 91), SACYCELS (SEQ ID NO: 92), RSIAT (SEQ ID NO: 93), RPACKIPNDLKQKVMNH (SEQ ID NO: 94), GGSAGGSGSGSSGGSSGASGTGTAGGTGSGSGTGSG (SEQ ID NO: 95), AAANSSIDLISVPVDSR (SEQ ID NO: 96), or GGSGGGSEGGGSEGGGSEGGGSEG
- a spacer can contain motifs, e.g., multiple or repeating motifs, of EAAAK (SEQ ID NO: 98). In some embodiments, a spacer can contain motifs, e.g., multiple or repeating motifs, of proline- rich sequences such as (XP) n , in which X may be any amino acid (e.g., A, K, or E) and n is from 1-5, and PAPAP (SEQ ID NO: 99).
- XP proline- rich sequences
- the length of the peptide spacer and the amino acids used can be adjusted depending on the two proteins involved and the degree of flexibility desired in the final protein fusion polypeptide.
- the length of the spacer can be adjusted to ensure proper protein folding and avoid aggregate formation.
- the polypeptides of the invention can be produced from a host cell.
- a host cell refers to a vehicle that includes the necessary cellular components, e.g., organelles, needed to express the polypeptides and fusion polypeptides described herein from their corresponding nucleic acids.
- the nucleic acids may be included in nucleic acid vectors that can be introduced into the host cell by conventional techniques known in the art (e.g., transformation, transfection, electroporation, calcium phosphate precipitation, direct microinjection, infection, or the like).
- transformation, transfection, electroporation, calcium phosphate precipitation, direct microinjection, infection, or the like The choice of nucleic acid vectors depends in part on the host cells to be used. Generally, preferred host cells are of either eukaryotic (e.g., mammalian) or prokaryotic (e.g., bacterial) origin.
- a nucleic acid sequence encoding the amino acid sequence of a polypeptide of the invention may be prepared by a variety of methods known in the art. These methods include, but are not limited to, oligonucleotide-mediated (or site-directed) mutagenesis, PCR mutagenesis, ligation, and overlap extension PCR.
- a nucleic acid molecule encoding a polypeptide of the invention may be obtained using standard techniques, e.g., gene synthesis.
- a nucleic acid molecule encoding a wild-type extracellular ActRIIA or ActRIIB may be mutated to include specific amino acid substitutions using standard techniques in the art, e.g., QuikChangeTM mutagenesis.
- Nucleic acid molecules can be synthesized using a nucleotide synthesizer or PCR techniques.
- a nucleic acid sequence encoding a polypeptide of the invention may be inserted into a vector capable of replicating and expressing the nucleic acid molecule in prokaryotic or eukaryotic host cells.
- Many vectors are available in the art and can be used for the purpose of the invention.
- Each vector may include various components that may be adjusted and optimized for compatibility with the particular host cell.
- the vector components may include, but are not limited to, an origin of replication, a selection marker gene, a promoter, a ribosome binding site, a signal sequence, the nucleic acid sequence encoding protein of interest, and a transcription termination sequence.
- mammalian cells may be used as host cells for the invention.
- mammalian cell types include, but are not limited to, human embryonic kidney (HEK) (e.g., HEK293, HEK 293F), Chinese hamster ovary (CHO), HeLa, COS, PC3, Vero, MC3T3, NS0, Sp2/0, VERY, BHK, MDCK, W138, BT483, Hs578T, HTB2, BT20, T47D, NS0 (a murine myeloma cell line that does not endogenously produce any immunoglobulin chains), CRL7030, and HsS78Bst cells.
- HEK human embryonic kidney
- CHO Chinese hamster ovary
- E. coli cells may also be used as host cells for the invention.
- E. coli strains include, but are not limited to, E. coli 294 (ATCC ® 31 ,446), E. coli l 1776 (ATCC ® 31 ,537, E. coli BL21 (DE3) (ATCC ® BAA- 1025), and E. coli RV308 (ATCC ® 31 ,608).
- Different host cells have characteristic and specific mechanisms for the posttranslational processing and modification of protein products (e.g., glycosylation). Appropriate cell lines or host systems may be chosen to ensure the correct modification and processing of the polypeptide expressed.
- the above-described expression vectors may be introduced into appropriate host cells using conventional techniques in the art, e.g., transformation, transfection, electroporation, calcium phosphate precipitation, and direct microinjection.
- host cells are cultured in conventional nutrient media modified as appropriate for inducing promoters, selecting transformants, or amplifying the genes encoding the desired sequences.
- Methods for expression of therapeutic proteins are known in the art, see, for example, Paulina Baibas, Argelia Lorence (eds.) Recombinant Gene Expression: Reviews and Protocols (Methods in Molecular Biology), Humana Press; 2nd ed. 2004 and Vladimir Voynov and Justin A. Caravella (eds.) Therapeutic Proteins: Methods and Protocols (Methods in Molecular Biology) Humana Press; 2nd ed. 2012. Protein production, recovery, and purification
- Host cells used to produce the polypeptides of the invention may be grown in media known in the art and suitable for culturing of the selected host cells.
- suitable media for mammalian host cells include Minimal Essential Medium (MEM), Dulbecco’s Modified Eagle’s Medium (DMEM), Expi293TM Expression Medium, DMEM with supplemented fetal bovine serum (FBS), and RPMI-1640.
- suitable media for bacterial host cells include Luria broth (LB) plus necessary supplements, such as a selection agent, e.g., ampicillin.
- Host cells are cultured at suitable temperatures, such as from about 20 °C to about 39 °C, e.g., from 25 °C to about 37 °C, preferably 37 °C, and CO2 levels, such as 5 to 10%.
- the pH of the medium is generally from about 6.8 to 7.4, e.g., 7.0, depending mainly on the host organism. If an inducible promoter is used in the expression vector of the invention, protein expression is induced under conditions suitable for the activation of the promoter.
- the expressed protein may be secreted from the host cells (e.g., mammalian host cells) into the cell culture media. Protein recovery may involve filtering the cell culture media to remove cell debris.
- the proteins may be further purified.
- a polypeptide of the invention may be purified by any method known in the art of protein purification, for example, by chromatography (e.g., ion exchange, affinity, and size-exclusion column chromatography), centrifugation, differential solubility, or by any other standard technique for the purification of proteins.
- the protein can be isolated and purified by appropriately selecting and combining affinity columns such as Protein A column (e.g., POROS Protein A chromatography) with chromatography columns (e.g., POROS HS-50 cation exchange chromatography), filtration, ultra filtration, salting-out and dialysis procedures.
- affinity columns such as Protein A column (e.g., POROS Protein A chromatography) with chromatography columns (e.g., POROS HS-50 cation exchange chromatography), filtration, ultra filtration, salting-out and dialysis procedures.
- host cells may be disrupted, e.g., by osmotic shock, sonication, or lysis, to recover the expressed protein.
- cell debris may be removed by centrifugation or filtration.
- a polypeptide can be conjugated to marker sequences, such as a peptide to facilitate purification.
- marker amino acid sequence is a hexa- histidine peptide (His-tag), which binds to nickel-functionalized agarose affinity column with micromolar affinity.
- peptide tags useful for purification include, but are not limited to, the hemagglutinin “HA” tag, which corresponds to an epitope derived from influenza hemagglutinin protein (Wilson et al., Cell 37:767, 1984).
- the polypeptides of the invention can be produced by the cells of a subject (e.g., a human), e.g., in the context of gene therapy, by administrating a vector (such as a viral vector (e.g., a retroviral vector, adenoviral vector, poxviral vector (e.g., vaccinia viral vector, such as Modified Vaccinia Ankara (MVA)), adeno-associated viral vector, and alphaviral vector)) containing a nucleic acid molecule encoding the polypeptide of the invention.
- a vector such as a viral vector (e.g., a retroviral vector, adenoviral vector, poxviral vector (e.g., vaccinia viral vector, such as Modified Vaccinia Ankara (MVA)), adeno-associated viral vector, and alphaviral vector)
- a vector such as a viral vector (e.g., a retroviral vector, aden
- the vector once inside a cell of the subject (e.g., by transformation, transfection, electroporation, calcium phosphate precipitation, direct microinjection, infection, etc.) will promote expression of the polypeptide, which is then secreted from the cell. If treatment of a disease or disorder is the desired outcome, no further action may be required. If collection of the protein is desired, blood may be collected from the subject and the protein purified from the blood by methods known in the art. VIII.
- compositions that include the polypeptides described herein (e.g., a polypeptide including an extracellular ActRI I chimera (e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- a polypeptide including an extracellular ActRI I chimera e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43).
- a pharmaceutical composition of the invention includes a polypeptide including an extracellular ActRI I chimera (e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) fused to a moiety (e.g., Fc domain monomer, or a dimer thereof, a wild-type Fc domain, an Fc domain with amino acid substitutions (e.g., one or more substitutions that reduce dimerization), an albumin-binding peptide, a fibronectin domain, or a human serum albumin) as the therapeutic protein.
- an extracellular ActRI I chimera e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a moiety e.g., Fc domain monomer, or a dimer thereof, a wild-type Fc domain, an Fc
- a pharmaceutical composition of the invention including a polypeptide of the invention may be used in combination with other agents (e.g., therapeutic biologies and/or small molecules) or compositions in a therapy.
- the pharmaceutical composition may include one or more pharmaceutically acceptable carriers or excipients, which can be formulated by methods known to those skilled in the art.
- a pharmaceutical composition of the invention includes a nucleic acid molecule (DNA or RNA, e.g., mRNA) encoding a polypeptide of the invention, or a vector containing such a nucleic acid molecule.
- Acceptable carriers and excipients in the pharmaceutical compositions are nontoxic to recipients at the dosages and concentrations employed.
- Acceptable carriers and excipients may include buffers such as phosphate, citrate, HEPES, and TAE, antioxidants such as ascorbic acid and methionine, preservatives such as hexamethonium chloride, octadecyldimethylbenzyl ammonium chloride, resorcinol, and benzalkonium chloride, proteins such as human serum albumin, gelatin, dextran, and immunoglobulins, hydrophilic polymers such as polyvinylpyrrolidone, amino acids such as glycine, glutamine, histidine, arginine, and lysine, and carbohydrates such as glucose, mannose, sucrose, and sorbitol.
- buffers such as phosphate, citrate, HEPES, and TAE
- antioxidants such as ascorbic acid and methionine
- preservatives such as
- compositions of the invention can be administered parenterally in the form of an injectable formulation.
- Pharmaceutical compositions for injection can be formulated using a sterile solution or any pharmaceutically acceptable liquid as a vehicle.
- Pharmaceutically acceptable vehicles include, but are not limited to, sterile water, physiological saline, and cell culture media (e.g., Dulbecco’s Modified Eagle Medium (DMEM), a-Modified Eagles Medium (a-MEM), F-12 medium).
- DMEM Modified Eagle Medium
- a-MEM a-Modified Eagles Medium
- F-12 medium F-12 medium.
- Formulation methods are known in the art, see e.g., Banga (ed.) Therapeutic Peptides and Proteins: Formulation, Processing and Delivery Systems (3rd ed.) Taylor & Francis Group, CRC Press (2015).
- the pharmaceutical compositions of the invention may be prepared in microcapsules, such as hydroxylmethylcellulose or gelatin-microcapsule and poly-(methylmethacrylate) microcapsule.
- the pharmaceutical compositions of the invention may also be prepared in other drug delivery systems such as liposomes, albumin microspheres, microemulsions, nanoparticles, and nanocapsules. Such techniques are described in Remington: The Science and Practice of Pharmacy 22 nd edition (2012).
- the pharmaceutical compositions to be used for in vivo administration must be sterile. This is readily accomplished by filtration through sterile filtration membranes.
- the pharmaceutical compositions of the invention may also be prepared as a sustained-release formulation.
- sustained-release preparations include semipermeable matrices of solid hydrophobic polymers containing the polypeptides of the invention.
- sustained release matrices include polyesters, hydrogels, polylactides, copolymers of L-glutamic acid and y ethyl-L- glutamate, non-degradable ethylene-vinyl acetate, degradable lactic acid-glycolic acid copolymers such as LUPRON DEPOTTM, and poly-D-(-)-3-hydroxybutyric acid.
- Some sustained-release formulations enable release of molecules over a few months, e.g., one to six months, while other formulations release pharmaceutical compositions of the invention for shorter time periods, e.g., days to weeks.
- the pharmaceutical composition may be formed in a unit dose form as needed.
- the amount of active component, e.g., a polypeptide of the invention, included in the pharmaceutical preparations is such that a suitable dose within the designated range is provided (e.g., a dose within the range of 0.01- 100 mg/kg of body weight).
- the pharmaceutical composition for gene therapy can be in an acceptable diluent, or can include a slow release matrix in which the gene delivery vehicle is imbedded. If hydrodynamic injection is used as the delivery method, the pharmaceutical composition containing a nucleic acid molecule encoding a polypeptide described herein or a vector (e.g., a viral vector) containing the nucleic acid molecule is delivered rapidly in a large fluid volume intravenously.
- a vector e.g., a viral vector
- Vectors that may be used as in vivo gene delivery vehicle include, but are not limited to, retroviral vectors, adenoviral vectors, poxviral vectors (e.g., vaccinia viral vectors, such as Modified Vaccinia Ankara), adeno-associated viral vectors, and alphaviral vectors.
- retroviral vectors e.g., retroviral vectors, adenoviral vectors, poxviral vectors (e.g., vaccinia viral vectors, such as Modified Vaccinia Ankara), adeno-associated viral vectors, and alphaviral vectors.
- compositions that include the polypeptides of the invention as the therapeutic proteins may be formulated for, e.g., intravenous administration, parenteral administration, subcutaneous administration, intramuscular administration, intra-arterial administration, intrathecal administration, or intraperitoneal administration.
- the pharmaceutical composition may also be formulated for, or administered via, oral, nasal, spray, aerosol, rectal, or vaginal administration.
- various effective pharmaceutical carriers are known in the art. See, e.g., ASHP Handbook on Injectable Drugs, Toissel, 18th ed. (2014).
- a pharmaceutical composition that includes a nucleic acid molecule encoding a polypeptide of the invention or a vector containing such nucleic acid molecule may be administered by way of gene delivery.
- Methods of gene delivery are well-known to one of skill in the art.
- Vectors that may be used for in vivo gene delivery and expression include, but are not limited to, retroviral vectors, adenoviral vectors, poxviral vectors (e.g., vaccinia viral vectors, such as Modified Vaccinia Ankara (MVA)), adeno-associated viral vectors, and alphaviral vectors.
- mRNA molecules encoding polypeptides of the invention may be administered directly to a subject.
- nucleic acid molecules encoding a polypeptide described herein or vectors containing such nucleic acid molecules may be administered using a hydrodynamic injection platform.
- a nucleic acid molecule encoding a polypeptide described herein is put under the control of a strong promoter in an engineered plasmid (e.g., a viral plasmid).
- the plasmid is often delivered rapidly in a large fluid volume intravenously.
- Hydrodynamic injection uses controlled hydrodynamic pressure in veins to enhance cell permeability such that the elevated pressure from the rapid injection of the large fluid volume results in fluid and plasmid extravasation from the vein.
- the expression of the nucleic acid molecule is driven primarily by the liver.
- mRNA molecules encoding a polypeptide described herein may be administered using hydrodynamic injection.
- a pharmaceutical composition of the invention may include a dosage of a polypeptide of the invention ranging from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1.25, 1.5, 1.75, 2, 2.25, 2.5, 2.75, 3, 3.25, 3.5, 3.75, 4, 4.25, 4.5, 4.75, 5, 10, 15, 20, 25, 30, 35, 40, 45,
- the dosage may be adapted by the physician in accordance with conventional factors such as the extent of the disease and different parameters of the subject.
- the pharmaceutical compositions are administered in a manner compatible with the dosage formulation and in such amount as is therapeutically effective to result in an improvement or remediation of the symptoms.
- the pharmaceutical compositions are administered in a variety of dosage forms, e.g., intravenous dosage forms, subcutaneous dosage forms, and oral dosage forms (e.g., ingestible solutions, drug release capsules).
- dosage forms e.g., intravenous dosage forms, subcutaneous dosage forms, and oral dosage forms (e.g., ingestible solutions, drug release capsules).
- therapeutic proteins are dosed at 0.1-100 mg/kg, e.g., 0.5-50 mg/kg.
- compositions that include a polypeptide of the invention may be administered to a subject in need thereof, for example, one or more times (e.g., 1-10 times or more) daily, weekly, biweekly, every four weeks, monthly, bimonthly, quarterly, biannually, annually, or as medically necessary.
- pharmaceutical compositions that include a polypeptide of the invention may be administered to a subject in need thereof weekly, biweekly, every four weeks, monthly, bimonthly, or quarterly. Dosages may be provided in either a single or multiple dosage regimens. The timing between administrations may decrease as the medical condition improves or increase as the health of the patient declines.
- the invention is based on the discovery that combining extracellular portions of ActRIIA and ActRIIB yields ActRII chimeras with improved properties (e.g., improved ligand binding properties) compared to wild-type extracellular ActRIIA and ActRIIB.
- the ActRII chimeras generated by combining extracellular portions of ActRIIA and ActRIIB may possess beneficial properties of both ActRIIB (e.g., an ability to increase muscle mass and strong binding affinity to activins A and B) and ActRIIA (e.g., reduced binding affinity to BMP9 and/or longer serum half-life as an Fc fusion protein (e.g., compared to ActRIIB- Fc), and/or an ability to increase red blood cell levels).
