COMPOSITIONS AND METHODS FOR TREATING SPINAL CORD INJURIES BACKGROUND [0001] Spinal cord injury (SCI) is a devastating and currently untreatable condition, aside from symptomatic treatments for some of the resulting complications. Spinal cord injury results in complete or partial loss of motor, sensory, and autonomic function. As a result, patients often lose mobility and may be wheelchair-bound, in addition to suffering numerous medical complications. Over 12,000 Americans suffer a spinal cord injury (SCI) each year, and approximately 1.3 million people in the United States are estimated to be living with a spinal cord injury. Traumatic SCI most commonly impacts individuals in their twenties and thirties, resulting in a high-level of permanent disability in young and previously healthy individuals. Individuals with SCI not only have impaired limb function, but suffer from impaired bowel and bladder function, reduced sensation, spasticity, autonomic dysreflexia, thromboses, sexual dysfunction, increased infections, decubitus ulcers and chronic pain, which can each significantly impact quality of life, and can even be life threatening in some instances. The life expectancy of an individual suffering a cervical spinal cord injury at age 20 is 20-25 years lower than that of a similarly aged individual with no SCI (NSCISC Spinal Cord Injury Facts and Figures 2013).To date, there are no treatments approved by the United States Food and Drug Administration (FDA) to induce neurological recovery following spinal cord injury (SCI). Several interventions including glucocorticoids, modulation of voltage-gated channels, tetracycline antibiotics, and cell-based therapies have been studied in clinical trials, however, none to date have met critical registration endpoints. [0002] The clinical effects of spinal cord injury vary with the site and extent of damage. The neural systems that may be permanently disrupted below the level of the injury not only involve loss of control of limb muscles and the protective roles of temperature and pain sensation, but impact the cardiovascular system, breathing, sweating, bowel control, bladder control, and sexual function (Anderson KD, Friden J, Lieber RL. Acceptable benefits and risks associated with surgically improving arm function in individuals living with cervical spinal cord injury. Spinal Cord.2009 Apr;47(4):334-8.) These losses lead to a succession of secondary problems, such as pressure sores and urinary tract infections that, until modern medicine, were rapidly fatal. Spinal cord injury often removes those unconscious control mechanisms that maintain the appropriate level of excitability in neural circuitry of the spinal
cord. As a result, spinal motoneurons can become spontaneously hyperactive, producing debilitating stiffness and uncontrolled muscle spasms or spasticity. This hyperactivity can also cause sensory systems to produce chronic neurogenic pain and paresthesias, unpleasant sensations including numbness, tingling, aches, and burning. In recent polls of spinal cord injury patients, recovery of ambulatory function was not the highest ranked function that these patients desired to regain, but in many cases, relief from the spontaneous hyperactivity sequelae was paramount (Anderson KD, Friden J, Lieber RL. Acceptable benefits and risks associated with surgically improving arm function in individuals living with cervical spinal cord injury. Spinal Cord.2009 Apr;47(4):334-38). [0003] There exists a need for treatments for spinal cord injury, and related pathologies. SUMMARY [0004] The examples and embodiments presented herein describe human embryonic stem cell (hESC) derived cells for the treatment of spinal cord injuries (SCI) as described in greater detail herein. [0005] For example, an OPC composition obtained in accordance with the present disclosure can be used in cellular therapy to improve one or more neurological functions in a subject in need of treatment. In an embodiment, an OPC cell population in accordance with the present disclosure can be injected, implanted, or otherwise delivered into a subject in need thereof. In an embodiment, a cell population in accordance with the present disclosure can be implanted or otherwise delivered into a subject in need thereof for treating spinal cord injury, stroke, or multiple sclerosis. [0006] The LCTOPC1 is a cell population containing a mixture of oligodendrocyte progenitor cells and other characterized cell types obtained following directed differentiation of an established and well-characterized line of hESC. AST-OPC1 (formerly known as GRNOPC1) is a cell population that contains a mixture of oligodendrocyte progenitor cells (OPCs) and other characterized cell types that are obtained following differentiation of undifferentiated human embryonic stem cells (uhESCs). Oligodendrocyte progenitor cells (OPCs) are a subtype of glial cells in the central nervous system (CNS) that arise in the ventricular zones of the brain and spinal cord and migrate throughout the developing CNS before maturing into oligodendrocytes. Mature oligodendrocytes produce the myelin sheath that insulates neuronal axons and remyelinate CNS
lesions where the myelin sheath has been lost. Oligodendrocytes also contribute to neuroprotection through other mechanisms, including production of neurotrophic factors that promote neuronal survival (Wilkins et al., 2001 Glia 36(1):48-57; Dai et al., 2003 J Neurosci.23(13):5846-53; Du and Dreyfus, 2002 J Neurosci Res. 68(6):647-54). Unlike most progenitor cells, OPCs remain abundant in the adult CNS where they retain the ability to generate new oligodendrocytes. Accordingly, OPCs and mature oligodendrocytes derived from OPCs are an important therapeutic target for demyelinating and dysmyelinating disorders (such as multiple sclerosis, adrenoleukodystrophy and adrenomyeloneuropathy), other neurodegenerative disorders (such as Alzheimer's disease, amyotrophic lateral sclerosis, and Huntington's disease) and acute neurological injuries (such as stroke and spinal cord injury (SCI)). [0007] An OPC composition obtained in accordance with the present disclosure can be used in cellular therapy to improve one or more neurological functions in a subject in need of treatment. In an embodiment, an OPC cell population in accordance with the present disclosure can be injected or implanted into a subject in need thereof. In an embodiment, a cell population in accordance with the present disclosure can be implanted into a subject in need thereof for treating spinal cord injury, stroke, or multiple sclerosis. [0008] In certain embodiments, the OPC1 composition is administered after the subject has suffered a traumatic spinal cord injury. In some embodiments, the OPC1 composition is administered between 14-90 days after the spinal cord injury, such as between 14-75 days after the spinal cord injury, such as between 14-60 days after the spinal cord injury, such as between 14-30 days after the injury, such as between 20-75 days after the injury, such as between 20-60 days after the injury, and such as between 20-40 days after the injury. In certain embodiments, the OPC1 composition is administered about 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 5,, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89 or 90 days after the injury. In certain embodiments, the OPC1 composition is administered between 14 days and the lifetime of the subject. [0009] Methods and compositions for obtaining a population of cells comprising dorsal neural progenitor cells (dNPCs) from undifferentiated human pluripotent stem cells can be found in WO/2020/154533, WO/2020/061371, U.S. Patent No.10, 286,009, WO/2017/031092, WO/2017/173064 and WO/2018/053210, each of which are incorporated by reference in their
entirety for all methods, compositions, cells, data, definitions, uses, and all other information provided therein. [0010] In an aspect, a method of improving one or more neurological functions in a subject having a spinal cord injury (SCI) is provided, the method including: administering to the subject a first dose of a composition including human pluripotent stem cell-derived oligodendrocyte progenitor cells (OPCs); and optionally administering two or more doses of the composition. [0011] In some embodiments, the method further includes administering to the subject a second dose of the composition. In some embodiments, the method further includes administering to the subject a third dose of the composition. In some embodiments, each administration includes delivering, for example by injection, the composition into the spinal cord of the subject. In some embodiments, each administration includes delivering two or more fractions of a dose. In some embodiments, the SCI is a subacute cervical SCI. In some embodiments, the SCI is a chronic cervical SCI. In some embodiments, the SCI is a subacute thoracic SCI. In some embodiments, the SCI is a chronic thoracic SCI. In some embodiments, the first dose, second dose, and/or third dose of the composition includes about 1 x 10
6 to about 3x10
7 OPC cells. In some embodiments, the first dose of the composition includes about 2 x 10
6 OPC cells. In some embodiments, the first dose or the second dose of the composition includes about 1 x 10
7 OPC cells. In some embodiments, the second dose or the third dose of the composition includes about 2 x 10
7 OPC cells. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 20 to about 45 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 14 to about 90 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 14 to about 75 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 14 to about 60 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 14 to about 30 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 20 to about 75 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 20 to about 60 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 20
to about 40 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered between about 14 days after the SCI and the lifetime of the subject. In some embodiments, the injection is performed in a caudal half of an epicenter of the SCI. In some embodiments, the injection is about 6 mm into the spinal cord of the subject. In some embodiments, the injection is about 5 mm into the spinal cord of the subject. [0012] In another, aspect, a method of improving one or more neurological functions in a subject having a spinal cord injury (SCI) is provided, the method including: administering to the subject a dose of a composition including human pluripotent stem cell-derived oligodendrocyte progenitor cells (OPCs). [0013] In some embodiments, the dose of the composition includes about 1 x 10
6 to about 3 x 10
7 OPC cells. In some embodiments, the dose of the composition includes about 2 x 10
6 OPC cells. In some embodiments, the administration of the composition includes injecting, implanting, or otherwise delivering the composition into the spinal cord of the subject. In some embodiments, the dose of the composition is administered about 7 to about 14 days after the SCI. In some embodiments, the injection is performed in a caudal half of an epicenter of the SCI. In some embodiments, the injection is about 6 mm into the spinal cord of the subject. In some embodiments, the injection is about 5 mm into the spinal cord of the subject. In some embodiments, the SCI is a subacute thoracic SCI. In some embodiments, the SCI is a chronic thoracic SCI. In some embodiments, the SCI is a subacute cervical SCI. In some embodiments, the SCI is a chronic cervical SCI. In some embodiments, improving one or more neurological functions includes an improvement in ISNCSCI exam upper extremity motor score (UEMS). In some embodiments, the improvement in UEMS occurs within about 6 months, about 12 months, about 18 months, about 24 months or more after injection. In some embodiments, the improvement is an increase in UEMS of at least 10%, compared to baseline. In some embodiments, improving one or more neurological functions includes an improvement in lower extremity motor scores (LEMS). In some embodiments, the improvement in LEMS occurs within about 6 months, about 12 months, about 18 months, about 24 months or more after injection. In some embodiments, the improvement is at least one motor level improvement. In some embodiments, the improvement is at least two motor level improvement. In some embodiments, the improvement is on one side of the subject’s body. In some embodiments, the improvement is on both sides of the subject’s body. In some embodiments, the dose of the composition is
administered about 14 to 90 days after the SCI. In some embodiments, the dose of the composition is administered about 14 to about 75 days after the SCI. In some embodiments, the dose of the composition is administered about 14 to about 60 days after the SCI. In some embodiments, the dose of the composition is administered about 14 to about 30 days after the SCI. In some embodiments, the dose of the composition is administered about 20 to about 75 days after the SCI. In some embodiments, the dose of the composition is administered about 20 to about 60 days after the SCI. In some embodiments, the dose of the composition is administered about 20 to about 40 days after the SCI. In some embodiments, the dose of the composition is administered between about 14 days after the SCI and the lifetime of the subject. [0014] In another, aspect, a cell population is provided, the cell population including an increased proportion of cells positive for oligodendrocyte progenitor cell marker NG2 and reduced expression of non-OPC markers CD49f, CLDN6, and EpCAM, wherein the cell population is prepared according to the following method: culturing undifferentiated human embryonic stem cells (uhESC) in Glial Progenitor Medium including a MAPK/ERK inhibitor, a BMP signaling inhibitor, and Retinoic Acid to obtain glial-restricted cells; differentiating the glial-restricted cells into oligodendrocyte progenitor cells (OPCs) having an increased proportion of cells positive for oligodendrocyte progenitor cell marker NG2 and reduced expression of non- OPC markers CD49f, CLDN6, and EpCAM. [0015] In some embodiments, the cell population is used in treating a thoracic spinal cord injury (SCI) in a subject. In some embodiments, the thoracic SCI is a subacute thoracic SCI. In some embodiments, the thoracic SCI is a chronic thoracic SCI. In some embodiments, the cell population is used in treating a cervical spinal cord injury (SCI) in a subject. In some embodiments, the cervical SCI is a subacute cervical SCI. In some embodiments, the cervical SCI is a chronic cervical SCI. In some embodiments, the composition is administered by implantation or other delivery method. In some embodiments, the composition is administered via injection to the subject after the SCI. In some embodiments, the injection is performed in a caudal half of an epicenter of the SCI. In some embodiments, the injection is about 6 mm into the spinal cord of the subject. In some embodiments, the injection is about 5 mm into the spinal cord of the subject. In some embodiments, the injection is performed about 14 to about 90 days after the SCI. In some embodiments, the injection is performed about 14 to about 75 days after the SCI. In some embodiments, the injection is performed about 14 to about 60 days after the SCI. In
some embodiments, the injection is performed about 14 to about 30 days after the SCI. In some embodiments, the injection is performed about 20 to about 75 days after the SCI. In some embodiments, the injection is performed about 20 to about 60 days after the SCI. In some embodiments, the injection is performed about 20 to about 40 days after the SCI. In some embodiments, the injection is performed between about 14 days after the SCI and the lifetime of the subject. [0016] In another, aspect, a method of improving one or more neurological functions in a subject having a spinal cord injury (SCI) is provided, the method including: administering to the subject a first dose of the cell population of claim 54; administering to the subject a second dose of the cell population; and optionally administering to the subject a third dose of the cell population. [0017] In some embodiments, the SCI is a subacute cervical SCI. In some embodiments, the SCI is a chronic cervical SCI. In some embodiments, the SCI is a subacute thoracic SCI. In some embodiments, the SCI is a chronic thoracic SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 14 to about 90 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 14 to about 75 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 14 to about 60 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 14 to about 30 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 20 to about 75 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 20 to about 60 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered about 20 to about 40 days after the SCI. In some embodiments, each of the first dose, second dose, and third dose of the composition are administered between about 14 days after the SCI and the lifetime of the subject. BRIEF DESCRIPTION OF THE DRAWINGS [0018] Embodiments will now be described, by way of example only, with reference to the accompanying drawings, in which:
[0019] FIG.1 is a Phase-1 clinical trial schematic timeline. [0020] FIG.2 is schematic for patient screening, treatment, and follow-up during a Phase-1 clinical trial (CONSORT flow diagram). [0021] FIG.3 is a diagram illustrating the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) screening and at 5-year follow-up (* one ISNSCI performed at 4-year). In the figure green denotes normal motor and/or sensation, red absent motor and/or sensation, orange and light red represent sensation that is present but abnormal. [0022] FIG.4 is an example questionnaire administered for the long-term protocol, annual visits were required in years 2-5. Subsequent to the year 5 annual visit, follow-up was by annual phone questionnaires. [0023] FIG.5 is a study schematic of subjects. [0024] FIG.6 is a clinical trial schematic timeline. [0025] FIG.7 is a schematic for patient screening and treatment during a clinical trial. [0026] FIG.8 is a schematic of the cohort structure and enrollment progression of a clinical trial consistent with the implementations of the present disclosure. [0027] FIG.9 is another Phase-1 clinical trial schematic timeline consistent with implementations of the present disclosure. [0028] FIG.10 is an overview of two example cell manufacturing processes consistent with implementations of the present disclosure. [0029] FIG.11 is a flow chart of a signaling sequence schematic of a cell differentiation process consistent with implementations of the present disclosure. [0030] FIG.12 is a flowchart of a production process flow consistent with implementations of the present disclosure. DETAILED DESCRIPTION [0031] Before the present compositions and methods are described, it is to be understood that the present disclosure is not limited to the particular processes, compositions, or methodologies described, as these may vary. It is also to be understood that the terminology used in the description is for the purpose of describing the particular versions or embodiments only, and is not intended to limit the scope of the present invention which will be limited only
by the appended claims For example, features illustrated with respect to one embodiment may be incorporated into other embodiments, and features illustrated with respect to a particular embodiment may be deleted from that embodiment. Thus, the disclosure contemplates that in some embodiments of the disclosure, any feature or combination of features set forth herein can be excluded or omitted. In addition, numerous variations and additions to the various embodiments suggested herein will be apparent to those skilled in the art in light of the instant disclosure, which do not depart from the instant disclosure. In other instances, well- known structures, interfaces, and processes have not been shown in detail in order not to unnecessarily obscure the invention. It is intended that no part of this specification be construed to effect a disavowal of any part of the full scope of the invention. Hence, the following descriptions are intended to illustrate some particular aspects of the disclosure, and not to exhaustively specify all permutations, combinations and variations thereof. [0032] Unless otherwise defined, all technical and scientific terms used herein have the same meaning as commonly understood by one of ordinary skill in the art to which this disclosure belongs. The terminology used in the description of the disclosure herein is for the purpose of describing particular embodiments only and is not intended to be limiting of the disclosure. [0033] All publications, patent applications, patents and other references cited herein are incorporated by reference in their entireties. [0034] Unless the context indicates otherwise, it is specifically intended that the various features of the disclosure described herein can be used in any combination. Moreover, the present disclosure also contemplates that in some embodiments of the disclosure, any feature or combination of features set forth herein can be excluded or omitted. [0035] Methods disclosed herein can comprise one or more steps or actions for achieving the described method. The method steps and/or actions may be interchanged with one another without departing from the scope of the present invention. In other words, unless a specific order of steps or actions is required for proper operation of the embodiment, the order and/or use of specific steps and/or actions may be modified without departing from the scope of the present invention.
