WO2023107328A1 - Assessing and treating melanoma - Google Patents
Assessing and treating melanoma Download PDFInfo
- Publication number
- WO2023107328A1 WO2023107328A1 PCT/US2022/051517 US2022051517W WO2023107328A1 WO 2023107328 A1 WO2023107328 A1 WO 2023107328A1 US 2022051517 W US2022051517 W US 2022051517W WO 2023107328 A1 WO2023107328 A1 WO 2023107328A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- polypeptide
- mrna encoding
- level
- mammal
- increased level
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P17/00—Drugs for dermatological disorders
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/68—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving nucleic acids
- C12Q1/6876—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes
- C12Q1/6883—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for diseases caused by alterations of genetic material
- C12Q1/6886—Nucleic acid products used in the analysis of nucleic acids, e.g. primers or probes for diseases caused by alterations of genetic material for cancer
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/5005—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving human or animal cells
- G01N33/5091—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving human or animal cells for testing the pathological state of an organism
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/575—Immunoassay; Biospecific binding assay; Materials therefor for cancer
- G01N33/5751—Immunoassay; Biospecific binding assay; Materials therefor for cancer of the skin, e.g. melanoma
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/118—Prognosis of disease development
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q2600/00—Oligonucleotides characterized by their use
- C12Q2600/158—Expression markers
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/52—Predicting or monitoring the response to treatment, e.g. for selection of therapy based on assay results in personalised medicine; Prognosis
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/54—Determining the risk of relapse
Definitions
- This document relates to methods and materials for assessing and/or treating mammals (e.g., humans) having melanoma (e.g., primary cutaneous melanoma (PCM)).
- mammals e.g., humans
- melanoma e.g., primary cutaneous melanoma (PCM)
- methods and materials provided herein can be used to determine whether or not a melanoma (e.g., a PCM) is likely to relapse (e.g., likely to relapse following treatment).
- a mammal e.g, a human
- melanoma e.g, PCM
- PCM cardiovascular disease 2019
- stage I/II patients with undetectable metastasis at diagnosis
- tumors of uncertain aggressiveness by conventional clinicopathologic staging parameters (Gershenwald et al., CA Cancer J. Clin., 67:472-92 (2017); and Morton et al., N. Engl. J. Med., 370:599-609 (2014)).
- stage III/IV patients patients with metastasis
- stage IIB-C patients are expected to become eligible for adjuvant treatment with pembrolizumab following the positive KEYNOTE-716 trial (Luke et al., Future Oncol., 16(3):4429-4438 (2020)).
- stage I/IIA patients are currently ineligible for adjuvant therapies.
- This document provides methods and materials for assessing and/or treating melanoma (e.g., PCM). In some cases, this document provides methods and materials for determining whether or not a melanoma (e.g., a PCM) is likely to relapse (e.g., likely to relapse following treatment).
- a melanoma e.g., a PCM
- a sample e.g, a tissue sample containing one or more melanoma cells obtained from a mammal having melanoma (e.g, PCM) can be assessed to determine if the melanoma is likely to relapse based, at least in part, on the presence or absence of altered levels (e.g., increased levels or decreased levels) of 4 or more (e.g., five, six, seven, eight, or nine) polypeptides (or mRNA encoding such polypeptides) in the sample.
- altered levels e.g., increased levels or decreased levels
- This document also provides methods and materials for treating a mammal (e.g., a human) having melanoma (e.g., PCM) where the treatment is selected based, at least in part, on whether or not the melanoma is likely to relapse.
- a mammal e.g., a human
- melanoma e.g., PCM
- a mammal having melanoma e.g., PCM
- HJURP holliday junction recognition protein
- NUF2 NDC80 kinetochore complex
- PPP1R9A protein phosphatase 1 regulatory subunit 9A
- SRSF11 serine/arginine-rich splicing factor 11
- a melanoma e.g., PCM
- a melanoma e.g., PCM
- relapse e.g., likely to relapse following treatment
- a mammal having a high- risk melanoma e.g., a melanoma that is identified as being likely to relapse as described herein
- a mammal having a low-risk melanoma e.g., a melanoma that is identified as not being likely to relapse as described herein
- can forgo unnecessary treatment e.g., lymph node surgery
- one aspect of this document features methods for assessing a mammal having a PCM.