- ActRII chimeras contain extracellular portions of ActRIIA and ActRIIB, they will be soluble and able to compete with endogenous activin receptors by binding to and sequestering ligands (e.g., activins A and B, myostatin, GDF11) without activating intracellular signaling pathways. Therefore, the extracellular ActRII chimeras described herein can be used to treat diseases or conditions in which elevated activin signaling has been implicated in pathogenesis (e.g., diseases or conditions in which increased expression of activin receptors or activin receptor ligands has been observed).
- diseases or conditions in which elevated activin signaling has been implicated in pathogenesis (e.g., diseases or conditions in which increased expression of activin receptors or activin receptor ligands has been observed).
- myostatin has been implicated in promoting fibrosis, inhibiting skeletal muscle growth, and regulating bone homeostasis, and elevated myostatin has been observed in subcutaneous and visceral fat of obese mice and plasma of obese and insulin resistant women.
- activin A has been reported to be upregulated in bone disease, clinical and experimental pulmonary hypertension, adipose tissue, and subcutaneous and visceral fat of obese mice, and has been found to inhibit osteoblast activity and promote fibrosis.
- Another activin receptor ligand, GDF11 has been found to be overexpressed in a mouse model of hemolytic anemia and associated with defects in red blood cell production, and both type I and type II activin receptors have been linked to pancreatic function and diabetes.
- a therapeutic agent that binds to activin receptor ligands may have therapeutic utility for treating or preventing a variety of diseases or conditions, such as muscle disease, bone disease, fibrosis, anemia, thrombocytopenia, neutropenia, metabolic disease (e.g., obesity, Type 1 diabetes, or Type 2 diabetes), or PH (e.g., PAH, venous PH, hypoxic PH, thromboembolic PH, or miscellaneous PH).
- compositions and methods described herein can be used to treat and/or prevent (e.g., prevent the development of or treat a subject diagnosed with) medical conditions, e.g., muscle disease (e.g., skeletal muscle weakness or atrophy), bone disease, low red blood cell levels (e.g., low hemoglobin levels or low red blood cell count, e.g., anemia), fibrosis, thrombocytopenia (e.g., low platelet count), neutropenia (e.g., low neutrophil count), metabolic disease (e.g., obesity, Type 1 diabetes, or Type 2 diabetes), or PH (e.g., PAH, venous PH, hypoxic PH, thromboembolic PH, or miscellaneous PH).
- medical conditions e.g., muscle disease (e.g., skeletal muscle weakness or atrophy), bone disease, low red blood cell levels (e.g., low hemoglobin levels or low red blood cell count, e.g., anemia), fibro
- the polypeptides described herein may be administered to increase muscle mass and strength in a subject in need thereof.
- the polypeptides described herein may be administered to increase lean mass.
- the polypeptides described herein may increase muscle mass and/or lean mass compared to measurements obtained prior to treatment.
- the subject may have or be at risk of developing a disease or condition that results in muscle weakness or atrophy (e.g., a neuromuscular disease, cachexia, sarcopenia, or treatment-related muscle loss or atrophy).
- a disease or condition that results in muscle weakness or atrophy
- the methods described herein are directed to affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of activin A, activin B, myostatin, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing a disease or condition involving weakness and atrophy of muscles.
- the polypeptides described herein may be administered to increase bone mineral density, increase bone formation, increase bone strength, reduce the risk or occurrence of bone fracture, or reduce bone resorption in a subject in need thereof.
- the polypeptides described herein may increase bone mineral density, increase bone formation, or reduce bone resorption compared to measurements obtained prior to treatment.
- the subject may have or be at risk of developing a disease that results in bone damage (e.g., osteoporosis or osteopenia).
- the methods described herein are directed to affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of activin A, activin B, myostatin, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing a disease or condition involving bone damage.
- the polypeptides described herein may be administered to increase red blood cell levels (e.g., increase hemoglobin levels, increase red blood cell count, increase red blood cell volume, increase red cell mass, increase hematocrit, or increase red blood cell formation or production), increase the maturation and/or differentiation of erythroid progenitors (early or late- (e.g., terminal) stage progenitors, e.g., early-stage erythroid progenitors, such burst-forming unit- erythroid cells (BFU-Es) and/or colony forming unit-erythroid cells (CFU-Es), e.g., increase the
- the polypeptides described herein may increase red blood cell levels, increase the maturation and/or differentiation of erythroid progenitors, increase late- stage erythroid precursor maturation, recruit early-stage progenitors into the erythroid lineage, increase the number of early-stage erythroid precursors, promote the progression of erythroid precursors through erythropoiesis, or reduce the accumulation of red blood cell progenitor cells compared to measurements obtained prior to treatment.
- the subject may have a disease or condition associated with low red blood cell levels (e.g., anemia or blood loss).
- the subject may have or be at risk of developing anemia or blood loss (e.g., the subject may have or be at risk of developing anemia due to other diseases or conditions, such as a myelodysplastic syndrome, myelofibrosis, chronic kidney disease, rheumatoid arthritis, ineffective hematopoiesis, cancer, or an inflammatory disease (e.g., Crohn’s disease, SLE, or ulcerative colitis), or due to medical treatments, such as chemotherapy, radiation therapy, or surgery).
- diseases or conditions such as a myelodysplastic syndrome, myelofibrosis, chronic kidney disease, rheumatoid arthritis, ineffective hematopoiesis, cancer, or an inflammatory disease (e.g., Crohn’s disease, SLE, or ulcerative colitis), or due to medical treatments, such as chemotherapy, radiation therapy, or surgery).
- the methods described herein are directed to affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of activin A, activin B, myostatin, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing a disease or condition involving low red blood cell levels.
- the polypeptides described herein may be administered to increase platelet levels (e.g., increase platelet count), promote megakaryocyte differentiation and/or maturation (e.g., to produce platelets), reduce platelet progenitor accumulation, improve blood clotting, reduce bleeding events, reduce bleeding in the skin (e.g., petechiae or bruising), and/or promote or increase platelet formation or production in a subject in need thereof.
- platelet levels e.g., increase platelet count
- promote megakaryocyte differentiation and/or maturation e.g., to produce platelets
- reduce platelet progenitor accumulation improve blood clotting
- reduce bleeding events reduce bleeding in the skin (e.g., petechiae or bruising)
- promote or increase platelet formation or production in a subject in need thereof may be administered to increase platelet levels (e.g., increase platelet count), promote megakaryocyte differentiation and/or maturation (e.g., to produce platelets), reduce platelet progenitor accumulation,
- the polypeptides described herein may increase platelet levels, promote megakaryocyte differentiation and/or maturation, reduce platelet progenitor accumulation (e.g., by stimulating progenitor cells to progress to maturation), improve blood clotting, reduce bleeding events, reducing bleeding in the skin, and/or promote or increase platelet formation or production compared to measurements obtained prior to treatment.
- the subject may have a disease or condition associated with low platelet levels (e.g., thrombocytopenia).
- a megakaryocyte can be contacted in vitro with a polypeptide described herein, a nucleic acid encoding the polypeptide, or a vector containing the nucleic acid to generate platelets for the treatment of thrombocytopenia.
- the subject may have or be at risk of developing thrombocytopenia (e.g., the subject may have or be at risk of developing thrombocytopenia due to other diseases or conditions, such as a myelodysplastic syndrome, myelofibrosis, myelofibrosis treatment (e.g., treatment with a JAK inhibitor, such as with ruxolitinib or fedratinib), ineffective hematopoiesis, Gaucher disease, aplastic anemia, Fanconi anemia, Diamond Blackfan anemia, Shwachman Diamond syndrome, heavy alcohol consumption, cirrhosis of the liver, cancer (e.g., leukemia or lymphoma), immune thrombocytopenia, an autoimmune disease (e.g., rheumatoid arthritis or lupus (e.g., SLE)), a viral infection (e.g., hepatitis C , HIV, chickenpox, mumps, rubella, parvovirus,
- the methods described herein are directed to affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of activin A, activin B, myostatin, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing a disease or condition involving low platelet levels.
- the polypeptides described herein may be administered to increase neutrophil levels (e.g., increase neutrophil count), increase or promote the differentiation and/or maturation of progenitor cells (e.g., myeloid progenitors, myeloblasts, or myelocytes) into neutrophils, and/or promote or increase neutrophil formation or production in a subject in need thereof.
- a polypeptide including an extracellular ActRI I chimera e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43), e.g., an effective amount of an ActRII chimera
- increase neutrophil levels e.g., increase neutrophil count
- progenitor cells e.g., myeloid progenitors, myeloblasts, or myelocytes
- the polypeptides described herein may increase neutrophil levels, increase or promote the differentiation and/or maturation of progenitor cells into neutrophils, and/or promote or increase neutrophil formation or production compared to measurements obtained prior to treatment.
- the subject may have a disease or condition associated with low neutrophil levels (e.g., neutropenia).
- the subject may have or be at risk of developing neutropenia (e.g., the subject may have or be at risk of developing neutropenia due to other diseases or conditions, such as a myelodysplastic syndrome, myelofibrosis, ineffective hematopoiesis, aplastic anemia, Fanconi anemia, Diamond Blackfan anemia, Shwachman Diamond syndrome, paroxysmal nocturnal hemoglobinuria, Pearson syndrome, dyskeratosis congenita, cancer (e.g., leukemia), a vitamin deficiency (e.g., B-12 deficiency or folate deficiency), an enlarged spleen, an autoimmune disease (e.g., granulomatosis with polyangiitis, lupus (e.g., SLE), Evans syndrome, Felty syndrome, Crohn’s disease, or rheumatoid arthritis), a viral infection (e.g., chickenpox, Epstein-Bar
- the methods described herein are directed to affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of activin A, activin B, myostatin, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing a disease or condition involving low neutrophil levels.
- the polypeptides described herein may be administered to prevent or reduce fibrosis in a subject in need thereof.
- the polypeptides described herein may be administered to slow or stop the progression of fibrosis, to reduce the risk of developing fibrosis, or to reduce (e.g., reduce the frequency or severity of) one or more symptom of fibrosis.
- the polypeptides described herein may reduce fibrosis or slow the progression of fibrosis by at least compared to the progression of fibrosis prior to treatment or compared to the progression of fibrosis in untreated subjects.
- the subject may have or be at risk of developing fibrosis (e.g., the subject may have a disease or condition associated with fibrosis, such as a wound, hepatitis B or C, fatty liver disease, kidney disease (e.g., chronic kidney disease), heart disease, or atherosclerosis, or may be undergoing treatment associated with the development of fibrosis, such as chemotherapy, radiation, or surgery).
- the polypeptides described herein prevent or delay the development of fibrosis in a subject at risk of developing fibrosis (e.g., a subject being treated with chemotherapy, radiation, or surgery, or a subject having a disease or condition associated with fibrosis, such as a wound, hepatitis B or C, fatty liver disease, kidney disease (e.g., chronic kidney disease), heart disease, or atherosclerosis).
- a subject at risk of developing fibrosis e.g., a subject being treated with chemotherapy, radiation, or surgery, or a subject having a disease or condition associated with fibrosis, such as a wound, hepatitis B or C, fatty liver disease, kidney disease (e.g., chronic kidney disease), heart disease, or atherosclerosis).
- the methods described herein are directed to affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of activin A, activin B, myostatin, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing fibrosis or a disease or condition associated with fibrosis.
- myostatin, activin A, activin B, and/or BMP9 signaling e.g., reducing or inhibiting the binding of activin A, activin B, myostatin, and/or BMP9 to their endogenous receptors
- the polypeptides described herein may be administered to treat PH, reduce PH (e.g., reduce the severity or frequency of one or more symptoms of PH, such as shortness of breath (dyspnea), fatigue, swelling (e.g., edema) of the legs, feet, belly (ascites), or neck, chest pain or pressure, racing pulse or heart palpitations, bluish color to lips or skin (cyanosis), dizziness, or fainting), prevent (e.g., prevent the development of) PH, reduce the risk of developing PH, or slow or stop the progression of PH in a subject in need thereof.
- reduce PH e.g., reduce the severity or frequency of one or more symptoms of PH, such as shortness of breath (dyspnea), fatigue, swelling (e.g., edema) of the legs, feet, belly (ascites), or neck, chest pain or pressure, racing pulse or heart palpitations, bluish color to lips or skin (cyanos
- the polypeptides described herein may reduce the symptoms of PH or slow the progression of PH compared to the symptoms or progression observed prior to treatment or compared to symptoms or progression of PH in untreated subjects.
- the subject may have or be at risk of developing PH (e.g., the subject may have idiopathic PAH; the subject may have a disease or condition associated with PAH (e.g., a disease or condition that leads to increased risk of developing PAH), such as HIV infection, schistosomiasis, portal hypertension, pulmonary veno-occlusive disease, pulmonary capillary hemangiomatosis, cirrhosis of the liver, a congenital heart abnormality, a connective tissue/autoimmune disorder (e.g., scleroderma or lupus), or drug use or abuse (e.g., methamphetamine or cocaine use); the subject may have a family history of PH (e.g., heritable PAH); the subject may have a disease or
- the polypeptides described herein prevent or delay the development of PH in a subject at risk of developing PH (e.g., a subject with a family history of PH (e.g., heritable PAH), or a subject having a disease or condition that leads to increased risk of developing PAH, venous PH, hypoxic PH, thromboembolic PH, or miscellaneous PH.
- a subject at risk of developing PH e.g., a subject with a family history of PH (e.g., heritable PAH)
- a subject having a disease or condition that leads to increased risk of developing PAH, venous PH, hypoxic PH, thromboembolic PH, or miscellaneous PH e.g., a subject with a family history of PH (e.g., heritable PAH)
- the methods described herein are directed to affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of activin A, activin B, myostatin, and/or BMP9 to their receptors) in a subject having or at risk of developing PH or a disease or condition associated with PH.
- the PH is PAH, venous PH, hypoxic PH, thromboembolic PH, or miscellaneous PH.
- the polypeptides described herein may be administered to reduce body fat (e.g., amount of body fat or body fat percentage), reduce body weight or body weight gain, reduce fasting insulin levels, increase glucose clearance, reduce LDL, reduce triglycerides, improve serum lipid profile, or increase insulin sensitivity (e.g., reduce in insulin resistance) in a subject in need thereof.
- body fat e.g., amount of body fat or body fat percentage
- reduce body weight or body weight gain e.g., amount of body fat or body fat percentage
- reduce fasting insulin levels e.g., increase glucose clearance, reduce LDL, reduce triglycerides, improve serum lipid profile, or increase insulin sensitivity (e.g., reduce in insulin resistance) in a subject in need thereof.
- the polypeptides described herein may reduce body fat (e.g., amount of body fat or body fat percentage), reduce body weight or body weight gain, reduce fasting insulin levels, increase glucose clearance, reduce LDL, reduce triglycerides, improve serum lipid profile, or increase insulin sensitivity (e.g., reduce in insulin resistance) compared to measurements obtained prior to treatment.
- the subject may have a disease or condition associated with obesity or diabetes (e.g., Type 1 or Type 2 diabetes).
- the subject may have or be at risk of developing a metabolic disease (e.g., obesity, Type 1 diabetes, or Type 2 diabetes, e.g., the subject may be overweight, have a family history of obesity, have other medical conditions or risk factors linked to increased risk of developing obesity or diabetes (e.g., advanced age, or treatment with a glucocorticoid, selective serotonin reuptake inhibitor (SSRI), tricyclic antidepressant, mood stabilizer, antipsychotic, serotonin-norepinephrine reuptake inhibitor (SNRI)), have a family history of diabetes, or have prediabetes).
- a metabolic disease e.g., obesity, Type 1 diabetes, or Type 2 diabetes, e.g., the subject may be overweight, have a family history of obesity, have other medical conditions or risk factors linked to increased risk of developing obesity or diabetes (e.g., advanced age, or treatment with a glucocorticoid, selective serotonin reuptake inhibitor (SSRI),
- the methods described herein are directed to affecting myostatin, activin A, activin B, and/or BMP9 signaling (e.g., reducing or inhibiting the binding of activin A, activin B, myostatin, and/or BMP9 to their endogenous receptors) in a subject having or at risk of developing a metabolic disease (e.g., obesity, Type 1 diabetes, or Type 2 diabetes).
- a metabolic disease e.g., obesity, Type 1 diabetes, or Type 2 diabetes.
- a polypeptide including an extracellular ActRI I chimera described herein reduces or inhibits the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors, e.g., ActRIIA, ActRIIB, and/or BMPRII.
- the polypeptides described herein may reduce the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors compared to the binding of myostatin, activin A, activin B, and/or BMP9 to their endogenous receptors in the absence of the polypeptides of the invention.