[0036] As used in the description of the disclosure and the appended claims, the singular forms "a," "an" and "the" are intended to include the plural forms as well, unless the context clearly indicates otherwise. [0037] As used herein, "and/or" refers to and encompasses any and all possible combinations of one or more of the associated listed items, as well as the lack of combinations when interpreted in the alternative ("or"). [0038] The terms "about" and "approximately" as used herein when referring to a measurable value such as a percentages, density, volume and the like, is meant to encompass variations of ± 20%, ± 10%, ± 5%, ± 1%, ± 0.5%, or even ± 0.1% of the specified amount. [0039] As used herein, phrases such as "between X and Y" and "between about X and Y" should be interpreted to include X and Y. As used herein, phrases such as "between about X and Y" mean "between about X and about Y" and phrases such as "from about X to Y" mean "from about X to about Y." [0040] The term "AST-OPC1" refers to a specific, characterized, in vitro differentiated cell population containing a mixture of oligodendrocyte progenitor cells (OPCs) and other characterized cell types obtained from undifferentiated human embryonic stem cells (uhESCs) according to specific differentiation protocols disclosed herein. [0041] Compositional analysis of AST-OPC1 by immunocytochemistry (ICC), flow cytometry, and quantitative polymerase chain reaction (qPCR) demonstrates that the cell population is comprised primarily of neural lineage cells of the oligodendrocyte phenotype. Other neural lineage cells, namely astrocytes and neurons, are present at low frequencies. The only non-neural cells detected in the population are epithelial cells. Mesodermal, endodermal lineage cells and uhESCs are routinely below quantitation or detection of the assays. [0042] The term "oligodendrocyte progenitor cells" (OPCs), as used herein, refers to cells of neuroectoderm/glial lineage having the characteristics of a cell type found in the central nervous system, capable of differentiating into oligodendrocytes. These cells typically express the characteristic markers Nestin, NG2 and PDGF-Ra. [0043] The terms "treatment," "treat" "treated," or "treating," as used herein, can refer to both therapeutic treatment or prophylactic or preventative measures, wherein the object is to prevent or slow down (lessen) an undesired physiological condition, symptom, disorder or
disease, or to obtain beneficial or desired clinical results. In some embodiments, the term may refer to both treating and preventing. For the purposes of this disclosure, beneficial or desired clinical results may include, but are not limited to one or more of the following: alleviation of symptoms; diminishment of the extent of the condition, disorder or disease; stabilization (i.e., not worsening) of the state of the condition, disorder or disease; delay in onset or slowing of the progression of the condition, disorder or disease; amelioration of the condition, disorder or disease state; and remission (whether partial or total), whether detectable or undetectable, or enhancement or improvement of the condition, disorder or disease. Treatment includes eliciting a clinically significant response. Treatment also includes prolonging survival as compared to expected survival if not receiving treatment. [0044] The term "subject," as used herein includes, but is not limited to, humans, nonhuman primates and non-human vertebrates such as wild, domestic and farm animals including any mammal, such as cats, dogs, cows, sheep, pigs, horses, rabbits, rodents such as mice and rats. In some embodiments, the term "subject," refers to a male. In some embodiments, the term "subject," refers to a female. [0045] As used herein, "implantation" or "transplantation" refers to the administration of a cell population into a target tissue using a suitable delivery technique, (e.g., using an injection device, implantation device, or other delivery device). [0046] As used herein, "engraftment" and "engrafting" refer to incorporation of implanted tissue or cells (i.e. "graft tissue" or "graft cells") into the body of a subject. The presence of graft tissue or graft cells at or near the implantation site 180 days or later, post implantation, is indicative of engraftment. In certain embodiments, imaging techniques (such as, e.g. MRI imaging), can be used to detect the presence of graft tissue. [0047] As used herein, "allogeneic" and "allogeneically derived" refer to cell populations derived from a source other than the subject and hence genetically non-identical to the subject. In certain embodiments, allogeneic cell populations are derived from cultured pluripotent stem cells. In certain embodiments, allogeneic cell populations are derived from hESCs. In other embodiments, allogeneic cell populations are derived from induced pluripotent stem (iPS) cells. In yet other embodiments, allogeneic cell populations are derived from primate pluripotent (pPS) cells.
[0048] As used herein, "parenchymal cavitation" refers to formation of a lesion or cavity within a CNS injury site or proximate to a CNS injury site, in an area normally occupied by parenchymal CNS tissue. The cavities or lesions can be filled with extracellular fluid and may contain macrophages, small bands of connective tissue and blood vessels. [0049] The terms "central nervous system" and "CNS" as used interchangeably herein refer to the complex of nerve tissues that control one or more activities of the body, which include but are not limited to, the brain and the spinal cord in vertebrates. [0050] The term ‘decorin’ as used herein refers to a proteoglycan that, in humans, is encoded by the DCN gene. Decorin is a small cellular or pericellular matrix proteoglycan, and the protein is a component of connective tissue, binds to type I collagen fibrils, and plays a role in matrix assembly. [0051] The term ‘chronic’ as used herein includes, but is not intended to be limited to, a condition occurring in a subject over a time period occurring between 90 days after an injury and the lifetime of a subject. [0052] The term ‘subacute’ as used herein includes, but is not intended to be limited to, a condition occurring in a subject over a time period of between 14 days and 90 days after an injury. [0053] There are multiple pathologies observed in the injured spinal cord due to the injury itself and subsequent secondary effects due to edema, hemorrhage and inflammation (Kakulas BA. The applied neuropathology of human spinal cord injury. Spinal Cord.1999 Feb;37(2):79-88). These pathologies include the severing of axons, demyelination, parenchymal cavitation and the production of ectopic tissue such as fibrous scar tissue, gliosis, and dystrophic calcification (Anderson DK, Hall ED. Pathophysiology of spinal cord trauma. Ann Emerg Med.1993 Jun;22(6):987-92; Norenberg MD, Smith J, Marcillo A. The pathology of human spinal cord injury: defining the problems. J. Neurotrauma.2004 Apr;21(4):429-40). Oligodendrocytes, which provide both neurotrophic factor and myelination support for axons are susceptible to cell death following SCI and therefore are an important therapeutic target (Almad A, Sahinkaya FR, Mctigue DM. Oligodendrocyte fate after spinal cord injury. Neurotherapics 20118(2): 262-73). Replacement of the oligodendrocyte population could both support the remaining and damaged axons and also remyelinate axons to promote electrical conduction (Cao Q, He Q, Wang Yet et al.
Transplantation of ciliary neurotrophic factor-expressing adult oligodendrocyte precursor cells promotes remyelination and functional recovery after spinal cord injury. J. Neurosci. 201030(8): 2989-3001). Oligodendrocyte progenitor cells (OPCs) are a subtype of glial cells in the central nervous system (CNS) that arise in the ventricular zones of the brain and spinal cord and migrate throughout the developing CNS before maturing into oligodendrocytes. Mature oligodendrocytes produce the myelin sheath that insulates neuronal axons and remyelinate CNS lesions where the myelin sheath has been lost. Oligodendrocytes also contribute to neuroprotection through other mechanisms, including production of neurotrophic factors that promote neuronal survival (Wilkins et al., 2001 Glia 36(1):48-57; Dai et al., 2003 J Neurosci.23(13):5846-53; Du and Dreyfus, 2002 J Neurosci Res.68(6):647-54). Additionally, OPCs are known to produce Decorin, a secreted factor which has been shown to suppress CNS scarring (Esmaeili, Berry et al, 2014, Gubbiotti, Vallet et al.2016). Unlike most progenitor cells, OPCs remain abundant in the adult CNS where they retain the ability to generate new oligodendrocytes. Accordingly, OPCs and mature oligodendrocytes derived from OPCs are an important therapeutic target for demyelinating and dysmyelinating disorders (such as multiple sclerosis, adrenoleukodystrophy and adrenomyeloneuropathy), other neurodegenerative disorders (such as Alzheimer’s disease, amyotrophic lateral sclerosis, and Huntington’s disease) and acute neurological injuries (such as stroke and spinal cord injury (SCI)). Propagation and Culture of Undifferentiated Pluripotent Stem Cells [0054] In certain embodiments, the present disclosure provides methods to produce large numbers of highly pure, characterized oligodendrocyte progenitor cells from pluripotent stem cells. Derivation of oligodendrocyte progenitor cells (OPCs) from pluripotent stem cells according to the methods of the invention provides a renewable and scalable source of OPCs for a number of important therapeutic, research, development, and commercial purposes, including treatment of acute spinal cord injury. [0055] Methods of propagation and culture of undifferentiated pluripotent stem cells have been previously described. With respect to tissue and cell culture of pluripotent stem cells, the reader may wish to refer to any of numerous publications available in the art, e.g., Teratocarcinomas and Embryonic Stem cells: A Practical Approach (E. J. Robertson, Ed.,
IRL Press Ltd.1987); Guide to Techniques in Mouse Development (P. M. Wasserman et al., Eds., Academic Press 1993); Embryonic Stem Cell Differentiation in Vitro (M. V. Wiles, Meth. Enzymol.225:900, 1993); Properties and Uses of Embryonic Stem Cells: Prospects for Application to Human Biology and Gene Therapy (P. D. Rathjen et al., Reprod. Fertil. Dev.10:31, 1998; and R. I. Freshney, Culture of Animal Cells, Wiley-Liss, New York, 2000). [0056] In certain embodiments, a method can be carried out on a pluripotent stem cell line. In other embodiments, a method can be carried out on an embryonic stem cell line. In an embodiment, a method can be carried out on a plurality of undifferentiated stem cells that are derived from an H1, H7, H9, H13, or H14 cell line. In another embodiment, undifferentiated stem cells can be derived from an induced pluripotent stem cell (iPS) line. In another embodiment, a method can be carried out on a primate pluripotent stem (pPS) cell line. In yet another embodiment, undifferentiated stem cells can be derived from parthenotes, which are embryos stimulated to produce hESCs without fertilization. [0057] In one embodiment, undifferentiated pluripotent stem cells can be maintained in an undifferentiated state without added feeder cells (see, e.g., (2004) Rosler et al., Dev. Dynam. 229:259). Feeder-free cultures are typically supported by a nutrient medium containing factors that promote proliferation of the cells without differentiation (see, e.g., U.S. Pat. No. 6,800,480). In one embodiment, conditioned media containing such factors can be used. Conditioned media can be obtained by culturing the media with cells secreting such factors. Suitable cells include, but are not limited to, irradiated (4,000 Rad) primary mouse embryonic fibroblasts, telomerized mouse fibroblasts, or fibroblast-like cells derived from pPS cells (U.S. Pat. No.6,642,048). Medium can be conditioned by plating the feeders in a serum free medium, such as knock-out DMEM supplemented with 20% serum replacement and 4 ng/mL bFGF. Medium that has been conditioned for 1-2 days can be supplemented with further bFGF, and used to support pPS cell culture for 1-2 days (see. e.g., WO 01/51616; Xu et al., (2001) Nat. Biotechnol.19:971). [0058] Alternatively, fresh or non-conditioned medium can be used, which has been supplemented with added factors (such as, e.g., a fibroblast growth factor or forskolin) that promote proliferation of the cells in an undifferentiated form. Non-limiting examples include a base medium like X-VIVOTM 10 (Lonza, Walkersville, Md.) or QBSFTM-60 (Quality
Biological Inc. Gaithersburg, Md.), supplemented with bFGF at 40-80 ng/mL, and optionally containing SCF (15 ng/mL), or Flt3 ligand (75 ng/mL) (see, e.g., Xu et al., (2005) Stem Cells 23(3):315). These media formulations have the advantage of supporting cell growth at 2-3 times the rate in other systems (see, e.g., WO 03/020920). In one embodiment, undifferentiated pluripotent cells such as hESCs, can be cultured in a media comprising bFGF and TGFP. Non-limiting example concentrations of bFGF include about 80 ng/ml. Non- limiting example concentrations of TGFP include about 0.5 ng/ml. [0059] In one embodiment, undifferentiated pluripotent cells can be cultured on a layer of feeder cells, typically fibroblasts derived from embryonic or fetal tissue (Thomson et al. (1998) Science 282:1145). Feeder cells can be derived, inter alia, from a human or a murine source. Human feeder cells can be isolated from various human tissues, or can be derived via differentiation of human embryonic stem cells into fibroblast cells (see, e.g., WO 01/51616). In one embodiment, human feeder cells that can be used include, but are not limited to, placental fibroblasts (see, e.g., Genbacev et al. (2005) Fertil. Steril.83(5):1517), fallopian tube epithelial cells (see, e.g., Richards et al. (2002) Nat. Biotechnol., 20:933), foreskin fibroblasts (see, e.g., Amit et al. (2003) Biol. Reprod.68:2150), and uterine endometrial cells (see, e.g., Lee et al. (2005) Biol. Reprod.72(1):42). [0060] Various solid surfaces can be used in the culturing of undifferentiated pluripotent cells. Those solid surfaces include, but are not limited to, standard commercially available cell culture plates, such as 6-well, 24-well, 96-well, or 144-well plates. Other solid surfaces include, but are not limited to, microcarriers and disks. Solid surfaces suitable for growing undifferentiated pluripotent cells can be made of a variety of substances including, but not limited to, glass or plastic such as polystyrene, polyvinylchloride, polycarbonate, polytetrafluorethylene, melinex, thermanox, or combinations thereof. In one embodiment, suitable surfaces can comprise one or more polymers, such as, e.g., one or more acrylates. In one embodiment, a solid surface can be three-dimensional in shape. Non-limiting examples of three-dimensional solid surfaces are described, e.g., in U.S. Patent Pub. No. 2005/0031598. [0061] In one embodiment, undifferentiated stem cells can be grown under feeder-free conditions on a growth substrate. In one embodiment, a growth substrate can be Matrigel