- the methods can include, or consist essentially of, (a) determining if a sample from a mammal having PCM contains the presence or absence of (1) an increased level of a HJURP polypeptide or mRNA encoding said HJURP polypeptide, (2) an increased level of a NUF2 polypeptide or mRNA encoding said NUF2 polypeptide, (3) an increased level of a PPP 1R9 A polypeptide or mRNA encoding said PPP 1R9 A polypeptide, (4) an increased level of a SRSF11 polypeptide or mRNA encoding said SRSF11 polypeptide, (5) an increased level of a NT5DC3 polypeptide or mRNA encoding said NT5DC3 polypeptide, (6) an increased level of a SERPINE2 polypeptide or mRNA encoding said SERPINE2 polypeptide, (7) a decreased level of
- the mammal can be a human.
- the presence or absence of the increased level of the HJURP polypeptide or mRNA encoding the HJURP polypeptide can be determined.
- the presence or absence of said increased level of the NUF2 polypeptide or mRNA encoding the NUF2 polypeptide can be determined.
- the presence or absence of the increased level of the PPP1R9A polypeptide or mRNA encoding the PPP1R9A polypeptide can be determined.
- the presence or absence of the increased level of the SRSF11 polypeptide or mRNA encoding the SRSF11 polypeptide can be determined.
- the presence or absence of the increased level of the NT5DC3 polypeptide or mRNA encoding the NT5DC3 polypeptide can be determined.
- the presence or absence of the decreased level of the SERPINE2 polypeptide or mRNA encoding the SERPINE2 polypeptide can be determined.
- the presence or absence of the decreased level of the PARM1 polypeptide or mRNA encoding the PARM1 polypeptide can be determined.
- the presence or absence of the decreased level of the EMP2 polypeptide or mRNA encoding the EMP2 polypeptide can be determined.
- the presence or absence of the decreased level of the PRKCB polypeptide or mRNA encoding the PRKCB polypeptide can be determined.
- the presence or absence of the decreased level of the CD IE polypeptide or mRNA encoding the CD IE polypeptide can be determined.
- the presence or absence of the decreased level of the ALDH2 polypeptide or mRNA encoding the ALDH2 polypeptide can be determined.
- the presence or absence of the decreased level of the CD200R1 polypeptide or mRNA encoding the CD200R1 polypeptide can be determined.
- the method also can include determining a Breslow depth of the PCM.
- the method can include determining the presence of the increased level of the HJURP polypeptide or mRNA encoding the HJURP polypeptide, the increased level of the NUF2 polypeptide or mRNA encoding the NUF2 polypeptide, the increased level of the PPP 1R9 A polypeptide or mRNA encoding the PPP 1R9 A polypeptide, the increased level of the SRSF11 polypeptide or mRNA encoding the SRSF11 polypeptide, the increased level of the NT5DC3 polypeptide or mRNA encoding the NT5DC3 polypeptide, the increased level of the SERPINE2 polypeptide or mRNA encoding the SERPINE2 polypeptide, the decreased level of the PARM1 polypeptide or mRNA encoding the PARM1 polypeptide, the decreased level of the EMP2 polypeptide or mRNA encoding the EMP2 polypeptide, the decreased level of the PRKCB polypeptide or mRNA encoding
- the method can include determining the absence of the increased level of the HJURP polypeptide or mRNA encoding the HJURP polypeptide, the increased level of the NUF2 polypeptide or mRNA encoding the NUF2 polypeptide, the increased level of the PPP1R9A polypeptide or mRNA encoding the PPP 1R9 A polypeptide, the increased level of the SRSF11 polypeptide or mRNA encoding the SRSF11 polypeptide, the increased level of the NT5DC3 polypeptide or mRNA encoding the NT5DC3 polypeptide, the increased level of the SERPINE2 polypeptide or mRNA encoding the SERPINE2 polypeptide, the decreased level of the PARM1 polypeptide or mRNA encoding the PARM1 polypeptide, the decreased level of the EMP2 polypeptide or mRNA encoding the EMP2 polypeptide, the decreased level of the PRKCB polypeptide or mRNA encoding
- this document features methods for selecting a treatment for a mammal having a PCM.