- affecting myostatin, activin A, activin B, and/or BMP9 signaling results in an increase in the subject’s muscle mass, an increase in the subject’s lean mass, an increase in the subject’s bone mineral density or bone formation, a decrease in the subject’s bone resorption, an increase in the subject’s red blood cell levels (e.g., hemoglobin levels, hematocrit, red blood cell count, red blood cell volume, or red cell mass, e.g., promotes or increases red blood cell formation or production), an increase the maturation and/or differentiation of erythroid progenitors, an increase in late-stage erythroid precursor maturation, recruitment of early-stage progenitors into the erythroid lineage,
- endogenous receptors e.g., ActRIIA, ActRIIB, and/or BMPRII
- the polypeptides described herein may be administered to a subject to increase muscle mass or strength, to increase lean mass, to increase bone mineral density, to increase bone formation, to increase bone strength, to reduce the risk or occurrence of bone fracture, to decrease bone resorption, to increase red blood cell levels, to increase the maturation and/or differentiation of erythroid progenitors, to increase late-stage erythroid precursor maturation, to recruit early-stage progenitors into the erythroid lineage, to reduce the accumulation of red blood cell progenitor cells, to increase the number of early-stage erythroid precursors and/or progenitors, to promote progression of erythroid precursors
- the extracellular ActRII chimeras may increase muscle mass or strength, increase lean mass, increase bone mineral density, increase bone formation, increase bone strength, reduce the risk or occurrence of bone fracture, decrease bone resorption, increase red blood cell levels, increase the maturation and/or differentiation of erythroid progenitors, increase late-stage erythroid precursor maturation (e.g., terminal maturation, such as the maturation of reticulocytes into red blood cells, or the maturation of erythroblasts into reticulocytes and/or red blood cells), recruit early-stage progenitors into the erythroid lineage, reduce the accumulation of red blood cell progenitor cells, increase the number of early-stage erythroid precursors and/or progenitors, promote progression of ery
- the invention also includes methods of treating a subject having or at risk of developing a disease or condition involving weakness or atrophy of muscles by administering to the subject an effective amount of a polypeptide described herein (e.g., a polypeptide including an extracellular ActRI I chimera (e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- a polypeptide described herein e.g., a polypeptide including an extracellular ActRI I chimera (e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43).
- a subject having or at risk of developing a disease or condition involving weakness or atrophy of muscles has or is at risk of developing a disease or condition including a neuromuscular disease (e.g., a muscular dystrophy, IBM, SMA, CMT, ALS, myasthenia gravis, or multiple sclerosis), sarcopenia, cachexia (e.g., cancer cachexia, HIV-related cachexia, cardiac cachexia (e.g., cachexia associated with heart failure), cachexia associated with chronic kidney disease, or pulmonary cachexia (e.g., cachexia associated with COPD)), disuse atrophy; treatment related muscle loss or atrophy (e.g., glucocorticoid treatment, FGF-21 treatment, GLP-1 treatment, bariatric surgery , cancer therapy, or treatment for obesity or Type 2 diabetes), hypotonia, hypoxia, or muscle loss or atrophy associated with a burn injury.
- a neuromuscular disease e.g., a muscular dystrophy, IBM, SMA, CMT,
- Muscular dystrophies include Duchenne muscular dystrophy (DMD), facioscapulohumeral muscular dystrophy (FSHD), Becker muscular dystrophy (BMD), myotonic dystrophy (DM), congenital muscular dystrophy, limb-girdle muscular dystrophy (LGMD), distal muscular dystrophy (DD), oculopharyngeal muscular dystrophy (OPMD), and Emery-Dreifuss muscular dystrophy (EDMD).
- DMD Duchenne muscular dystrophy
- FSHD facioscapulohumeral muscular dystrophy
- BMD Becker muscular dystrophy
- DM myotonic dystrophy
- congenital muscular dystrophy limb-girdle muscular dystrophy
- LGMD distal muscular dystrophy
- OPMD oculopharyngeal muscular dystrophy
- EDMD Emery-Dreifuss muscular dystrophy
- congenital muscular dystrophies which include congenital muscular dystrophy type 1A (MDC1A, associated with mutations in laminin alpha 2), congenital muscular dystrophy type 1C (MDC1C, associated with mutations in FKRP), congenital muscular dystrophy type 1 D (MDC1 D, associated with mutations in LARGE), congenital muscular dystrophy type 1 B (MDC1 B), Fukuyama congenital muscular dystrophy (FCMD, associated with mutations in fukutin), muscle-eye-brain disease (MEB, which may be associated with mutations in POMGnTI), Walker-Warburg Syndrome (WWS, associated with mutations in B3GNT1 (MDDGA type), POMT1 (MDDGA 1 type), POMT2 (MDDGA2 type), ISPD (MDDGA7 type), GTDC2 (MDDGA8 type), TMEM5 (MDDGA10 type), B3GALNT2 (MDDGA11 type), or SGK196 (MDDGA
- MDC1A
- the methods described herein increase muscle mass, e.g., increase muscle mass, lean mass, and/or muscle strength, e.g., increase muscle mass, lean mass, and/or muscle strength compared to measurements obtained prior to treatment or compared to measurements typically observed in untreated subjects having the same disease or condition.
- the muscle is skeletal muscle.
- the subject is identified as having a disease or condition that results in muscle weakness or atrophy prior to treatment with an ActRII chimera described herein.
- the method includes a step of identifying the subject as having a disease or condition that results in muscle weakness or atrophy (e.g., by evaluating lean mass, muscle mass, or strength or by genetic testing for congenital muscular dystrophy) prior to treatment with an ActRII chimera described herein.
- the method can further include evaluating lean mass, muscle mass, or strength after administration of an ActRII chimera described herein (e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days, 1 , 2, 3, 4, 5, 6, 7, or 8 weeks, or 1 , 2, 3, 4, 5, or 6 months or more after treatment initiation).
- the invention also includes methods of treating a subject having or at risk of developing bone disease by administering to the subject an effective amount of a polypeptide described herein (e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- a polypeptide described herein e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43).
- a subject having or at risk of developing bone disease has or is at risk of developing a disease or condition including primary osteoporosis, secondary osteoporosis, osteopenia, osteopetrosis, osteogenesis imperfecta, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, neuromuscular disease-related bone loss, burn-induced bone loss, anorexia-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity, low gravity-related bone loss, or immobility-related bone loss.
- a disease or condition including primary osteoporosis, secondary osteoporosis, osteopenia, osteopetrosis, osteogenesis imperfecta, bone fracture, bone cancer or cancer metastasis-related bone loss, Paget’s disease, renal osteodystrophy, treatment-related bone loss, neuromuscular disease-related bone loss, burn-induced bone loss, anorexia-related bone loss, diet-related bone loss, bone loss associated with the treatment of obesity,
- the primary osteoporosis is age-related or hormone-related osteoporosis (e.g., related to a decline in estrogen).
- the secondary osteoporosis is immobilization- induced or glucocorticoid-induced osteoporosis.
- the bone cancer is multiple myeloma or the cancer metastasis-related bone loss is caused by multiple myeloma.
- the treatment-related bone loss occurs due to treatment with FGF-21 or GLP-1 , due to treatment with an FGF-21 or GLP-1 containing therapeutic, due to treatment of Type 2 diabetes and/or obesity, due to bariatric surgery, due to androgen or estrogen deprivation therapy, or due to cancer therapy (e.g., chemotherapy or radiation).
- the diet-related bone loss is rickets (e.g., vitamin D deficiency).
- the low-gravity related bone loss is lack of load- related bone loss.
- the methods described herein increase bone mineral density (e.g., increase bone mass), reduce bone resorption (e.g., reduce bone catabolic activity), increase bone formation (e.g., increase bone anabolic activity or increase osteogenesis), increase osteoblast activity or osteoblastogenesis, and/or decrease osteoclast activity or osteoclastogenesis, e.g., increase bone mineral density, reduce bone resorption, increase bone formation, increase osteoblast activity or osteoblastogenesis, and/or decrease osteoclast activity or osteoclastogenesis compared to measurements obtained prior to treatment or compared to measurements typically observed in untreated subjects having the same disease or condition.
- the bone is cortical or trabecular bone.
- the subject is identified as having a bone disease prior to treatment with an ActRII chimera described herein.
- the method includes a step of identifying the subject as having a bone disease prior to treatment with an ActRII chimera described herein.
- the method can further include evaluating bone mineral density, bone formation, or bone resorption after administration of an ActRII chimera described herein (e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days,
- the invention also includes methods of treating a subject having or at risk of developing anemia or blood loss by administering to the subject an effective amount of a polypeptide described herein (e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- a subject having or at risk of developing low red blood cell levels e.g., low hemoglobin levels, low hematocrit, or low red blood cell counts
- the anemia is associated with a nutritional deficit (e.g., a vitamin deficiency, such as vitamin B-12 deficiency, folate deficiency), a bone marrow defect (e.g., paroxysmal nocturnal hemoglobinuria), adverse reaction to medication (e.g., anti-retroviral HIV drugs), a myelodysplastic syndrome, bone marrow transplantation, myelofibrosis, ineffective hematopoiesis, cancer (e.g., a solid tumor, such as breast cancer, lung cancer, colon cancer; a tumor of the lymphatic system, such as chronic lymphocytic leukemia, non-Hodgkin’s lymphoma, Hodgkin’s lymphoma; or a tumor of the hematopoietic system, such as leukemia or multiple myeloma), cancer treatment (e.g., radiation or chemotherapy, e.g., chemotherapy with platinum-containing agents), myelofibros
- psoriasis or inflammatory bowel disease (e.g., Crohn's disease or ulcerative colitis), cystitis, gastritis), acute or chronic renal disease or failure (e.g., chronic kidney disease) including idiopathic or congenital conditions, diabetes, acute or chronic liver disease, acute or chronic bleeding, infection (e.g., malaria, osteomyelitis), splenomegaly, porphyria, vasculitis, hemolysis, urinary tract infection, hemoglobinopathy (e.g., sickle cell disease), thalassemia (e.g., a- or b-thalassemia), Churg- Strauss syndrome, Felty syndrome, Pearson syndrome, dyskeratosis congenita, graft versus host disease, hematopoietic stem cell transplantation, osteomyelofibrosis, pancytopenia, pure red-cell aplasia, purpura Schoenlein-Henoch, Shwachman syndrome (e.g., Sh
- the myelodysplastic syndrome may be myelodysplastic syndrome with unilineage dysplasia (MDS-SLD), myelodysplastic syndrome with multilineage dysplasia (MDS-MLD), myelodysplastic syndrome with ring sideroblasts (MDS-RS, which includes single lineage dysplasia (MDS-RS-SLD) and multilineage dysplasia (MDS-RS- MLD)), myelodysplastic syndrome associated with isolated del chromosome abnormality (MDS with isolated del(5q)), myelodysplastic syndrome with excess blasts (MDS-EB; which includes myelodysplastic syndrome with excess blasts — type 1 (MDS-EB-1) and myelodysplastic syndrome with excess blasts — type 2 (MDS-EB-2)), myelodysplastic syndrome, unclassifiable (MDS-U), or myelodysplastic syndrome/myeloproliferative neoplasm with ring sideroblasts and
- the myelodysplastic syndrome may be a very low, low, or intermediate risk MDS as determined by the Revised International Prognostic Scoring System (IPSS-R).
- the myelodysplastic syndrome may be an RS-positive myelodysplastic syndrome (e.g., the subject with a myelodysplastic syndrome may have ring sideroblasts) or a non-RS myelodysplastic syndrome (e.g., the subject with a myelodysplastic syndrome may lack ring sideroblasts).
- the RS-positive myelodysplastic syndrome is associated with a splicing factor mutation, such as a mutation in SF3B1.
- the MDS is associated with a defect in terminal maturation (often observed in RS-positive MDS and in subjects having splicing factor mutations, such a subject may have increased erythroid progenitor cells in the bone marrow relative to a healthy subject).
- the MDS is associated with a defect in early-stage hematopoiesis (e.g., early-stage erythroid cell development, such as commitment or early differentiation, such a subject may have fewer erythroid progenitor cells in the bone marrow compared to a healthy subject or to a subject with a defect in terminal maturation).
- the MDS is associated with elevated endogenous erythropoietin levels.
- the myelodysplastic syndrome is associated with hypocellular bone marrow (e.g., a subject with MDS has hypocellular bone marrow).
- the subject may have a low transfusion burden or a high transfusion burden.
- the subject has a low transfusion burden and received 1-3 RBC units in the eight weeks prior to treatment with an ActRII chimera described herein.
- the subject has a low transfusion burden and did not receive a transfusion (received 0 RBC units) in the eight weeks prior to treatment with an ActRII chimera described herein.
- the anemia is aplastic anemia, iron deficiency anemia, vitamin deficiency anemia, anemia of chronic disease (also called anemia of inflammation), anemia associated with bone marrow disease, hemolytic anemia, sickle cell anemia, microcytic anemia, hypochromic anemia, sideroblastic anemia, congenital dyserythropoietic anemia, Diamond Blackfan anemia, Fanconi anemia, or refractory anemia with excess of blasts.
- the sideroblastic anemia can be acquired sideroblastic anemia or congenital sideroblastic anemia.
- the congenital sideroblastic anemia is associated with a mutation in ALAS2, SLC25A38, FECH, GLRX5, HSPA9, HSCB, SLC25A38, or ABCB7. In some embodiments, the congenital sideroblastic anemia is associated with a mutation in PUS1 , YARS2, LARS2, TRNT1 , MT-ATP6, NDUFB11 , or SLC19A2, or with an mtDNA mutation.
- compositions and methods described herein can also be used to treat subjects that do not respond well to erythropoietin (EPO) or that are susceptible to adverse effects of EPO (e.g., hypertension, headaches, vascular thrombosis, influenza-like syndrome, obstruction of shunts, and myocardial infarction) or to treat subjects that do not respond to an erythroid maturation agent.
- EPO erythropoietin
- the subject has previously been treated with an ESA.
- the subject has not previously been treated with an ESA.
- the blood loss is due to surgery, trauma, a wound, an ulcer, urinary tract bleeding, digestive tract bleeding, frequent blood donation, or heavy menstrual bleeding (e.g., menorrhagia).
- the methods described herein increase red blood cell levels (e.g., hemoglobin levels, hematocrit, red blood cell counts, red blood cell volume, and/or red cell mass), increase or induce red blood cell formation or production, increase the maturation and/or differentiation of erythroid progenitors (e.g., early-stage erythroid progenitors, such as BFU-Es and/or CFU-Es, e.g., increase the maturation and/or differentiation of BFU- Es and/or CFU-Es into proerythroblasts, reticulocytes, or red blood cells, e.g., increase proerythroblast and/or reticulocyte numbers), increase late-stage erythroid precursor maturation, recruit early-stage progenitors into the erythroid lineage, increase the number of early-stage erythroid precursors and/or progenitors, promote the progression of erythroid precursors and/or progenitors through erythropoiesis, and/or reduce
- the compositions and methods described herein reduce the need of a subject for a blood transfusion (e.g., reduce transfusion burden, for example, the subject no longer needs blood transfusions, or the subject needs less frequent blood transfusion than before treatment with the compositions and methods described herein).
- Subjects with normal red blood cell levels can also be treated using the methods and compositions described herein to increase red blood cell levels so that blood can be drawn and stored for later use in transfusions.
- the compositions and methods described herein slow or inhibit the progression of lower- risk MDS to higher-risk MDS and/or acute myeloid leukemia (AML).
- AML acute myeloid leukemia
- treatment of anemia in a subject having a very low, low, or intermediate risk MDS and a low transfusion burden may lead to a hemoglobin increase of greater than or equal to 1.5 g/dL from baseline or pretreatment measurements (e.g., for at least one day, two days, three days, four days, five days, six days, one week, two weeks, three weeks, one month, two months, or longer during treatment).
- treatment of anemia in a subject having a very low, low, or intermediate risk MDS and a high transfusion burden may lead to a reduction of > 50% or > 4 RBC units transfused compared to pretreatment (e.g., comparing an eight-week period during treatment to an eight-week period prior to treatment).
- the subject is identified as having anemia (e.g., anemia associated with a myelodysplastic syndrome or myelofibrosis) prior to treatment with an ActRII chimera described herein.
- the method includes a step of identifying the subject as having anemia (e.g., by evaluating red blood cell, hemoglobin, or hematocrit levels) prior to treatment with an ActRII chimera described herein.
- the method can further include evaluating red blood cell, hemoglobin, or hematocrit levels after administration of an ActRII chimera described herein (e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days, 1 , 2, 3, 4, 5, 6, 7, or 8 weeks, or 1 , 2, 3, 4, 5, or 6 months or more after treatment initiation).
- an ActRII chimera described herein e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days, 1 , 2, 3, 4, 5, 6, 7, or 8 weeks, or 1 , 2, 3, 4, 5, or 6 months or more after treatment initiation.
- the invention also includes methods of treating a subject having or at risk of developing thrombocytopenia by administering to the subject an effective amount of a polypeptide described herein (e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- a subject having or at risk of developing low platelet levels e.g., low platelet counts
- the thrombocytopenia is associated with a bone marrow defect, a myelodysplastic syndrome, bone marrow transplantation, myelofibrosis, myelofibrosis treatment (e.g., treatment with a JAK inhibitor, such as with ruxolitinib or fedratinib), ineffective hematopoiesis, Gaucher disease, aplastic anemia, Fanconi anemia, Diamond Blackfan anemia, Shwachman Diamond syndrome, heavy alcohol consumption, cirrhosis of the liver, cancer (e.g., leukemia or lymphoma), an autoimmune disease (e.g., rheumatoid arthritis, lupus (e.g., SLE), antiphospholipid syndrome (APS), Evans syndrome, or immune thyroid disease), a viral infection (e.g., hepatitis C , HIV, chickenpox, mumps, rubella, parvovirus, or Epstein-Barr virus), a bacterial infection (e.