® (e.g., Matrigel
® or Matrigel
® GFR), recombinant Laminin, or Vitronectin. In another
embodiment, undifferentiated stem cells can be subcultured using various methods such as using collagenase, or such as manual scraping. In another embodiment, undifferentiated stem cells can be subcultured using non-enzymatic means, such as 0.5 mM EDTA in PBS, or such as using ReLeSR
Tm. In an embodiment, a plurality of undifferentiated stem cells are seeded or subcultured at a seeding density that allows the cells to reach confluence in about three to about ten days. In an embodiment, the seeding density can range from about 6.0 x 10
3 cells/cm
2 to about 5.0 x 10
5 cells/cm
2, such as about 1.0 x 10
4 cells/cm
2, such as about 5.0 x 10
4 cells/cm
2, such as about 1.0 x 10
5 cells/cm
2, or such as about 3.0 x 10
5 cells/cm
2 of growth surface. In another embodiment, the seeding density can range from about 6.0 x 10
3 cells/cm
2 to about 1.0 x 10
4 cells/cm
2 of growth surface, such as about 6.0 x 10
3 cells/cm
2 to about 9.0 x 10
3 cells/cm
2, such as about 7.0 x 10
3 cells/cm
2 to about 1.0 x 10
4 cells/cm
2, such as about 7.0 x 10
3 cells/cm
2 to about 9.0 x 10
3 cells/cm
2, or such as about 7.0 x 10
3 cells/cm
2 to about 8.0 x 10
3 cells/cm
2 of growth surface. In yet another embodiment the seeding density can range from about 1.0 x 10
4 cells/cm
2 to about 1.0 x 10
5 cells/cm
2 of growth surface, such as about 2.0 x 10
4 cells/cm
2 to about 9.0 x 10
4 cells/cm
2, such as about 3.0 x 10
4 cells/cm
2 to about 8.0 x 10
4 cells/cm
2, such as about 4.0 x 10
4 cells/cm
2 to about 7.0 x 10
4 cells/cm
2, or such as about 5.0 x 10
4 cells/cm
2 to about 6.0 x 10
4 cells/cm
2 of growth surface. In an embodiment, the seeding density can range from about 1.0 x 10
5 cells/cm
2 to about 5.0 x 10
5 cells/cm
2 of growth surface, such as about 1.0 x 10
5 cells/cm
2 to about 4.5 x 10
5 cells/cm
2, such as about 1.5 x 10
5 cells/cm
2 to about 4.0 x 10
5 cells/cm
2, such as about 2.0 x 10
5 cells/cm
2 to about 3.5 x 10
5 cells/cm
2, or such as about 2.5 x 10
5 cells/cm
2 to about 3.0 x 10
5 cells/cm
2 of growth surface. [0062] Any of a variety of suitable cell culture and sub-culturing techniques can be used to culture cells in accordance with the present disclosure. For example, in one embodiment, a culture medium can be exchanged at a suitable time interval. In one embodiment, a culture medium can be completely exchanged daily, initiating about 2 days after sub-culturing of the cells. In another embodiment, when a culture reaches about 90% colony coverage, a surrogate flask can be sacrificed and enumerated using one or more suitable reagents, such as, e.g., Collagenase IV and 0.05% Trypsin-EDTA in series to achieve a single cell suspension for quantification. In an embodiment, a plurality undifferentiated stem cells can then be subcultured before seeding the cells on a suitable growth substrate (e.g., Matrigel
® GFR) at a seeding density that allows the cells to reach confluence over a suitable period of
time, such as, e.g., in about three to ten days. In one embodiment, undifferentiated stem cells can be subcultured using Collagenase IV and expanded on a recombinant laminin matrix. In one embodiment, undifferentiated stem cells can be subcultured using Collagenase IV and expanded on a Matrigel
® matrix. In one embodiment, undifferentiated stem cells can be subcultured using ReLeSRTM and expanded on a Vitronectin matrix. [0063] In one embodiment, the seeding density can range from about 6.0 x 10
3 cells/cm
2 to about 5.0 x 10
5 cells/cm
2, such as about 1.0 x 10
4 cells/cm
2, such as about 5.0 x 10
4 cells/cm
2, such as about 1.0 x 10
5 cells/cm
2, or such as about 3.0 x 10
5 cells/cm
2 of growth surface. In another embodiment, the seeding density can range from about 6.0 x 10
3 cells/cm
2 to about 1.0 x 10
4 cells/cm
2 of growth surface, such as about 6.0 x 10
3 cells/cm
2 to about 9.0 x 10
3 cells/cm
2, such as about 7.0 x 10
3 cells/cm
2 to about 1.0 x 10
4 cells/cm
2, such as about 7.0 x 10
3 cells/cm
2 to about 9.0 x 10
3 cells/cm
2, or such as about 7.0 x 10
3 cells/cm
2 to about 8.0 x 10
3 cells/cm
2 of growth surface. In yet another embodiment, the seeding density can range from about 1.0 x 10
4 cells/cm
2 to about 1.0 x 10
5 cells/cm
2 of growth surface, such as about 2.0 x 10
4 cells/cm
2 to about 9.0 x 10
4 cells/cm
2, such as about 3.0 x 10
4 cells/cm
2 to about 8.0 x 10
4 cells/cm
2, such as about 4.0 x 10
4 cells/cm
2 to about 7.0 x 10
4 cells/cm
2, or such as about 5.0 x 10
4 cells/cm
2 to about 6.0 x 10
4 cells/cm
2 of growth surface. In an embodiment, the seeding density can range from about 1.0 x 10
5 cells/cm
2 to about 5.0 x 10
5 cells/cm
2 of growth surface, such as about 1.0 x 10
5 cells/cm
2 to about 4.5 x 10
5 cells/cm
2, such as about 1.5 x 10
5 cells/cm
2 to about 4.0 x 10
5 cells/cm
2, such as about 2.0 x 10
5 cells/cm
2 to about 3.5 x 10
5 cells/cm
2, or such as about 2.5 x 10
5 cells/cm
2 to about 3.0 x 10
5 cells/cm
2 of growth surface. Oligodendrocyte Progenitor Cell Compositions [0064] As discussed above, the present disclosure provides compositions comprising a population of oligodendrocyte progenitor cells (OPCs) as well as methods of making and using the same from use in the treatment of acute spinal cord injury and other related CNS conditions. In certain embodiments, the OPCs of the present disclosure are capable of producing and secreting one or more biological factors that may augment neural repair. [0065] In one embodiment, a cell population can have a common genetic background. In an embodiment, a cell population may be derived from one host. In an embodiment, a cell population can be derived from a pluripotent stem cell line. In another embodiment, a cell population can be derived from an embryonic stem cell line. In an embodiment, a cell
population can be derived from a hESC line. In an embodiment, a hESC line can be an H1, H7, H9, H13, or H14 cell line. In another embodiment, a cell population can be derived from an induced pluripotent stem cell (iPS) line. In an embodiment a cell population can be derived from a subject in need thereof (e.g., a cell population can be derived from a subject that is in need to treatment). In yet another embodiment, a hESC line can be derived from parthenotes, which are embryos stimulated to produce hESCs without fertilization. [0066] In certain embodiments, the OPCs of the present disclosure express one or more markers chosen from Nestin, NG2, Olig 1 and PDGF-Ra. In certain embodiments, the OPCs of the present disclosure express all of the markers Nestin, NG2, Olig 1 and PDGF-Ra. [0067] In certain embodiments, the OPCs of the present disclosure are capable of secreting one or more biological factors. In certain embodiments, the one or more biological factors secreted by the OPCs of the present disclosure may promote, without limitation, neural repair, axonal outgrowth and/or glial differentiation, or any combination thereof. In some embodiments, the OPCs are capable of secreting one or more factors that stimulate axonal outgrowth. In some embodiments, the OPCs are capable of secreting one or more factors promoting glial differentiation by neural precursor cells. In some embodiments, the OPCs are capable of secreting one or more chemoattractants for neural precursor cells. In some embodiments, the OPCs are capable of secreting one or more inhibitors of matrix metalloproteinases. In some embodiments, the OPCs are capable of secreting one or more factors inhibiting cell death after spinal cord injury. In some embodiments, the OPCs are capable of secreting one or more factors that are upregulated post-cellular injury and that aid in the clearance of misfolded proteins. [0068] In certain embodiments, the OPCs are capable of producing and secreting one or more biological factors selected from MCP-1, Clusterin, ApoE, TIMP1 and TIMP2. In further embodiments the OPCs are capable of producing and secreting MCP-1 and one or more of the factors selected from Clusterin, ApoE, TIMP1 and TIMP2. In yet further embodiments, the OPCs are capable of producing and secreting all of the factors MCP-1, Clusterin, ApoE, TIMP1 and TIMP2. [0069] In an embodiment, a biological factor can be secreted by a composition comprising a population of OPCs at a concentration of more than about 50 pg/ml, such as more than about 100 pg/ml, such as more than about 200 pg/ml, such as more than about 300 pg/ml, such as
more than about 400 pg/ml, such as more than about 500 pg/ml, such as more than about 1,000 pg/ml, such as more than about 2,000 pg/ml, such as more than about 3,000 pg/ml, such as more than about 4,000 pg/ml, such as more than about 5,000 pg/ml, such as more than about 6,000 pg/ml, or such as more than about 7,000 pg/ml. In certain embodiments, a biological factor can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 50 pg/ml to about 100,000 pg/ml, such as about 100 pg/ml, such as about 150 pg/ml, such as about 200 pg/ml, such as about 250 pg/ml, such as about 300 pg/ml, such as about 350 pg/ml, such as about 400 pg/ml, such as about 450 pg/ml, such as about 500 pg/ml, such as about 550 pg/ml, such as about 600 pg/ml, such as about 650 pg/ml, such as about 700 pg/ml, such as about 750 pg/ml, such as about 800 pg/ml, such as about 850 pg/ml, such as about 900 pg/ml, such as about 1,000 pg/ml, such as about 1,500 pg/ml, such as about 2,000 pg/ml, such as about 2,500 pg/ml, such as about 3,000 pg/ml, such as about 3,500 pg/ml, such as about 4,000 pg/ml, such as about 4,500 pg/ml, such as about 5,000 pg/ml, such as about 5,500 pg/ml, such as about 6,000 pg/ml, such as about 6,500 pg/ml, such as about 7,000 pg/ml, such as about 7,500 pg/ml, such as about 8,000 pg/ml, such as about 8,500 pg/ml, such as about 9,000 pg/ml, such as about 10,000 pg/ml, such as about 15,000 pg/ml, such as about 20,000 pg/ml, such as about 25,000 pg/ml, such as about 30,000 pg/ml, such as about 35,000 pg/ml, such as about 40,000 pg/ml, such as about 45,000 pg/ml, such as about 50,000 pg/ml, such as about 55,000 pg/ml, such as about 60,000 pg/ml, such as about 65,000 pg/ml, such as about 70,000 pg/ml, such as about 75,000 pg/ml, such as about 80,000 pg/ml, such as about 85,000 pg/ml, such as about 90,000 pg/ml, such as about 95,000 pg/ml. [0070] In certain embodiments, a biological factor can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 1,000 pg/ml to about 10,000 pg/ml, such as about 1,000 pg/ml to about 2,000 pg/ml, such as about 2,000 pg/ml to about 3,000 pg/ml, such as about 3,000 pg/ml to about 4,000 pg/ml, such as about 4,000 pg/ml to about 5,000 pg/ml, such as about 5,000 pg/ml to about 6,000 pg/ml, such as about 6,000 pg/ml to about 7,000 pg/ml, such as about 7,000 pg/ml to about 8,000 pg/ml, such as about 8,000 pg/ml to about 9,000 pg/ml, or such as about 9,000 pg/ml to about 10,000 pg/ml. [0071] In certain embodiments, a biological factor can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about
10,000 pg/ml to about 100,000 pg/ml, such as about 10,000 pg/ml to about 20,000 pg/ml, such as about 20,000 pg/ml to about 30,000 pg/ml, such as about 30,000 pg/ml to about 40,000 pg/ml, such as about 40,000 pg/ml to about 50,000 pg/ml, such as about 50,000 pg/ml to about 60,000 pg/ml, such as about 60,000 pg/ml to about 70,000 pg/ml, such as about 70,000 pg/ml to about 80,000 pg/ml, such as about 80,000 pg/ml to about 90,000 pg/ml, or such as about 90,000 pg/ml to about 100,000 pg/ml. [0072] In some embodiments, Clusterin can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 1,000 pg/ml to about 100,000 pg/ml. In certain embodiments, Clusterin can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 10,000 pg/ml to about 50,000 pg/ml. In some embodiments, MCP-1 can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 500 pg/ml to about 50,000 pg/ml. In certain embodiments, MCP-1 can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 5,000 pg/ml to about 15,000 pg/ml. In some embodiments, ApoE can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 100 pg/ml to about 10,000 pg/ml. In certain embodiments, ApoE can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 500 pg/ml to about 5,000 pg/ml. In some embodiments, TIMP1 can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 100 pg/ml to about 10,000 pg/ml. In certain embodiments, TIMP1 can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 500 pg/ml to about 5,000 pg/ml. In some embodiments, TIMP2 can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 100 pg/ml to about 10,000 pg/ml. In certain embodiments, TIMP2 can be secreted by a composition comprising a population of cells comprising OPCs at a concentration ranging from about 500 pg/ml to about 5,000 pg/ml. Pharmaceutical Compositions [0073] The OPCs of the present disclosure can be administered to a subject in need of therapy, such as SCI therapy. Alternatively, the cells of the present disclosure can be