- the methods can include, or consist essentially of, (a) determining that a sample from a mammal having a PCM contains the presence of at least 4 of (1) an increased level of a HJURP polypeptide or mRNA encoding the HJURP polypeptide, (2) an increased level of a NUF2 polypeptide or mRNA encoding the NUF2 polypeptide, (3) an increased level of a PPP 1R9 A polypeptide or mRNA encoding the PPP 1R9 A polypeptide, (4) an increased level of a SRSF11 polypeptide or mRNA encoding the SRSF11 polypeptide, (5) an increased level of a NT5DC3 polypeptide or mRNA encoding the NT5DC3 polypeptide, (6) an increased level of a SERPINE2 polypeptide or mRNA encoding the SERPINE2 polypeptide, (7),
- the method also can include determining that the PCM has a Breslow depth of from about 0.8 mm to about 10 mm.
- the mammal can be a human.
- the adjuvant therapy can include radiation therapy.
- the adjuvant therapy can include administering an anti-cancer drug to the mammal.
- the anti-cancer drug can be nivolumab, ipilimumab, pembrolizumab, talimogene laherparepvec, vemurafenib, dabrafenib, encorafenib, trametinib, cobimetinib, binimetinib, atezolizumab, avelumab, or durvalumab.
- this document features methods for selecting a treatment for a mammal having a PCM.
- the methods can include, or consist essentially of, (a) determining that a sample from a mammal having a PCM contains the absence of (1) an increased level of a HJURP polypeptide or mRNA encoding the HJURP polypeptide, (2) an increased level of a NUF2 polypeptide or mRNA encoding the NUF2 polypeptide, (3) an increased level of a PPP1R9A polypeptide or mRNA encoding the PPP 1R9 A polypeptide, (4) an increased level of a SRSF11 polypeptide or mRNA encoding the SRSF11 polypeptide, (5) an increased level of a NT5DC3 polypeptide or mRNA encoding the NT5DC3 polypeptide, (6) an increased level of a SERPINE2 polypeptide or mRNA encoding the SERPINE2 polypeptide, (7), a decreased level of
- the method also can include determining that the PCM has a Breslow depth of from about 0.1 mm to about 0.8 mm.
- the mammal can be a human.
- the adjuvant therapy can include radiation therapy.
- the adjuvant therapy can include administering an anti-cancer drug to the mammal.
- the anti-cancer drug can be nivolumab, ipilimumab, pembrolizumab, talimogene laherparepvec, vemurafenib, dabrafenib, encorafenib, trametinib, cobimetinib, binimetinib, atezolizumab, avelumab, or durvalumab.
- this document features methods for treating a mammal having a PCM.
- the methods can include, or consist essentially of, (a) determining that a sample from a mammal having a PCM contains the presence of at least 4 of (1) an increased level of a HJURP polypeptide or mRNA encoding the HJURP polypeptide, (2) an increased level of a NUF2 polypeptide or mRNA encoding the NUF2 polypeptide, (3) an increased level of a PPP1R9A polypeptide or mRNA encoding the PPP 1R9 A polypeptide, (4) an increased level of a SRSF11 polypeptide or mRNA encoding the SRSF11 polypeptide, (5) an increased level of a NT5DC3 polypeptide or mRNA encoding the NT5DC3 polypeptide, (6) an increased level of a SERPINE2 polypeptide or mRNA encoding the SERPINE2 polypeptide, (7), a decreased level of
- the method also can include determining that the PCM has a Breslow depth of from about 0.8 mm to about 10 mm.
- the mammal can be a human.
- the adjuvant therapy can include radiation therapy.
- the adjuvant therapy can include administering an anti-cancer drug to the mammal.
- the anti-cancer drug can be nivolumab, ipilimumab, pembrolizumab, talimogene laherparepvec, vemurafenib, dabrafenib, encorafenib, trametinib, cobimetinib, binimetinib, atezolizumab, avelumab, or durvalumab.
- this document features methods for treating a mammal having a PCM.