- the myelodysplastic syndrome may be myelodysplastic syndrome with unilineage dysplasia (MDS-SLD), myelodysplastic syndrome with multilineage dysplasia (MDS-MLD), myelodysplastic syndrome with ring sideroblasts (MDS-RS, which includes single lineage dysplasia (MDS-RS-SLD) and multilineage dysplasia (MDS-RS-MLD)), myelodysplastic syndrome associated with isolated del chromosome abnormality (MDS with isolated del(5q)), myelodysplastic syndrome with excess blasts (MDS-EB; which includes myelodysplastic syndrome with excess blasts — type 1 (MDS-EB-1) and myelodysplastic syndrome with excess blasts — type 2 (MDS-EB-2)), myelodysplastic syndrome, unclassifiable (MDS-U), or myelodysplastic syndrome/myeloproliferative neoplasm with ring sideroblasts and
- the myelodysplastic syndrome may be a very low, low, or intermediate risk MDS as determined by the Revised International Prognostic Scoring System (IPSS-R).
- the myelodysplastic syndrome may be an RS-positive myelodysplastic syndrome (e.g., the subject with a myelodysplastic syndrome may have ring sideroblasts) or a non-RS myelodysplastic syndrome (e.g., the subject with a myelodysplastic syndrome may lack ring sideroblasts).
- the RS-positive myelodysplastic syndrome is associated with a splicing factor mutation, such as a mutation in SF3B1.
- the MDS is associated with a defect in terminal maturation (often observed in RS-positive MDS and in subjects having splicing factor mutations). In some embodiments, the MDS is associated with a defect in early- stage hematopoiesis (e.g., commitment or early differentiation). In some embodiments, the MDS is associated with elevated endogenous erythropoietin levels. In some embodiments, the myelodysplastic syndrome is associated with hypocellular bone marrow (e.g., the subject with MDS has hypocellular bone marrow). The subject may have a low transfusion burden or a high transfusion burden.
- the subject has a low transfusion burden and received 1-3 RBC units in the eight weeks prior to treatment with an ActRII chimera described herein. In some embodiments, the subject has a low transfusion burden and did not receive a transfusion (received 0 RBC units) in the eight weeks prior to treatment with an ActRII chimera described herein. In some embodiments, the subject does not respond well to erythropoietin (EPO) or is susceptible to adverse effects of EPO (e.g., hypertension, headaches, vascular thrombosis, influenza-like syndrome, obstruction of shunts, and myocardial infarction).
- EPO erythropoietin
- the compositions and methods described herein can also be used to treat subjects that do not respond to an erythroid maturation agent.
- the subject has previously been treated with an ESA.
- the subject has not previously been treated with an ESA.
- the thrombocytopenia is familial thrombocytopenia (also referred to as inherited thrombocytopenia, e.g., thrombocytopenia associated with a genetic mutation, such as May-Hegglin anomaly, Sebastian syndrome, Fechtner syndrome, Epstein’s syndrome, Wiskott-Aldrich syndrome, congenital amegakaryocytic thrombocytopenia, platelet storage pool deficiency, Hermansky-Pudlak syndrome, Bernard-Soulier syndrome, Von Willebrand Disease Type 2B, ANKRD26-related thrombocytopenia, thrombocytopenia absent radius syndrome, familial platelet disorder with associated myeloid malignancy (FPD/AML, associated with mutations in
- the thrombocytopenia is immune thrombocytopenia.
- the methods described herein increase platelet levels, increase or induce megakaryocyte differentiation and/or maturation, promote or increase platelet formation or production, reduce the accumulation of platelet progenitor cells, and/or improve blood clotting, reduce bleeding events, and/or reduce bleeding in the skin (petechiae or bruising) compared to measurements obtained prior to treatment or compared to measurements typically observed in untreated subjects having the same disease or condition.
- the subject is identified as having thrombocytopenia prior to treatment with an ActRII chimera described herein.
- the method includes a step of identifying the subject as having thrombocytopenia (e.g., by evaluating platelet levels) prior to treatment with an ActRII chimera described herein.
- the method can further include evaluating platelet levels after administration of an ActRII chimera described herein (e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days, 1 , 2, 3, 4, 5, 6, 7, or 8 weeks, or 1 , 2, 3, 4, 5, or 6 months or more after treatment initiation).
- the invention also includes methods of treating a subject having or at risk of developing neutropenia by administering to the subject an effective amount of a polypeptide described herein (e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- a subject having or at risk of developing low neutrophil levels e.g., low neutrophil cell counts
- the neutropenia is associated with a bone marrow defect, a myelodysplastic syndrome, bone marrow transplantation, myelofibrosis, ineffective hematopoiesis, aplastic anemia, Fanconi anemia, Diamond Blackfan anemia, Shwachman Diamond syndrome, paroxysmal nocturnal hemoglobinuria, Pearson syndrome, dyskeratosis congenita, cancer (e.g., leukemia), a vitamin deficiency (e.g., B-12 deficiency or folate deficiency), an enlarged spleen, an autoimmune disease (e.g., granulomatosis with polyangiitis, lupus (e.g., SLE), Evans syndrome, Felty syndrome, Crohn’s disease, or rheumatoid arthritis), a viral infection (e.g., chickenpox, Epstein-Barr, Hepatitis A, Hepatitis B, Hepatitis C,
- the myelodysplastic syndrome may be myelodysplastic syndrome with unilineage dysplasia (MDS-SLD), myelodysplastic syndrome with multilineage dysplasia (MDS-MLD), myelodysplastic syndrome with ring sideroblasts (MDS-RS, which includes single lineage dysplasia (MDS-RS-SLD) and multilineage dysplasia (MDS-RS-MLD)), myelodysplastic syndrome associated with isolated del chromosome abnormality (MDS with isolated del(5q)), myelodysplastic syndrome with excess blasts (MDS-EB; which includes myelodysplastic syndrome with excess blasts — type 1 (MDS-EB-1) and myelodysplastic syndrome with excess blasts — type 2 (MDS-EB-2)), myelodysplastic syndrome, unclassifiable (MDS-U), or myelodysplastic syndrome/myeloproliferative neoplasm with ring sideroblasts and
- the myelodysplastic syndrome may be a very low, low, or intermediate risk MDS as determined by the Revised International Prognostic Scoring System (IPSS-R).
- the myelodysplastic syndrome may be an RS-positive myelodysplastic syndrome (e.g., the subject with a myelodysplastic syndrome may have ring sideroblasts) or a non-RS myelodysplastic syndrome (e.g., the subject with a myelodysplastic syndrome may lack ring sideroblasts).
- the RS-positive myelodysplastic syndrome is associated with a splicing factor mutation, such as a mutation in SF3B1.
- the MDS is associated with a defect in terminal maturation (often observed in RS-positive MDS and in subjects having splicing factor mutations). In some embodiments, the MDS is associated with a defect in early-stage hematopoiesis (e.g., commitment or early differentiation). In some embodiments, the MDS is associated with elevated endogenous erythropoietin levels. In some embodiments, the myelodysplastic syndrome is associated with hypocellular bone marrow (e.g., a subject with MDS has hypocellular bone marrow). The subject may have a low transfusion burden or a high transfusion burden.
- the subject has a low transfusion burden and received 1-3 RBC units in the eight weeks prior to treatment with an ActRII chimera described herein. In some embodiments, the subject has a low transfusion burden and did not receive a transfusion (received 0 RBC units) in the eight weeks prior to treatment with an ActRII chimera described herein. In some embodiments, the subject does not respond well to erythropoietin (EPO) or is susceptible to adverse effects of EPO (e.g., hypertension, headaches, vascular thrombosis, influenza-like syndrome, obstruction of shunts, and myocardial infarction).
- EPO erythropoietin
- compositions and methods described herein can also be used to treat subjects that do not respond to an erythroid maturation agent.
- the subject has previously been treated with an ESA.
- the subject has not previously been treated with an ESA.
- the neutropenia is chronic idiopathic neutropenia.
- the neutropenia is familial neutropenia (also referred to as inherited neutropenia, e.g., cyclic neutropenia, chronic benign neutropenia, or severe congenital neutropenia (SCN), which may be associated with mutations in the genes ELANE (associated with SCN1), HAX1 (associated with SCN3), G6PC3 (associated with SCN4), GFI1 (associated with SCN2), CSF3R, WAS (associated with X-linked neutropenia/X-linked SCN), CXCR4, VPS45A (associated with SCN5), or JAGN1).
- familial neutropenia also referred to as inherited neutropenia, e.g., cyclic neutropenia, chronic benign neutropenia, or severe congenital neutropenia (SCN)
- ELANE associated with SCN1
- HAX1 associated with SCN3
- G6PC3 associated with SCN4
- GFI1 associated with SCN2
- the methods described herein increase neutrophil levels, increase or induce neutrophil formation or production, and/or increase or induce the differentiation and/or maturation of progenitor cells (e.g., myeloid progenitors, myeloblasts, or myelocytes) into neutrophils compared to measurements obtained prior to treatment or compared to measurements typically observed in untreated subjects having the same disease or condition.
- progenitor cells e.g., myeloid progenitors, myeloblasts, or myelocytes
- the methods described herein reduce the susceptibility of the subject to infection.
- the subject is identified as having neutropenia prior to treatment with an ActRII chimera described herein.
- the method includes a step of identifying the subject as having neutropenia (e.g., by evaluating neutrophil levels) prior to treatment with an ActRII chimera described herein.
- the method can further include evaluating neutrophil levels after administration of an ActRII chimera described herein (e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days, 1 , 2, 3, 4, 5, 6, 7, or 8 weeks, or 1 , 2, 3, 4, 5, or 6 months or more after treatment initiation).
- the invention also includes methods of treating a subject having or at risk of developing fibrosis by administering to the subject an effective amount of a polypeptide described herein (e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- a polypeptide described herein e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43).
- a polypeptide described herein e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs
- the fibrosis is fibrosis is chemotherapeutic drug-induced fibrosis, radiation-induced fibrosis, pulmonary fibrosis (e.g., cystic fibrosis, idiopathic fibrosis, or fibrosis related to tuberculosis, pneumonia, or coal dust), hepatic fibrosis (e.g., cirrhosis, biliary atresia), renal fibrosis (e.g., fibrosis related to chronic kidney disease), corneal fibrosis, heart fibrosis (e.g., endomyocardial fibrosis, or fibrosis related to myocardial infarction), bone marrow fibrosis, myelofibrosis, mediastinal fibrosis, retroperitoneal fibrosis, arthrofibrosis, osteoarticular fibrosis, tissue fibrosis (e.g., fibrosis affecting muscle tissue, skin epidermis
- the fibrosis is associated with a wound, a burn, hepatitis B or C infection, fatty liver disease, Schistosoma infection, kidney disease (e.g., chronic kidney disease), heart disease, macular degeneration, retinal orvitreal retinopathy, Crohn’s disease, systemic or local scleroderma, atherosclerosis, or restenosis.
- kidney disease e.g., chronic kidney disease
- heart disease e.g., macular degeneration, retinal orvitreal retinopathy, Crohn’s disease
- systemic or local scleroderma atherosclerosis, or restenosis.
- the subject is at risk of developing fibrosis related to cancer treatment (chemotherapy or radiation), disease or infection (e.g., tuberculosis, pneumonia, myocardial infarction, hepatitis B or C infection, fatty liver disease, Schistosoma infection, kidney disease (e.g., chronic kidney disease), heart disease, macular degeneration, retinal or vitreal retinopathy, Crohn’s disease, systemic or local scleroderma, atherosclerosis, restenosis, surgery, a wound, or a burn.
- the methods described herein reduce fibrosis compared to measurements obtained prior to treatment or compared to fibrosis in untreated subjects.
- the methods described herein prevent the development of fibrosis or reduce the risk of developing fibrosis (e.g., reduce the risk of developing fibrosis compared to the development of fibrosis in untreated subjects). In some embodiments, the methods described herein slow or stop the progression of fibrosis (e.g., slow the progression of fibrosis compared to progression prior to treatment or compared to progression without treatment or in an untreated subject). In some embodiments, the methods described herein reduce the frequency or severity of one or more symptom of fibrosis. In some embodiments, the methods described herein improve organ or tissue function (e.g., the function of the organ or tissue having fibrosis) compared to organ or tissue function prior to treatment.
- organ or tissue function e.g., the function of the organ or tissue having fibrosis
- Tissue and organ function can be assessed using any standard clinical test commonly used to evaluate tissue and organ function.
- the subject is identified as having fibrosis prior to treatment with an ActRII chimera described herein.
- the method includes a step of identifying the subject as having fibrosis (e.g., using imaging to visualize scar formation) prior to treatment with an ActRII chimera described herein.
- the method can further include evaluating fibrosis after administration of an ActRII chimera described herein (e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days, 1 , 2, 3, 4, 5, 6, 7, or 8 weeks, or 1 , 2, 3, 4, 5, or 6 months or more after treatment initiation).
- the invention also includes methods of treating a subject having or at risk of developing PH (e.g., PAH, venous PH, hypoxic PH, thromboembolic PH, or miscellaneous PH) by administering to the subject an effective amount of a polypeptide described herein (e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1- 43 (e.g., SEQ ID NOs: 22-43)).
- a polypeptide described herein e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1- 43 (e.g., SEQ ID NOs: 22-43).
- the subject may have or be at risk of developing PH.
- the PH is PAH.
- the PAH is idiopathic PA
- the PAH is heritable PAH.
- the PAH is PAH related to (e.g., caused by or associated with) HIV infection, schistosomiasis, portal hypertension, pulmonary veno-occlusive disease, pulmonary capillary hemangiomatosis, cirrhosis of the liver, a congenital heart abnormality, a connective tissue/autoimmune disorder (e.g., scleroderma or lupus), or drug use or abuse (e.g., methamphetamine or cocaine use).
- the PH is venous PH.
- the venous PH is venous PH related to (e.g., caused by or associated with) left ventricular systolic dysfunction, left ventricular diastolic dysfunction, valvular heart disease, congenital cardiomyopathy, or congenital/acquired pulmonary venous stenosis.
- the PH is hypoxic PH.
- the hypoxic PH is hypoxic PH related to (e.g., caused by or associated with) chronic obstructive pulmonary disease (e.g., emphysema), interstitial lung disease, sleep-disordered breathing (e.g., sleep apnea), lung disease (e.g., pulmonary fibrosis), an alveolar hypoventilation disorder, chronic exposure to high altitude, or a developmental abnormality.
- the PH is thromboembolic PH.
- the thromboembolic PH is thromboembolic PH related to (e.g., caused by or associated with) chronic thromboembolic pulmonary hypertension, or other pulmonary artery obstructions (e.g., pulmonary emboli, angiosarcoma, arteritis, congenital pulmonary artery stenosis, or parasitic infection).
- the PH is miscellaneous PH.
- the miscellaneous PH is miscellaneous PH related to (e.g., caused by or associated with) a hematologic disease (e.g., chronic hemolytic anemia, sickle cell disease), a systemic disease (e.g., sarcoidosis, pulmonary Langerhans cell histiocytosis, lymphangioleiomyomatosis, neurofibromatosis, or vasculitis), a metabolic disorder (e.g., glycogen storage disease, Gaucher disease, or a thyroid disease), pulmonary tumoral thrombotic microangiopathy, fibrosing mediastinitis, chronic kidney failure, or segmental pulmonary hypertension).
- a hematologic disease e.g., chronic hemolytic anemia, sickle cell disease
- a systemic disease e.g., sarcoidosis, pulmonary Langerhans cell histiocytosis, lymphangioleiomyomatosis, neurofibromatosis, or vasculitis
- the methods described herein reduce the symptoms (e.g., reduce the severity or frequency of symptoms, such as shortness of breath (dyspnea), fatigue, swelling (e.g., edema) of the legs, feet, belly (ascites), or neck, chest pain or pressure, racing pulse or heart palpitations, bluish color to lips or skin (cyanosis), dizziness, or fainting) of PH compared to the frequency or severity of symptoms prior to treatment.
- the methods described herein prevent the development of PH or reduce the risk of developing PH (e.g., reduce the risk of developing PH compared to the development of PH in untreated subjects).
- the methods described herein slow or stop the progression of PH (e.g., slow the progression of PH compared to progression prior to treatment or compared to progression without treatment or in an untreated subject).
- the methods described herein reduce pulmonary vascular remodeling or vascular remodeling in the heart of a subject (e.g., the initiation or progression of vascular remodeling in the heart or lungs) compared to vascular remodeling prior to treatment or compared to vascular remodeling in an untreated subject.
- the methods described herein reduce right ventricular hypertrophy (e.g., reduce right ventricular hypertrophy or the progression of right ventricular hypertrophy) compared to right ventricular hypertrophy prior to treatment or compared to right ventricular hypertrophy in an untreated subject.
- the methods described herein reduce PH-associated bone loss (e.g., reduce PAH- associated bone loss, such as preventing or reducing the reduction in bone mineral density that occurs in subjects with PAH) compared to bone loss prior to treatment or compared to bone loss in an untreated subject.
- the methods described herein reduce pulmonary arterial muscularization and/or pulmonary arterial wall thickening compared to pulmonary arterial muscularization and/or pulmonary arterial wall thickening prior to treatment or compared to pulmonary arterial muscularization and/or pulmonary arterial wall thickening in an untreated subject.
- the methods described herein reduce right ventricular compensation compared to right ventricular compensation prior to treatment or compared to right ventricular compensation in an untreated subject.