administered to the subject in need of SCI therapy in a pharmaceutical composition together with a suitable carrier and/or using a delivery system. [0074] As used herein, the term "pharmaceutical composition" refers to a preparation comprising a therapeutic agent or therapeutic agents in combination with other components, such as physiologically suitable carriers and excipients. [0075] As used herein, the term "therapeutic agent" can refer to the cells of the present disclosure accountable for a biological effect in the subject. Depending on the embodiment of the disclosure, "therapeutic agent" can refer to the oligodendrocyte progenitor cells of the disclosure. Alternatively, "therapeutic agent" can refer to one or more factors secreted by the oligodendrocyte progenitor cells of the disclosure. [0076] As used herein, the terms "carrier", "pharmaceutically acceptable carrier" and "biologically acceptable carrier" may be used interchangeably and refer to a diluent or a carrier substance that does not cause significant adverse effects or irritation in the subject and does not abrogate the biological activity or effect of the therapeutic agent. In certain embodiments, a pharmaceutically acceptable carrier can comprise dimethyl sulfoxide (DMSO). In other embodiments, a pharmaceutically acceptable carrier does not comprise dimethyl sulfoxide. The term "excipient" refers to an inert substance added to a pharmaceutical composition to further facilitate administration of the therapeutic agent. [0077] The therapeutic agent or agents of the present disclosure can be administered as a component of a hydrogel, such as those described in US Patent Application No.14/275,795, filed May 12, 2014, and US Patent Nos.8,324,184 and 7,928,069. [0078] The compositions in accordance with the present disclosure can be formulated for parenteral administration by injection, e.g., by bolus injection or continuous infusion. Formulations for injection can be presented in unit dosage form, e.g., in ampoules or in multi-dose containers, with an added preservative. The compositions can contain formulatory agents such as suspending, stabilizing and/or dispersing agents. In certain embodiments, the compositions can be formulated to be adapted for cryopreservation. [0079] The compositions in accordance with the present disclosure can be formulated for administration via injection to the spinal cord of a subject. The compositions may also be formulation for direct injection to the spinal cord of a subject. The compositions can be formulated for administration via implantation or other delivery methods. In certain
embodiments, a composition in accordance with the present disclosure can be formulated for intracerebral, intraventricular, intrathecal, intranasal, or intracisternal administration to a subject. In certain embodiments, a composition in accordance with the present disclosure can be formulated for administration via an injection directly into or immediately adjacent to an infarct cavity in the brain of a subject. In certain embodiments, a composition in accordance with the present disclosure can be formulated for administration through implantation. In certain embodiments, a composition in accordance with the present disclosure can be formulated for administration through other suitable delivery methods. In certain embodiments, a composition in accordance with the present disclosure can be formulated as a solution. [0080] In certain embodiments, a composition in accordance with the present disclosure can comprise from about 1 x 10
6 to about 5 x 10
8 cells per milliliter, such as about 1 x 10
6 cells per milliliter, such as about 2 x 10
6 cells per milliliter, such as about 3 x 10
6 cells per milliliter, such as about 4 x 10
6 cells per milliliter, such as about 5 x 10
6 cells per milliliter, such as about 6 x 10
6 cells per milliliter, such as about 7 x 10
6 cells per milliliter, such as about 8 x 10
6 cells per milliliter, such as about 9 x 10
6 cells per milliliter, such as about 1 x 10
7 cells per milliliter, such as about 2 x 10
7 cells per milliliter, such as about 3 x 10
7 cells per milliliter, such as about 4 x 10
7 cells per milliliter, such as about 5 x 10
7 cells per milliliter, such as about 6 x 10
7 cells per milliliter, such as about 7 x 10
7 cells per milliliter, such as about 8 x 10
7 cells per milliliter, such as about 9 x 10
7 cells per milliliter, such as about 1 x 10
8 cells per milliliter, such as about 2 x 10
8 cells per milliliter, such as about 3 x 10
8 cells per milliliter, such as about 4 x 10
8 cells per milliliter, or such as about 5 x 10
8 cells per milliliter. In certain embodiments, a composition in accordance with the present disclosure can comprise from about 1 x 10
8 to about 5 x 10
8 cells per milliliter, such as about 1 x 10
8 to about 4 x 10
8 cells per milliliter, such as about 2 x 10
8 to about 5 x 10
8 cells per milliliter, such as about 1 x 10
8 to about 3 x 10
8 cells per milliliter, such as about 2 x 10
8 to about 4 x 10
8 cells per milliliter, or such as about 3 x 10
8 to about 5 x 10
8 cells per milliliter. In yet another embodiment, a composition in accordance with the present disclosure can comprise from about 1 x 10
7 to about 1 x 10
8 cells per milliliter, such as about 2 x 10
7 to about 9 x 10
7 cells per milliliter, such as about 3 x 10
7 to about 8 x 10
7 cells per milliliter, such as about 4 x 10
7 to about 7 x 10
7 cells per milliliter, or such as about 5 x 10
7 to about 6 x 10
7 cells per milliliter. In an embodiment, a composition in accordance with the present disclosure can comprise from about 1 x 10
6 to
about 1 x 10
7 cells per milliliter, such as about 2 x 10
6 to about 9 x 10
6 cells per milliliter, such as about 3 x 10
6 to about 8 x 10
6 cells per milliliter, such as about 4 x 10
6 to about 7 x 10
6 cells per milliliter, or such as about 5 x 10
6 to about 6 x 10
6 cells per milliliter. In yet another embodiment, a composition in accordance with the present disclosure can comprise at least about 1 x 10
6 cells per milliliter, such as at least about 2 x 10
6 cells per milliliter, such as at least about 3 x 10
6 cells per milliliter, such as at least about 4 x 10
6 cells per milliliter, such as at least about 5 x 10
6 cells per milliliter, such as at least about 6 x 10
6 cells per milliliter, such as at least about 7 x 10
6 cells per milliliter, such as at least about 8 x 10
6 cells per milliliter, such as at least about 9 x 10
6 cells per milliliter, such as at least about 1 x 10
7 cells per milliliter, such as at least about 2 x 10
7 cells per milliliter, such as at least about 3 x 10
7 cells per milliliter, such as at least about 4 x 10
7 cells per milliliter, or such as at least about 5 x 10
7 cells per milliliter. In an embodiment, a composition in accordance with the present disclosure can comprise up to about 1 x 10
8 cells or more, such as up to about 2 x 10
8 cells per milliliter or more, such as up to about 3 x 10
8 cells per milliliter or more, such as up to about 4 x 10
8 cells per milliliter or more, such as up to about 5 x 10
8 cells per milliliter or more, or such as up to about 6 x 10
8 cells per milliliter. [0081] In an embodiment, a composition in accordance with the present disclosure can comprise from about 4 x 10
7 to about 2 x 10
8 cells per milliliter. [0082] In yet another embodiment, a composition in accordance with the present disclosure can have a volume ranging from about 10 microliters to about 5 milliliters, such as about 20 microliters, such as about 30 microliters, such as about 40 microliters, such as about 50 microliters, such as about 60 microliters, such as about 70 microliters, such as about 80 microliters, such as about 90 microliters, such as about 100 microliters, such as about 200 microliters, such as about 300 microliters, such as about 400 microliters, such as about 500 microliters, such as about 600 microliters, such as about 700 microliters, such as about 800 microliters, such as about 900 microliters, such as about 1 milliliter, such as about 1.5 milliliters, such as about 2 milliliters, such as about 2.5 milliliters, such as about 3 milliliters, such as about 3.5 milliliters, such as about 4 milliliters, or such as about 4.5 milliliters. In an embodiment, a composition in accordance with the present disclosure can have a volume ranging from about 10 microliters to about 100 microliters, such as about 20 microliters to about 90 microliters, such as about 30 microliters to about 80 microliters,
such as about 40 microliters to about 70 microliters, or such as about 50 microliters to about 60 microliters. In another embodiment, a composition in accordance with the present disclosure can have a volume ranging from about 100 microliters to about 1 milliliter, such as about 200 microliters to about 900 microliters, such as about 300 microliters to about 800 microliters, such as about 400 microliters to about 700 microliters, or such as about 500 microliters to about 600 microliters. In yet another embodiment, a composition in accordance with the present disclosure can have a volume ranging from about 1 milliliter to about 5 milliliters, such as about 2 milliliter to about 5 milliliters, such as about 1 milliliter to about 4 milliliters, such as about 1 milliliter to about 3 milliliters, such as about 2 milliliter to about 4 milliliters, or such as about 3 milliliter to about 5 milliliters. In an embodiment, a composition in accordance with the present disclosure can have a volume of about 20 microliters to about 500 microliters. In another embodiment, a composition in accordance with the present disclosure can have a volume of about 50 microliters to about 100 microliters. In yet another embodiment, a composition in accordance with the present disclosure can have a volume of about 50 microliters to about 200 microliters. In another embodiment, a composition in accordance with the present disclosure can have a volume of about 20 microliters to about 400 microliters. [0083] In certain embodiments, the present disclosure provides a container comprising a composition comprising a population of OPCs derived in accordance with one or more methods of the present disclosure. In certain embodiments, a container can be configured for cryopreservation. In certain embodiments, a container can be configured for administration to a subject in need thereof. In certain embodiments, a container can be a prefilled syringe. [0084] For general principles in medicinal formulation, the reader is referred to Allogeneic Stem Cell Transplantation, Lazarus and Laughlin Eds. Springer Science+ Business Media LLC 2010; and Hematopoietic Stem Cell Therapy, E.D. Ball, J. Lister & P. Law, Churchill Livingstone, 2000. Choice of the cellular excipient and any accompanying elements of the composition will be adapted in accordance with the route and device used for administration. In certain embodiments, the composition can also comprise or be accompanied by one or more other ingredients that facilitate the engraftment or functional mobilization of the enriched target cells. Suitable ingredients can include matrix proteins that support or promote adhesion of the target cell type or that promote vascularization of the implanted tissue.
Uses of the Cells of the Present Disclosure [0085] In various embodiments as described herein, the present disclosure provides methods of using a cell population that comprises pluripotent stem cell-derived OPCs for improving one or more neurological functions in a subject in need of therapy. In certain embodiments, methods for using pluripotent stem-cell derived OPCs in the treatment of acute spinal cord injury are provided. In other embodiments, methods for using pluripotent stem-cell derived OPCs in the treatment of other traumatic CNS injuries are provided. In other embodiments, methods for using pluripotent stem-cell derived OPCs in the treatment of non-traumatic CNS disorders or conditions are provided. In certain embodiments, a cell population in accordance with the present disclosure can be injected or implanted into a subject in need thereof. [0086] In certain embodiments, methods for using pluripotent stem-cell derived OPCs in the treatment of conditions requiring myelin repair or remyelination are provided. The following are non-limiting examples of conditions, diseases and pathologies requiring myelin repair or remyelination: multiple sclerosis, the leukodystrophies, the Guillain-Barre Syndrome, the Charcot-Marie-Tooth neuropathy, Tay-Sachs disease, Niemann-Pick disease, Gaucher disease and Hurler syndrome. Other conditions that result in demyelination include but are not limited to inflammation, stroke, immune disorders, metabolic disorders and nutritional deficiencies (such as lack of vitamin B12). The OPCs of the present disclosure can also be used for myelin repair or remyelination in traumatic injuries resulting in loss of myelination, such as acute spinal cord injury. [0087] The OPCs are administered in a manner that permits them to graft or migrate to the intended tissue site and reconstitute or regenerate the functionally deficient area. Administration of the cells can be achieved by any method known in the art. For example the cells can be administered surgically directly to the organ or tissue in need of a cellular transplant. Alternatively non-invasive procedures can be used to administer the cells to the subject. Non-limiting examples of non-invasive delivery methods include the use of syringes and/or catheters to deliver the cells into the organ or tissue in need of cellular therapy. [0088] The subject receiving the OPCs of the present disclosure may be treated to reduce immune rejection of the transplanted cells. Methods contemplated include the administration of traditional immunosuppressive drugs such as, e.g., tacrolimus,
cyclosporin A (Dunn et al., Drugs 61:1957, 2001), or inducing immunotolerance using a matched population of pluripotent stem cell-derived cells (WO 02/44343; U.S. Patent No. 6,280,718; WO 03/050251). Alternatively a combination of anti-inflammatory (such as prednisone) and immunosuppressive drugs can be used. The OPCs of the invention can be supplied in the form of a pharmaceutical composition, comprising an isotonic excipient prepared under sufficiently sterile conditions for human administration. [0089] Use in treatment of CNS traumatic injury. In certain embodiments, a cell population in accordance with the present disclosure can be capable of engrafting at a spinal cord injury site following implantation of a composition comprising the cell population into the spinal cord injury site. [0090] In certain embodiments, a cell population in accordance with the present disclosure is capable of remaining within the spinal cord injury site of the subject for a period of about 180 days or longer following implantation of a dose of the composition into the spinal cord injury site. In other embodiments, a cell population in accordance with the present disclosure is capable of remaining within the spinal cord injury site of the subject for a period of about 2 years or longer following implantation of a dose of the composition into the spinal cord injury site. In further embodiments, a cell population in accordance with the present disclosure is capable of remaining within the spinal cord injury site of the subject for a period of about 3 years or longer following implantation of a dose of the composition into the spinal cord injury site. In yet further embodiments, a cell population in accordance with the present disclosure is capable of remaining within the spinal cord injury site of the subject for a period of about 4 years or longer following implantation of a dose of the composition into the spinal cord injury site. [0091] In certain embodiments, a cell composition in accordance with the present disclosure is capable of reducing spinal cord injury-induced parenchymal cavitation in a subject. In certain embodiments, a lesion volume is reduced by formation of a tissue matrix in the spinal cord injury site. In certain embodiments, the cells of the present disclosure are capable of forming a tissue matrix in the spinal cord injury site within about 180 days or less. In certain embodiments, the subject with reduced injury-induced parenchymal cavitation is human. [0092] In certain embodiments, a cell population in accordance with the present disclosure can be capable of reducing a volume of an injury-induced central nervous system parenchymal cavitation in about 12 months or less. In certain embodiments, a cell population