- the methods can include, or consist essentially of, subjecting a mammal having a PCM to a surgery to remove the PCM and administering an adjuvant therapy to the mammal, when the mammal is identified as having at least 4 of: (1) an increased level of a HJURP polypeptide or mRNA encoding the HJURP polypeptide, (2) an increased level of a NUF2 polypeptide or mRNA encoding the NUF2 polypeptide, (3) an increased level of a PPP1R9A polypeptide or mRNA encoding the PPP 1R9 A polypeptide, (4) an increased level of a SRSF11 polypeptide or mRNA encoding the SRSF11 polypeptide, (5) an increased level of a NT5DC3 polypeptide or mRNA encoding the NT5DC3 polypeptide, (6) an increased level of a SERPINE2 polypeptide or m
- the method also can include determining that the PCM has a Breslow depth of from about 0.8 mm to about 10 mm.
- the mammal can be a human.
- the adjuvant therapy can include radiation therapy.
- the adjuvant therapy can include administering an anti-cancer drug to the mammal.
- the anti-cancer drug can be nivolumab, ipilimumab, pembrolizumab, talimogene laherparepvec, vemurafenib, dabrafenib, encorafenib, trametinib, cobimetinib, binimetinib, atezolizumab, avelumab, or durvalumab.
- this document features methods for treating a mammal having a PCM.
- the methods can include, or consist essentially of, (a) determining if a sample from a mammal having a PCM contains the absence of (1) an increased level of a HJURP polypeptide or mRNA encoding the HJURP polypeptide, (2) an increased level of a NUF2 polypeptide or mRNA encoding the NUF2 polypeptide, (3) an increased level of a PPP1R9A polypeptide or mRNA encoding the PPP 1R9 A polypeptide, (4) an increased level of a SRSF11 polypeptide or mRNA encoding the SRSF11 polypeptide, (5) an increased level of a NT5DC3 polypeptide or mRNA encoding the NT5DC3 polypeptide, (6) an increased level of a SERPINE2 polypeptide or mRNA encoding the SERPINE2 polypeptide, (7), a decreased level of a PAR
- the method also can include determining that the PCM has a Breslow depth of from about 0.1 mm to about 0.8 mm.
- the mammal can be a human.
- the adjuvant therapy can include radiation therapy.
- the adjuvant therapy can include administering an anti-cancer drug to the mammal.
- the anti-cancer drug can be nivolumab, ipilimumab, pembrolizumab, talimogene laherparepvec, vemurafenib, dabrafenib, encorafenib, trametinib, cobimetinib, binimetinib, atezolizumab, avelumab, or durvalumab.
- this document features methods for treating a mammal having a PCM.
- the methods can include, or consist essentially of, subjecting a mammal having a PCM to a surgery to remove the PCM in the absence of an adjuvant therapy, when the mammal is identified as lacking: (1) an increased level of a HJURP polypeptide or mRNA encoding the HJURP polypeptide, (2) an increased level of a NUF2 polypeptide or mRNA encoding the NUF2 polypeptide, (3) an increased level of a PPP 1R9 A polypeptide or mRNA encoding the PPP 1R9 A polypeptide, (4) an increased level of a SRSF11 polypeptide or mRNA encoding the SRSF11 polypeptide, (5) an increased level of a NT5DC3 polypeptide or mRNA encoding the NT5DC3 polypeptide, (6) an increased level of a SERPINE2 polypeptide or mRNA encoding the SERPINE
- the method also can include determining that the PCM has a Breslow depth of from about 0.1 mm to about 0.8 mm.
- the mammal can be a human.
- the adjuvant therapy can include radiation therapy.
- the adjuvant therapy can include administering an anti-cancer drug to the mammal.
- the anti-cancer drug can be nivolumab, ipilimumab, pembrolizumab, talimogene laherparepvec, vemurafenib, dabrafenib, encorafenib, trametinib, cobimetinib, binimetinib, atezolizumab, avelumab, or durvalumab.
- Figure 1 shows an exemplary method for step-by-step filtering of genes derived from RNA sequencing experiments to identify markers for predicting melanoma relapse.
- Figure 2 contains graphs showing receiver operating characteristics (ROCs) from LASSO survival models at different time points.
- the models are derived from normalized gene expression data obtained by RNA sequencing experiments.
- Figure 3 contains a graph showing variables which appear at least 10% of times in the 300 models. These variables are derived from data obtained by RNA sequencing experiments.
- Figure 4 contains a table showing exemplary polypeptides having altered levels in melanoma cells from PCMs that are likely to relapse. These results are derived from data obtained by RNA sequencing experiments.
- Figure 5 contains graphs showing receiver operating characteristics (ROCs) from LASSO survival models at different time points.
