WO2023080154A1 - 有害事象リスクの判定方法 - Google Patents
有害事象リスクの判定方法 Download PDFInfo
- Publication number
- WO2023080154A1 WO2023080154A1 PCT/JP2022/040978 JP2022040978W WO2023080154A1 WO 2023080154 A1 WO2023080154 A1 WO 2023080154A1 JP 2022040978 W JP2022040978 W JP 2022040978W WO 2023080154 A1 WO2023080154 A1 WO 2023080154A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- hadrus
- risk
- therapy
- bacteria
- specimen
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Images



Classifications
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/02—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving viable microorganisms
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/02—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving viable microorganisms
- C12Q1/04—Determining presence or kind of microorganism; Use of selective media for testing antibiotics or bacteriocides; Compositions containing a chemical indicator therefor
- C12Q1/06—Quantitative determination
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/02—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving viable microorganisms
- C12Q1/04—Determining presence or kind of microorganism; Use of selective media for testing antibiotics or bacteriocides; Compositions containing a chemical indicator therefor
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/68—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving nucleic acids
- C12Q1/6876—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes
- C12Q1/6888—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for detection or identification of organisms
- C12Q1/689—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for detection or identification of organisms for bacteria
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/569—Immunoassay; Biospecific binding assay; Materials therefor for microorganisms, e.g. protozoa, bacteria, viruses
- G01N33/56911—Bacteria
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/52—Predicting or monitoring the response to treatment, e.g. for selection of therapy based on assay results in personalised medicine; Prognosis
Definitions
- the present invention relates to a method for determining the risk of adverse events during multimodal therapy.
- Non-Patent Document 1 the development of febrile neutropenia by having patients take synbiotics during DCF therapy (three-drug combination therapy of docetaxel, cisplatin and 5-fluorouracil), which is preoperative chemotherapy for esophageal cancer and severe diarrhea are reported to be remarkably alleviated.
- preventive measures such as consideration of the amount of anticancer drugs to be used and concomitant use of synbiotics can be considered in advance.
- Anaerostipes hadrus is one of the dominant bacteria in the intestine, and is known as a bacterium that uses lactic acid and acetic acid in the intestine to produce butyric acid.
- A. Deletion of hadrus inositol catabolism/butyrate biosynthetic pathway has been reported to be associated with increased host body weight and metabolic disease risk (Non-Patent Document 2).
- Non-Patent Document 2 A.I. The relationship between hadrus and adverse events during treatments such as chemotherapy is unknown.
- Motoori M et al. Clin Nutr, 2017, 36: 93-99 Zeevi D, et al. Nature, 2019, 568: 43-48
- an object of the present invention is to provide a method for determining the risk of adverse events during multimodal therapy.
- Anaerostipes hadrus which is a type of intestinal bacteria, and the occurrence or severity of adverse events during treatment.
- Anaerostipes hadrus as an index, it was found that the risk of adverse events during combined modality therapy can be determined.
- the present invention provides the following [1] to [12].
- [1] A method for determining the risk of adverse events during combined modality therapy, including measuring Anaerostipes hadrus in a specimen collected from a subject.
- [2] The method of [1], wherein the adverse event risk is the risk of onset or aggravation of an adverse event.
- [3] The method of [1] or [2], wherein the multimodal therapy is a therapy selected from drug therapy, surgical therapy, radiation therapy, and a combination thereof.
- [4] The method of any one of [1] to [3], wherein the multidisciplinary treatment is drug therapy.
- [5] The method of any one of [1] to [4], wherein the adverse event is at least one selected from the group consisting of febrile neutropenia and diarrhea.
- [6] The method of any one of [1] to [5], wherein the specimen is a stool specimen from a subject.
- [7] Comparing the number of Anaerostipes hadrus bacteria in the specimen with a reference value, and determining that the risk of adverse events during combined modality treatment is high when the number of bacteria is equal to or less than the reference value, [1 ] to [6].
- the present invention it is possible to easily determine the risk of developing adverse events or the risk of aggravation during multidisciplinary therapy. This makes it possible to take measures against adverse events, such as selection of treatment to be implemented, adjustment of drug dosage, and preventive measures for adverse events, according to the level of risk, and selection of the appropriate treatment regimen for each individual patient. It becomes possible.
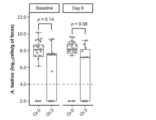
- Gr. 0 refers to patients who did not develop febrile neutropenia
- Gr. 3 indicates a patient who developed febrile neutropenia.
- Baseline indicates before the DCF therapy, and Day 8 indicates the 8th day of the first course of the DCF therapy. *p ⁇ 0.05, **p ⁇ 0.01.
- Gr. 0 refers to patients who did not develop febrile neutropenia; Gr.
- Anaerostipes hadrus (Eubacterium hadrum) is a Gram-positive bacterium and a type of human intestinal bacterium. As used herein, “Anaerostipes hadrus” means bacteria belonging to Anaerostipes hadrus.
- multimodal therapy includes drug therapy using agents such as anticancer drugs, surgical therapy such as surgery, radiotherapy, and combinations thereof.
- surgical therapy such as surgery, radiotherapy, and combinations thereof.
- at the time of treatment includes both during and after treatment.
- the term "adverse event” refers to an undesirable or unintended sign, symptom, or illness that occurs in a patient during or after treatment, regardless of whether or not it is causally related to the treatment.
- adverse events and their severity for example, Common Terminology Criteria for Adverse Events (CTCAE) v4.0 published by the National Cancer Institute (NCI) Adverse events included and their grades are listed.
- Grade 1 mild; no symptoms or mild symptoms; clinical or laboratory findings only; no treatment required.
- Grade 2 Moderate; minimal/local/non-invasive treatment required; age-appropriate limitation of activities of daily living except self care.
- Grade 3 Severe or medically significant, but not immediately life-threatening; hospitalization or extended hospitalization required; inactivity/incapacity; limitation of self-care activities of daily living.
- Grade 4 life-threatening; urgent treatment required.
- Grade 5 Death due to adverse events. In the present specification, no onset is defined as grade 0.
- adverse event risk refers to the risk of developing an adverse event or the risk of aggravating an adverse event.
- Adverse event risk refers to the possibility of developing an adverse event. That is, that an individual belongs to a high-risk group means that the individual is expected to have a high probability of developing an adverse event, and that an individual belongs to a low-risk group means that the individual has an adverse event It means that it is expected that the possibility of developing
- adjuvantavation risk refers to the possibility of an adverse event being aggravated. That is, when an individual belongs to a high-risk group, it means that the individual is expected to develop an adverse event and the adverse event is likely to be severe, and the individual belongs to a low-risk group. By is meant that the individual is unlikely to develop an adverse event or, if the individual does develop an adverse event, the adverse event is expected to be unlikely to be severe.
- determination includes the concepts of “detection”, “examination”, “measurement”, “prediction” or “diagnosis”, but does not include medical practice such as diagnosis by a doctor .
- Anaerostipes hadrus in the specimen is used as an index.
- the method detects the presence of A. Including measuring hadrus. Specifically, the method detects A. including measuring the number of S. hadrus.
- the method comprises determining the amount of A. in total bacteria in a specimen taken from a subject. Including measuring hadrus occupancy.
- the occupancy rate of A. hadrus is the total number of bacteria in the sample. means the ratio of the number of A. hadrus bacteria in the intestinal flora of the subject from whom the specimen was derived. This value corresponds to the occupancy rate of hadrus.
- Subjects are not particularly limited, but those that require assessment of adverse event risk during combined modality therapy, such as patients scheduled to receive combined modality therapy, patients receiving combined modality therapy, etc. .
- Examples of the specimen include biological samples derived from a subject, such as intestinal juice, feces, and other gastrointestinal tract contents.
- the means for measuring the number of A. hadrus bacteria is not particularly limited, but A. hadrus is preferably used. Based on the nucleotide sequence of the 16S rRNA gene of hadrus, for example, RT-PCR method, sequencing method, etc., can be used for measurement, and among these, RT-PCR method is more preferable.
- the analysis method using the RT-PCR method includes, for example, (1) a step of extracting RNA of intestinal bacteria in a sample, (2) synthesizing cDNA from the extracted RNA by reverse transcription; It can be performed by a step of performing PCR using a nucleic acid fragment (primer) that hybridizes to hadrus-derived cDNA, and (3) a step of detecting the DNA fragment amplified in step (2).
- amplification reaction By performing an amplification reaction by combining the above nucleic acid fragment with template cDNA derived from a sample, A.
- a DNA fragment (PCR product) specific to H. hadrus can be obtained.
- A It becomes possible to quantify the number of bacteria of Hadrus.
- Observation of the amplified PCR product over time can be performed by labeling the PCR product with an intercalating fluorescent dye such as SYBR (registered trademark) Green I and measuring the fluorescence intensity at each PCR step.
- Intercalating dyes have the property of increasing fluorescence intensity by intercalating with double-stranded nucleic acids. PCR products generated by PCR reaction from hadrus cDNA can be accurately measured, and SYBR Green I is particularly preferably used.