in accordance with the present disclosure can be capable of reducing a volume of an injury- induced central nervous system parenchymal cavitation in a subject in about 6 months or less, about 5 months or less, or less than about 4 months. In certain embodiments, the subject is human. [0093] In an embodiment, one or more cells from a cell population in accordance with the present disclosure can be capable of migrating from a first location to one or more second locations within the central nervous system of a subject in need thereof. In an embodiment, one or more cells from a cell population in accordance with the present disclosure can be capable of migrating from the spinal cord of a subject to an affected tissue within the brain of the subject. In one embodiment, one or more cells from a cell population in accordance with the present disclosure can be capable of migrating from a first location within the spinal cord of a subject to a second location at an affected tissue within the spinal cord of the subject. In one embodiment, one or more cells from a cell population in accordance with the present disclosure can be capable of migrating from a first location within the brain of a subject to a second location at an affected tissue within the brain of the subject. In one embodiment, one or more cells from a cell population in accordance with the present disclosure can be capable of migrating from a first location within the brain of a subject to an affected tissue within the spinal cord of the subject. In one embodiment, one or more cells from a cell population in accordance with the present disclosure can be capable of migrating from a first location within the spinal cord of a subject to a second location at an affected tissue within the spinal cord of the subject, as well as to one or more locations at one or more affected tissues within the brain of the subject. In one embodiment, one or more cells from a cell population in accordance with the present disclosure can be capable of migrating from a first location within the brain of a subject to a second location at an affected tissue within the brain of the subject, as well as to one or more locations at one or more affected tissues within the spinal cord of the subject. [0094] In an embodiment, one or more cells from a cell population in accordance with the present disclosure can be capable of migrating from a first location to one or more second locations at one or more affected tissues within the central nervous system of a subject in less than about 150 days, such as less than about 100 days, such as less than about 50 days, or such as less than about 10 days. In an embodiment, one or more cells from a cell population
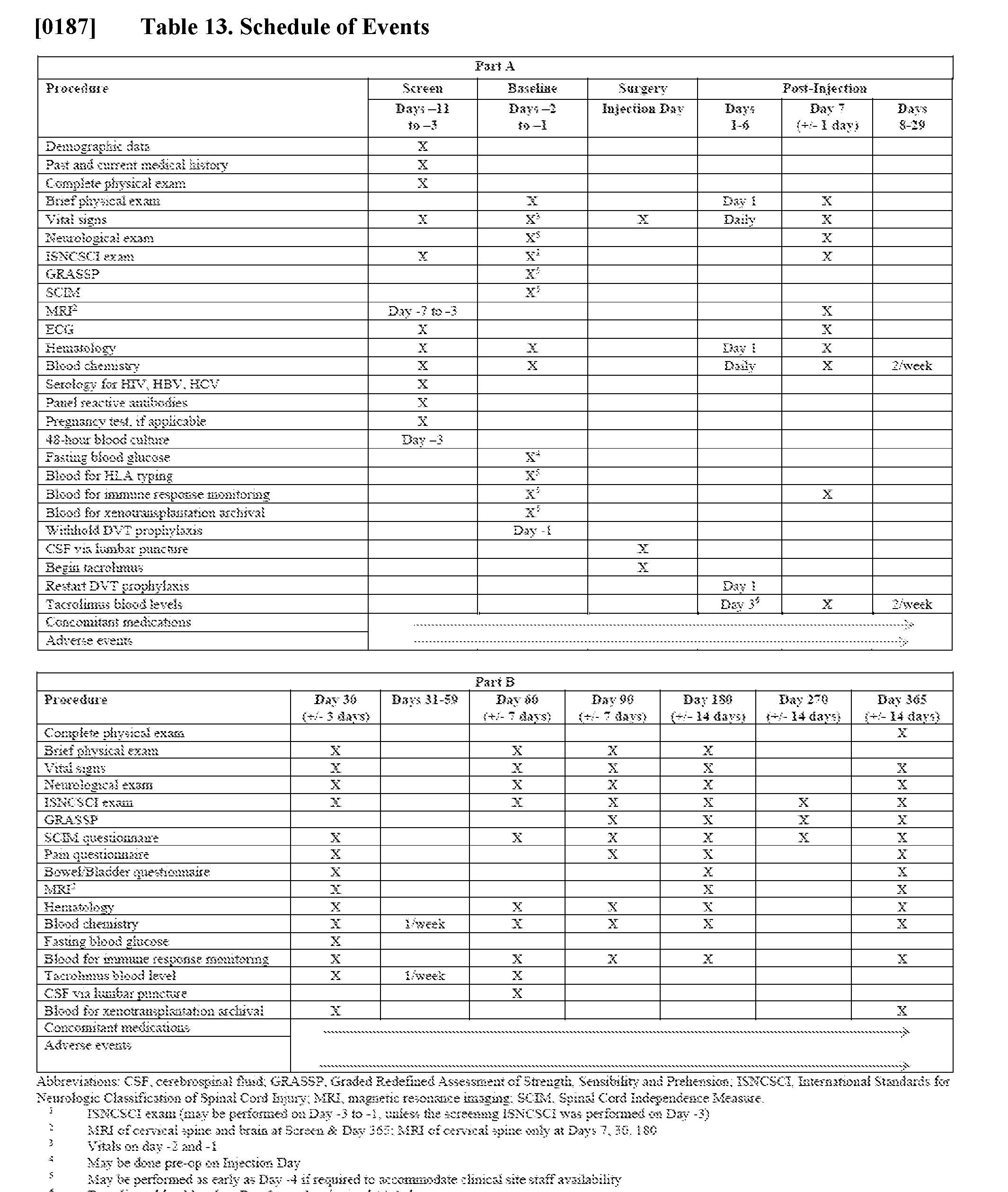
in accordance with the present disclosure can be capable of migrating from a first location to one or more second locations at one or more affected tissues within the central nervous system of a subject in about 180 days or less. EXAMPLES [0095] Examples 1-8 describe the first-in-human Phase 1 safety clinical trial of oligodendrocyte progenitor cells derived from human pluripotent stem cells (LCTOPC1) which have mechanistic properties to support survival and potential repair of key cellular components and architecture of the SCI site. Example 9 describes a Phase 1/2a dose escalation study of oligodendrocyte progenitor cells derived from human pluripotent stem cells (AST-OPC1) for use in subacute cervical SCI. Example 1 - Patients and Methods [0096] Study design. The trial design was an open-label, multicenter study. A single dose of 2 × 10^6 LCTOPC1 was injected within 7 to 14 days following SCI. Subjects who received LCTOPC1 also received tacrolimus to prevent rejection. Subjects will be followed by protocol for 15 years following administration of LCTOPC1. [0097] Study Participants. Male or female participants from 18 to 65 years of age with acute traumatic spinal cord injury were eligible for study participation. As this was a first in man study, with a risk of neurological deterioration, inclusion was limited to neurologically complete injuries (American Spinal Injury Association Impairment Scale A), with a single neurological level of injury (NLI) from levels T3-T10, with no spared motor function < 5 levels (i.e. zone of partial preservation) below the single neurological level. These inclusion criteria were chosen to minimize loss of function if neurological deterioration were to occur. [0098] Post-stabilization magnetic resonance imaging (MRI) was used to confirm the presence of a single spinal cord lesion with sufficient visualization of the spinal cord for 30 mm above and below the injury epicenter to enable post-injection safety monitoring. Participants had to be eligible for an elective surgical procedure to inject LCTOPC17 to 14 days following SCI. [0099] This study was a Phase 1, multi-center, non-randomized, a single group assignment interventional clinical trial. The Participants were enrolled from one of seven centers in the United Sates. The study was registered (NCT01217008) and the primary endpoint was safety, as measured by the frequency and severity of adverse events related to LCTOPC1, the injection
procedure used to administer LCTOPC1, and/or the concomitant immunosuppression administered. The secondary endpoint was neurological function as measured by sensory scores and lower extremity motor scores on ISNCSCI examinations. The eligibility criteria are summarized in Supplemental Table 1. Participants have been followed by protocol for a total of 5 years of in-person visits and are being followed for an additional 10 years of annual phone visits. Figure 1 provides an overall study schema for the clinical trial. [0100] The LCTOPC1 product is a cell population containing a mixture of oligodendrocyte progenitor cells and other characterized cell types obtained following directed differentiation of undifferentiated human embryonic stem cells. The initial characterization of the LCTOPC1 population was reported by Nistor et al 2005, who showed that these cells could differentiate into oligodendroglial progenitors. Subsequent studies demonstrated that the oligodendroglial progenitor cells survived after delivery to the spinal cord injury site in an acute incomplete rat contusion injury model. The cells led to sparing of tissue at the contusion site with evidence of remyelination of denuded axons. When delivered in the acute injury period, the cells led to improvement in locomotor function as measured in standardized behavioral testing. Preclinical studies in rats and mice demonstrated that the intended clinical, cryopreserved human equivalent dose formulation of LCTOPC1 could survive and migrate after injection in the SCI site, produce neurotrophic factors to support cell survival, provide remyelination potential to support denuded axons, and lead to tissue sparing at the SCI contusion site. Moreover, studies demonstrated that the cells did not produce teratomas, and did not lead to increased pain in injured animals. [0101] This Phase 1 clinical trial was reviewed by the FDA, the Data and Safety Monitoring Board (DSMB), the SCI clinical community, surgical and outcomes steering committees, internal and external ethics committees, internal and clinical trial site stem cell research oversight committees, and the IRBs for each participating clinical trial site. As a first-in-human study, the trial design accounted for the need to minimize the risk to participants, and hence individuals with complete SCI localized between the thoracic neurological levels T3-T11 were chosen for intervention. The trial was an open-label, unblinded, non-randomized, non-placebo-controlled study to establish the safety of intraparenchymal injection of LCTPOC1 as well as to determine changes in neurological function. [0102] Determining the long-term safety of stem cell therapeutics is a critical step in enabling future trials to investigate novel stem cell therapeutics or combination therapies. Ten years post-
implantation, there have been no medical or neurological complications to indicate that LCTOPC1 implantation is unsafe. Specifically, there have been no Serious Adverse Events (SAEs) related to the procedure, cell implant, or immunosuppression. In addition, there have been no significant changes in neurological function. Safety data from this first-in-human study supported progression to a clinical trial for individuals with cervical spinal cord injuries. [0103] The starting material for the production of AST-OPC1 is an H1 master cell bank produced from the H1 uhESC line derived at the University of Wisconsin in 1998. Compositional analysis of LCTOPC1 by immunocytochemistry and flow cytometry indicates that the cell population is comprised mostly of neural lineage cells of the oligodendrocyte progenitor phenotype. In this safety study, the intended route of administration for LCTOPC1 was a direct injection of 2 × 10^6 viable LCTOPC1 cells into the spinal cord at a level 5 mm caudal to the injury epicenter. [0104] The rationale for the selection of this dose was based upon pre-clinical studies involving rats and mice, and upon dose extrapolation to humans using two methods: 1) comparing the relative sizes of the human and rat spinal cords, and 2) evaluating tumorigenicity with respect to the absolute number of injected cells. Further, the rationale for the selection of this route of delivery was based on the results from nonclinical pharmacology studies, which showed that LCTOPC1 has properties that support repair of pathology in spinal cord lesions. Results from these studies also demonstrated that improvements in locomotor recovery were associated with robust LCTOPC1 cell survival at the lesion site. [0105] Spinal cord injuries localized between the T3 and T11 neurological level, as assessed by the ISNCSCI, were chosen as the target for intervention. The primary goal of this first-in- human study was to establish the safety of intraparenchymal injection of hESC derived oligodendrocyte precursor cells into the spinal cord of individuals between 7-14 days post-injury. The secondary outcome measure in this trial was the ISNCSCI examination which allowed for the identification of motor and sensory changes at any of 13 in-person evaluations scheduled within the first five years post-injection. [0106] Ten-years post-implantation, there have been no medical or neurological complications to indicate that the cell implantation was unsafe. Specifically, there have been no serious adverse events (SAEs) related to the procedure, cell implant, or immunosuppression. This report will
review the first 10 years of data from this landmark clinical trial including early post-operative events, in-person follow-up through year 5 and conclude with data from telephone follow-up to the current time. [0107] Investigational Product, Dose Preparation, Dose and Mode of Administration. LCTOPC1 is a cell population containing a mixture of oligodendrocyte progenitor cells and other characterized cell types that are obtained following differentiation of undifferentiated human embryonic stem cells (hESC) from the H1 stem cell line, produced at the University of Wisconsin in 1998. [0108] Compositional analysis of LCTOPC1 by immunocytochemistry and flow cytometry indicates that the cell population is comprised mostly of neural lineage cells of the oligodendrocyte progenitor phenotype. In this safety study, the intended route of administration for LCTOPC1 was a direct injection of 2 × 10^6 viable LCTOPC1 cells into the spinal cord at a level 5 mm caudal to the injury epicenter. [0109] LCTOPC1 is a cryopreserved cell therapy product. At the time of cryopreservation, each vial contained 7.5 × 10
6 viable cells in 1.2 mL of cryoprotectant solution. LCTOPC1 was supplied in 2.0 mL cryovials and shipped to the clinical sites in the vapor phase of liquid nitrogen and stored under the same conditions at the site. Prior to administration, LCTOPC1 was thawed and prepared by study personnel who were trained and qualified in the preparation of the study drug. [0110] Participants received a single administration of 2 × 10
6 viable LCTOPC1 cells suspended in Hank’s balanced salt solution (HBSS) total volume per dose = 50 μL. The rationale for selection of this dose was based upon pre-clinical studies involving rats and mice, and upon dose extrapolation to humans using two methods: 1) comparing the relative sizes of the human and rat spinal cords, and 2) evaluating tumorigenicity risks with respect to the absolute number of injected cells. At that time during the development of LCTOPC1, 2x10
6 cells was the highest dose that was feasible to administer in the injured rat spinal cord and the rat was the largest animal that could be utilized to satisfy the animal number required for the IND-enabling studies for this novel product. Hence, to be conservative, 2x 10
6 cells, the highest dose tested in rats, was used as the dose for the Phase 1 trial. Participants who received LCTOPC1 also received tacrolimus to prevent rejection of this allogeneic cell-based product.