- the models are derived from normalized gene expression data obtained by quantitative PCR experiments.
- Figure 6 contains a graph showing variables which appear at least 10% of times in the 300 models. These variables are derived from data obtained by quantitative PCR experiments.
- Figure 7 contains a table showing exemplary polypeptides having altered levels in melanoma cells from PCMs that are likely to relapse. These results are derived from quantitative PCR experiments.
- Figure 8 shows levels of a HJURP polypeptide and mRNA encoding a HJURP polypeptide in humans.
- Figure 9 shows levels of a NUF2 polypeptide and mRNA encoding a NUF2 polypeptide in humans.
- Figure 10 shows levels of a PPP1R9A polypeptide and mRNA encoding a PPP1R9A polypeptide in humans.
- Figure 11 shows levels of a SRSF11 polypeptide and mRNA encoding a SRSF11 polypeptide in humans.
- Figure 12 shows levels of a NT5DC3 polypeptide and mRNA encoding a NT5DC3 polypeptide in humans.
- Figure 13 shows levels of a SERPINE2 polypeptide and mRNA encoding a SERPINE2 polypeptide in humans.
- Figure 14 shows levels of a PARM1 polypeptide and mRNA encoding a PARM1 polypeptide in humans.
- Figure 15 shows levels of an EMP2 polypeptide and mRNA encoding an EMP2 polypeptide in humans.
- Figure 16 shows levels of a PRKCB polypeptide and mRNA encoding a PRKCB polypeptide in humans.
- Figure 17 shows levels of a CD1E polypeptide and mRNA encoding a CD1E polypeptide in humans.
- Figure 18 shows levels of an ALDH2 polypeptide and mRNA encoding an ALDH2 polypeptide in humans.
- Figure 19 shows levels of a CD200R1 polypeptide and mRNA encoding a CD200R1 polypeptide in humans.
- a melanoma e.g., a PCM
- a sample e.g., a tissue sample containing one or more melanoma cells obtained from a mammal having melanoma e.g., PCM
- an altered level e.g., an increased level or a decreased level
- the methods and materials provided herein also can include treating a mammal having melanoma e.g., PCM) where one or more cancer treatments are selected based, at least in part, on whether or not the melanoma is likely to relapse.
- PCM melanoma
- a mammal e.g., a human having melanoma e.g., PCM) can be assessed to determine whether or not the melanoma is likely to relapse e.g., likely to relapse following treatment) by detecting the presence or absence of an altered level e.g., an increased level or a decreased level) of 4 or more polypeptides in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the mammal.
- a sample e.g., a tissue sample containing one or more melanoma cells
- an altered level e.g., an increased level or a decreased level
- a sample e.g., a tissue sample containing one or more melanoma cells
- a mammal having melanoma e.g., PCM
- Any appropriate mammal having melanoma can be assessed and/or treated as described herein.
- mammals that can have melanoma (e.g., PCM) and can be assessed and/or treated as described herein include, without limitation, humans, nonhuman primates (e.g., monkeys), dogs, cats, horses, cows, pigs, sheep, mice, and rats.
- a human having melanoma e.g., PCM
- PCM human having melanoma
- the melanoma can be any type of melanoma.
- a melanoma can be any stage of melanoma (e.g., stage 0, stage I, stage II, stage III, or stage IV).
- a melanoma can be at any location on a mammal (e.g., a human) being assessed and/or treated as described herein.
- a melanoma can be at a location on a mammal’s body that has been exposed to ultraviolet (UV) radiation.
- UV ultraviolet
- a melanoma can be at a location on a mammal’s body that has had exposure to the sun.
- a melanoma can be at a location on a mammal’s body that has had exposure to a tanning lamp and/or a tanning bed.
- locations on a mammal’s body where a melanoma that can be assessed and/or treated as described herein include, without limitation, chest, back, legs, arms, face, soles of the feet, palms of the hands, fingernail beds, and/or toenail beds.
- the methods described herein can include identifying a mammal (e.g., a human) as having melanoma (e.g., PCM). Any appropriate method can be used to identify a mammal as having melanoma (e.g., PCM).
- a mammal can be identified as having melanoma (e.g., PCM) without having been subjected to a sentinel lymph node biopsy (SLNb). In some cases, a mammal can be identified as having melanoma (e.g., PCM) and having a negative SLNb.