- Cq value the number of PCR cycles
- DNA amount the number of PCR cycles
- Cq value the number of PCR cycles
- Molecular Beacon or the like labeled with a fluorescent dye
- TaqMan probes and Molecular Beacons are probes in which a fluorescent dye and a quencher are bound to an oligonucleotide having homology to the internal sequence of the region amplified by PCR, and are used together in the PCR reaction. Since the fluorescent dye bound to the probe interacts with the quencher to emit fluorescence corresponding to the PCR amplification reaction, the amplified PCR product can be observed over time by measuring the fluorescence intensity at each PCR step. can.
- the number of hadrus bacteria can be obtained from a calibration curve of the logarithmic value of the number of bacteria measured by the DAPI counting method, the culture method, or the like, and the Cq value. That is, A. A standard curve was prepared in advance by plotting the logarithm of the number of A. hadrus bacteria on the horizontal axis and the Cq value on the vertical axis. Hadrus counts are measured.
- A.A. in the specimen In the measurement of the number of A. hadrus bacteria, A. A. hadrus on the 16S rRNA gene. It is conserved within the species A. hadrus. Primers that can specifically hybridize and amplify regions that are not conserved in species other than hadrus may be used. A. Primers for counting hadrus bacteria are not limited to these, but for example, the primers of SEQ ID NOs: 3 and 4 can be used.
- the means for measuring the occupancy rate of hadrus is not particularly limited, but preferable examples include means for measuring by RT-PCR method, sequencing method, etc., based on the nucleotide sequence of the 16S rRNA gene of enterobacteria. Of these, it is more preferable to measure by a sequencing method (eg, 16S rRNA gene amplicon analysis).
- 16S rRNA gene amplicon analysis includes, for example, (1) a step of extracting the genomic DNA of the intestinal bacterium in the specimen, (2) using the extracted genomic DNA as a template, a nucleic acid that hybridizes to the 16S rRNA gene of the intestinal bacterium. (3) determining the base sequence of the DNA fragment amplified in step (2); and (4) analyzing the sequence data obtained in step (3). It can be performed according to the process.
- a DNA fragment (PCR product) derived from the 16S rRNA gene of intestinal bacteria can be obtained by combining the nucleic acid fragment with template genomic DNA derived from a specimen and performing an amplification reaction.
- the sequence data is compiled as an amplicon sequence variant (ASV), and compared with a known database to assign phylogenetic information to each ASV.
- ASV amplicon sequence variant
- the region of the intestinal bacterium 16S rRNA gene amplified by PCR is a region amplified using primers that hybridize to a conserved region that is universally conserved among bacterial species, and It is preferably a region containing a variable region that is not conserved among bacterial strains and is rich in variation.
- the variable region includes at least one of the V1 to V9 regions of the 16s rRNA gene, preferably a region containing V1 and V2 or a region containing V3 and V4.
- the primers may optionally contain adapter sequences for sequencing and/or index sequences for sample identification. Examples of such primers include universal primers for amplifying bacterial 16S rRNA genes that are commonly used in this field. For example, the primers of SEQ ID NOS: 1 and 2 can be used.
- the base sequence of the amplified PCR product can be determined by a known method, but can be rapidly sequenced using a next-generation sequencer such as the MiSeq platform (Illumina). Sequence data analysis can be performed using analysis software such as QIIME2 (Quantitative Insights Into Microbial Ecology 2), and sequence errors can be removed using QIIME2's DADA2 (Divisive Amplicon Denoising Algorithm 2) plug-in. can be done. The obtained sequence data can be classified into ASVs based on sequence identity, and the attribution of each ASV to a bacterial species can be determined with reference to known databases such as SILVA and Greengenes. From the abundance ratio corresponding to each ASV species determined in this way and the number of sequence reads, A. . The hadrus occupancy can be calculated.
- Non-Patent Document 1 Lacticaseibacillus paracasei strain Shirota ( LcS) and Bifidobacterium breve strain Yakult (BbrY) (Bifidobacterium breve YIT 12272 (FERM BP-11320)) using galacto-oligosaccharides as prebiotics.
- LcS is Lactobacillus casei YIT9029 (FERM BP-1366 ), and was deposited on January 12, 1981 at the National Institute of Advanced Industrial Science and Technology Patent Organism Depositary Center (currently the National Institute of Technology and Evaluation, Patent Microorganism Depositary Center).
- A. hadrus can be used as an index for determining the risk of adverse events not only during drug therapy such as DCF therapy but also during combined modality therapy.
- Multimodality therapy includes drug therapy, surgical therapy, radiation therapy, and combinations thereof, preferably drug therapy, more preferably drug therapy using an anticancer agent, still more preferably docetaxel, Drug therapy (DCF therapy) using cisplatin and 5-fluorouracil.
- DCF therapy is known as one of the therapeutic methods for esophageal cancer.
- the adverse events subject to risk assessment are not particularly limited, and examples include blood and lymphatic disorders, heart disorders, ear and labyrinth disorders, endocrine disorders, eye disorders, gastrointestinal disorders, general/systemic disorders, and administration site disorders.
- the method of the present invention is preferably used to determine the risk of at least one type of adverse event selected from the group consisting of blood and lymphatic disorders and gastrointestinal disorders, specifically febrile neutropenia and diarrhea At least one risk determination selected from the group consisting of, that is, at least one risk determination selected from the group consisting of febrile neutropenia risk and diarrhea risk.
- the severity of febrile neutropenia is classified into the following grades according to CTCAE v4.0.
- Grade 1 - (not defined)
- Grade 2 - (not defined)
- Grade 3 Fever of ⁇ 38.0°C with absolute neutrophil count ⁇ 1,000/mm 3 and >38.3°C at any one time or lasting >1 hour.
- Grade 4 life-threatening; urgent treatment required.
- Grade 5 Death According to CTCAE v4.0, the severity of diarrhea is classified into the following grades.
- the baseline refers to the defecation habit (number of defecations) in daily life.
- Grade 1 ⁇ 4 stools/day increase over baseline; mild increase in colostomy output over baseline.
- Grade 2 4-6 stools/day increase over baseline; moderate increase in colostomy output over baseline.
- Grade 3 7 or more stools/day increase over baseline; fecal incontinence; hospitalization required; highly increased colostomy output over baseline; limitation of self-care activities of daily living.
- Grade 4 life-threatening; urgent treatment required.
- Grade 5 Death
- the risk of adverse events during combined modality therapy is determined by the amount of A.
- the number of hadrus bacteria may be used as an index for determination. Specifically, the amount of A. The lower the number of A. hadrus bacteria, the higher the risk of adverse events during combined modality therapy. It can be determined that the greater the number of hadrus bacteria, the lower the risk of adverse events during combined modality therapy. Such risk determination is based on the presence of A. It is preferable to compare the number of hadrus bacteria with a preset reference value (cutoff value) according to the level of risk. For example, the reference value is set in advance by A.
- ROC Receiver Operating Characteristic
- the risk of developing adverse events during combined modality therapy is determined by the amount of A.
- the number of hadrus bacteria may be used as an index for determination. Specifically, the amount of A. The lower the number of A. hadrus bacteria, the higher the risk of developing adverse events during multidisciplinary treatment. It can be determined that the greater the number of hadrus bacteria, the lower the risk of developing adverse events during combined modality therapy. Such risk determination is based on the presence of A. It is preferable to compare the number of hadrus bacteria with a preset reference value according to the level of risk. The reference value can be appropriately set by those skilled in the art as described above. A.
- the number of hadrus bacteria When the number of hadrus bacteria is equal to or less than the reference value, it can be determined that the risk of developing adverse events during combined modality therapy is high. On the other hand, A. When the number of hadrus bacteria is greater than the reference value, it can be determined that the risk of developing adverse events during combined modality therapy is low. In one example, if the adverse event is febrile neutropenia, the amount of A. When the number of A. hadrus bacteria is 10 7.7 or less per 1 g of the sample, it can be determined that the risk of developing febrile neutropenia during combined modality therapy is high. When the number of hadrus bacteria is more than 10 7.7 per 1 g of the specimen, it can be determined that the risk of developing febrile neutropenia during combined modality therapy is low.
- the amount of A if the adverse event is diarrhea, the amount of A.
- the number of A. hadrus bacteria per 1 g of the specimen is 10 7.6 or less, it can be determined that the risk of developing diarrhea during multidisciplinary treatment is high.
- the number of hadrus bacteria is more than 10 7.6 per 1 g of the sample, it can be determined that the risk of developing diarrhea during combined modality therapy is low. Determination of the risk of developing adverse events during combined modality therapy is particularly suitably applied when the adverse event is febrile neutropenia.
- the risk of aggravation of adverse events during combined modality therapy is determined by the amount of A.
- the number of hadrus bacteria may be used as an index for determination. Specifically, the amount of A. The lower the number of A. hadrus bacteria, the higher the risk of aggravation of adverse events during multidisciplinary treatment. It can be determined that the greater the number of hadrus bacteria, the lower the risk of aggravation of adverse events during combined modality therapy. Such risk determination is based on the presence of A. It is preferable to compare the number of hadrus bacteria with a preset reference value according to the level of risk. The reference value can be appropriately set by those skilled in the art as described above. A.