[0111] The intended route of administration for LCTOPC1 was intra-parenchymal at a depth of 6 mm, in the midline, 5 mm caudal to the epicenter of injury as determined by MRI, as modeled in preclinical studies. A caudal injection was selected out of an abundance of caution to avoid any potential direct tissue damage above the injury level. Based on preclinical studies, it was anticipated that the injected cells would migrate rostrally throughout the injury site. LCTOPC1 was administered to the spinal cord in a dedicated surgical procedure 7-14 days following injury. This time frame was chosen based on results of animal studies suggesting poor graft survival for implantation within the first 7 days of injury while attempting to maximize the potential neuroprotective and remyelinating effect. A custom-designed syringe positioning device was utilized to assist neurosurgeons with the controlled delivery of the cells. [0112] Tacrolimus Immunosuppression. Immunosuppression with tacrolimus was initiated between 6 and 12 hours after injection of LCTOPC1. If the participant was unable to take oral medication, tacrolimus was administered intravenously at a starting dose of 0.01 mg/kg/day, given as a continuous intravenous infusion. Participants were switched to oral tacrolimus as possible. The starting dose for oral tacrolimus was 0.03 mg/kg/day, divided into 2 daily doses. The tacrolimus dose was adjusted to achieve a target whole blood trough level of 3 to 7 ng/mL. [0113] On Day 46, the tacrolimus dose was decreased by 50% (rounded to the nearest 0.5 mg, as this was the smallest capsule size available). On Day 53, the tacrolimus dose was decreased by another 50% (rounded to the nearest 0.5 mg). If the rounded total daily dose was 0.5 mg or lower, the participant received 0.5 mg once per day until tacrolimus was discontinued. Tacrolimus was discontinued at Day 60. The dose of tacrolimus was lowered if the trough blood level exceeded 7 ng/mL. In addition, an expert reviewed all ISNCSCI examination forms to assess whether there were any changes in neurological function that may have been associated with tacrolimus tapering and/or discontinuation. [0114] Follow-up and Assessments. An overview of study visits for the one-year protocol follow-up (CP35A007) and 2-15-year protocol follow-up (CP35A008) is provided in the study schema (Figure 1). As this was a first clinical trial of cells derived from hESCs, a high number of study visits and long-term follow-up were required. In the one-year protocol, three study visits were required prior to product administration, with 13 in the first year following study administration. For the long-term protocol, annual visits were required in years 2-5. Subsequent to the year 5 annual visit, follow-up was by annual phone questionnaires (Figure 4) and in-person
evaluations, as necessary. Phone assessments include documentation of all new medications taken for longer than 30 days, admissions to the hospital, and documentation of AEs and SAEs. [0115] Safety Assessments. The primary endpoint of the Phase 1 clinical trial was safety, as measured by the frequency and severity of adverse events (AEs) within 1 year of LCTOPC1 injection that were related to LCTOPC1, the injection procedure used to administer LCTOPC1, and/or the concomitant immunosuppression administered. Safety assessments included physical examination, vital signs, ISNCSCI neurological examination, pain questionnaire, electrocardiogram, MRI, laboratory tests for hematology and blood chemistry, laboratory tests for immunosuppression safety monitoring (whole blood trough levels of tacrolimus, serum levels of creatinine, potassium, magnesium, phosphate, ionized calcium, aspartate aminotransferase, alanine aminotransferase, and total bilirubin), concomitant medications, and AEs. [0116] Definition of an Adverse Event. AEs were tabulated by system organ class and by preferred term within system organ class according to the Medical Dictionary for Regulatory Activities (MedDRA®) Version 10. An AE was any untoward medical event that occurred to a study participant once the participant had signed the informed consent form until the study participant’s last study visit, whether or not the event was considered drug-related. The severity of AEs and the characterization of Serious Adverse Events (SAEs) were evaluated using standard FDA criteria. [0117] The relationship of AEs to the investigational drug was determined by each site investigator and was categorized as “Possibly Related” based on the following criteria: 1) the AE was reasonably related in time with LCTOPC1 exposure, the injection procedure used to administer LCTOPC1, and/or the concomitant immunosuppression administered AND 2) the AE could be explained either by exposure to the investigational product or equally well by factors or causes other than exposure to the investigational product. Adverse events were monitored by the External Medical Monitor, Sponsor Medical Monitor, and DSMB. [0118] Neurological Assessments. The secondary endpoint was neurological function including measurement of sensory scores and lower extremity motor scores. Neurological function was evaluated using the ISNCSCI examination for motor and sensory testing and for designation of the American Spinal Injury Association (ASIA) impairment scale (AIS). [0119] Exploratory Endpoints. Pain assessment was performed using the International Spinal Cord Injury Pain Basic Data Set. A set of three questions was added to assess allodynia. These
questions covered the presence and severity of pain provoked or increased by brushing, pressure or contact with cold. Information on pain medication was collected as part of the assessment of concomitant medications. Potential exploratory endpoints for recovery of neurological function were: University of Alabama-Birmingham Index of Motor Recovery (UAB-IMR), Spinal Cord Independence Measure (SCIM), and assessment of bowel and bladder function. [0120] Lumbar Puncture. A lumbar puncture to obtain 10 mL of cerebrospinal fluid (CSF) was conducted after receiving general anesthesia but prior to LCTOPC1 injection as well as at day 60 post-injection. The volume required at individual study sites for the following tests were sent to the hospital laboratory: white blood cell count, glucose, total protein, oligoclonal banding, myelin basic protein, and immunoglobulin G index. In addition, CSF was evaluated by the sponsor to assess immune response to LCTOPC1. [0121] Magnetic Resonance Imaging. Screening/Baseline MRI was obtained between 3 and 5 days prior to injection (Day-3 and Day -5) of LCTOPC1 but no earlier than 4 days after SCI. Screening/baseline MRI included the brain, cerebellum, and entire spinal cord, with and without contrast (gadolinium dietheylenetriamine pentaacetic acid [Gd-DTPA]). If surgery for LCTOPC1 injection was subsequently delayed for more than 3 days, then a repeat MRI of the thoracic spine, without contrast, was obtained. Follow-up MRIs of the spinal cord and cerebellum, with and without contrast (Gd-DTPA), were obtained on Days 7, 60, 120, and 270 post-injection. A full central nervous system MRI, with and without contrast (Gd-DTPA), was obtained on Days 30, 90, 180, and 365 as well as yearly between years 2-5. Image acquisition protocols were standardized. Image review was centralized and standardized with by an independent radiologist, DD at Radiology Imaging Associates Denver. [0122] HLA Typing and Immunological Monitoring. LCTOPC1 cells do not express Human Leukocyte Antigen (HLA) Class II and are resistant to NK cell lysis. However, one concern in regard to the safety and potential efficacy of LCTOPC1 was the possibility of allogeneic rejection by the host’s immune system. Immunosuppression was minimized in terms of duration to 60 days and dosed below the typical long-term maintenance therapy levels used for solid organ transplant. Peripheral blood and cerebrospinal fluid (CSF) samples from LSTOPC1 injected participants were collected according to protocol. A lumbar puncture to obtain 10 mL of CSF was conducted after receiving general anesthesia but prior to LCTOPC1 injection as well as at day 60 post-injection to assess for rejection of allogenic cells as well as for immunologic
monitoring. The following assessments occurred at the hospital laboratory: white blood cell count, glucose, total protein, oligoclonal banding, myelin basic protein, and immunoglobulin G index. Peripheral blood was examined for the presence of antibodies specific for the donor- specific HLA molecules on LCTOPC1 and to detect T cell-mediated responses to LCTOPC1. In addition, CSF was evaluated by the sponsor to further assess immune response to LCTOPC1 and for the presence of LCTOPC1 (day 60) using a PCR based assay. [0123] Statistical Methods. Descriptive analysis was used due to the small sample size, open- label, and non-randomized study design. The primary and secondary endpoints of this study are presented descriptively in table, figure, and text form. Results [0124] Study Participants. The first participant was implanted the winter of 2010 and the last participant was enrolled in the winter of 2011. Eleven individuals with SCI were screened for enrollment, with six individuals who failed screening: four due to MRI artifacts which prohibited adequate spinal cord visualization, one based on the ISNCSCI examination (NLI T1), and one due to elevated liver enzymes. A total of five individuals with SCI received LCTOPC1 at three study sites. Figure 2 provides a Consolidated Standard of Reporting Trials (CONSORT) flow diagram. In this trial, the most common mechanism of injury was motor vehicle-related for four of five individuals, with a fall being the cause of injury in one individual. Four of five participants enrolled were male. The cohort age ranged from 21 to 32 years of age (Table 1).

[0125] Participant Follow-up. As of this publication, all participants have entered their tenth year of follow-up. In agreement with the FDA, the trial was structured to begin with 5 years of in-person evaluation followed in years 6 through 15 with phone interviews. During the first 5
years of the study, 24 of 25 in-person annual visits were completed. One participant did not participate in the year 5 in-person visit but has participated in scheduled phone follow-up. From year 6 to the current time, 21 of 21 annual phone interviews have been completed. One participant has completed 10 years of follow-up and four participants are entering their 10-year follow-up interviews. [0126] Primary Outcome Measure: Evaluation of Safety. All SAEs and AEs (related and unrelated to procedure, cell implant, or immunosuppression) are summarized in Table 2 and described below. [0127] Table 2.

[0128] Serious Adverse Events Related to Procedure, Cell Implant, or Immunosuppression. There were no SAEs related to the procedure, cell implant, or immunosuppression. There were no findings of clinical concern on MRI scans of the full central nervous system through five years post-injection in any participant. During long-term phone follow-up participants denied
having any fever of unknown cause, no changes in sensation in chest, arms, or legs (other than described below), and no participants have been diagnosed with any type of cancer. No participants died during the study. Safety events were monitored by the DSMB and no suspension rules were triggered. [0129] Serious Adverse Events Unrelated to Procedure, Cell Implant, or Immunosuppression. Three participants have reported four SAEs unrelated to the procedure, cell implant, or immunosuppression. These SAEs included urinary tract infection (UTI) and subsequent transitory autonomic dysreflexia in one individual, pyelonephritis, and a mood disorder in two different individuals. [0130] Adverse Events Categorized by Grade. Over the course of the trial, 25 AEs were judged by the Investigators to be possibly related to LCTOPC1 (Grade 1 / Mild [n=9], Grade 2 / Moderate [n=15], and Grade 3 / Severe [n=1]). The Grade 3 AE was described as a burning sensation in the trunk and lower extremities first reported on Day 57 post-injection with Grade 1 severity, increasing to Grade 3 severity on Day 90 post-injection. This neuropathic pain resulted in three additional Grade 2 severity AEs and was ongoing through year 9 follow-up. Grade 2 AEs included: surgical site pain, hypomagnesemia, urinary tract infection, vaginal yeast infection, emesis, upper back pain, shoulder pain, pain with range of motion, and autonomic discomfort during catheterization relieved after treatment with lidocaine. Grade 1 AEs included: hypomagnesemia, urinary tract infection, fever, headache, nausea, and spasticity. [0131] Adverse Events Categorized by Relation to Procedure, Cell Implant, or Immunosuppression. Nine of the 25 related adverse events were deemed possibly related specifically to the injection procedure. Eight of the nine were Grade 1 or 2 in severity and one was Grade 3. The AEs were predominantly transient postoperative pain, one fever, and one urinary tract infection. There were no AEs attributed to the cell implant. Moreover, the immunosuppression regiment was well tolerated, and all five participants completed the regimen per protocol. Sixteen of the 25 adverse events were deemed possibly related specifically to the immunosuppression. Seven Grade 1 AEs and nine Grade 2 AEs were judged to be possibly related specifically to tacrolimus. These AEs were primarily known common adverse reactions to tacrolimus (nausea/emesis, low magnesium level, infections). Among reported infections, 1 of 7 was a vaginal yeast infection and 6 of 7 infections were in the urinary tract, which is a common complication of SCI.
[0132] Adverse Events Unrelated to Procedure, Cell Implant, or Immunosuppression. At year 6, one participant reported an increase in frequency and intensity of muscle spasms attributed to functional electrical stimulation (FES) cycling. This participant reported resolution of these symptoms during years 7 through 9 and is currently not using any medication for muscle spasms. In year 9, a different individual received outpatient testing after developing a deep vein thrombosis (DVT). [0133] Secondary Outcome Measure: Neurological Assessment. After discharge from acute inpatient rehabilitation and through the first five years post-implantation, participants continued to be evaluated in-person according to the schedule shown in Figure 1. Of note, between baseline and Year 5, participants’ annual in-person evaluations included at least 13 ISNCSCI exams. All participants had an ASIA impairment Score (AIS) grade of A on enrollment in the trial and all participants have maintained the same impairment grade. The highest single and lowest NLI enrolled in the study were T3 and T8 respectively. Only the individual with T3 NLI improved to T4 with a sensory ZPP initially at T4 bilaterally noted to improve to T5 on the left and T6 on the right at one year follow-up. In total three of five participants experienced at least one level of improvement in their ZPP. All participants began and ended the 5 years of in-person ISNCSCI examination with intact upper extremity motor function with an upper extremity motor score (UEMS) of 50 out of 50, and lower extremity motor score (LEMS) of 0 out of 50 (Table 3). Over the course of 5 years of in-person follow-up, sensory examinations have not materially changed. Figure 3 provides a diagrammatic representation of the motor and sensory function of each patient at baseline and at 5 years post LCTOPC1 administration.
Table 3 presents total sensory score (TSS), upper extremity motor score (UEMS), lower extremity motor score (LEMS), sensory neurological level of injury (NLl), motor NLl, sensory zone of partial preservation (ZPP), Motor ZPP, and ASIA impairment Score (AIS) grade at baseline, year 1 and year S, All five Individuals were AIS Grade A at enrollment and there were no conversions to AIS B, The highest single and lowest NU enrolled in the study were T3 and T8 respectively. Only the Individual with the T3 NLl improved to T4 with a sensory ZPP initially at T4 bilaterally noted to improve to T5 on the left and 76 on the right at one year follow up. In total three of five participants experienced at least 1 level of improvement in their ZPP. ND= Unable to determine.
[0134] MRI Findings. No participant exhibited evidence of an enlarging cyst, enlarging mass, spinal cord damage related to the injection procedure, intramedullary hemorrhage, CSF leak, epidural abscess or infection, inflammatory lesions in the spinal cord, CSF flow obstruction, or masses in the ventricular system. No evidence of any adverse neurological changes or adverse changes on MRI was reported during tacrolimus tapering or after tacrolimus discontinuation.