- Symptoms of PH can be evaluated before and after treatment using standard clinical tests. Commonly used tests for evaluating PH include electrocardiograms, pulmonary function tests, echocardiograms, right heart catheterization, computed tomography scan, measurement of pulmonary vascular resistance, and the 6- minute walk test.
- the methods described herein reduce pulmonary vascular resistance (e.g., result in a reduction in pulmonary vascular resistance compared to pulmonary vascular resistance prior to treatment).
- the methods described herein improve performance in the 6-minute walk test compared to performance in the 6-minute walk test prior to treatment.
- the subject is identified as having PH prior to treatment with an ActRII chimera described herein.
- the method includes a step of identifying the subject as having PH (e.g., by evaluating symptoms of PH) prior to treatment with an ActRII chimera described herein.
- the method can further include evaluating PH symptoms after administration of an ActRII chimera described herein (e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days, 1 , 2, 3, 4, 5, 6, 7, or 8 weeks, or 1 , 2, 3, 4, 5, or 6 months or more after treatment initiation).
- the invention also includes methods of treating a subject having or at risk of developing a metabolic disease (e.g., obesity, Type 1 diabetes, or Type 2 diabetes) by administering to the subject an effective amount of a polypeptide described herein (e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- a polypeptide described herein e.g., a polypeptide including an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43).
- the subject may have a disease that results in obesity.
- the polypeptides described herein may be administered to a subject to prevent the development of obesity (e.g., in a subject at risk of developing obesity, e.g., a subject who is overweight, who has a family history of obesity, or who has other medical conditions or risk factors linked to increased risk of obesity (e.g., advanced age, or treatment with a medication associated with the development of obesity, such as a glucocorticoid (e.g., a corticosteroid, such as prednisone), a selective serotonin reuptake inhibitors (SSRI, e.g., paroxetine, mirtazapine, fluoxetine, escitalopram, sertraline), a tricyclic antidepressant (e.g., amitriptyline), a mood stabilizer (e.g., valproic acid, lithium), an antipsychotic (e.g., olanzapine, chlorpromazine, clozapine), and
- the subject has age-related obesity or metabolic disease. In some embodiments, the subject has treatment-related obesity or metabolic disease.
- Administration of an ActRII chimera described herein may reduce bodyweight by decreasing the amount of body fat. In some embodiments, the ActRII chimera decreases the amount of body fat while maintaining or increasing the amount of lean mass.
- the polypeptides described herein may be administered to a subject to prevent the development of diabetes (e.g., Type 1 or Type 2 diabetes, e.g., in a subject at risk of developing diabetes associated with advanced age or treatment with a medication associated with the development of diabetes, such as a glucocorticoid (e.g., a corticosteroid, e.g., glucocorticoid-induced diabetes mellitus), an SSRI, a serotonin-norepinephrine reuptake inhibitors (SNRI), a mood stabilizer (e.g., lithium and valproic acid), and an antipsychotic (e.g., olanzapine and clozapine)) and/or to treat a subject already diagnosed with diabetes.
- diabetes e.g., Type 1 or Type 2 diabetes
- a medication associated with the development of diabetes such as a glucocorticoid (e.g., a corticosteroid,
- the subject has age-related diabetes or metabolic disease. In some embodiments, the subject has treatment-related diabetes or metabolic disease.
- Subjects who are likely to develop diabetes e.g., subjects with a genetic predisposition to diabetes, a family history of diabetes, prediabetes, an autoimmune disease associated with diabetes, another metabolic disease, subjects of advanced age, or subjects treated with a medication associated with the development of diabetes may be administered the polypeptides described herein (e.g., a polypeptide including an ActRII chimera (e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) e.g., an effective amount of an ActRII chimera) prophylactically, such that the extracellular ActRII chimeras may maintain the normal function and health of b-cells and/or prevent or delay autoimmune inflammatory damage to b-cells.
- an ActRII chimera e.g.,
- the polypeptides described herein may be administered to individuals before diagnosis with diabetes (e.g., Type 1 and Type 2 diabetes) or the development of clinical symptoms of diabetes, e.g., high blood glucose level, high fasting insulin level, insulin resistance, polyuria, polydipsia, and polyphagia.
- the extracellular ActRII chimeras may be administered to patients prior to the patients needing insulin.
- the administration of extracellular ActRII chimeras may delay, reduce, or eliminate the need for insulin treatment in diabetic patients.
- administration of the extracellular ActRII chimeras of the invention to a subject may help to increase the rate of glucose clearance from the blood.
- the methods described herein reduce body fat (e.g., reduce the amount of subcutaneous, visceral, and/or hepatic fat, reduce adiposity, reduce the weights of epididymal and perirenal fat pads, or reduce body fat percentage). In some embodiments, the methods described herein reduce body weight or reduce body weight gain (e.g., reduce the percentage of body weight gain). In some embodiments, the methods described herein reduce the proliferation of adipose cells. In some embodiments, the methods described herein reduce LDL. In some embodiments, the methods described herein reduce triglycerides. In some embodiments, the methods described herein improve the serum lipid profile of the subject.
- the methods described herein reduce body fat and increase muscle mass. In some embodiments, the methods described herein reduce blood glucose levels (e.g., fasting glucose levels) or and/or increase glucose clearance. In some embodiments, the methods described herein reduce fasting insulin levels and/or improve insulin sensitivity (e.g., reduce insulin resistance). In some embodiments, the methods described herein regulate insulin biosynthesis and/or secretion from b-cells. These outcomes can be assessed by comparing measurements obtained after treatment to measurements taken prior to treatment. In some embodiments, the methods described herein do not affect the appetite for food intake.
- blood glucose levels e.g., fasting glucose levels
- the methods described herein reduce fasting insulin levels and/or improve insulin sensitivity (e.g., reduce insulin resistance).
- the methods described herein regulate insulin biosynthesis and/or secretion from b-cells. These outcomes can be assessed by comparing measurements obtained after treatment to measurements taken prior to treatment. In some embodiments, the methods described herein do not affect the appetite for food intake.
- polypeptides described herein may decrease body fat, decrease body weight, or increase insulin sensitivity and/or glucose clearance by increasing muscle mass.
- the subject is identified as having a metabolic disease prior to treatment with an ActRII chimera described herein.
- the method includes a step of identifying the subject as having a metabolic disease (e.g., by evaluating body weight, body fat, glucose clearance, or insulin sensitivity) prior to treatment with an ActRII chimera described herein.
- the method can further include evaluating body fat (e.g., amount of body fat or body fat percentage), body weight or body weight gain, fasting insulin levels, glucose clearance, serum lipid profile, or insulin sensitivity after administration of an ActRII chimera described herein (e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days, 1 , 2, 3, 4, 5, 6, 7, or 8 weeks, or 1 , 2, 3, 4, 5, or 6 months or more after treatment initiation).
- body fat e.g., amount of body fat or body fat percentage
- body weight or body weight gain e.g., fasting insulin levels, glucose clearance, serum lipid profile, or insulin sensitivity after administration of an ActRII chimera described herein (e.g., 12 hours, 24 hours, 1 , 2, 3, 4, 5, 6, or 7 days, 1 , 2, 3, 4, 5, 6, 7, or 8 weeks, or 1 , 2, 3, 4, 5, or 6 months or more after treatment initiation).
- a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a C-terminal extension of one to six amino acids e.g., 1 , 2, 3, 4, 5, 6 or more amino acids from extracellular ActRIIA or ActRIIB
- a dimer e.g., homodimer or heterodimer
- a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a polypeptide including an extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) fused to a moiety (e.g., a wild-type Fc domain, an Fc domain with amino acid substitutions (e.g., one more substitutions that reduce dimerization), an albumin-binding peptide, a fibronectin domain, or a serum albumin) may be used as the therapeutic protein.
- Nucleic acids encoding the polypeptides described herein, or vectors containing said nucleic acids can also be administered according to any of the methods described herein.
- the polypeptide, nucleic acid, or vector can be administered as part of a pharmaceutical composition.
- Expression plasmids encoding the fusion proteins were transiently expressed in HEK293 or CHO cells and conditioned media was collected. Conditioned media was loaded onto a protein A column, and target protein was eluted with a low pH buffer. Following buffer exchange into TBS, pH 7.4, the purified protein was characterized by CE-SDS using LabChip GXII (Perkin Elmer). The sequences of these proteins are provided in Table 5, below. Table 5. Sequences of tested ActRII-Fc and ActRII chimera-Fc proteins
- the GE Biacore 3000 was used to measure the kinetics of the interactions between the ActRII- and chimera-Fc proteins and Activin A/Activin B/growth differentiation factor 11 (GDF-11)/BMP-9/BMP- 10.
- Anti-human capture antibody was immobilized on all four flow cells of a CM4 or CM5 chip using the reagents and protocol in the Biacore Human Antibody Capture Kit (GE Life Sciences). Briefly, antihuman IgG was diluted to 25 pg/mL in immobilization buffer. The carboxylated surface of the sensor was activated by injecting a mixture of EDC and NHS.
- the anti-human IgG was injected into the activated sensor chip flow cells at 10 mL/min for a total of 7 minutes until the chip had reached an immobilization level of 9000 response units (RU). Ethanolamine was injected to deactivate the sensor surfaces. Flow cell 1 was left empty and served as a reference cell to measure and subtract any nonspecific binding. The ActRII- and chimera-Fc proteins were captured in flow cells 2-4 to a maximum analyte binding response of 100 resonance units. This was done by injecting between 5-10 ml_ of the ActRII- and chimera-FC proteins into the flow cells at a concentration of 2 pg/mL until 200 RU. Each ligand was run in a duplicate concentration series. The data was analyzed using Scrubbed by BioLogic Software to calculate the KD of each interaction (Table 6).
- Example 2 Evaluation of ActRII chimeras using a gene luciferase reporter assay
- ActRII- and chimera-Fc proteins were assayed for their ability to inhibit BMP-9
- BMP-10, activin A, activin B, and GDF-11 signaling were incubated with cells expressing a luciferase reporter, which activated the downstream signaling that results in luciferase expression.
- a functional inhibitor e.g., an ActRII- and chimera-Fc protein
- C2C12 cells containing a BMP-responsive BRE-Luciferase construct (produced using protocol from Zilberberg, 2007) were used to assess inhibition of BMP-9 and BMP-10 signaling
- HEK293 cells containing a Smad binding element SBE-Luciferase (BPS Bioscience) were used to assess inhibition of activin A, activin B, and GDF-11 signaling.
- Cells were plated on 96-well plates in DMEM supplemented with 2% FBS and placed in an incubator overnight to acclimate to the plate surface.
- a dilution series spanning between 10 ng/mL to 100 pg/mL of each chimera-Fc or positive control (ActRIIA-Fc and ActRIIB-Fc) was made in 2% DMEM at concentrations spanning the IC50 and incubated with Activin A (1 nM), Activin B (1 nM), GDF-11 (2 nM), BMP-9 (0.2 nM), or BMP10 (0.4 nM) for 60 minutes at 37 °C.
- Wells containing only the ligand and no ActRII- or chimera-Fc served as the positive control against which inhibition was calculated.
- Media on the plates was aspirated and the chimera- Fc/ligand mixtures were added to the plates as media replacement.
- the remaining wells were used for replicates of positive controls and background.
- the plates were incubated overnight at 37 °C, Promega Steady Glo was added to the plate according to the kit instructions, and the ODs of the wells were read on a Molecular Devices Spectramax M5e. Percent inhibition was calculated for each well by comparing the luciferase signal observed to the signal generated by the positive control. By testing a series of ActRII concentrations ranging from no inhibition to complete inhibition, the IC50 concentrations were calculated using GraphPad Prism software in a 4-parameter nonlinear regression model. The cell- based assays demonstrate the ability of the chimeras to inhibit signaling at the endogenous cell surface receptors (Table 7).
- Example 3 Effect of hydrodynamic injection of extracellular ActRII chimeras on body weight and lean mass
- hydrodynamic delivery of Chimera 1-Fc, Chimera 2-Fc, Chimera 2 E81Q-Fc, and Chimera 2 I65F E81Q-Fc significantly increased body weight in mice compared to vehicle control (****p ⁇ 0.0001 compared to vehicle cohort).
- hydrodynamic delivery of Chimera 1-Fc, Chimera 2-Fc, Chimera 2 E81Q-Fc, and Chimera 2 I65F E81Q-Fc significantly increased lean mass in mice compared to control (FIG. 3, ****p ⁇ 0.0001 compared to vehicle cohort).
- Example 5 Effect of extracellular ActRII chimeras on lean mass, hematology, and bone density and structure
- mice were enrolled in the study. Pre-dosing, mice were weight and lean mass determined using a small rodent nuclear magnetic resonance (NMR) analyzer (Bruker, Minispec LF50).
- NMR nuclear magnetic resonance
- HDI hydrodynamic tail vain injections
- blood was sampled from the submandibular vein in restrained conscious mice.
- EDTA was used as an anticoagulant and blood was analyzed using a Heska HT5 veterinary blood analyzer.
- FIGS. 6A-6D The effect of extracellular ActRI I chimeras on red blood cell, hemoglobin, and hematocrit levels and absolute reticulocytes is shown in FIGS. 6A-6D. Data are shown as average ⁇ SEM. Statistics are shown relative to vehicle treatment using 1-way ANOVA with a Fisher’s LSD post test. *** P ⁇ 0.001 , **** P ⁇ 0.0001 . FIG. 7 shows the effect of the extracellular ActRII chimeras on lean mass. Data are shown as average ⁇ SEM. Statistics are shown relative to vehicle treatment using 1-way ANOVA with a Fisher’s LSD post test. * P ⁇ 0.05 and **** P ⁇ 0.0001.
- FIGS. 8A-8D The effect of the extracellular ActRII chimeras on tibial bone mineral density, trabecular bone volume fraction of the proximal end of the tibia, trabecular spacing within the proximal end of the tibia, and trabecular number of the proximal end of the tibia are shown in FIGS. 8A-8D. Data are shown as average ⁇ SEM. Statistics are shown relative to vehicle treatment using 1- way ANOVA with a Fisher’s LSD post test. * P ⁇ 0.05, ** P ⁇ 0.01 , *** P ⁇ 0.001 , **** P ⁇ 0.0001.
- UUO unilateral ureteral obstruction
- the UUO model involves complete ligation of the left ureter while keeping the right kidney function intact. Briefly, UUO is performed on mice under anesthesia, whereby the left ureter is accessed via flank incision, and two ligatures are placed on the proximal one-third of the ureter using silk thread at 5 mm apart. Sham surgeries are performed in a similar fashion without placing any ligatures on the ureter. In this model, severe fibrosis develops in the kidney within 14 days following UUO, assessed by measuring kidney collagen by directly measuring the amount of hydroxyproline in the sample.
- PAH is induced in male rats using a single subcutaneous injection of monocrotaline (MCT, 40 mg/kg).
- MCT monocrotaline
- ActRII chimeras are randomized into vehicle or ActRII chimera treatment groups 24 hours after PAH induction and treated twice per week with an ActRII chimera (5 or 15 mg/kg) or vehicle for 21 days.
- Ventricular function and right ventricular (RV) remodeling are examined by electrocardiogram at day 14 by anesthetizing rats with 1.5% isoflurane and using a small animal high-frequency ultrasound probe to detect pulmonary flow acceleration, right ventricular function and hypertrophy, and left ventricular function while the animal is held in a supine position.
- RVH RV hypertrophy
- PAH is induced in male rats using a single subcutaneous injection of monocrotaline (MCT, 40 mg/kg).
- MCT monocrotaline
- Rats are injected again with MCT on day 18 and randomized into vehicle or ActRII chimera treatment groups. Rats are injected three times per week with an ActRII chimera (15 mg/kg) or vehicle. Hemodynamics and RVH are examined on day 35 as described above.
- Chow Purina LabDiet 5001 ; St. Louis, MO
- HFD high fat diet
- Body weights are measured twice per week at
- Example 9 Treatment of muscle disease by administration of an extracellular ActRII chimera
- a physician of skill in the art can treat a subject, such as a human patient, having muscle disease (e.g., neuromuscular disease, such as a muscular dystrophy, IBM, SMA, CMT, ALS, myasthenia gravis, or multiple sclerosis; sarcopenia; or cachexia) so as to increase muscle mass or maintain or improve muscle strength (e.g., reduce muscle weakness).
- muscle disease e.g., neuromuscular disease, such as a muscular dystrophy, IBM, SMA, CMT, ALS, myasthenia gravis, or multiple sclerosis; sarcopenia; or cachexia
- the method of treatment can include diagnosing or identifying a subject as a candidate for treatment based on standard clinical tests for muscle diseases (e.g., blood test, muscle biopsy, genetic test, and/or electromyogram).
- a physician of skill in the art can administer to the subject a composition containing an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the composition containing the extracellular ActRII chimera may be administered to the subject, for example, by parenteral injection (e.g., intravenous or subcutaneous injection) or by local administration (e.g., injection into the muscle) to treat muscle disease.
- the extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) is administered in a therapeutically effective amount, such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75,
- the extracellular ActRII chimera is administered bimonthly, once a month, once every four weeks, once every two weeks, or at least once a week or more (e.g., 1 , 2, 3, 4, 5, 6, or 7 times a week or more).
- the extracellular ActRII chimera is administered in an amount sufficient to increase muscle mass or maintain or improve muscle strength (e.g., reduce muscle weakness).