- the number of hadrus bacteria When the number of hadrus bacteria is equal to or less than the reference value, it can be determined that the risk of aggravation of adverse events during combined modality therapy is high. On the other hand, A. When the number of hadrus bacteria is greater than the reference value, it can be determined that the risk of aggravation of adverse events during combined modality therapy is low. In one example, if the adverse event is febrile neutropenia, the amount of A. When the number of A. hadrus bacteria is 10 7.7 or less per 1 g of the specimen, it can be determined that the risk of aggravation of febrile neutropenia during combined modality therapy is high, and A. hadrus bacteria in the specimen is high.
- the number of hadrus bacteria is more than 10 7.7 per 1 g of the sample, it can be determined that the risk of aggravation of febrile neutropenia during combined modality therapy is low. More specifically, the amount of A. If the number of hadrus bacteria is 10 7.7 or less per 1 g of the specimen, it can be determined that febrile neutropenia during combined modality treatment is likely to be equivalent to grade 3 above, and A . When the number of hadrus bacteria is more than 10 7.7 per 1 g of the specimen, it can be determined that febrile neutropenia during combined modality treatment is highly likely to correspond to grade 0 above. In another example, if the adverse event is diarrhea, the amount of A. When the number of A.
- hadrus bacteria per 1 g of the specimen is 10 7.6 or less, it can be judged that the risk of severe diarrhea during multimodal treatment is high, and the A. hadrus bacteria count in the specimen is high. When the number of hadrus bacteria per 1 g of the specimen is more than 10 7.6 , it can be determined that the risk of severe diarrhea during multimodality therapy is low. More specifically, the amount of A. If the number of hadrus bacteria is 10 7.6 or less per 1 g of the specimen, it can be determined that the diarrhea during multimodal treatment is likely to be equivalent to grade 3 or higher, for example, grade 3 to 4. A.
- the risk of adverse events during combined modality therapy is determined by A.
- the hadrus occupancy rate may be used as an index for determination. Specifically, the A. The lower the occupancy of hadrus, the higher the risk of adverse events during combined modality therapy, and the higher the risk of A. It can be determined that the higher the hadrus occupancy, the lower the risk of adverse events during combined modality therapy. Such risk determination is based on the A. It is preferable to compare the occupancy rate of hadrus with a preset reference value according to the level of risk. The reference value is, for example, previously determined by the total bacterial A.
- ROC Receiver Operating Characteristic
- the risk of developing adverse events during multimodal therapy is determined by the amount of A.
- the occupancy rate of hadrus may be used as an index for determination. Specifically, the A. The lower the occupancy of hadrus, the higher the risk of developing adverse events during multimodal therapy, and the higher the risk of developing adverse events during multimodal therapy, and the higher the A. It can be determined that the higher the occupancy rate of hadrus, the lower the risk of developing adverse events during combined modality therapy. Such risk determination is based on the A. It is preferable to compare the occupancy rate of hadrus with a preset reference value according to the level of risk. The reference value can be appropriately set by those skilled in the art as described above. A. in total bacteria in the specimen.
- the occupancy rate of hadrus When the occupancy rate of hadrus is equal to or less than the reference value, it can be determined that the risk of developing adverse events during combined modality therapy is high. On the other hand, A. in the total bacteria in the specimen When the hadrus occupancy rate is higher than the reference value, it can be determined that the risk of developing adverse events during combined modality therapy is low. In one example, if the adverse event is febrile neutropenia, A. When the occupancy rate of hadrus was 0.25% or less, the risk of developing febrile neutropenia during combined modality therapy was high, and A. When the occupancy rate of hadrus is higher than 0.25%, it can be determined that the risk of developing febrile neutropenia during combined modality therapy is low.
- the total bacteria in the specimen are A.
- the occupancy rate of hadrus was 0.084% or less, the risk of developing diarrhea during multimodal treatment was high, and A.
- the occupancy rate of hadrus is higher than 0.084%, it can be determined that the risk of developing diarrhea during combined modality therapy is low. Determination of the risk of developing adverse events during combined modality therapy is particularly suitably applied when the adverse event is febrile neutropenia.
- the risk of aggravation of adverse events during multimodal therapy is determined by the total bacteria in the sample.
- the occupancy rate of hadrus may be used as an index for determination. Specifically, the A. The lower the occupancy of hadrus, the higher the risk of exacerbation of adverse events during combined modality therapy, and the higher the risk of aggravation of adverse events during combined modality treatment, and the higher the risk of A. It can be determined that the higher the occupancy rate of hadrus, the lower the risk of exacerbation of adverse events during combined modality therapy. Such risk determination is based on the A. It is preferable to compare the occupancy rate of hadrus with a preset reference value according to the level of risk.
- the reference value can be appropriately set by those skilled in the art as described above.
- the occupancy rate of hadrus When the occupancy rate of hadrus is higher than 0.25%, it can be determined that the risk of aggravation of febrile neutropenia during combined modality therapy is low. More specifically, A . When the occupancy rate of hadrus is 0.25% or less, it can be determined that febrile neutropenia during combined modality treatment is likely to be equivalent to Grade 3, and A. When the occupancy rate of hadrus is higher than 0.25%, it can be determined that febrile neutropenia during combined modality treatment is highly likely to correspond to Grade 0 above. In another example, if the adverse event is diarrhea, the total bacteria in the specimen are A. When the occupancy rate of hadrus is 0.084% or less, it can be determined that the risk of diarrhea aggravation during multimodal treatment is high, and A.
- the occupancy rate of hadrus is higher than 0.084%, it can be determined that the risk of aggravation of diarrhea during combined modality therapy is low. More specifically, A .
- the occupancy rate of hadrus is 0.084% or less, it can be determined that the diarrhea during multimodal treatment is likely to be equivalent to grade 3 or higher, for example grade 3 to 4, and the total bacteria in the specimen A.
- the occupancy rate of hadrus is higher than 0.084%, it can be determined that diarrhea during multimodal therapy is highly likely to correspond to grade 0 to 2 above. Determination of the risk of exacerbation of adverse events is particularly preferably applied when the adverse event is diarrhea.
- the method of the present invention is preferably carried out before combined modality therapy or at the beginning of combined modality therapy (for example, during one course of multimodal therapy including multiple courses or after completion of one course), and before combined modality therapy It is more preferable to implement
- the risk of adverse events during multidisciplinary treatment can be determined early, especially before treatment, so that it is possible to make a more appropriate treatment plan for each individual patient, and thus the patient's It leads to improvement of quality of life and treatment effect.
- Patients determined to have a low risk of adverse events during combined modality therapy according to the method of the present invention can be administered planned combined modality therapy, and adverse events during combined modality therapy can be Patients determined to be at high risk can be treated to prevent or alleviate adverse events, such as reducing drug doses and concomitant use of synbiotics.
- kits containing a protocol for measuring hadrus are used.
- the kit includes A. Reagents and protocols for measuring A. hadrus (methods for measuring A. hadrus, criteria for judging the risk of adverse events during combined modality therapy, factors affecting measurement results and the extent of their effects, etc. are described) included. Such criteria can be used to determine as in the method described above.
- the "variation in the number of bacteria" used as an index means that A.C.
- the number of A. hadrus bacteria increased, the number of A.
- the increase in the number of A. hadrus bacteria was promoted, A.
- This concept includes the case where the decrease in the number of hadrus bacteria is suppressed. That is, in vitro or in vivo, A.
- a test substance that increases the number of hadrus bacteria, promotes an increase in the number of bacteria, or suppresses a decrease in the number of bacteria is judged to have the effect of reducing the risk of adverse events during multimodal therapy.
- the "variation in occupancy rate" used as an index means that the A.D.
- a test substance that increases hadrus occupancy, promotes an increase in occupancy, or inhibits a decrease in occupancy is judged to have an effect of reducing the risk of adverse events during combined modality therapy.
- a test substance is administered to a human or an experimental animal such as a mouse, rat or rabbit, and compared with an unadministered human or experimental animal. Determine whether or not to change the number of hadrus bacteria or the occupancy rate.
- the test substance is A.
- the test substance was treated as an agent for reducing the risk of adverse events during multimodal therapy.
- the test substance is A.
- the test substance was treated as an agent for reducing the risk of adverse events during multimodality therapy. available as
- Example 1 1. Method (1) Subjects for analysis Eighty-one patients with esophageal cancer between the ages of 20 and 80 who were scheduled to receive preoperative chemotherapy were enrolled in the study. Of these, 73 subjects (38 in the prophylactic antibiotic administration group and 35 in the synbiotics administration group) whose feces were collected both at the time of registration and on the 8th day after the start of DCF therapy were analyzed. Consent to participate in the study was obtained by consent form prior to participation from all patients who participated in the study.