[0196] TABLE 15. Summary of Related Adverse Events in All Treated Participants

[0197] DISCUSSION. The safety data from this study suggest that AST-OPC1 can be safely administered to participants in the subacute period after cervical SCI. The injection procedure and the low-dose temporary immunosuppression regimen were well tolerated. None of the 25 participants who received LCTOPC1 showed evidence of neurological deterioration. There were no SAEs reported as directly related to LCTOPC1 and evaluation of the AEs did not show an increase in incidence for commonly reported SCI complications, such as urinary tract infections, muscle spasms, or neuropathic pain (Sezer 2015). In this study involving participants with cervical C4-C7 AIS-A and AIS-B, at one-year follow-up, 24/25 (96%) of participants recovered one or more levels of motor function on at least one side of their body and 8/25 (32%) of participants
recovered two or more levels of motor function on at least one side of their body. Improvement of two motor levels can change a person’s functional capacity from requiring total assistance for activities of daily living to near independence (Whiteneck et al.1999). The safety and neurological recovery data, from both the thoracic and cervical trials, have provided evidence that hESC- derived treatments can be safely delivered into the spinal cord. Example 10 – Decorin Secretion as a Potency Assay for OPC1. [0198] Treatment with recombinant Decorin in rat models of spinal cord injuries (SCI) has been shown to inhibit inflammation and glial scar formation and may promote axonal growth across the injury interface after acute spinal cord injury (Wu, Li et al, 2013, Ahmed, Bansal et al. 2014). Decorin has been shown to suppress acute scarring and wound cavitation and induce dissolution of mature scar tissue in dorsal funicular lesion SCI model system of the spinal cord in adult rats (Wu, Li et al, 2013, Ahmed, Bansal et al 2014). DFL cavity treatment with recombinant Decorin suppresses inflammation and scar deposition in the acute and subacute phases of the CNS injury response in rat model of SCI and also contributes to dissolution of the mature scar following SCI (Esmaeli, Berry et al 2014, Ahmed, Bansal et al 2014). OPC1 treatment in non-clinical models of SCI has demonstrated similar results to that seen in the published studies above. [0199] OPC1 cells have been shown to produce large amounts of Decorin. The results seen in the OPC1 animal studies demonstrate very similar anatomical outcomes to that seen in the studies above. Thus, the anatomical effects observed in the nonclinical efficacy studies of OPC1 transplantation into SCI injury may be attributed, at least in part, to the secretion of Decorin. [0200] While the preclinical studies to date have established the optimal window for OPC1 implantation to achieve maximum efficacy between 14-60 days post-injury, Decorin has been shown to have an effect in dissolving mature scars following SCI (Esmaeli, Berry et al 2014, Ahmed, Bansal et al 2014), lending evidence for a potential role of OPC1 cells in the treatment of chronic SCI subjects. [0201] Introduction [0202] Decorin is a naturally occurring extracellular small leucine-rich proteoglycan TGF- β1/2 antagonist which regulates diverse cellular functions through interactions with components of the extracellular matrix (ECM) and plays several key roles in the cellular response to spinal
cord injury. Accordingly, Decorin secretion in vitro was developed and qualified as a potency assay for OPC1. [0203] Briefly, OPC1 Drug Product cells are thawed and cultured for 48 hours, then the media is collected and secreted Decorin concentration measured by an ELISA assay. [0204] Preliminary molecular analysis and an initial ELISA revealed that Decorin is not secreted by H1 hESC, and that its expression is gradually turned on during OPC1 differentiation, with the highest levels of a secreted protein detected in the drug product. This, along with scientific literature showing a biological activity inclusive of scarring suppression at injury site and stimulation of axonal growth through spinal cord injury (SCI) site, supports Decorin as a suitable potency candidate. [0205] Decorin (secretion) is useful as a potency indicator for OPC1 cells by describing its ability to modulate SCI tissue remodeling, via attenuating harmful processes. [0206] Decorin is a biological modulator secreted by OPC1 [0207] OPC1 Drug Product is a cryopreserved cell population containing oligodendrocyte progenitor cells and other characterized cell types that are obtained following differentiation of H1 human embryonic stem cells (hESC). OPC1 has been shown to have three potentially reparative functions which address the complex pathologies observed at the SCI injury site. These activities of OPC1 include production of neurotrophic factors, stimulation of vascularization, and induction of remyelination of denuded axons, all of which are critical for survival, regrowth and conduction of nerve impulses through axons at the injury site. One of the potential routes by which OPC overcome the inhibitory factors at the injury site may be Decorin upregulation as a response of NG2
+ (neuron-glial antigen 2, CSPG4) cells to retinoic acid (Goncalves, Wu et al.2019). [0208] It is important to note that Decorin secretion is acquired by OPC1 cells during the differentiation process as part of their maturation, feature enabling easy and quantifiable Decorin measurement as a possible potency marker of OPC1. [0209] Decorin secretion was approximately 25 ng Decorin per day. Accordingly, the current threshold for the Decorin potency assay was defined as 25 ng/ml. [0210] Decorin has been shown to be effective in reducing scarring, when produced endogenously by different cell types at the injury site or given exogenously in a recombinant form in non-clinical models of SCI, as described below.
[0211] Thus, active de-novo secretion of endogenous Decorin by OPC1 during its implantation into the SCI cavity may be a key component to ensure successful treatment, and, as such, may be a good potency marker. [0212] Spinal Cord Injury [0213] The majority of traumatic SCIs result in contusion or compression of the spinal cord. The mechanical insult (primary injury) in these cases causes a cascade of molecular and cellular changes that are collectively referred to as the secondary injury (Kakulas 1999). Some of the pathological changes associated with secondary injury include petechial hemorrhages progressing to hemorrhagic necrosis, free radical-induced lipid peroxidation, elevated intracellular calcium leading to activation of neutral proteases, accumulation of extracellular potassium, accumulation of excitatory amino acids, and ischemia (Anderson 1993, Hulsebosch 2002). Traumatic demyelination also begins within a few hours after injury (Kakulas 1999). [0214] The cellular response to SCI is generally considered to consist of 3 phases: an acute hemorrhagic phase when hematogenous inflammatory cells invade the wound; a sub-acute phase when scarring is initiated from astrocytes interacting with invading meningeal fibroblasts to produce a glia limitans around the wound cavity with a core of extracellular matrix (ECM) proteins, revascularization is also initiated, and axon growth is arrested at the wound margins; and a consolidation or chronic phase when ECM deposits are remodeled by proteases to establish a mature contracted scar. [0215] The superimposition of progressive wound cavitation on top of the cellular response results in a progressive cystic expansion of an astrocyte-free void filled with proteoglycans and macrophages and bordered by a proteoglycan-rich neurophils that cause secondary destruction of axons. [0216] Cellular and extracellular composition of the spinal cord injury scar tissue [0217] Traumatic SCI triggers a complex cascade of events that culminates in the formation of a scar which consists of multiple cell types, as well as extracellular and non-neural components. In the acute post-injury phase (0–72 h), cell death and damage lead to release of a number of cellular and blood-derived damage associated molecular patterns (DAMPs). These are powerful activating and inflammatory stimuli for stromal cells, astrocytes, NG2+ OPCs and microglia. Fibroblast-like cells proliferate from perivascular origin in this acute phase. Activated cells increase deposition of
ECM molecules such as Chondroitin sulfate proteoglycans (CSPGs) and stromal-derived matrix. Circulating immune-responders (neutrophils, monocytes) are recruited, their relative expression of cytokines, chemokines and matrix metalloproteinases is that of a mixed cell phenotype (pro- inflammatory and pro-resolving). Over time, the injury microenvironment becomes increasingly proinflammatory. In the chronic spinal injury scar, monocyte-derived macrophages/microglia adopt a predominantly pro-inflammatory phenotype. Rather than entering a resolution phase, responding innate immune cells present DAMPs to circulating adaptive immune cells and the pathology spreads. Hypertrophy of reactive astrocytes, upregulated expression of intermediate-filament associated proteins and secretion of matrix CSPGs occur. Scar-forming reactive astrocytes are organized into a barrier-like structure, which separates spared tissue from a central region of inflammation and fibrosis where wound-healing fails to undergo resolution. In most mammalian species, a chronic cystic cavity develops. Wallerian degeneration of injured axonal projections contributes to continued extracellular deposition of axonal and myelin debris, which is ineffectively processed by immune cells, and along with CSPGs, acts to inhibit neuronal regeneration and neuroplasticity (Bradbury and Burnside 2019). [0218] Function of Decorin in Spinal Cord Injury [0219] OPC1 clinical application is aimed at the sub-acute phase, 21-60 days post-SCI. It is thus assumed that the transplantation of OPC1 occurs during the transition from acute to chronic phase, in an inflammatory active environment. Hence, the ability of OPC1 to actively secrete Decorin that can potentially reduce the ongoing negative cues may be useful for its therapeutic activity. [0220] Decorin suppresses CNS scarring through several mechanisms (Esmaeili, Berry et al. 2014, Gubbiotti, Vallet et al. 2016) including: (1) attenuating both TGF-β1/2 receptor activation and signaling through down-stream SMADs (a family of intracellular proteins that mediate signaling by members of the TGF-beta superfamily), that mediate transcriptional activation of ECM production; (2) binding to type I collagen fibrils to inhibit fibrogenesis; (3) forming an activity-blocking complex with connective tissue growth factor (CTGF); (4) binding to fibronectin and inhibiting cell adhesion and fibroblast migration; (5) abrogating inflammation, CSPG/laminin/fibronectin-rich scar formation and the injury responses of astrocytes, microglia and macrophages; (6) stimulating microglia to secrete plasminogen/plasmin (the activity of which is moderated by PAI-1), which then regulates matrix metalloproteinase (MMP): tissue inhibitors
of MMP (TIMP) ratios in wounds to initiate fibrolytic degradation of ECM underpinning remodeling during the consolidation phase of acute scarring; and (7) binding to the epidermal growth factor receptor (EGFR), hepatocyte growth factor (Met) receptor and toll-like receptors to modulate angiogenesis and inflammatory responses. [0221] Recombinant human Decorin (Galacorin), was investigated as a potential treatment for macular degeneration, diabetic retinopathy and diabetic macular edema (Nastase, Janicova et al. 2018). In the patent US9061047B2, the authors suggest using Galacorin for preventing or reducing scar formation by its administration to patients with neurological conditions including central nervous system injuries and/or diseases. A formulation of Decorin in an eye drop was reported as an anti-scarring agent that can replace corneal transplantation (Hill, Moakes et al.2018). [0222] Decorin promotes axon regeneration directly by suppressing the production of scar- derived growth inhibitory ligands (Esmaeili, Berry et al. 2014) and indirectly by: (1) plasmin activation of neurotrophins (Davies, Tang et al.2006); (2) disinhibition of axon growth cone advance by digestion of CSPG and CNS myelin inhibitors through plasmin and plasmin induced activation of MMP (Minor, Tang et al.2008); and (3) suppression of EGFR activity in growth cones, thereby potentially blocking CSPG/CNS myelin mediated growth cone collapse. [0223] Treatment with recombinant Decorin in rat models of SCI supports therapeutic potential [0224] Recombinant human Decorin (rh-Decorin) has been shown to inhibit inflammation, glial scar formation and CSPG expression, and may promote axonal growth across the injury interface after acute spinal cord injury (Wu, Li et al.2013, Ahmed, Bansal et al.2014). These data show that Decorin treatment in animal models commenced immediately after spinal cord injury, inhibits TGF-β1/2-mediated invasion of inflammatory cells, scar deposition and cavitation and that later, during the consolidation phase, regulates ECM remodeling by both the induction of MMP and tissue plasminogen activator (tPA) activity and suppression of TIMP and PAI-1. Moreover, in Decorin-treated mature scars in which acute titers of TGF-f31/2 have declined, scar dissolution appears to be induced by MMP/tPA mediated fibrolytic activities and enhanced by depressed levels of TIMP and PAI-1 activity. [0225] Decorin suppressed acute scarring (fibrogenesis) and wound cavitation, and induced dissolution of mature scar tissue (fibrolysis) in dorsal funicular lesion (DFL) SCI model system of the spinal cord in adult rats (Wu, Li et al.2013, Ahmed, Bansal et al.2014). DFL cavity treatment
with recombinant Decorin suppresses inflammation and scar deposition in the acute and subacute phases of the CNS injury response in rat model of SCI and also contributes to dissolution of the mature scar following SCI. Decorin treatment of spinal cord injury (Esmaeili, Berry et al. 2014, Ahmed, Bansal et al.2014). [0226] Additionally, Decorin promoted axonal regrowth in both acute and chronic experiments. In both cases, axons were absent in PBS-treated DFL, but present in Decorin-treated DFL. [0227] OPC1 treatment in non-clinical models of SCI demonstrates similar results to that seen with Decorin treatment [0228] In five studies (Table 16) of OPC1 transplant into rodent models of SCI, a statistically significant reduction of cavitation area was observed in OPC1-treated animals, as compared to animals injected with control vehicle (HBSS or IsoLyte plus Human Serum Albumin). In these studies, axonal regrowth through the SCI lesion was seen in all OPC1- treated animals but not in the control animals. Tabulated results of these studies are shown below. The rat model of SCI injury that was used closely emulates the damage and outcomes seen in human after a contusion or crush injury of the cervical spinal cord. For rat model treatment time windows after SCI injury are defined as: Day 1-7: acute stage; Day 7-14: subacute stage; and over 14 days: chronic. [0229] Table 16. Summary of preclinical studies demonstrating similar results seen with Decorin treatment


[0230] Staining for the presence of myelinated axonal fibers performed in the first four studies listed above has shown the presence of myelinated axonal fibers traversing the lesion area in animals treated with OPC1 but not in the animal treated with the control. [0231] The results observed in the OPC1 animal studies demonstrate very similar anatomical outcomes to that seen in the studies where Decorin infused implants were transplanted into animals with spinal cord injuries as described above (Wu, Li et al. 2013, Ahmed, Bansal et al. 2014). Thus, the anatomical effects observed in the nonclinical efficacy studies of OPC1 transplantation into SCI injury may be attributed, at least in part, to the secretion of Decorin. [0232] Summary [0233] The current knowledge, as presented above, on the positive role that Decorin plays in attenuating the damage in the SCI cavity and the nonclinical studies results in Decorin-treated and OPC1-treated models of SCI justifies its utilization as a potency indicator for OPC1. It is projected that the ability of OPC1 cells to produce and secrete Decorin is one of the key therapeutic effects of OPC1, by positively modulating scarring and axon regrowth inhibiting processes. Therefore, we intend to use a qualified Decorin assay to be included in the panel of release testing for the new, improved OPC1 production process. [0234] References for Example 10: Ahmed, Z., D. Bansal, K. Tizzard, S. Surey, M. Esmaeili, A. M. Gonzalez, M. Berry and A. Logan (2014). "Decorin blocks scarring and cystic cavitation in acute and induces scar dissolution in chronic spinal cord wounds." Neurobiol Dis 64: 163-176. Bradbury, E. J. and E. R. Burnside (2019). "Moving beyond the glial scar for spinal cord repair." Nat Commun 10(1): 3879. Davies, J. E., X. Tang, J. C. Bournat and S. J. Davies (2006). "Decorin promotes plasminogen/plasmin expression within acute spinal cord injuries and by adult microglia in
vitro." J Neurotrauma 23(3-4): 397-408. Esmaeili, M., M. Berry, A. Logan and Z. Ahmed (2014). "Decorin treatment of spinal cord injury." Neural Regen Res 9(18): 1653-1656. Goncalves, M. B., Y. Wu, E. Clarke, J. Grist, C. Hobbs, D. Trigo, J. Jack and J. P. T. Corcoran (2019). "Regulation of Myelination by Exosome Associated Retinoic Acid Release from NG2- Positive Cells." J Neurosci 39(16): 3013-3027. Gubbiotti, M. A., S. D. Vallet, S. Ricard-Blum and R. V. Iozzo (2016). "Decorin interacting network: A comprehensive analysis of decorin-binding partners and their versatile functions." Matrix Biol 55: 7-21. Hill, L. J., R. J. A. Moakes, C. Vareechon, G. Butt, A. Ng, K. Brock, G. Chouhan, R. C. Vincent, S. Abbondante, R. L. Williams, N. M. Barnes, E. Pearlman, G. R. Wallace, S. Rauz, A. Logan and L. M. Grover (2018). "Sustained release of decorin to the surface of the eye enables scarless corneal regeneration." NPJ Regen Med 3: 23. Minor, K., X. Tang, G. Kahrilas, S. J. Archibald, J. E. Davies and S. J. Davies (2008). "Decorin promotes robust axon growth on inhibitory CSPGs and myelin via a direct effect on neurons." Neurobiol Dis 32(1): 88-95. Nastase, M. V., A. Janicova, H. Roedig, L. T. Hsieh, M. Wygrecka and L. Schaefer (2018). "Small Leucine-Rich Proteoglycans in Renal Inflammation: Two Sides of the Coin." J Histochem Cytochem 66(4): 261-272. Wu, L., J. Li, L. Chen, H. Zhang, L. Yuan and S. J. Davies (2013). "Combined transplantation of GDAs(BMP) and hr-decorin in spinal cord contusion repair." Neural Regen Res 8(24): 2236- 2248. Example 11 - Comparability of GPOR OPC1 Cells and LTCOPC1 OPC1 Cells [0235] Some of the process for making the cells and the OPC1 product, such as some of those used in the clinical studies described in the Examples herein, are referred to as Geron process and Geron cells or GPOR. The new processes described in this and other Examples herein are used for making the LCTOPC1 product. The LCTOPC1 process described herein is the process used for current GMP production of cells for clinical use. Data will be provided in this Example, supporting comparability between these manufacturing processes.