- a practitioner of skill in the art can monitor the patient’s improvement in response to the therapy by a variety of methods. For example, a physician can monitor the patient’s muscle mass, muscle strength, and motor function. A finding that the patient exhibits increased muscle mass or maintains or improves muscle strength following administration of the composition compared to test results prior to administration of the composition indicates that the patient is responding favorably to the treatment. Subsequent doses can be determined and administered as needed.
- Example 10 Treatment of bone disease by administration of an extracellular ActRII chimera
- a physician of skill in the art can treat a subject, such as a human patient, having bone disease (e.g., osteoporosis, osteogenesis imperfecta, or osteopenia) so as to increase bone mineral density, increase bone formation, reduce bone resorption, reduce bone loss, or reduce the risk or occurrence of bone fracture.
- the method of treatment can include diagnosing or identifying a subject as a candidate for treatment based on standard clinical tests for bone mineral density (e.g., dual X-ray absorptiometry).
- a physician of skill in the art can administer to the subject a composition containing an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the composition containing the extracellular ActRII chimera may be administered to the subject, for example, by parenteral injection (e.g., intravenous or subcutaneous injection) to treat bone disease.
- the extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) is administered in a therapeutically effective amount, such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1 .25, 1 .5, 1 .75, 2, 2.25, 2.5, 2.75, 3, 3.25, 3.5, 3.75, 4, 4.25, 4.5, 4.75, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 100, 150, 200, 250, 300, 350, 400, 450, or 500 mg/kg).
- a therapeutically effective amount such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1 .25, 1 .5, 1 .75, 2, 2.25
- the extracellular ActRII chimera is administered bimonthly, once a month, once every four weeks, once every two weeks, or at least once a week or more (e.g., 1 , 2, 3, 4, 5, 6, or 7 times a week or more).
- the extracellular ActRII chimera is administered in an amount sufficient to increase bone mineral density, increase bone formation, reduce bone resorption, reduce bone loss, or reduce the risk or occurrence of bone fracture.
- a practitioner of skill in the art can monitor the patient’s improvement in response to the therapy by a variety of methods. For example, a physician can monitor the patient’s bone mineral density by performing dual X-ray absorptiometry. A finding that the patient exhibits increased bone mineral density, increased bone formation, reduced bone resorption, reduced bone loss, or a reduced risk or occurrence of bone fracture following administration of the composition compared to test results prior to administration of the composition indicates that the patient is responding favorably to the treatment. Subsequent doses can be determined and administered as needed.
- Example 11 Treatment of anemia by administration of an extracellular ActRII chimera
- a physician of skill in the art can treat a subject, such as a human patient, having anemia (e.g., anemia of inflammation, anemia associated with myelofibrosis, anemia associated with a myelodysplastic syndrome, or anemia associated with chronic kidney disease) so as to increase a parameter of red cell mass, such as red blood cell count, hemoglobin levels, or hematocrit, or to increase the maturation and/or differentiation of erythroid progenitors, increase late- stage erythroid precursor maturation, increase the number of early-stage erythroid precursors and/or progenitors, promote the progression of erythroid precursors and/or progenitors through erythropoiesis, or recruit early-stage progenitors into the erythroid lineage.
- anemia e.g., anemia of inflammation, anemia associated with myelofibrosis, anemia associated with a myelodysplastic syndrome, or anemia associated with chronic kidney disease
- red cell mass such as
- the method of treatment can include diagnosing or identifying a subject as a candidate for treatment based on a blood test measuring hematological parameters.
- a physician of skill in the art can administer to the subject a composition containing an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the composition containing the extracellular ActRII chimera may be administered to the subject, for example, by parenteral injection (e.g., intravenous or subcutaneous injection) to treat anemia.
- the extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) is administered in a therapeutically effective amount, such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1.25, 1.5, 1.75, 2, 2.25, 2.5, 2.75, 3, 3.25, 3.5, 3.75, 4, 4.25, 4.5, 4.75, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 100, 150, 200, 250, 300, 350, 400, 450, or 500 mg/kg).
- a therapeutically effective amount such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1.25, 1.5, 1.75, 2, 2.25, 2.5, 2.75, 3, 3.25, 3.5
- the extracellular ActRII chimera is administered bimonthly, once a month, once every four weeks, once every two weeks, or at least once a week or more (e.g., 1 , 2, 3, 4, 5, 6, or 7 times a week or more).
- the extracellular ActRII chimera is administered in an amount sufficient to increase hemoglobin levels, increase red blood cell counts, increase hematocrit, increase the maturation and/or differentiation of erythroid progenitors, increase late-stage erythroid precursor maturation, increase the number of early- stage erythroid precursors and/or progenitors, promote the progression of erythroid precursors and/or progenitors through erythropoiesis, or recruit early-stage progenitors into the erythroid lineage.
- a practitioner of skill in the art can monitor the patient’s improvement in response to the therapy by a variety of methods. For example, a physician can monitor the patient’s hemoglobin levels, red blood cell counts, or hematocrit by performing a blood test. A finding that the patient exhibits improved hemoglobin levels, red blood cell counts, or hematocrit following administration of the composition compared to test results prior to administration of the composition indicates that the patient is responding favorably to the treatment. Subsequent doses can be determined and administered as needed.
- Example 12 Treatment of fibrosis by administration of an extracellular ActRII chimera
- a physician of skill in the art can treat a subject, such as a human patient, having fibrosis (e.g., pulmonary fibrosis, myelofibrosis, or fibrosis associated with chronic kidney disease) so as to reduce the symptoms of fibrosis or slow or stop the progression of fibrosis.
- the method of treatment can include diagnosing or identifying a subject as a candidate for treatment based on clinical tests for fibrosis (e.g., imaging tests, such as X-ray or CT scan).
- a physician of skill in the art can administer to the subject a composition containing an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the composition containing the extracellular ActRII chimera may be administered to the subject, for example, by parenteral injection (e.g., intravenous or subcutaneous injection) to treat fibrosis, or can be locally administered (e.g., injected) to the fibrotic tissue or organ.
- the extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) is administered in a therapeutically effective amount, such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1.25, 1.5, 1.75, 2,
- the extracellular ActRII chimera is administered bimonthly, once a month, once every four weeks, once every two weeks, or at least once a week or more (e.g., 1 , 2, 3, 4, 5, 6, or 7 times a week or more).
- the extracellular ActRII chimera is administered in an amount sufficient to reduce the symptoms of fibrosis or slow or stop the progression of fibrosis.
- a practitioner of skill in the art can monitor the patient’s improvement in response to the therapy by a variety of methods. For example, a physician can monitor the patient’s fibrosis by performing imaging tests and can monitor the patient’s symptoms using standard clinical tests. A finding that the patient’s symptoms are reduced or that progression of the patient’s fibrosis slows or stops following administration of the composition compared to test results prior to administration of the composition indicates that the patient is responding favorably to the treatment. Subsequent doses can be determined and administered as needed.
- Example 13 Treatment of pulmonary hypertension by administration of an extracellular ActRII chimera
- a physician of skill in the art can treat a subject, such as a human patient, having pulmonary hypertension (PH, e.g., PAH) so as to reduce the symptoms of PH or slow or stop the progression of PH.
- the method of treatment can include diagnosing or identifying a subject as a candidate for treatment based on standard clinical tests for PH (e.g., echocardiogram, electrocardiogram, chest X-ray, or right heart catheterization).
- a physician of skill in the art can administer to the subject a composition containing an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the composition containing the extracellular ActRI I chimera may be administered to the subject, for example, by parenteral injection (e.g., intravenous or subcutaneous injection) to treat PH.
- the extracellular ActRI I chimera (e.g., an extracellular ActRI I chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) is administered in a therapeutically effective amount, such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1 .25, 1 .5, 1 .75, 2, 2.25, 2.5, 2.75, 3, 3.25, 3.5, 3.75, 4, 4.25, 4.5, 4.75, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 100, 150, 200, 250, 300, 350, 400, 450, or 500 mg/kg).
- a therapeutically effective amount such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1 .25, 1 .5, 1 .75, 2, 2.25
- the extracellular ActRI I chimera is administered bimonthly, once a month, once every four weeks, once every two weeks, or at least once a week or more (e.g., 1 , 2, 3, 4, 5, 6, or 7 times a week or more).
- the extracellular ActRII chimera is administered in an amount sufficient to reduce the symptoms of PH or slow or stop the progression of PH.
- a practitioner of skill in the art can monitor the patient’s improvement in response to the therapy by a variety of methods. For example, a physician can monitor the patient’s symptoms using standard clinical tests and patient self-reporting. A finding that the patient’s symptoms are reduced the symptoms of PH or that progression of the patient’s PH slows or stops following administration of the composition compared to test results prior to administration of the composition indicates that the patient is responding favorably to the treatment. Subsequent doses can be determined and administered as needed.
- Example 14 Treatment of metabolic disease by administration of an extracellular ActRII chimera
- a physician of skill in the art can treat a subject, such as a human patient, having a metabolic disease (e.g., obesity) so as to reduce body weight, body fat or percent body fat, or improve the serum lipid profile of the subject.
- a physician of skill in the art can administer to the subject a composition containing an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the composition containing the extracellular ActRII chimera may be administered to the subject, for example, by parenteral injection (e.g., intravenous or subcutaneous injection) to treat obesity.
- the extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)) is administered in a therapeutically effective amount, such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1 .25, 1 .5, 1 .75, 2, 2.25, 2.5, 2.75, 3, 3.25, 3.5, 3.75, 4, 4.25, 4.5, 4.75, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 100, 150, 200, 250, 300, 350, 400, 450, or 500 mg/kg).
- a therapeutically effective amount such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75, 1 , 1 .25, 1 .5, 1 .75, 2, 2.25
- the extracellular ActRII chimera is administered bimonthly, once a month, once every four weeks, once every two weeks, or at least once a week or more (e.g., 1 , 2, 3, 4, 5, 6, or 7 times a week or more).
- the extracellular ActRII chimera is administered in an amount sufficient to reduce body weight, body fat or percent body fat, or improve the serum lipid profile of the subject.
- a practitioner of skill in the art can monitor the patient’s improvement in response to the therapy by a variety of methods. For example, a physician can monitor the patient’s symptoms using standard clinical tests and patient self-reporting. A finding that the patient’s body weight, body fat, or percent body fat is reduced, or that the patient’s serum lipid profile is improved following administration of the composition compared to test results prior to administration of the composition indicates that the patient is responding favorably to the treatment. Subsequent doses can be determined and administered as needed.
- Example 15 Treatment of thrombocytopenia by administration of an extracellular ActRII chimera
- a physician of skill in the art can treat a subject, such as a human patient, having thrombocytopenia (e.g., thrombocytopenia associated with a myelodysplastic syndrome or myelofibrosis) so as to increase platelet levels (e.g., increase platelet count), increase platelet production, and/or increase megakaryocyte differentiation and/or maturation.
- thrombocytopenia e.g., thrombocytopenia associated with a myelodysplastic syndrome or myelofibrosis
- platelet levels e.g., increase platelet count
- megakaryocyte differentiation and/or maturation e.g., megakaryocyte differentiation and/or maturation.
- a physician of skill in the art can administer to the subject a composition containing an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-4
- the composition containing the extracellular ActRII chimera may be administered to the subject, for example, by parenteral injection (e.g., intravenous or subcutaneous injection) to treat thrombocytopenia.
- the extracellular ActRII chimera e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)
- a therapeutically effective amount such as from 0.01 to 500 mg/kg (e.g., 0.01 , 0.1 , 0.2, 0.3, 0.4, 0.5, 0.75,
- the extracellular ActRII chimera is administered bimonthly, once a month, once every four weeks, once every two weeks, or at least once a week or more (e.g., 1 , 2, 3, 4, 5, 6, or 7 times a week or more).
- the extracellular ActRII chimera is administered in an amount sufficient to increase platelet levels (e.g., increase platelet count), increase platelet production, and/or increase megakaryocyte differentiation and/or maturation.
- a practitioner of skill in the art can monitor the patient’s improvement in response to the therapy by a variety of methods. For example, a physician can monitor the patient’s platelet count using a blood test. A finding that the patient’s platelet levels are increased (e.g., a finding of an increased platelet count) following administration of the composition compared to test results prior to administration of the composition indicates that the patient is responding favorably to the treatment. Subsequent doses can be determined and administered as needed.
- Example 16 Treatment of neutropenia by administration of an extracellular ActRII chimera
- a physician of skill in the art can treat a subject, such as a human patient, having neutropenia (e.g., neutropenia associated with a myelodysplastic syndrome or myelofibrosis) so as to increase neutrophil levels (e.g., increase neutrophil count), increase neutrophil production, and/or increase the differentiation and/or maturation of progenitor cells (e.g., myeloid progenitors, myeloblasts, or myelocytes) into neutrophils.
- neutropenia e.g., neutropenia associated with a myelodysplastic syndrome or myelofibrosis
- neutrophil levels e.g., increase neutrophil count
- progenitor cells e.g., myeloid progenitors, myeloblasts, or myelocytes
- a physician of skill in the art can administer to the subject a composition containing an extracellular ActRII chimera (e.g., an extracellular ActRII chimera having the sequence of any one of SEQ ID NOs: 1-43 (e.g., SEQ ID NOs: 22-43)).
- the composition containing the extracellular ActRII chimera may be administered to the subject, for example, by parenteral injection (e.g., intravenous or subcutaneous injection) to treat neutropenia.