- Lacol NF-containing enteral liquid (Otsuka Pharmaceutical Factory Co., Ltd.) to 600 mL per day, 3 days before the start of chemotherapy 1 course Lacticaseibacillus paracasei strain Shirota (Lacticaseibacillus paracasei YIT 9029: LcS) as a probiotic until the end of chemotherapy (Lactobacillus casei YIT 902 before the 2020 Lactobacillus reclassification) 9 (FERM BP-1366)) and Bifidobacterium breve strain Yakult ( BbrY) (Bifidobacterium breve YIT 12272 (FERM BP-11320)) containing 3 ⁇ 10 8 cells or more of each of the viable bacteria Yakult BL antiflatulent drug (Yakult Honsha Co., Ltd.) 3 g per day, Oligomate S- as a prebiotic 15 mL
- RNA extraction 40 ⁇ L of fecal suspension was transferred to a new 2 mL tube containing 1 mL PBS, centrifuged (4° C., 13,000 ⁇ g, 5 minutes), and the supernatant was removed by decantation. bottom. This pellet was stored at -80°C until RNA extraction.
- 200 ⁇ L of suspension was transferred to a new 2 mL tube with 1 mL of PBS and vortexed. After centrifugation (4° C., 13,000 ⁇ g, 5 minutes), 1 mL of the supernatant was removed. After adding 1 mL of PBS again, suspending and centrifuging (4° C., 13,000 ⁇ g, 5 minutes), 1 mL of the supernatant was removed. The resulting 200 ⁇ L suspension was stored at ⁇ 30° C. until DNA extraction.
- 16S rRNA gene amplicon analysis by next-generation sequencer DNA was extracted from stool samples using QIAamp DNA Stool Mini Kit (QIAGEN GmbH) according to the manual. 16S rRNA gene amplicon analysis was performed as follows. The V1-V2 region of the 16S rRNA gene of each sample was amplified with the ABI 7500 Real-Time PCR System (Thermo Fisher Scientific) using 27Fmod2 forward and 338R reverse primers (SEQ ID NOs: 1 and 2).
- PCR reaction solution 50 ⁇ L
- 2 ⁇ SYBR Premix Ex Taq II 50 ⁇ L, Takara Bio
- Nuclease-Free Water 22 ⁇ L
- each primer 100 nM, 1 ⁇ L
- template DNA 10 ng/mL, 1 ⁇ L
- the PCR reaction was carried out under the conditions of 25 cycles of 95°C for 5 seconds, 55°C for 30 seconds, and 72°C for 40 seconds.
- Amplification products were purified with the AMPure XP Kit (Beckman Coulter Genomics) and quantified with the Quant-iT PicoGreen dsDNA Kit (Invitrogen).
- a primer set (SEQ ID NOs: 3 and 4) was designed consisting of an AH7F forward primer and an AH1R reverse primer specific for the hadrus 16S rRNA gene. Using the primer set, cultured A . Quantitative RT-PCR was performed using RNA extracted from hadrus as a template. Qiagen OneStep RT-PCR kit (Qiagen) was used for quantitative RT-PCR.
- PCR reaction solution (10 ⁇ L), 1 ⁇ Qiagen Onestep RT-PCR Buffer (2 ⁇ L), 0.5 ⁇ Q-solution (2 ⁇ L), dNTP Mixture (400 ⁇ M each), 100,000-fold diluted SYBR Green I (Molecular Probes ), Qiagen OneStep RT-PCR enzyme mix (0.4 ⁇ L), AH7F forward primer and AH1R reverse primer (0.6 ⁇ M), and template RNA (5 ⁇ L) were mixed.
- the RT-PCR reaction was heated at 50°C for 30 minutes to perform reverse transcription, heated at 95°C for 15 minutes for initial denaturation, and 40 seconds at 94°C for 5 seconds, 55°C for 30 seconds, and 72°C for 50 seconds.
- AGPC acid guanidinium thiocyanate-phenol-chloroform extraction
- the A. Species-specific primers SEQ ID NOS: 3 and 4
- Threshold cycle (Cq) values in the linear range of the assay were imputed into the standard curve to determine the corresponding bacterial counts in each sample. From this, the number of bacteria in each sample was determined.
- the standard curve is for the standard strain A. spp., which has already been counted by Cq value and DAPI staining.
- a dilution series of hadrus YIT10092 T DSM3319 T ) was used.
- the limit of detection (LOD) was the smallest number of bacteria in the standard curve (10 -2 cells/reaction).
- RT-qPCR products (10 ⁇ L) were purified by MultiScreen® Filter Plate (Merck Millipore). Cycle sequencing reactions were performed using the BigDye® Terminator version 3.1 Cycle Sequencing kit (Applied Biosystems) according to the manufacturer's manual. Amplification products were purified by ethanol precipitation, dissolved in formamide (1 ⁇ L), denatured, and sequenced using an ABI PRISM 3130 Genetic Analyzer (Applied Biosystems). Comparison of the resulting rRNA sequences for assignment to specific species was performed using NCBI's BLAST program (http://blast.ncbi.nlm.nih.gov/Blast.cgi).
- A. Changes in A. hadrus counts A. hadrus in feces before DCF therapy. There was no significant difference in the number of hadrus bacteria between the Antibiotics group and the Synbiotics group. Eight days after the start of DCF therapy, A.C. A tendency toward a decrease in the number of A. hadrus bacteria (p 0.11) was observed, but in the Synbiotics group, A. hadrus bacteria decreased after DCF therapy. No decrease in the number of Hadrus bacteria was observed. With DCF therapy and administration of prophylactic antibiotics, A. Although the number of hadrus bacteria decreased, such a decrease in the number of bacteria was suppressed by oral administration of synbiotics.