- PCM sentinel lymph node biopsy
- a melanoma (e.g., PCM) can be identified as likely to relapse (e.g., likely to relapse following treatment) based, at least in part, on the presence of an altered level of 4 or more polypeptides (or mRNA encoding such polypeptides) in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from a mammal having the melanoma.
- a sample e.g., a tissue sample containing one or more melanoma cells
- an altered level can be an increased level of one or more polypeptides (or mRNA encoding such polypeptides) in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from a mammal having melanoma (e.g., PCM).
- a sample e.g., a tissue sample containing one or more melanoma cells obtained from a mammal having melanoma (e.g., PCM).
- the term “increased level” as used herein with respect to a level of a polypeptide (or mRNA encoding that polypeptide) in a sample refers to any level that is higher than a reference level of the polypeptide (or mRNA).
- an altered level can be a decreased level of a polypeptide (or mRNA encoding that polypeptide) in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from a mammal having melanoma (e.g., PCM).
- a sample e.g., a tissue sample containing one or more melanoma cells obtained from a mammal having melanoma (e.g., PCM).
- the term “decreased level” as used herein with respect to a level of a polypeptide (or mRNA encoding that polypeptide) in a sample refers to any level that is lower than a reference level of the polypeptide (or mRNA).
- reference level refers to the level of the polypeptide (or mRNA) typically observed in a control sample.
- Control samples are samples obtained from mammals having melanoma at the time of initial diagnosis and having a SLNb performed within 90 days of the diagnosis, where the mammal after treatment experienced relapse-free survival for at least 4 years. It will be appreciated that levels of polypeptides (or mRNAs) from comparable samples are used when determining whether or not a particular level is an altered level of a polypeptide (or mRNA).
- a melanoma (e.g., PCM) that is likely to relapse (e.g., likely to relapse following treatment) can have the presence of an altered level of any appropriate polypeptides (or mRNAs encoding the polypeptides) in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from a mammal having the melanoma.
- a sample e.g., a tissue sample containing one or more melanoma cells
- polypeptides that can be assessed to determine if an elevated level is present or absent within a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from a mammal having melanoma (e.g., PCM) as described herein include, without limitation, a HJURP polypeptide, a NUF2 polypeptide, a PPP1R9A polypeptide, a SRSF11 polypeptide, a NT5DC3 polypeptide, a PARM1 polypeptide, an EMP2 polypeptide, a PRKCB polypeptide, a CD1E polypeptide, an ALDH2 polypeptide, a CD200R1 polypeptide, a SERPINE2 polypeptide, and a SPP1 polypeptide.
- a sample e.g., a tissue sample containing one or more melanoma cells
- PCM melanoma
- mRNAs that can be assessed to determine if an altered level is present or absent within a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from a mammal having melanoma (e.g., PCM) as described herein include, without limitation, mRNAs encoding a HJURP polypeptide, a NUF2 polypeptide, a PPPlR9A polypeptide, a SRSF11 polypeptide, a NT5DC3 polypeptide, a PARM1 polypeptide, an EMP2 polypeptide, a PRKCB polypeptide, a CD1E polypeptide, an ALDH2 polypeptide, a CD200R1 polypeptide, a SERPINE2 polypeptide, or a SPP1 polypeptide.
- a sample e.g., a tissue sample containing one or more melanoma cells
- PCM melanoma
- a polypeptide that can be assessed to determine if an elevated level is present or absent within a sample can be as listed in Figure 4 or Figure 7.
- a tissue sample containing one or more melanoma cells obtained from a mammal having melanoma (e.g, PCM)
- an mRNA encoding a polypeptide as listed in Figure 4 or Figure 7 can be assessed to determine if an altered level is present or absent within a sample (e.g, a tissue sample containing one or more melanoma cells) obtained from a mammal having melanoma (e.g., PCM).