Landscapes
- Health & Medical Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Organic Chemistry (AREA)
- General Health & Medical Sciences (AREA)
- Medicinal Chemistry (AREA)
- Engineering & Computer Science (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Public Health (AREA)
- Pharmacology & Pharmacy (AREA)
- Animal Behavior & Ethology (AREA)
- Veterinary Medicine (AREA)
- Genetics & Genomics (AREA)
- Zoology (AREA)
- Molecular Biology (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- General Chemical & Material Sciences (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Biophysics (AREA)
- Biochemistry (AREA)
- Gastroenterology & Hepatology (AREA)
- Toxicology (AREA)
- Immunology (AREA)
- Physical Education & Sports Medicine (AREA)
- Hematology (AREA)
- Diabetes (AREA)
- Orthopedic Medicine & Surgery (AREA)
- Cell Biology (AREA)
- Epidemiology (AREA)
- Rheumatology (AREA)
- Biomedical Technology (AREA)
- Neurology (AREA)
- General Engineering & Computer Science (AREA)
- Wood Science & Technology (AREA)
- Biotechnology (AREA)
- Obesity (AREA)
- Pulmonology (AREA)
- Child & Adolescent Psychology (AREA)
- Microbiology (AREA)
Abstract
Description









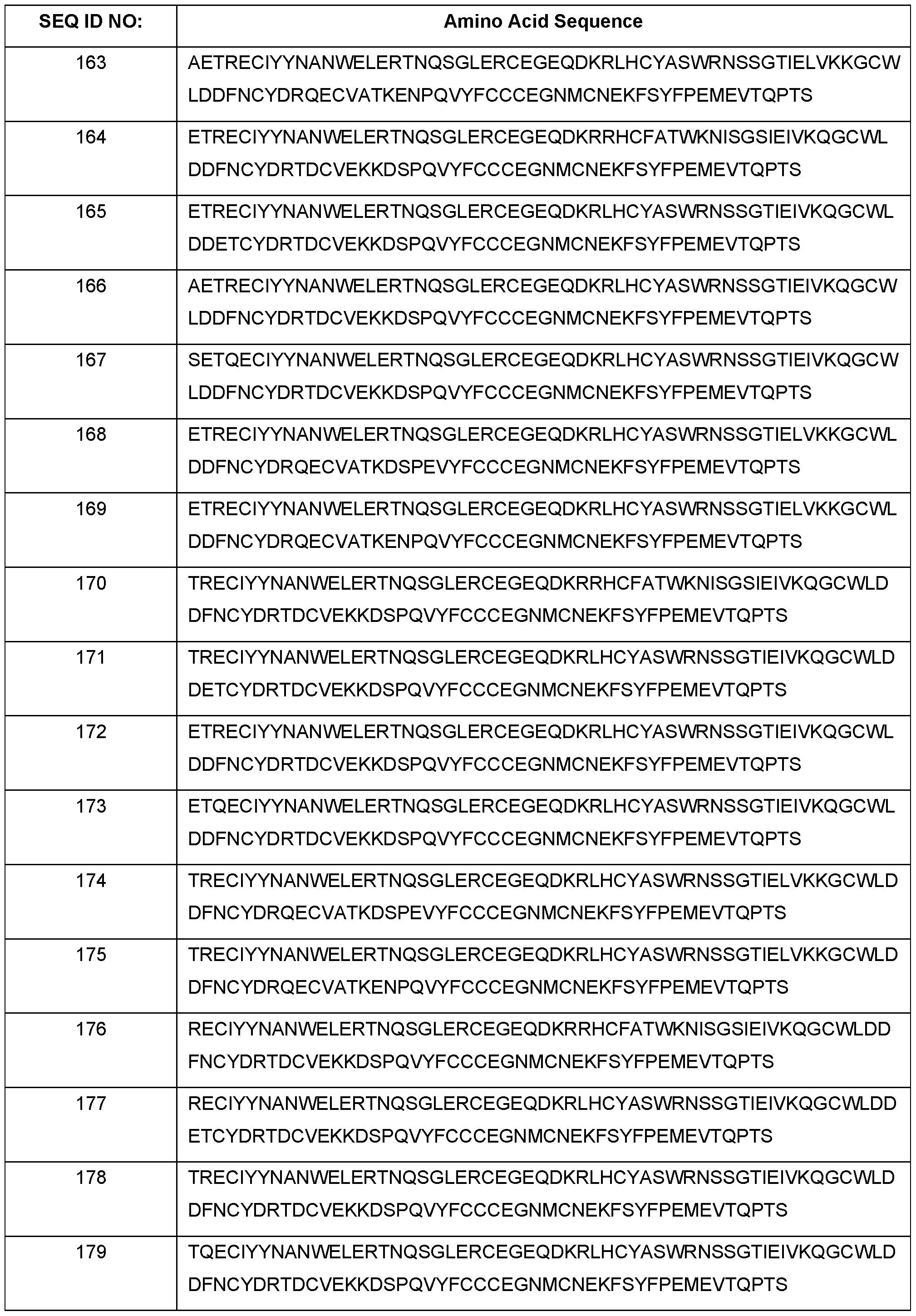







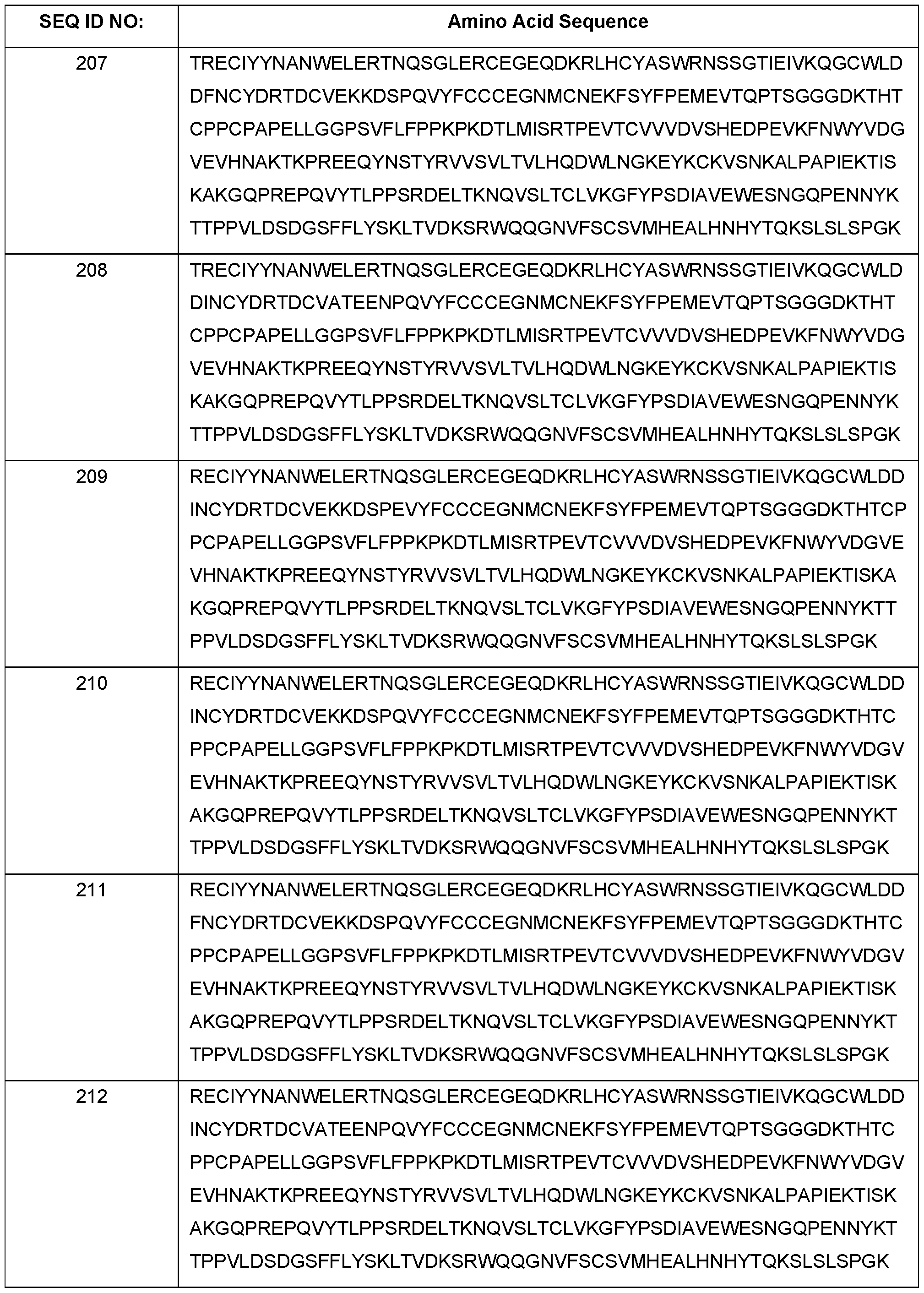















Claims
Priority Applications (10)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| CN202180036856.2A CN115768457A (en) | 2020-03-20 | 2021-03-19 | Activin receptor type II chimeras and methods of use thereof |
| AU2021237730A AU2021237730A1 (en) | 2020-03-20 | 2021-03-19 | Activin receptor type II chimeras and methods of use thereof |
| JP2022556076A JP2023518260A (en) | 2020-03-20 | 2021-03-19 | Activin receptor type II chimera and method of use thereof |
| KR1020227036350A KR20230004515A (en) | 2020-03-20 | 2021-03-19 | Activin receptor type II chimeras and methods of use thereof |
| IL296394A IL296394A (en) | 2020-03-20 | 2021-03-19 | Activin receptor type ii chimeras and methods of use thereof |
| CA3176735A CA3176735A1 (en) | 2020-03-20 | 2021-03-19 | Activin receptor type ii chimeras and methods of use thereof |
| EP21770547.4A EP4121078A4 (en) | 2020-03-20 | 2021-03-19 | Activin receptor type ii chimeras and methods of use thereof |
| US17/945,299 US12522646B2 (en) | 2020-03-20 | 2022-09-15 | Activin receptor type II chimeras and methods of use thereof |
| JP2025131256A JP2025179059A (en) | 2020-03-20 | 2025-08-06 | Activin receptor type II chimeras and methods of use thereof |
| US19/415,215 US20260098078A1 (en) | 2020-03-20 | 2025-12-10 | Activin receptor type ii chimeras and methods of use thereof |
Applications Claiming Priority (6)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US202062992839P | 2020-03-20 | 2020-03-20 | |
| US62/992,839 | 2020-03-20 | ||
| US202063029443P | 2020-05-23 | 2020-05-23 | |
| US63/029,443 | 2020-05-23 | ||
| US202063109821P | 2020-11-04 | 2020-11-04 | |
| US63/109,821 | 2020-11-04 |
Related Child Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| US17/945,299 Continuation US12522646B2 (en) | 2020-03-20 | 2022-09-15 | Activin receptor type II chimeras and methods of use thereof |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2021189019A1 true WO2021189019A1 (en) | 2021-09-23 |
Family
ID=77771655
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2021/023353 Ceased WO2021189019A1 (en) | 2020-03-20 | 2021-03-19 | Activin receptor type ii chimeras and methods of use thereof |
Country Status (9)
| Country | Link |
|---|---|
| US (2) | US12522646B2 (en) |
| EP (1) | EP4121078A4 (en) |
| JP (2) | JP2023518260A (en) |
| KR (1) | KR20230004515A (en) |
| CN (1) | CN115768457A (en) |
| AU (1) | AU2021237730A1 (en) |
| CA (1) | CA3176735A1 (en) |
| IL (1) | IL296394A (en) |
| WO (1) | WO2021189019A1 (en) |
Cited By (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US11484573B2 (en) | 2017-11-09 | 2022-11-01 | Keros Therapeutics, Inc. | Activin receptor type IIa variants and methods of use thereof |
| US11717558B2 (en) | 2016-11-10 | 2023-08-08 | Keros Therapeutics, Inc. | Nucleic acid molecules encoding activin receptor type IIA variants |
| US11884715B2 (en) | 2018-01-12 | 2024-01-30 | Keros Therapeutics, Inc. | Activin receptor type IIB variants and methods of use thereof |
| US11945856B2 (en) | 2022-01-28 | 2024-04-02 | 35Pharma Inc. | Activin receptor type IIB variants and uses thereof |
| WO2024238950A1 (en) * | 2023-05-18 | 2024-11-21 | Keros Therapeutics, Inc. | Methods of using activin receptor type ii variants |
| WO2025039072A1 (en) * | 2023-08-18 | 2025-02-27 | 35Pharma Inc. | Activin receptor type iib variants and uses thereof |
| WO2025050218A1 (en) * | 2023-09-08 | 2025-03-13 | 35Pharma Inc. | Combination therapy with actriib receptor variants and glp-1 agonists |
| US12364737B2 (en) | 2018-05-09 | 2025-07-22 | Keros Therapeutics, Inc. | Activin receptor type IIA variants and methods of use thereof |
| US12440539B2 (en) | 2020-03-20 | 2025-10-14 | Keros Therapeutics, Inc. | Methods of using activin receptor type IIB variants |
| EP4653010A1 (en) | 2024-05-14 | 2025-11-26 | 35Pharma Inc. | Activin receptor type iib traps for use in improving body composition |
Families Citing this family (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN116919968A (en) * | 2023-08-14 | 2023-10-24 | 上海交通大学医学院附属第九人民医院 | Application of ponifinib phosphate in preparation of medicine for promoting skin wound healing |
| WO2025147483A1 (en) * | 2024-01-02 | 2025-07-10 | Keros Therapeutics, Inc. | Methods of using activin receptor type ii chimeras |
Citations (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20180148491A1 (en) * | 2015-04-22 | 2018-05-31 | Alivegen Usa, Inc. | Novel Hybrid ActRIIB Ligand Trap Proteins For Treating Muscle Wasting Diseases |
| US20180161426A1 (en) * | 2015-05-20 | 2018-06-14 | Maria CAPPELLINI | In vitro cell culture methods for beta-thalassemia using activin type ii receptor ligand traps |
| WO2019094751A1 (en) * | 2017-11-09 | 2019-05-16 | Keros Therapeutics, Inc. | Activin receptor type iia variants and methods of use thereof |
| US20190330307A1 (en) * | 2016-10-20 | 2019-10-31 | Biogen Ma Inc. | Methods for treating muscle wasting and bone disease using novel hybrid actriib ligand trap proteins |
| US20190345225A1 (en) * | 2016-11-10 | 2019-11-14 | Keros Therapeutics, Inc. | Activin receptor type iia variants and methods of use thereof |
Family Cites Families (100)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20040223966A1 (en) | 2002-10-25 | 2004-11-11 | Wolfman Neil M. | ActRIIB fusion polypeptides and uses therefor |
| JP2008507288A (en) | 2004-07-23 | 2008-03-13 | アクセルロン ファーマ インコーポレーテッド | ActRII receptor polypeptides, methods, and compositions |
| US8008453B2 (en) | 2005-08-12 | 2011-08-30 | Amgen Inc. | Modified Fc molecules |
| US8067562B2 (en) | 2005-11-01 | 2011-11-29 | Amgen Inc. | Isolated nucleic acid molecule comprising the amino acid sequence of SEQ ID NO:1 |
| ES2649983T3 (en) | 2005-11-23 | 2018-01-16 | Acceleron Pharma, Inc. | Activin-ActRIIa antagonists in their use to promote bone growth |
| US8101564B2 (en) | 2006-05-03 | 2012-01-24 | Trustees Of The University Of Pennsylvania | Methods for regulating osteoclast differentiation and bone resorption using LRRc17 |
| CN104524548A (en) | 2006-12-18 | 2015-04-22 | 阿塞勒隆制药公司 | Activin-ACTRII antagonists and uses for increasing red blood cell levels |
| US20100028332A1 (en) | 2006-12-18 | 2010-02-04 | Acceleron Pharma Inc. | Antagonists of actriib and uses for increasing red blood cell levels |
| AU2016250354B2 (en) | 2006-12-18 | 2019-01-17 | Acceleron Pharma Inc. | Activin-ActRII antagonists and uses for increasing red blood cell levels |
| US8895016B2 (en) | 2006-12-18 | 2014-11-25 | Acceleron Pharma, Inc. | Antagonists of activin-actriia and uses for increasing red blood cell levels |
| MX2009008222A (en) | 2007-02-01 | 2009-10-12 | Acceleron Pharma Inc | Activin-actriia antagonists and uses for treating or preventing breast cancer. |
| TW201803890A (en) | 2007-02-02 | 2018-02-01 | 艾瑟勒朗法瑪公司 | Variants derived from ActRIIB and their uses |
| EA018221B1 (en) | 2007-02-09 | 2013-06-28 | Акселерон Фарма Инк. | ACTIVIN-ActRIIa ANTAGONISTS AND USES FOR PROMOTING BONE GROWTH IN CANCER PATIENTS |
| US7947646B2 (en) | 2007-03-06 | 2011-05-24 | Amgen Inc. | Variant activin receptor polypeptides |
| US8501678B2 (en) | 2007-03-06 | 2013-08-06 | Atara Biotherapeutics, Inc. | Variant activin receptor polypeptides and uses thereof |
| WO2009015345A1 (en) | 2007-07-25 | 2009-01-29 | Amgen Inc. | Pharmaceutical compositions comprising fc fusion proteins |
| CN101861161B (en) | 2007-09-18 | 2017-04-19 | 阿塞勒隆制药公司 | ACTIN-ACTRIIA ANTAGONISTS AND USE FOR REDUCING OR INHIBITING FSH SECRETION |
| EP2242506A4 (en) | 2008-01-07 | 2011-12-28 | Janssen Biotech Inc | Method of treating erythropoietin hyporesponsive anemias |
| WO2009111793A2 (en) | 2008-03-07 | 2009-09-11 | Myoscience, Inc. | Subdermal tissue remodeling using myostatin, methods and related systems |
| CN102131822A (en) | 2008-06-26 | 2011-07-20 | 阿塞勒隆制药公司 | Methods for dosing activin-actriia antagonist and monitoring of treated patients |
| DK2318028T3 (en) | 2008-06-26 | 2020-05-04 | Acceleron Pharma Inc | ANTAGONISTS OF SOLVABLE ACTIVIN ACTIVIA AND APPLICATIONS TO INCREASE RED BLOOD CELL LEVELS |
| TW201803586A (en) | 2008-08-14 | 2018-02-01 | 艾瑟勒朗法瑪公司 | Use GDF traps to increase red blood cell levels |
| US8216997B2 (en) | 2008-08-14 | 2012-07-10 | Acceleron Pharma, Inc. | Methods for increasing red blood cell levels and treating anemia using a combination of GDF traps and erythropoietin receptor activators |
| JP5611222B2 (en) | 2008-11-26 | 2014-10-22 | アムジエン・インコーポレーテツド | Activin IIB receptor polypeptide variants and uses thereof |
| AU2010204985A1 (en) | 2009-01-13 | 2011-08-04 | Acceleron Pharma Inc. | Methods for increasing adiponectin |
| KR20120049214A (en) | 2009-06-08 | 2012-05-16 | 악셀레론 파마 인코포레이티드 | Methods for increasing thermogenic adipocytes |
| KR20180026795A (en) | 2009-06-12 | 2018-03-13 | 악셀레론 파마 인코포레이티드 | TRUNCATED ActRIIB-FC FUSION PROTEINS |
| AU2010282361B2 (en) | 2009-08-13 | 2015-03-19 | Acceleron Pharma Inc. | Combined use of GDF traps and erythropoietin receptor activators to increase red blood cell levels |
| EP3202459B1 (en) | 2009-09-09 | 2021-04-14 | Acceleron Pharma Inc. | Actriib antagonists and dosing and uses thereof for treating obesity or type 2 diabetes by regulating body fat content |
| AU2010315245B2 (en) | 2009-11-03 | 2016-11-03 | Acceleron Pharma Inc. | Methods for treating fatty liver disease |
| EP3332796A1 (en) | 2009-11-17 | 2018-06-13 | Acceleron Pharma Inc. | Actriib proteins and variants and uses therefore relating to utrophin induction for muscular dystrophy therapy |
| WO2012027065A2 (en) | 2010-08-27 | 2012-03-01 | Celgene Corporation | Combination therapy for treatment of disease |
| AU2011326586A1 (en) | 2010-11-08 | 2013-05-30 | Acceleron Pharma, Inc. | ActRIIA binding agents and uses thereof |
| US8501768B2 (en) | 2011-05-17 | 2013-08-06 | Hoffmann-La Roche Inc. | Hexahydrocyclopentapyrrolone, hexahydropyrrolopyrrolone, octahydropyrrolopyridinone and octahydropyridinone compounds |
| KR20140084211A (en) | 2011-10-17 | 2014-07-04 | 악셀레론 파마 인코포레이티드 | Methods and compositions for treating ineffective erythropoiesis |
| DK2780368T3 (en) | 2011-11-14 | 2018-02-05 | Regeneron Pharma | COMPOSITIONS AND PROCEDURES FOR INCREASING MUSCLE MASS AND MUSCLE STRENGTH BY SPECIFIC ANTAGONIZATION OF GDF8 AND / OR ACTIVIN A |
| GR1007832B (en) | 2011-11-21 | 2013-02-14 | Ιδρυμα Ιατροβιολογικων Ερευνων Ακαδημιας Αθηνων, | Activin neutralisers and uses thereof for treatment of diseases associated with aberrant "host defence response" activation |
| HK1203384A1 (en) | 2011-12-19 | 2015-12-11 | Amgen Inc. | Variant activin receptor polypeptides, alone or in combination with chemotherapy, and uses thereof |
| KR101995751B1 (en) | 2012-01-05 | 2019-07-03 | 주식회사 와이바이오로직스 | Myostatin inhibitor including extracellular domain of delta-like 1 homolog |
| EP2844271B1 (en) | 2012-05-17 | 2018-02-28 | Paranta Biosciences Limited | Use of follistatin or of an activin inhibitor for preventing or treating tissue graft dysfunction |
| NZ703724A (en) | 2012-06-11 | 2017-06-30 | Amgen Inc | Dual receptor antagonistic antigen-binding proteins and uses thereof |
| UA116639C2 (en) | 2012-10-09 | 2018-04-25 | Рег'Юлес Терап'Ютікс Інк. | Methods for treatment of alport syndrome |
| HK1214504A1 (en) | 2012-10-24 | 2016-07-29 | 细胞基因公司 | Methods for treating anemia |
| WO2014138485A1 (en) | 2013-03-08 | 2014-09-12 | Irm Llc | Ex vivo production of platelets from hematopoietic stem cells and the product thereof |
| US20160038588A1 (en) | 2013-03-15 | 2016-02-11 | Amgen Inc. | Myostatin Antagonism in Human Subjects |
| RS61778B1 (en) | 2013-05-06 | 2021-06-30 | Scholar Rock Inc | Compositions and methods for growth factor modulation |