- the cut-off value for the number of hadrus bacteria was calculated by receiver operating characteristic (ROC) analysis.
- ROC receiver operating characteristic
- the cut-off value was 10 7.7 per 1 g of specimen.
- A. Hadrus can be used to determine the risk of adverse events during multimodality therapy, particularly during drug therapy.
Landscapes
- Chemical & Material Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Health & Medical Sciences (AREA)
- Engineering & Computer Science (AREA)
- Organic Chemistry (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Immunology (AREA)
- Zoology (AREA)
- Wood Science & Technology (AREA)
- Molecular Biology (AREA)
- Analytical Chemistry (AREA)
- Physics & Mathematics (AREA)
- Microbiology (AREA)
- Biotechnology (AREA)
- General Health & Medical Sciences (AREA)
- Biochemistry (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Biophysics (AREA)
- Genetics & Genomics (AREA)
- General Engineering & Computer Science (AREA)
- Hematology (AREA)
- Biomedical Technology (AREA)
- Urology & Nephrology (AREA)
- Toxicology (AREA)
- Food Science & Technology (AREA)
- Cell Biology (AREA)
- Medicinal Chemistry (AREA)
- General Physics & Mathematics (AREA)
- Pathology (AREA)
- Virology (AREA)
- Tropical Medicine & Parasitology (AREA)
- Measuring Or Testing Involving Enzymes Or Micro-Organisms (AREA)
Abstract
Description
〔1〕被験者より採取した検体中のAnaerostipes hadrusを測定することを含む、集学的治療時の有害事象リスクの判定方法。
〔2〕有害事象リスクが有害事象の発症リスク又は重症化リスクである、〔1〕記載の方法。
〔3〕集学的治療が薬物療法、外科療法、放射線治療、及びその組み合わせから選択される治療である、〔1〕又は〔2〕記載の方法。
〔4〕集学的治療が薬物療法である、〔1〕~〔3〕のいずれかに記載の方法。
〔5〕有害事象が発熱性好中球減少症及び下痢からなる群より選択される少なくとも1種である、〔1〕~〔4〕のいずれかに記載の方法。
〔6〕検体が被験者の糞便検体である、〔1〕~〔5〕のいずれかに記載の方法。
〔7〕検体中のAnaerostipes hadrusの菌数を基準値と比較し、菌数が基準値以下である場合に、集学的治療時の有害事象リスクが高いと判定することをさらに含む、〔1〕~〔6〕のいずれかに記載の方法。
〔8〕検体中の総細菌におけるAnaerostipes hadrusの占有率を基準値と比較し、占有率が基準値以下である場合に、集学的治療時の有害事象リスクが高いと判定することをさらに含む、〔1〕~〔6〕のいずれかに記載の方法。
〔9〕検体中のAnaerostipes hadrusの菌数が、検体1gあたり、107.7個以下であるか、検体中の総細菌におけるAnaerostipes hadrusの占有率が0.25%以下である場合に、集学的治療時の発熱性好中球減少症リスクが高いと判定することをさらに含む、〔1〕~〔6〕のいずれかに記載の方法。
〔10〕検体中のAnaerostipes hadrusの菌数が、検体1gあたり、107.6個以下であるか、検体中の総細菌におけるAnaerostipes hadrusの占有率が0.084%以下である場合に、集学的治療時の下痢リスクが高いと判定することをさらに含む、〔1〕~〔6〕のいずれかに記載の方法。
〔11〕検体中のAnaerostipes hadrusの測定試薬及びプロトコールを含む、〔1〕~〔10〕のいずれかに記載の方法を実施するためのキット。
〔12〕Anaerostipes hadrusの菌数又は占有率を指標とする、集学的治療時の有害事象リスクの低減剤のスクリーニング方法。
本明細書において、「治療時」には治療中及び治療後を包含する。
グレード1:軽症;症状がない、又は軽度の症状がある;臨床所見又は検査所見のみ;治療を要さない。
グレード2:中等症;最小限/局所的/非侵襲的治療を要する;年齢相応の身の回り以外の日常生活動作の制限。
グレード3:重症又は医学的に重大であるが、ただちに生命を脅かすものではない;入院又は入院期間の延長を要する;活動不能/動作不能;身の回りの日常生活動作の制限。
グレード4:生命を脅かす;緊急処置を要する。
グレード5:有害事象による死亡。
尚、本明細書において、発症なしをグレード0と定義する。
「有害事象発症リスク」とは、有害事象を発症する可能性をいう。すなわち、ある個体が高リスク群に属するとは、該個体が有害事象を発症する可能性が高いと予想されることを意味し、ある個体が低リスク群に属するとは、該個体が有害事象を発症する可能性が低いと予想されることを意味する。
また、「有害事象重症化リスク」とは、有害事象が重症化する可能性をいう。すなわち、ある個体が高リスク群に属するとは、該個体が有害事象を発症し、該有害事象が重症化する可能性が高いと予想されることを意味し、ある個体が低リスク群に属するとは、該個体が有害事象を発症する可能性が低いか、該個体が有害事象を発症したとしても該有害事象が重症化する可能性は低いと予想されることを意味する。
また、DCF療法施行中に発熱性好中球減少症を発症しなかった患者では、発熱性好中球減少症を発症した患者に比して、治療前後ともにA.hadrusの菌数が有意に高値を示した(図1)。DCF療法に加え、シンバイオティクス療法を受けた群のみの解析でも、該療法施行中に発熱性好中球減少症を発症しなかった患者では、発熱性好中球減少症を発症した患者に比して、治療前後ともにA.hadrusの菌数が高い傾向がみられた(図2)。ここで、シンバイオティクス療法は、DCF療法による発熱性好中球減少症や重篤な下痢を顕著に軽減することが報告されており(非特許文献1)、プロバイオティクスとしてLacticaseibacillus paracasei strain Shirota(LcS)とBifidobacterium breve strain Yakult(BbrY)(Bifidobacterium breve YIT 12272(FERM BP-11320))とを、プレバイオティクスとしてガラクトオリゴ糖を用いるものである。尚、LcSは、2020年のLactobacillus属細菌の再分類(Zheng J et al. Int J Syst Evol Microbiol. 2020 Apr; 70(4): 2782-2858)以前には、Lactobacillus casei YIT9029(FERM BP-1366)として知られていた菌株であり、昭和56年1月12日、独立行政法人産業技術総合研究所特許生物寄託センター(現在は、独立行政法人製品評価技術基盤機構 特許微生物寄託センター)に寄託されている。ロジスティック解析の結果から、DCF療法前のA.hadrusの菌数及び占有率の低さは、発熱性好中球減少症発症のリスク因子となることが示唆された。
さらに、DCF療法施行中に下痢を発症しなかった又は下痢の重症度が低かった患者(ベースラインと比べて排便回数増加が6回/日以下)では、極めて重度の下痢を発症した患者(ベースラインと比べて7回以上/日の排便回数増加、便失禁あり、入院もしくは緊急処置を要する)に比して、治療前後ともにA.hadrusの菌数が有意に高値を示した(図3)。DCF療法に加え、シンバイオティクス療法を受けた群のみの解析でも、該療法施行中に下痢を発症しなかった又は下痢の重症度が低かった患者では、極めて重度の下痢を発症した患者に比して、治療前後ともにA.hadrusの菌数が高い傾向がみられた(図4)。ロジスティック解析の結果から、DCF療法前のA.hadrusの菌数及び占有率の低さは、下痢重症化のリスク因子となることが示唆された。
また、リスク判定対象となる有害事象は、特に限定されず、例えば、血液及びリンパ系障害、心臓障害、耳及び迷路障害、内分泌障害、眼障害、胃腸障害、一般・全身障害及び投与部位の障害、肝胆道系障害、免疫系障害、代謝及び栄養障害、筋骨格系及び結合組織障害、神経系障害、精神障害、腎及び尿路障害、生殖系及び乳房障害、呼吸器、胸郭及び縦隔障害、皮膚及び皮下組織障害、血管障害などが挙げられる。本発明の方法は、有害事象として血液及びリンパ系障害並びに胃腸障害からなる群より選択される少なくとも1種のリスク判定に好適に用いられ、具体的には、発熱性好中球減少症及び下痢からなる群より選択される少なくとも1種のリスク判定、つまり、発熱性好中球減少症リスク及び下痢リスクからなる群より選択される少なくとも1種のリスク判定により好適に用いられる。
グレード1:-(定義なし)
グレード2:-(定義なし)
グレード3:好中球絶対数<1,000/mm3で、かつ1回でも38.3℃を超える、又は1時間を超えて持続する38.0℃以上の発熱。
グレード4:生命を脅かす;緊急処置を要する。
グレード5:死亡
また、下痢の重症度は、CTCAE v4.0によれば、以下のグレードに分類されている。なお、ベースラインとは日常生活における排便習慣(排便回数)をさす。
グレード1:ベースラインと比べて<4回/日の排便回数増加;ベースラインと比べて人工肛門からの排泄量が軽度に増加。
グレード2:ベースラインと比べて4~6回/日の排便回数増加;ベースラインと比べて人工肛門からの排泄量が中等度増加。
グレード3:ベースラインと比べて7回以上/日の排便回数増加;便失禁;入院を要する;ベースラインと比べて人工肛門からの排泄量が高度に増加;身の回りの日常生活動作の制限。
グレード4:生命を脅かす;緊急処置を要する。
グレード5:死亡
本発明の方法により、集学的治療時の有害事象リスクが低いと判定された患者に対しては、予定されている集学的治療を実施することができ、集学的治療時の有害事象リスクが高いと判定された患者に対しては、薬剤量の低減や、シンバイオティクスの併用等の有害事象の予防又は軽減のための処置を行うことができる。