LIST OF ABBREVIATIONS ASIA American Spinal Injury Association Impairment bFGF Basic FGF BMP Bone Morphogenic Protein CMC Chemistry Manufacturing Controls CS10 CryoStor 10 DP Drug Product ECM Extracellular Matrix FCM Flow Cytometry GMP Good manufacturing Process GPM Glial Progenitor Medium GPOR Geron Process of Records hESC Human Embryonic Stem Cells hsFGF Heat-Stable FGF IPC In-process Controls MCB Master Cell Bank NB Neurobody NLI Neurological Level of Injury OCB Original Cell Bank OL Oligodendrocytes POC Proof-of-Concept QC Quality Control RA Retinoic Acid R&D Research and Develoment rhEGF Recombinant Human EGF RL Risk Level RMAT Regenerative Medicine Advanced Therapy SCI Spinal Cord Injury TAI Thaw-and-Inject UEMS Upper Extremity Motor Score WCB Working Cell Bank
[0236] LCTOPC1 (OPC1), previously referred to as GRNOPC1 and then AST-OPC1, is an oligodendrocyte progenitor cell population derived from the H1 hESC line intended for one-time administration for the treatment of subacute spinal cord injury (SCI). OPC1 has been shown in pre-clinical studies to produce neurotrophic factors, migrate in the spinal cord parenchyma, stimulate vascularization, and induce remyelination of denuded axons, all of which are essential functions of oligodendrocyte progenitors and are important for survival, regrowth and function of axons. [0237] Clinical evaluation of LCTOPC1 was initiated in 2010 by Geron Corporation. The first clinical trial was a Phase 1 safety study (NCT01217008) in which a low dose of 2 x 10
6 OPC1 cells was injected into the lesion site of subjects with subacute, neurologically complete thoracic spinal T3-T11 injuries. A total of 5 subjects out of the planned 8 received OPC1 as part of the original Phase 1 CP35A007 safety study from October 2010 through November 2011. [0238] In 2014, a Phase 1/2a study (NCT02302157) dose escalation of OPC1 in subjects with subacute sensorimotor complete (American Spinal Injury Association Impairment Scale A (ASIA Impairment Scale A)), Single Neurological Level (SNL) from C5 to C7 cervical spinal cord injuries was initiated, with the later expansion of the study to patients with a C4 Neurological Level of Injury (NLI) if the Upper Extremity Motor Score (UEMS) ≥ 1 and changing the dosing window from 14-30 days to 21-42 days post-spinal cord injury. A total of 25 subjects across 5 cohorts were enrolled in the AST-OPC-01 study and received a single administration of OPC1 cells delivered by intra-parenchymal injection into the spinal cord injury site using a Syringe Positioning Device, during a dedicated surgical procedure. The enrollment for AST-OPC-01 study was completed in December 2017 and reported in December 2020. [0239] Briefly, the origin of the new Master Cell Bank (MCB) is the H1 Bank Lot. No. MCBH101. MCBH101 was manufactured by Geron directly from the H1 Original Cell Bank (OCB) in 2009. It was manufactured in feeder-free conditions using well-defined raw materials, new culturing system and harvesting procedure, and cryopreserved by an hESC-customized cryopreservation process. In addition, the method for assessment of H1 hESC pluripotency was optimized. The new WCB originated from the new MCB and was expanded in tissue culture for 4 passages, while maintaining hESC characteristics, and then cryopreserved. The WCB will provide the starting material for LCTOPC1 manufacturing.
[0240] The purpose of this Example is also to present the scientific data generated during the development of LCTOPC1 CMC program. The provided information includes the development plans for LCTOPC1 with regards to preliminary comparability results based on R&D runs of the improved manufacturing process, comparability between the GPOR and LCT R&D manufactured material, introduction of a new proposed potency assay, review of the OPC1 safety status based on the GPOR in vivo data and reanalysis of GPOR lots, utilizing improved analytical methods. [0241] RATIONALE FOR PROCESS IMPROVEMENTS [0242] OPC1 is an investigational drug studied in a Phase 1 and a Phase 1/2a spinal injury clinical studies using OPC1 clinical lots produced by Geron Inc. Geron’s (GPOR) manufacturing process was originally developed in the early 2000s. At that time, well-defined and cell therapy grade reagents and materials were not widely available. As such, Stage 1 of the manufacturing process included the propagation of H1 embryonic cells on Matrigel
TM, an animal derived Extracellular Matrix (ECM), collagenase, and manual scraping of the culture dish surface for harvesting, passaging and expansion of the H1 embryonic stem cells. [0243] Furthermore, the GPOR manufacturing process was based on a poorly controlled differentiation process, driven by three guiding molecules. Most of the differentiation process occurred in cell aggregates starting directly from pluripotent H1 cells, in the form of Embryoid bodies (day 0 to day 26, Figure 10), which have a strong susceptible to spontaneous differentiation. From day 27 on, the differentiation was completed on Matrigel™ coated adherent surface for oligodendrocyte progenitor expansion and maturation. The GPOR manufacturing process had low yields, and key quality attributes defined by purity/impurity/non-targeted cell population markers exhibited limited reproducibility. Additionally, the final cryopreserved product required upon thawing, washing and formulation preparation prior to administration. [0244] The development of the improved manufacturing process focused on a more controlled directed differentiation of H1 towards OPC, guided by a specific sequence of growth factors and small molecules to inhibit or direct differentiation pathways using cell therapy grade materials when possible (as detailed in Figure 11). Moreover, the new process reduces the lengthy aggregate phase used by Geron, from 26 days directly from pluripotent cell state, which is prone to spontaneous aberrant differentiation, to 7 days, following 14 days of monolayer directed differentiation of H1 cells into neuroectoderm, reducing the possibility for spontaneous differentiation in the aggregates phase. The GPOR Vs. LCTOPC1 differentiation processes are summarized in Figure 10. The
biological rationale for the signaling sequence of inducing and inhibitory factors of the improved differentiation process is described in Figure 11. Additionally, new in-process controls (IPCs) were added to better monitor and characterize the differentiation process, as detailed in Figure 12. [0245] Materials used to manufacture of OPC1 cells (both the original GPOR and the modified processes) are summarized in Table 17. [0246] Table 17. Materials used during the production of OPC cells (GPOR and LCTOPC1 processes).

[0247] OVERVIEW OF THE LCTOPC1 MANUFACTURING PROCESS [
0248] Stage I - H1 Expansion [0249] Pluripotent H1 cells are thawed and cultured for 12-15 days on laminin-coated vessels in mTeSR Plus Medium. The cells are passaged and expanded using a non-enzymatic reagent ReLeSR (as described for the MCB and WCB hESC culturing). [0250] During the expansion, the cells are morphologically assessed, and at the end of 3 passages (before the initiation of differentiation process), hESC pluripotency is evaluated by flow cytometry-based [0251] Stage II - H1 Differentiation into OPC1 [0252] From day 0 of differentiation until the end of the process, the cells are cultured in Glial Progenitor Medium (GPM) – which is DMEM/F-12 supplemented with B27 and T3. [0253] Day 0-7 - on day 0, when the H1 culture reaches the required criteria which is defined by lactate concentration and cell morphology, the differentiation process is initiated by changing
the medium for the expanded pluripotent hESC cultured on laminin-coated vessels as follows. On days 0-3, GPM medium is supplemented with Retinoic Acid (RA), Dorsomorphin and PD0325901, in order to direct the differentiation process towards the neuroectoderm pathway (Kudoh, Wilson et al.2002). Dorsomorphin inhibits Bone Morphogenic Protein (BMP) signaling (SMAD pathway) and therefore inhibits mesoderm and trophoblast differentiation (Li and Parast 2014). PD0325901 inhibits downstream bFGF signaling at MEK1 and MEK2, and inhibits pluripotency and endoderm differentiation (Sui, Bouwens et al.2013). In summary, inhibition of pluripotency, endoderm, mesoderm and trophoblast formation in addition to activation of the RA signaling pathway, promotes neural tube (neuroectoderm) formation (Watabe and Miyazono 2009, Sui, Bouwens et al. 2013, Li and Parast 2014, Patthey and Gunhaga 2014, Janesick, Wu et al. 2015). On days 4-7, the culture is supplemented with Retinoic Acid and Ascorbic Acid to continue neuroectoderm differentiation induction (Duester 2008). [0254] Day 7-14 - On day 7 the cells are enzymatically harvested using TrypLE Select, and then seeded as a monolayer culture from day 7 to day 14 on laminin-coated vessels and cultured in GPM supplemented with rhEGF, hsFGF and ROCK inhibitor (ROCK Inhibitor only for the first 48 hours) (Hu, Du et al.2009, Patthey and Gunhaga 2014, Zheng, Li at al.2018). [0255] Day 14-21 - On Day 14, in order to promote neurobody (NB) aggregate formation, the cells are enzymatically harvested using TrypLE Select, and cultured for a week as a dynamic suspension culture in GPM supplemented with ROCK inhibitor (for the first 48 hours), and rhEGF and hs-rhFGF throughout. [0256] Day 21-42 - On Day 21 the aggregates are plated back as an adherent culture on laminin-coated vessels in GPM supplemented with rhEGF and PDGF (Ota and Ito 2006, Koch, Lehal et al.2013), and then on Day 28, the cells are harvested enzymatically using TrypLE Select, and expanded as an adherent culture on laminin-coated vessels in GPM supplemented with rhEGF and PDGF until days 35-42 for final expansion and maturation, with enzymatic passaging every ~7 days using TrypLE Select. [0257] At the end of the expansion process, the OPC1 cells are harvested using TrypLE Select and cryopreserved in CryoStor
®10 (CS10; BioLife Solutions, Inc.) cryopreservation solution as a Thaw-and-Inject (TAI) formulation. The LCTOPC1 production process flow is depicted in Figure 12.
[0258] In-Process Control tests are performed at every key step during the differentiation process of hESC to OPC1, as depicted in Figure 12. Biomarker proteins and mRNA expression are assessed using multicolor Flow Cytometry (FCM) and qPCR methods (respectively). The cells are tested for the expression of OPC1, epithelial, mesodermal, astrocytes and neuronal biomarkers, and residual hESC. In addition, viability, cell yield and metabolic activity (e.g., lactate) are assessed during the process. Lactate concentration is used as indicator for initiating differentiation starting on day 0, and on day 21 as a surrogate to cell counting in order to determine the surface area required for aggregate plating for pre-OPC generation and expansion. [0259] PROPOSED CMC COMPARABILITY TESTING [0260] OPC1 will be manufactured according to the improved process, released according to revised release parameters, and cryopreserved. LCTOPC1 DP will be compared to Geron’s manufactured representative batches and characterized with the updated analytical methods used for the release of the OPC1 manufactured via the new process. The plan will include testing of attributes used as release criteria for GPOR plus additional markers that were identified. The suggestion for comparison is based on quality attributes that characterize the Drug Product as described in Table 18. [0261] The side-by-side comparison between LCTOPC1 and GPOR OPC1 batches will be based on statistical analysis, calculating the expected range for quantitative measurements of the quality attributes from GPOR OPC1 batches. The values of those quality attributes measured in LCTOPC1 batches will be assessed in relation to those expected ranges for the quality attributes tested. The comparability data analysis is expected to establish reproducible release criteria for the LCTOPC1 process and demonstrate that LCTOPC1 has low batch to batch variability. [0262] The tested quality attributes will include viability, identity/purity, impurity/non- targeted population, gene profiling, and function/potency assays for 2-3 representative GPOR and LCT OPC1 batches each. [0263] Suggested comparability quality attributes are as follows: Viability - a critical quality attribute of any live cell drug product; Identity/Purity- assessment of characteristic oligodendrocyte progenitor cell protein markers: NG2, GD3, PDGFRα and PDGRFβ; Non- targeted cells population/impurities - (i) Residual H1 hESC from starting material - human embryonic stem cells protein markers TRA-1-60 and Oct-4 as a potential source for teratogenic agents combined in a multi-color Flow Cytometry test. TRA-1-60 and Oct-4 are commonly known
and used markers for embryonic stem cells and were used previously as an OPC1 release criteria, and (ii) Assessment of potential aberrant differentiation paths (Epithelial cells protein markers: Keratin 7, Claudin-6, EpCAM and CD49f known epithelial markers, Mesodermal cells protein markers CXCR4 and CD56 as known mesodermal and cartilage markers, Astrocytes cells protein marker GFAP as known astrocytes marker, Neuronal phenotype cells protein marker b-Tubulin 3 as known neuronal marker, Mesenchymal cells mRNA OLR1 that induces epithelial-mesenchymal transition, Endoderm cells mRNA markers of FOXA2, SOX17 and AFP as known endodermal markers, and does not include previously used Nestin and α-actinin attributes, since new data indicate that Nestin is not specific for OPC, but rather a marker for NSC and other cell types and α-actinin can be effectively replaced by combination of CXCR4/CD56. CXCR4 is expressed in definitive endoderm and mesoderm); In-vitro Cells Function/Potency- (i) Decorin secretion - a small secreted cellular matrix proteoglycan, as a potency indicator for OPC1. Decorin expressed by neurons and astrocytes in the central nervous system attenuates scar tissue formation, inhibits cavitation and promotes wound healing. The detailed rationale for the decorin secretion as a proposed potency assay is discussed in Example 10. (ii) OPC1 cells migration in response to platelet-derived growth factor-BB (PDGF-BB) which is important for cell motility at the injury site to ensure broadest anatomical coverage from a single injection location in the spine. (iii) Development of new potency test for assessment of the maturation and myelinization potential of OPC1. This assay is based on an essential function of OPC1 cells-remyelination of denuded axons. In this assay, OPC1 cells are thawed and plated in a specific media in a 3D tissue culture environment (e.g., Matrigel or Nanofiber tubes) that should induce the maturation of OPC1 into Oligodendrocytes (OL). [0264] The 3D environment nanotube mimics denuded axons in order to induce myelinization activity by OPC1 cells in a simple in-vitro setting. The assay will measure secretion of proteins associated with OL function (MBP and decorin) and will test OL protein markers (MBP, O4, MAG, MOG) expression by immunocytochemistry. The assay is currently being developed as a Proof-of-Concept (POC) and will be established if it proves to be robust enough. [0265] The proposed test panel to be used to examine GPOR OPC1 and LCTOPC1 along with proposed release criteria for LCTOPC1 can be seen below in Table 18.
[0266] Table 18. The proposed test panel and rationale used for process development, release and comparability.