| US20160333418A1 (en) | 2014-01-14 | 2016-11-17 | Santa Maria Biotherapeutics, Inc. | Activin Inhibitor Response Prediction and Uses for Treatment |
| JP2017509647A (en) | 2014-03-21 | 2017-04-06 | アクセルロン ファーマ, インコーポレイテッド | Methods of treating red blood cell production by increasing red blood cell levels by inhibiting activin B and / or GDF11 |
| EP3808778A1 (en) | 2014-04-18 | 2021-04-21 | Acceleron Pharma Inc. | Methods for increasing red blood cell levels and treating sickle-cell disease |
| PE20170471A1 (en) | 2014-06-13 | 2017-05-14 | Santa Maria Biotherapeutics Inc | FORMULATED RECEPTOR POLYPEPTIDES AND RELATED METHODS |
| CN114699529A (en) | 2014-06-13 | 2022-07-05 | 阿塞勒隆制药公司 | Methods and compositions for treating ulcers |
| MX373052B (en) | 2014-06-17 | 2020-05-11 | Nippon Shinyaku Co Ltd | ANTISENSE NUCLEIC ACIDS. |
| CA2958585C (en) | 2014-08-21 | 2024-01-09 | Stealth Biotherapeutics Corp | Use of peptide d-arg-2',6'-dmt-lys-phe-nh2 for the treatment of alport syndrome |
| MA41052A (en) | 2014-10-09 | 2017-08-15 | Celgene Corp | TREATMENT OF CARDIOVASCULAR DISEASE USING ACTRII LIGAND TRAPS |
| GB201421379D0 (en) | 2014-12-02 | 2015-01-14 | Isis Innovation Ltd And Medical Res Council | Molecule |
| MA41119A (en) | 2014-12-03 | 2017-10-10 | Acceleron Pharma Inc | METHODS OF TREATMENT OF MYELODYSPLASIC SYNDROMES AND SIDEROBLASTIC ANEMIA |
| JP2018501307A (en) | 2014-12-03 | 2018-01-18 | セルジーン コーポレイション | Activin-ActRII antagonist and use for treating anemia |
| US20230142386A1 (en) | 2014-12-03 | 2023-05-11 | Celgene Corporation | Activin-actrii antagonists and uses for treating anemia |
| MA41920B1 (en) * | 2015-04-06 | 2021-05-31 | Acceleron Pharma Inc | Single-arm type i and type ii receptor fusion proteins and their uses |
| US10358476B2 (en) | 2015-04-06 | 2019-07-23 | Acceleron Pharma Inc. | Single arm type I and type II receptor fusion proteins and uses thereof |
| US20180125928A1 (en) | 2015-05-13 | 2018-05-10 | Celgene Corporation | Treatment of beta-thalassemia using actrii ligand traps |
| WO2017079591A2 (en) | 2015-11-04 | 2017-05-11 | Acceleron Pharma Inc. | Methods for increasing red blood cell levels and treating ineffective erythropoiesis |
| EP3380121B1 (en) | 2015-11-23 | 2023-12-20 | Acceleron Pharma Inc. | Actrii antagonist for use in treating eye disorders |
| US20170240639A1 (en) | 2016-02-22 | 2017-08-24 | Acceleron Pharma Inc. | Actrii antagonists for use in increasing immune activity |
| DK3496739T3 (en) | 2016-07-15 | 2021-05-10 | Acceleron Pharma Inc | COMPOSITIONS INCLUDING ACTRIIA POLYPEPTIDES FOR USE IN THE TREATMENT OF PULMONAL HYPERTENSION |
| MA45811A (en) | 2016-07-27 | 2019-06-05 | Acceleron Pharma Inc | METHODS AND COMPOSITIONS OF TREATMENT OF DISEASE. |
| CN110036025B (en) | 2016-10-05 | 2024-03-22 | 阿塞勒隆制药公司 | Variant ActRIIB proteins and uses thereof |
| CA3039074A1 (en) | 2016-10-05 | 2018-04-12 | Acceleron Pharma Inc. | Compositions and method for treating kidney disease |
| CA3039573A1 (en) | 2016-10-05 | 2018-04-12 | Acceleron Pharma Inc. | Alk4:actriib heteromultimers and uses thereof |
| WO2018089702A1 (en) | 2016-11-10 | 2018-05-17 | Keros Therapeutics, Inc. | Gdnf fusion polypeptides and methods of use thereof |
| GB201620119D0 (en) | 2016-11-29 | 2017-01-11 | Pharmafox Therapeutics Ag | Compounds |
| EP3576773B1 (en) | 2017-02-01 | 2023-10-18 | Acceleron Pharma Inc. | Tgf beta and actrii antagonists for use in treating leukemia |
| CA3052625A1 (en) | 2017-02-06 | 2018-08-09 | Acceleron Pharma Inc. | Compositions and methods for treating heart failure |
| PL3638243T3 (en) | 2017-06-14 | 2025-02-10 | Celgene Corporation | TREATMENT METHODS FOR MYELOFIBROSIS ASSOCIATED WITH MYELOPROLIFERATIVE NEOPLASIA AND ANEMIA |
| IL320014A (en) | 2018-01-12 | 2025-06-01 | Keros Therapeutics Inc | Activin receptor type IIB variants and methods of using them |
| US12303498B2 (en) | 2018-03-23 | 2025-05-20 | Cytoo | ALK5 inhibitors as skeletal muscle hypertrophy inducers |
| KR20250133994A (en) | 2018-05-09 | 2025-09-09 | 케로스 테라퓨틱스, 인크. | Activin receptor type iia variants and methods of use thereof |
| JP2021532191A (en) | 2018-07-25 | 2021-11-25 | ベーリンガー インゲルハイム インターナショナル ゲゼルシャフト ミット ベシュレンクテル ハフツング | Empagliflozin for use in the treatment of Alport syndrome |
| US20220372135A1 (en) | 2019-09-27 | 2022-11-24 | Disc Medicine, Inc. | Methods for treating myelofibrosis and related conditions |
| AU2021236249A1 (en) | 2020-03-13 | 2022-10-06 | Acceleron Pharma Inc. | Single-arm ActRIIA and ActRIIB heteromultimers and methods for treating renal diseases or conditions |
| WO2021189006A1 (en) | 2020-03-20 | 2021-09-23 | Keros Therapeutics, Inc. | Methods of using activin receptor type iia variants |
| WO2021189010A1 (en) | 2020-03-20 | 2021-09-23 | Keros Therapeutics, Inc. | Methods of using activin receptor type iib variants |
| US20230174620A1 (en) | 2020-04-28 | 2023-06-08 | Acceleron Pharma Inc. | Actrii proteins and use in treating post-capillary pulmonary hypertension |
| JP7854402B2 (en) | 2020-06-23 | 2026-05-01 | アクセルロン ファーマ インコーポレイテッド | ACTRI II protein for the treatment of pulmonary arterial hypertension (PAH) |
| CA3193654A1 (en) | 2020-10-02 | 2022-04-07 | Jasbir S. Seehra | Methods of using activin receptor type ii variants |
| WO2022099166A1 (en) | 2020-11-09 | 2022-05-12 | Keros Therapeutics, Inc. | Methods of treating cardiovascular-related disease |
| WO2022235620A1 (en) | 2021-05-04 | 2022-11-10 | Keros Therapeutics, Inc. | Activin receptor type ii chimeras and methods of use thereof |
| WO2022271716A2 (en) | 2021-06-21 | 2022-12-29 | Keros Therapeutics, Inc. | Methods of using activin receptor type ii signaling inhibitors |
| PE20240777A1 (en) | 2021-07-19 | 2024-04-17 | Acceleron Pharma Inc | ACTRII PROTEINS AND USES THEREOF |
| KR20240051971A (en) | 2021-08-19 | 2024-04-22 | 케로스 테라퓨틱스, 인크. | Method using activin receptor type II signaling inhibitor |
| KR20240099142A (en) | 2021-08-27 | 2024-06-28 | 버사니스 바이오, 인크. | combination therapy |
| US11945856B2 (en) | 2022-01-28 | 2024-04-02 | 35Pharma Inc. | Activin receptor type IIB variants and uses thereof |
| WO2024054985A2 (en) | 2022-09-09 | 2024-03-14 | Keros Therapeutics, Inc. | Methods of administering an activin type iib variant |
| WO2024102906A2 (en) | 2022-11-10 | 2024-05-16 | Keros Therapeutics, Inc. | Activin receptor type ii chimeras and methods of use thereof |
| IL321591A (en) | 2022-12-22 | 2025-08-01 | 35Pharma Inc | Activin receptor type iib variants and uses thereof |
| WO2024238950A1 (en) | 2023-05-18 | 2024-11-21 | Keros Therapeutics, Inc. | Methods of using activin receptor type ii variants |
| WO2024238920A1 (en) | 2023-05-18 | 2024-11-21 | Keros Therapeutics, Inc. | Methods of using activin receptor type ii variants |
| CN121729426A (en) | 2023-07-26 | 2026-03-24 | 35制药有限公司 | Activin type IIB receptor variants and uses thereof |
| WO2025122830A1 (en) | 2023-12-08 | 2025-06-12 | Keros Therapeutics, Inc. | Methods of using activin receptor type ii signaling inhibitors |
| WO2025147483A1 (en) | 2024-01-02 | 2025-07-10 | Keros Therapeutics, Inc. | Methods of using activin receptor type ii chimeras |
-
2021
- 2021-03-19 WO PCT/US2021/023353 patent/WO2021189019A1/en not_active Ceased
- 2021-03-19 CN CN202180036856.2A patent/CN115768457A/en active Pending
- 2021-03-19 IL IL296394A patent/IL296394A/en unknown
- 2021-03-19 KR KR1020227036350A patent/KR20230004515A/en active Pending
- 2021-03-19 AU AU2021237730A patent/AU2021237730A1/en active Pending
- 2021-03-19 JP JP2022556076A patent/JP2023518260A/en active Pending
- 2021-03-19 EP EP21770547.4A patent/EP4121078A4/en active Pending
- 2021-03-19 CA CA3176735A patent/CA3176735A1/en active Pending
-
2022
- 2022-09-15 US US17/945,299 patent/US12522646B2/en active Active
-
2025
- 2025-08-06 JP JP2025131256A patent/JP2025179059A/en active Pending
- 2025-12-10 US US19/415,215 patent/US20260098078A1/en active Pending
Patent Citations (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20180148491A1 (en) * | 2015-04-22 | 2018-05-31 | Alivegen Usa, Inc. | Novel Hybrid ActRIIB Ligand Trap Proteins For Treating Muscle Wasting Diseases |
| US20180161426A1 (en) * | 2015-05-20 | 2018-06-14 | Maria CAPPELLINI | In vitro cell culture methods for beta-thalassemia using activin type ii receptor ligand traps |
| US20190330307A1 (en) * | 2016-10-20 | 2019-10-31 | Biogen Ma Inc. | Methods for treating muscle wasting and bone disease using novel hybrid actriib ligand trap proteins |
| US20190345225A1 (en) * | 2016-11-10 | 2019-11-14 | Keros Therapeutics, Inc. | Activin receptor type iia variants and methods of use thereof |
| WO2019094751A1 (en) * | 2017-11-09 | 2019-05-16 | Keros Therapeutics, Inc. | Activin receptor type iia variants and methods of use thereof |
Non-Patent Citations (1)
| Title |
|---|
| See also references of EP4121078A4 * |
Cited By (14)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US12350313B2 (en) | 2016-11-10 | 2025-07-08 | Keros Therapeutics, Inc. | Activin receptor type IIa variants and methods of use thereof |
| US11717558B2 (en) | 2016-11-10 | 2023-08-08 | Keros Therapeutics, Inc. | Nucleic acid molecules encoding activin receptor type IIA variants |
| US12582700B2 (en) | 2016-11-10 | 2026-03-24 | Keros Therapeutics, Inc. | Activin receptor type IIA variants and methods of use thereof |
| US11484573B2 (en) | 2017-11-09 | 2022-11-01 | Keros Therapeutics, Inc. | Activin receptor type IIa variants and methods of use thereof |
| US11884715B2 (en) | 2018-01-12 | 2024-01-30 | Keros Therapeutics, Inc. | Activin receptor type IIB variants and methods of use thereof |
| US12269858B2 (en) | 2018-01-12 | 2025-04-08 | Keros Therapeutics, Inc. | Activin receptor type IIB variants and methods of use thereof |
| US12364737B2 (en) | 2018-05-09 | 2025-07-22 | Keros Therapeutics, Inc. | Activin receptor type IIA variants and methods of use thereof |
| US12440539B2 (en) | 2020-03-20 | 2025-10-14 | Keros Therapeutics, Inc. | Methods of using activin receptor type IIB variants |
| US11945856B2 (en) | 2022-01-28 | 2024-04-02 | 35Pharma Inc. | Activin receptor type IIB variants and uses thereof |
| US12421296B2 (en) | 2022-01-28 | 2025-09-23 | 35Pharma Inc. | Activin receptor type IIB variants and uses thereof |
| WO2024238950A1 (en) * | 2023-05-18 | 2024-11-21 | Keros Therapeutics, Inc. | Methods of using activin receptor type ii variants |
| WO2025039072A1 (en) * | 2023-08-18 | 2025-02-27 | 35Pharma Inc. | Activin receptor type iib variants and uses thereof |
| WO2025050218A1 (en) * | 2023-09-08 | 2025-03-13 | 35Pharma Inc. | Combination therapy with actriib receptor variants and glp-1 agonists |
| EP4653010A1 (en) | 2024-05-14 | 2025-11-26 | 35Pharma Inc. | Activin receptor type iib traps for use in improving body composition |
Also Published As
| Publication number | Publication date |
|---|---|
| US20230079602A1 (en) | 2023-03-16 |
| JP2025179059A (en) | 2025-12-09 |
| EP4121078A4 (en) | 2024-08-14 |
| AU2021237730A1 (en) | 2022-10-06 |
| US12522646B2 (en) | 2026-01-13 |
| JP2023518260A (en) | 2023-04-28 |
| US20260098078A1 (en) | 2026-04-09 |
| IL296394A (en) | 2022-11-01 |
| CA3176735A1 (en) | 2021-09-23 |
| KR20230004515A (en) | 2023-01-06 |
| EP4121078A1 (en) | 2023-01-25 |
| CN115768457A (en) | 2023-03-07 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US12522646B2 (en) | Activin receptor type II chimeras and methods of use thereof | |
| US12440539B2 (en) | Methods of using activin receptor type IIB variants | |
| US12269858B2 (en) | Activin receptor type IIB variants and methods of use thereof | |
| US20250270287A1 (en) | Activin receptor type ii chimeras and methods of use thereof | |
| WO2022235620A1 (en) | Activin receptor type ii chimeras and methods of use thereof | |
| US20230265162A1 (en) | Methods of using activin receptor type iia variants | |
| US12331124B2 (en) | ALK2 antibodies and methods of use thereof | |
| US20250188148A1 (en) | Methods of administering an activin receptor type iib variant | |
| HK40089125A (en) | Activin receptor type ii chimeras and methods of use thereof | |
| HK40127518A (en) | Activin receptor type iib variants and methods of use thereof |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 21770547 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 2022556076 Country of ref document: JP Kind code of ref document: A Ref document number: 3176735 Country of ref document: CA |
|
| ENP | Entry into the national phase |
Ref document number: 2021237730 Country of ref document: AU Date of ref document: 20210319 Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2021770547 Country of ref document: EP |
|
| ENP | Entry into the national phase |
Ref document number: 2021770547 Country of ref document: EP Effective date: 20221020 |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| WWD | Wipo information: divisional of initial pct application |
Ref document number: 831006 Country of ref document: NZ |