例えば、ヒトや、マウス、ラット又はウサギ等の実験動物に被検物質を投与して、未投与のヒトや実験動物と比較し、当該被検物質が検体中のA.hadrusの菌数又は占有率を変動させるか否かを判定する。当該被検物質がA.hadrusの菌数を増加させた、菌数の増加を促進した、菌数の低下を抑制した物質と判定された際には、当該被検物質を集学的治療時の有害事象リスクの低減剤として利用できる。あるいは、当該被検物質がA.hadrusの占有率を増加させた、占有率の増加を促進した、占有率の低下を抑制した物質と判定された際には、当該被検物質を集学的治療時の有害事象リスクの低減剤として利用できる。
1.方法
(1)解析対象
術前化学療法が予定されている20歳から80歳までの食道がん患者81名が試験に登録された。そのうち、登録時、及びDCF療法開始後8日目ともに糞便が採取された73名(予防的抗生剤投与群38名、シンバイオティクス投与群35名)を解析対象とした。本試験に参加した全ての患者から、参加前に同意書による試験参加の同意を得た。
DCF療法は、ドセタキセル 70mg/m2とシスプラチン 70mg/m2をDay1に点滴で、5-フルオロウラシル 700mg/m2をDay1からDay5に持続点滴で投与した。基本的に、化学療法は3週間間隔を空けて2コース行った。予防的抗生剤投与群の患者は、化学療法各コースのDay5からDay15まで、レボフロキサシン 500mgを1日1回内服した。シンバイオティクス投与群の患者は、化学療法各コースの開始3日前からDay12まで、ラコールNF配合経腸用液(株式会社大塚製薬工場)を1日600mLに加えて、化学療法1コース開始3日前から化学療法終了まで、プロバイオティクスとしてLacticaseibacillus paracasei strain Shirota(Lacticaseibacillus paracasei YIT 9029:LcS)(2020年のLactobacillus属細菌の再分類以前のLactobacillus casei YIT 9029(FERM BP-1366))とBifidobacterium breve strain Yakult(BbrY)(Bifidobacterium breve YIT 12272(FERM BP-11320))の生菌をそれぞれ3×108cells以上含むヤクルトBL整腸薬(株式会社ヤクルト本社)を1日3g、プレバイオティクスとしてオリゴメイトS-HP(ヤクルト薬品工業株式会社)を1日15mL(ガラクトオリゴ糖を5g含む)内服した。
化学療法の有害事象である発熱性好中球減少症及び下痢の毒性は、米国国立がん研究所(NCI)が公表する有害事象共通用語基準v4.0(CTCAE v4.0)のクライテリアを用いて評価した。
試験登録時及び化学療法1コース目のDay8に、約1.0gの新鮮便を2mLのRNAlater(Ambion)とφ5mmジルコニアビーズを入れた予め秤量済みのチューブに採取スプーンにて採取した。振とうして懸濁した後、その後の操作まで4℃で保存した。核酸抽出に用いる糞便サンプルの一次処理は以下の方法で行った。糞便サンプルの重量を測定した後、10倍容になるようにRNALaterを添加した。これをShakeMaster Auto(Biomedical science)を用いて1,048rpmで10分間振とうした。RNA抽出用として、40μLの糞便懸濁液を1mL PBSが添加された新たな2mLチューブに移し、遠心分離(4℃,13,000×g,5分間)した後、デカンテーションにより上清を除去した。このペレットをRNA抽出まで-80℃で保存した。DNA抽出用として、200μLの懸濁液を1mLのPBSが添加された新たな2mLチューブに移し、ボルテックスで攪拌した。これを遠心分離(4℃,13,000×g,5分間)した後、上清1mLを除いた。再度1mLのPBSを添加し、懸濁、遠心分離(4℃,13,000×g,5分間)した後、上清1mLを除いた。得られた200μLの懸濁液をDNA抽出まで-30℃で保存した。
糞便サンプルからのDNAの抽出はQIAamp DNA Stool Mini Kit(QIAGEN GmbH)を用いて、マニュアルに従って行った。16S rRNA遺伝子アンプリコン解析は以下のようにして行った。各サンプルの16S rRNA遺伝子のV1-V2領域を27Fmod2フォワードプライマー及び338Rリバースプライマー(配列番号1及び2)を用いて、ABI 7500 Real-Time PCR System(Thermo Fisher Scientific)により増幅した。PCR反応液(50μL)として、2×SYBR Premix Ex Taq II(50μL,Takara Bio)、Nuclease-Free Water(22μL)、各プライマー(100nM,1μL)、及び鋳型DNA(10ng/mL,1μL)を混合した。PCR反応は95℃で30秒加熱して初期変性した後、95℃で5秒、55℃で30秒、72℃で40秒を25サイクルの条件で行った。増幅産物をAMPure XP Kit(Beckman Coulter Genomics)で精製し、Quant-iT PicoGreen dsDNA Kit(Invitrogen)で定量した。各々のサンプル中の増幅産物を等量となるように混合してライブラリーを作製し、MiSeq Reagent Kits v2(Illumina)を用いて、MiSeq platform(Illumina)でシーケンスを行った。結果として、2,621,476のアンプリコンシーケンスリード(サンプル当たり9,158~36,003リード)が得られた。
シーケンスデータの処理にはQIIME2(ver.2019.10,https://qiime2.org/)を用いた。DADA2プラグインを用いてシーケンスデータのクオリティコントロールを実施した後、シーケンスデータをASV(amplicon sequence variant)へと纏め、被験者ごとの各ASVの占有率を算出した。系統情報のアサインにはSILVA 138 database(https://www.arb-silva.de/)をデータベースとして使用した。
DDBJ/GenBank/EMBL databaseより得た16S rRNA配列を用いて、A.hadrus及び近縁種のマルチプルアラインメントをClustalXにより構築した。このアラインメントに基づき、Primer3plus software(http://www.bioinformatics.nl/cgi-bin/primer3plus/primer3plus.cgi)を用いてA.hadrusの16S rRNA遺伝子に特異的なAH7Fフォワードプライマー及びAH1Rリバースプライマーからなるプライマーセット(配列番号3及び4)を設計した。該プライマーセットを用いて、QuantStudio 12K Flex Real-Time PCR System(Thermo Fisher)により、培養したA.hadrusより抽出したRNAを鋳型として定量的RT-PCRを行った。定量的RT-PCRにはQiagen OneStep RT-PCR kit(Qiagen)を用いた。PCR反応液(10μL)として、1×Qiagen Onestep RT―PCR Buffer(2μL)、0.5×Q-solution(2μL)、dNTP Mixture(各々400μM)、100,000倍希釈したSYBR Green I(Molecular Probes)、Qiagen OneStep RT-PCR enzyme mix(0.4μL)、AH7Fフォワードプライマー及びAH1Rリバースプライマー(0.6μM)、鋳型RNA(5μL)を混合した。RT-PCR反応は50℃で30分加熱して逆転写反応を行い、95℃で15分加熱して初期変性し、94℃で5秒、55℃で30秒、72℃で50秒を40サイクルの条件で行った結果、A.hadrusの基準株であるYIT10092T(DSM3319T)から抽出したRNAを用いた際に増幅産物が得られることを確認した。また、Primer-Blast program(https://www.ncbi.nlm.nih.gov/tools/primer-blast/)を用いて、設計したプライマーによる非特異的な増幅産物が既存のデータベース中に存在しないことを確認した。さらに、設計したプライマーの特異性をYakult Intestinal Flora-SCAN(YIF-SCAN(登録商標))の標準菌株である腸内細菌叢の主要構成細菌23種から抽出したRNA(105cells相当)を用いて上記の条件で定量的RT-PCRを実施して検証した結果、いずれの菌種にも交差性を示さないことを確認した。
糞便サンプルからのtotal RNAの抽出は、AGPC(acid guanidinium thiocyanate-phenol-chloroform extraction)法を改良して行った。解凍したサンプルを346.5μLのRLT Buffer(Qiagen)、3.5μLのβ―mercaptoethanol(Sigma-Aldrich)、および100μLのTris-EDTA bufferを混合した溶液に再懸濁した。ガラスビーズ(0.1mm,300mg,BioSpec Products)を加えて、ShakeMaster Auto(Biomedical science)を用いて1,048rpmで5分間振とうした。水飽和フェノール(500μL)を加えて、60℃で10分インキュベーションした後、chloroform-isoamyl alcohol(24:1,100μL)を加えて攪拌し、遠心分離(4℃,14,000×g,5分間)した。上清470μLを分取し、同量のchloroform-isoamyl alchol(24:1)を加えて攪拌した。上清400μLを分取し、イソプロパノール沈殿によりRNAを沈殿させて回収した後、200μLのnuclease-free water(Ambion)に溶解した。サンプル中のA.hadrusの定量には、定量的RT-PCR法(RT-qPCR)を基本原理とするYIF-SCAN(登録商標)を用いた。RT-qPCRには、上述のA.hadrusに対する16S rRNAを標的とした菌種特異的プライマー(配列番号3及び4)と反応条件を用いた。アッセイの線形範囲のthreshold cycle(Cq)値を標準曲線に代入して、各サンプル中の対応する菌数を求めた。ここから、各サンプル中の菌数を決定した。標準曲線は、Cq値とDAPI染色により菌数決定済みの標準株A.hadrus YIT10092T(DSM3319T)の希釈系列を使用して作成した。検出限界値(LOD)は標準曲線中の最も小さな菌数とした(10-2cells/reaction)。

増幅産物が標的微生物由来のものかを確認するため、RT-qPCRにより増幅された菌種をシーケンス解析により推定した。RT-qPCR産物(10μL)をMultiScreen(登録商標) Filter Plate(Merck Millipore)により精製した。サイクルシーケンス反応をBigDye(登録商標) Terminator version 3.1 Cycle Sequencing kit(Applied Biosystems)を用いて製造元のマニュアルに従って行った。増幅産物をエタノール沈殿により精製し、ホルムアミド(1μL)に溶解して変性させ、ABI PRISM 3130 Genetic Analyzer(Applied Biosystems)によりシーケンスを行った。特定の種へのアサインを行うための得られたrRNA配列の比較は、NCBIのBLAST program(http://blast.ncbi.nlm.nih.gov/Blast.cgi)を用いて行った。