- a melanoma (e.g., PCM) is not assessed for an altered (e.g., an increased or a decreased) level of a TGFBR1 polypeptide (and an mRNA encoding a TGFBR1 polypeptide), a SERPINE2 polypeptide (and an mRNA encoding a SERPINE2 polypeptide), a CXCL8 polypeptide (and an mRNA encoding a CXCL8 polypeptide), a GDF15 polypeptide (and an mRNA encoding a GDF15 polypeptide), a PLAT polypeptide (and an mRNA encoding a PLAT polypeptide), a MLANA polypeptide (and an mRNA encoding a MLANA polypeptide), a ITGB3 polypeptide (and an mRNA encoding a ITGB3 polypeptide), and/or a LOXL4 polypeptide (and an mRNA encoding a LOXL
- a melanoma that is likely to relapse (e.g., likely to relapse following treatment) can lack an increased level of a TGFBR1 polypeptide (or an mRNA encoding a TGFBR1 polypeptide), an increased level of a SERPINE2 polypeptide (or an mRNA encoding a SERPINE2 polypeptide), an increased level of a CXCL8 polypeptide (or an mRNA encoding a CXCL8 polypeptide), an increased level of a GDF 15 polypeptide (or an mRNA encoding a GDF 15 polypeptide), an increased level of a PLAT polypeptide (or an mRNA encoding a PLAT polypeptide), an increased level of a MLANA polypeptide (or an mRNA encoding a MLANA polypeptide), an increased level of a ITGB3 polypeptide (or an mRNA encoding a ITGB3 polypeptide (or an mRNA encoding a
- an altered level of a polypeptide can be an increased level of a HJURP polypeptide (or an increased level of an mRNA encoding a HJURP polypeptide).
- HJURP polypeptides and nucleic acid sequences encoding a HJURP polypeptide include, without limitation, those set forth in the National Center for Biotechnology Information (NCBI) databases at, for example, accession no Q8NCD3 (version Q8NCD3.2).
- an increased level of a HJURP polypeptide can be any level that is higher than a reference level of the HJURP polypeptide (or a reference level of an mRNA encoding a HJURP polypeptide).
- a reference level of a HJURP polypeptide in humans can be a level of a HJURP polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 1 picogram (pg)/melanoma cell to about 2.3 pg/melanoma cell.
- an increased level of a HJURP polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of a HJURP polypeptide.
- an increased level of a HJURP polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of a HJURP polypeptide.
- a reference level of an mRNA encoding a HJURP polypeptide in humans can be a level of such mRNA that is from about 0.17 pg/melanoma cell to about 0.3 pg/melanoma cell.
- an increased level of mRNA encoding a HJURP polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of mRNA encoding a HJURP polypeptide.
- an increased level of mRNA encoding a HJURP polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of mRNA encoding a HJURP polypeptide.
- an altered level of a polypeptide can be an increased level of a NUF2 polypeptide.
- NUF2 polypeptides and nucleic acid sequences encoding a NUF2 polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. Q9BZD4 (version Q9BZD4.2).
- an increased level of a NUF2 polypeptide (or an mRNA encoding a NUF2 polypeptide) can be any level that is higher than a reference level of the NUF2 polypeptide (or a reference level of an mRNA encoding a NUF2 polypeptide).
- a reference level of a NUF2 polypeptide in humans can be a level of a NUF2 polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 0.9 pg/melanoma cell to about 1.5 pg/melanoma cell.
- a sample e.g., a tissue sample containing one or more melanoma cells
- an increased level of a NUF2 polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of a NUF2 polypeptide.
- an increased level of a NUF2 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of a NUF2 polypeptide.
- a reference level of an mRNA encoding a NUF2 polypeptide in humans can be a level of such mRNA that is from about 0.11 pg/melanoma cell to about 0.19 pg/melanoma cell.
- an increased level of mRNA encoding a NUF2 polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of mRNA encoding a NUF2 polypeptide.
- an increased level of mRNA encoding a NUF2 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of mRNA encoding a NUF2 polypeptide.
- an altered level of a polypeptide can be an increased level of a PPP1R9A polypeptide.
- PPP 1R9 A polypeptides and nucleic acid sequences encoding a PPP1R9A polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. Q9ULJ8 (version Q9ULJ8.2).
- an increased level of a PPP 1R9 A polypeptide (or an mRNA encoding a PPP 1R9 A polypeptide) can be any level that is higher than a reference level of the PPP 1R9 A polypeptide (or a reference level of an mRNA encoding a PPP1R9A polypeptide).
- a reference level of a PPP1R9A polypeptide in humans can be a level of a PPP 1R9 A polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 1.3 pg/melanoma cell to about 2.6 pg/melanoma cell.