統計解析にはR(ver 3.6.0)(https://www.r-project.org/)を用いた。連続変数は中央値(四分位範囲)で表した。2群間の差の検定は、non-parametric Mann-Whitney U testを用いた。群間での腸内細菌叢のASVの組成の違いは、有心対数比変換データによるANOVA-Like Differential Expression Analysis(ALDEx)解析で評価した。ALDEx解析にはaldex関数(ALDEx2パッケージ)を用いた。RT-qPCR解析結果について、定量下限値以下であった検体については定量下限値の半値を代入して解析に用いた。いずれの解析においても、p<0.05を有意差ありと判断した。
(1)有害事象の発症及び重症度によるDCF療法後の腸内細菌叢の比較
予防的抗生剤投与群(Antibiotics群)及びシンバイオティクス投与群(Synbiotics群)においてDCF療法開始後8日目に検出されたASV(amplicon sequence variant)の組成を、DCF療法の有害事象である発熱性好中球減少症の重症度により比較した。DCF療法1コース中に発熱性好中球減少症を発症しなかった患者(グレード0)では、発熱性好中球減少症を発症した患者(グレード3)と比較してASV15の占有率が有意に高かった。参照データベースとしてSILVAを用いたアサインの結果、ASV15はAnaerostipes hadrusと推定された。
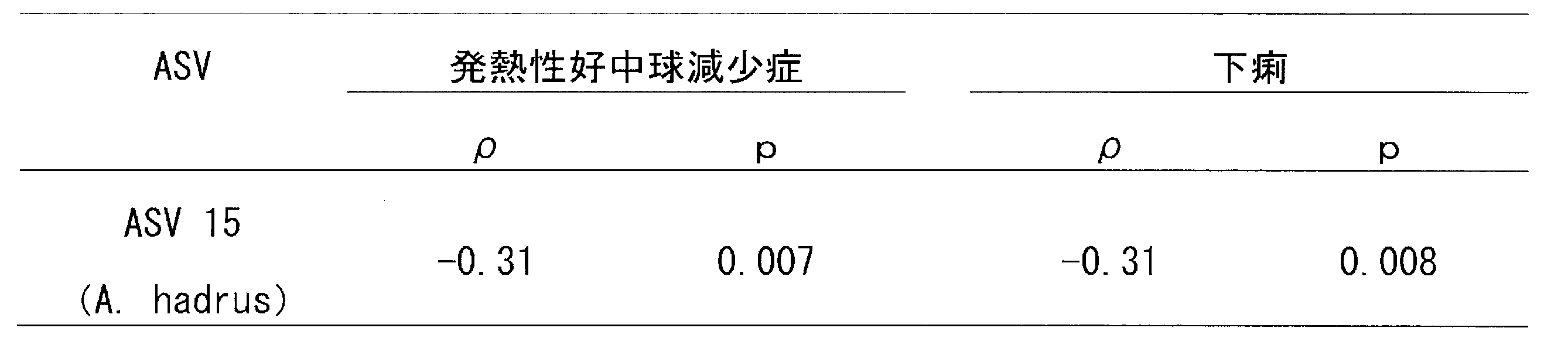
有害事象との関連が示唆されたASV15の占有率と発熱性好中球減少症及び下痢の重症度の相関を解析し、スピアマンの相関係数を求めた結果、ASV15は発熱性好中球減少症及び下痢の重症度との間に有意な負の相関が認められた(表2)。
DCF療法前の糞便中のA.hadrusの菌数は、Antibiotics群及びSynbiotics群の間に有意な差は認められなかった。DCF療法開始後8日目に、Antibiotics群ではDCF療法前と比較してA.hadrusの菌数が低下する傾向(p=0.11)が認められたが、Synbiotics群ではDCF療法後のA.hadrusの菌数の低下は認められなかった。DCF療法及び予防的抗生剤の投与によりA.hadrusの菌数は低下するが、シンバイオティクスの内服により、そのような菌数の低下が抑制されていた。
Antibiotics群及びSynbiotics群において、DCF療法1コース中に発熱性好中球減少症を発症しなかった患者(グレード0)では、発熱性好中球減少症を発症した患者(グレード3)と比較して、DCF療法前後ともにA.hadrusの菌数が有意に高値を示した(図1)。Synbiotics群のみの解析においても、発熱性好中球減少症を発症しなかった患者(グレード0)では、発熱性好中球減少症を発症した患者(グレード3)と比較して、A.hadrusの菌数はDCF療法前後ともに高い傾向がみられた(図2)。よって、治療前から、腸内のA.hadrusの菌数が高い患者では、発熱性好中球減少症が軽減されることが示唆された。
Antibiotics群及びSynbiotics群において、DCF療法1コース中に極めて重度の下痢を発症した患者(グレード3~4:ベースラインと比べて7回以上/日の排便回数増加;便失禁あり;入院もしくは緊急処置を要する)と下痢の重症度が低かった患者(グレード0~2:発症なしもしくはベースラインと比べて<6回/日の排便回数増加)とを比較した場合、DCF療法前後ともに重症度が低い患者においてA.hadrusの菌数が有意に高値を示した(図3)。Synbiotics群のみの解析でも、下痢の重症度が低かった患者(グレード0~2)では、極めて重度の下痢を発症した患者(グレード3~4)と比較して、A.hadrusの菌数はDCF療法前後ともに高い傾向が認められた(図4)。よって、治療前から、腸内のA.hadrusの菌数が高い患者では、下痢が軽減されることが示唆された。
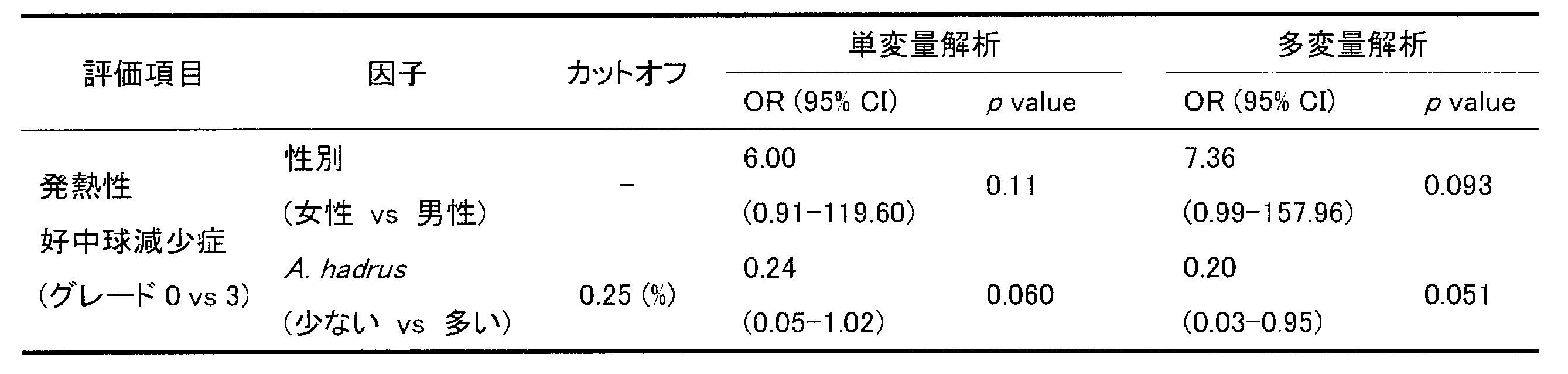
Synbiotics群の発熱性好中球減少症の発症の有無でベースライン特性を比較したところ、患者の性別にわずかに差がある傾向が認められたものの、患者の年齢、BMI、dysphagia score、腫瘍位置、ステージ、白血球数、好中球数、総リンパ球数、及び血清アルブミンに有意な差は認められなかった。そこで、シンバイオティクス療法下でのDCF療法における有害事象のリスク因子を検討するため、患者の性別及びA.hadrusの菌数を用いてロジスティック回帰を行った。結果を表3に示す。表3中、CIは信頼区間を、ORはオッズ比を示し、A.hadrusの菌数のカットオフ値は、受信者動作特性(ROC)分析により算出した値である。単変量解析において、DCF療法施行前のA.hadrusの菌数は、発熱性好中球減少症の発症リスクの減少と有意に関連した(OR,0.13;95%CI,0.02-0.66,p=0.023)。さらに、患者の性別を加えた多変量解析においても、DCF療法施行前のA.hadrusの菌数は、発熱性好中球減少症の発症リスクの減少と有意に関連した(OR,0.11;95%CI,0.01-0.60,p=0.019)。また、カットオフ値は、検体1gあたり、107.7個であった。

シンバイオティクス療法下でのDCF療法における有害事象のリスク因子を検討するため、患者の性別及びA.hadrusの占有率を用いてロジスティック回帰を行った。結果を表4に示す。表4中、CIは信頼区間を、ORはオッズ比を示し、A.hadrusの占有率のカットオフ値は、受信者動作特性(ROC)分析により算出した値である。単変量解析において、DCF療法施行前のA.hadrusの占有率は発熱性好中球減少症の発症リスクの減少と関連する傾向があった(OR,0.24;95%CI,0.05-1.02,p=0.060)。さらに、患者の性別を加えた多変量解析においても、DCF療法施行前のA.hadrusの占有率は発熱性好中球減少症の発症リスクの減少と関連する傾向があった(OR,0.20;95%CI,0.03-0.95,p=0.051)。また、カットオフ値は、0.25%であった。
Synbiotics群の下痢の重症度の軽重でベースライン特性を比較したところ、患者の年齢、性別、BMI、dysphagia score、腫瘍位置、ステージ、白血球数、好中球数、総リンパ球数、及び血清アルブミンに有意な差は認められなかった。そこで、シンバイオティクス療法下でのDCF療法における有害事象のリスク因子を検討するため、A.hadrusの菌数を用いてロジスティック回帰を行った。結果を表5に示す。表5中、CIは信頼区間を、ORはオッズ比を示し、A.hadrusの菌数のカットオフ値は、受信者動作特性(ROC)分析により算出した値である。単変量解析において、DCF療法施行前のA.hadrusの菌数は、下痢の重症化リスクの減少と関連する傾向があった(OR,0.14;95%CI,0.01-1.13,p=0.11)。また、カットオフ値は、検体1gあたり、107.6個であった。

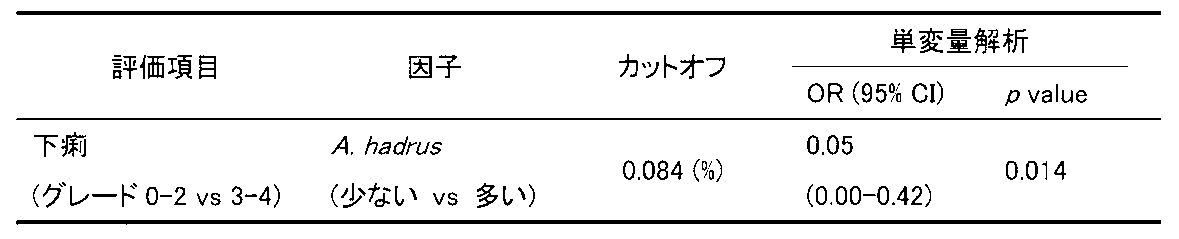
シンバイオティクス療法下でのDCF療法における有害事象のリスク因子を検討するため、A.hadrusの占有率を用いてロジスティック回帰を行った。結果を表6に示す。表6中、CIは信頼区間を、ORはオッズ比を示し、A.hadrusの占有率のカットオフ値は、受信者動作特性(ROC)分析により算出した値である。単変量解析において、DCF療法施行前のA.hadrusの占有率は下痢の重症化リスクの減少と関連する傾向があった(OR,0.05;95%CI,0.00-0.42,p=0.014)。また、カットオフ値は、0.084%であった。
Claims (12)
- 被験者より採取した検体中のAnaerostipes hadrusを測定することを含む、集学的治療時の有害事象リスクの判定方法。
- 有害事象リスクが有害事象の発症リスク又は重症化リスクである、請求項1記載の方法。
- 集学的治療が薬物療法、外科療法、放射線治療、及びその組み合わせから選択される治療である、請求項1又は2記載の方法。
- 集学的治療が薬物療法である、請求項1~3のいずれか1項記載の方法。
- 有害事象が発熱性好中球減少症及び下痢からなる群より選択される少なくとも1種である、請求項1~4のいずれか1項記載の方法。
- 検体が被験者の糞便検体である、請求項1~5のいずれか1項記載の方法。
- 検体中のAnaerostipes hadrusの菌数を基準値と比較し、菌数が基準値以下である場合に、集学的治療時の有害事象リスクが高いと判定することをさらに含む、請求項1~6のいずれか1項記載の方法。
- 検体中の総細菌におけるAnaerostipes hadrusの占有率を基準値と比較し、占有率が基準値以下である場合に、集学的治療時の有害事象リスクが高いと判定することをさらに含む、請求項1~6のいずれか1項記載の方法。
- 検体中のAnaerostipes hadrusの菌数が、検体1gあたり、107.7個以下であるか、検体中の総細菌におけるAnaerostipes hadrusの占有率が0.25%以下である場合に、集学的治療時の発熱性好中球減少症リスクが高いと判定することをさらに含む、請求項1~6のいずれか1項記載の方法。
- 検体中のAnaerostipes hadrusの菌数が、検体1gあたり、107.6個以下であるか、検体中の総細菌におけるAnaerostipes hadrusの占有率が0.084%以下である場合に、集学的治療時の下痢リスクが高いと判定することをさらに含む、請求項1~6のいずれか1項記載の方法。
- 検体中のAnaerostipes hadrusの測定試薬及びプロトコールを含む、請求項1~10のいずれか1項記載の方法を実施するためのキット。
- Anaerostipes hadrusの菌数又は占有率を指標とする、集学的治療時の有害事象リスクの低減剤のスクリーニング方法。
Priority Applications (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2023558048A JPWO2023080154A1 (ja) | 2021-11-05 | 2022-11-02 | |
| CN202280073323.6A CN118251502A (zh) | 2021-11-05 | 2022-11-02 | 不良事件风险的判定方法 |
| EP22889974.6A EP4428242A4 (en) | 2021-11-05 | 2022-11-02 | METHOD FOR DETERMINING THE RISK OF AN UNDESIRABLE EVENT |
| US18/706,814 US20250320539A1 (en) | 2021-11-05 | 2022-11-02 | Method for determining risk of adverse event |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2021-181204 | 2021-11-05 | ||
| JP2021181204 | 2021-11-05 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2023080154A1 true WO2023080154A1 (ja) | 2023-05-11 |
Family
ID=86241558
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2022/040978 Ceased WO2023080154A1 (ja) | 2021-11-05 | 2022-11-02 | 有害事象リスクの判定方法 |
Country Status (5)
| Country | Link |
|---|---|
| US (1) | US20250320539A1 (ja) |
| EP (1) | EP4428242A4 (ja) |
| JP (1) | JPWO2023080154A1 (ja) |
| CN (1) | CN118251502A (ja) |
| WO (1) | WO2023080154A1 (ja) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2025187666A1 (ja) * | 2024-03-04 | 2025-09-12 | 株式会社ヤクルト本社 | 新規なアナエロスティペス・ハドラス属細菌とその利用 |
Family Cites Families (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP3378949A1 (en) * | 2017-03-22 | 2018-09-26 | Assistance Publique - Hôpitaux de Paris | Method for determining the potential efficacy of anticancer treatment |
-
2022
- 2022-11-02 JP JP2023558048A patent/JPWO2023080154A1/ja active Pending
- 2022-11-02 EP EP22889974.6A patent/EP4428242A4/en active Pending
- 2022-11-02 US US18/706,814 patent/US20250320539A1/en active Pending
- 2022-11-02 CN CN202280073323.6A patent/CN118251502A/zh active Pending
- 2022-11-02 WO PCT/JP2022/040978 patent/WO2023080154A1/ja not_active Ceased
Non-Patent Citations (6)
| Title |
|---|
| AGNELLO MELISSA, CARROLL LAUREN N, IMAM NABEEL, PINO RODOLFO, PALMER CHRISTINA, VARAS IGNACIO, GREENE CLAIRE, HITSCHFELD MAUREEN, : "Gut microbiome composition and risk factors in a large cross-sectional IBS cohort", BMJ OPEN GASTROENTEROLOGY, vol. 7, no. 1, 1 April 2020 (2020-04-01), pages e000345, XP093062253, DOI: 10.1136/bmjgast-2019-000345 * |
| ANONYMOUS: "B.1. Points for early detection and early responseB.4. (1) Disorders requiring discrimination", MANUAL FOR MANAGEMENT OF SERIOUS DRUG REACTIONS. SEVERE DIARRHEA, MINISTRY OF HEALTH, LABOUR AND WELFARE, JP, 1 March 2010 (2010-03-01), JP, pages 1 - 20, XP009546672 * |
| MOTOORI M ET AL., CLIN NUTR, vol. 36, 2017, pages 93 - 99 |
| See also references of EP4428242A4 |
| ZEEVI D ET AL., NATURE, vol. 568, 2019, pages 43 - 48 |
| ZHENG J ET AL., INT J SYST EVOL MICROBIOL., vol. 70, no. 4, April 2020 (2020-04-01), pages 2782 - 2858 |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2025187666A1 (ja) * | 2024-03-04 | 2025-09-12 | 株式会社ヤクルト本社 | 新規なアナエロスティペス・ハドラス属細菌とその利用 |
Also Published As
| Publication number | Publication date |
|---|---|
| JPWO2023080154A1 (ja) | 2023-05-11 |
| US20250320539A1 (en) | 2025-10-16 |
| EP4428242A4 (en) | 2025-12-10 |
| CN118251502A (zh) | 2024-06-25 |
| EP4428242A1 (en) | 2024-09-11 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| JP7109794B2 (ja) | Th1細胞誘導性細菌に対する抗菌組成物 | |
| US11655493B2 (en) | Biomarker for mental disease | |
| US20240398876A1 (en) | Biological marker of intestinal dysbiosis, useful for predicting the response of a cancer patient to an anti-pdi drug | |
| WO2021197254A1 (en) | Use of microorganisms in regulation of bodyweight and cholesterol level | |
| JP2025004152A (ja) | 結腸直腸進行新生物、進行腺腫、及び/又は結腸直腸癌をスクリーニング、診断、及び/又はモニタリングする改善された方法 | |
| EP2909335B1 (en) | Prognostic of diet impact on obesity-related co-morbidities | |
| WO2023080154A1 (ja) | 有害事象リスクの判定方法 | |
| JP2021500921A (ja) | Fimh遮断剤の治療効率を評価するための新規ツール | |
| CN110637093B (zh) | 帕金森病的判定标志物和判定方法 | |
| CN114231648B (zh) | 牙周梭杆菌作为食管鳞状细胞癌生物标志物及其应用 | |
| WO2016119191A1 (en) | Biomarkers for colorectal cancer related diseases | |
| JP2014064543A (ja) | ビフィドバクテリウム・ロンガムの検出および/または定量用オリゴヌクレオチド | |
| RU2834789C2 (ru) | Улучшенный способ скрининга, диагностики и/или мониторинга колоректальной неоплазии на поздней стадии, аденомы на поздней стадии и/или колоректального рака | |
| KR20250171623A (ko) | 새끼돼지의 장내 면역세포의 수준 예측 방법 | |
| CN116997798A (zh) | 可用于预测癌症患者对抗pd1药物的反应的肠道生态失调的生物标志物 | |
| Lee et al. | Characterization of tumor-associated microbiome in multifocal small intestinal neuroendocrine tumors (SI-NETs) | |
| JP2026010237A (ja) | 膵癌を検査するための方法、マーカーおよび検査キットならびに膵癌の予防改善剤のスクリーニング方法 | |
| JP2009165401A (ja) | 標的物質の定量方法 | |
| Willing | Twin studies reveal specific imbalances in the mucosa-associated microbiota of patients with ileal | |
| Willing | Twin studies reveal specific imbalances in the mucosa-associated microbiota of patients |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 22889974 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 202280073323.6 Country of ref document: CN |
|
| ENP | Entry into the national phase |
Ref document number: 2023558048 Country of ref document: JP Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 202417038766 Country of ref document: IN |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2022889974 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2022889974 Country of ref document: EP Effective date: 20240605 |
|
| WWP | Wipo information: published in national office |
Ref document number: 18706814 Country of ref document: US |