- a sample e.g., a tissue sample containing one or more melanoma cells
- an increased level of a PPP 1R9 A polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of a PPP1R9A polypeptide.
- an increased level of a PPP 1R9 A polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of a PPP1R9A polypeptide.
- a reference level of an mRNA encoding a PPP1R9A polypeptide in humans can be a level of such mRNA that is from about 0.37 pg/melanoma cell to about 0.77 pg/melanoma cell.
- an increased level of mRNA encoding a PPP1R9A polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of mRNA encoding a PPP1R9A polypeptide.
- an increased level of mRNA encoding a PPP1R9A polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of mRNA encoding a PPP1R9A polypeptide.
- an altered level of a polypeptide can be an increased level of a SRSF11 polypeptide.
- SRSF11 polypeptides and nucleic acid sequences encoding a SRSF11 polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. Q05519 (version Q05519.1).
- an increased level of a SRSF11 polypeptide (or an mRNA encoding a SRSF11 polypeptide) can be any level that is higher than a reference level of the SRSF11 polypeptide (or a reference level of an mRNA encoding a SRSF11 polypeptide).
- a reference level of a SRSF11 polypeptide in humans can be a level of a SRSF11 polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 3.2 pg/melanoma cell to about 7.0 pg/melanoma cell.
- a sample e.g., a tissue sample containing one or more melanoma cells
- an increased level of a SRSF11 polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of a SRSF11 polypeptide.
- an increased level of a SRSF11 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of a SRSF11 polypeptide.
- a reference level of an mRNA encoding a SRSF11 polypeptide in humans can be a level of such mRNA that is from about 0.79 pg/melanoma cell to about 1.71 pg/melanoma cell.
- an increased level of mRNA encoding a SRSF11 polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of mRNA encoding a SRSF11 polypeptide.
- an increased level of mRNA encoding a SRSF11 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of mRNA encoding a SRSF11 polypeptide.
- an altered level of a polypeptide can be an increased level of a NT5DC3 polypeptide.
- NT5DC3 polypeptides and nucleic acid sequences encoding a NT5DC3 polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. Q86UY8 (version Q86UY8.1).
- an increased level of a NT5DC3 polypeptide (or an mRNA encoding a NT5DC3 polypeptide) can be any level that is higher than a reference level of the NT5DC3 polypeptide (or a reference level of an mRNA encoding a NT5DC3 polypeptide).
- a reference level of a NT5DC3 polypeptide in humans can be a level of a NT5DC3 polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 3.8 pg/melanoma cell to about 8.2 pg/melanoma cell.
- a sample e.g., a tissue sample containing one or more melanoma cells
- an increased level of a NT5DC3 polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of a NT5DC3 polypeptide.
- an increased level of a NT5DC3 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of a NT5DC3 polypeptide.
- a reference level of an mRNA encoding a NT5DC3 polypeptide in humans can be a level of such mRNAthat is from about 1.5 pg/melanoma cell to about 3.28 pg/melanoma cell.
- an increased level of mRNA encoding a NT5DC3 polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of mRNA encoding a NT5DC3 polypeptide.
- an increased level of mRNA encoding a NT5DC3 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of mRNA encoding a NT5DC3 polypeptide.
- an altered level of a polypeptide can be an increased level of a SERPINE2 polypeptide.
- SERPINE2 polypeptides and nucleic acid sequences encoding a SERPINE2 polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. P07093 (version P07093.1).
- an increased level of a SERPINE2 polypeptide (or an mRNA encoding a SERPINE2 polypeptide) can be any level that is higher than a reference level of the SERPINE2 polypeptide (or a reference level of an mRNA encoding a SERPINE2 polypeptide).
- a reference level of a SERPINE2 polypeptide in humans can be a level of a SERPINE2 polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 2.0 pg/melanoma cell to about 22.1 pg/melanoma cell.
- a sample e.g., a tissue sample containing one or more melanoma cells
- an increased level of a SERPINE2 polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of a SERPINE2 polypeptide.
- an increased level of a SERPINE2 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of a SERPINE2 polypeptide.
- a reference level of an mRNA encoding a SERPINE2 polypeptide in humans can be a level of such mRNA that is from about 0.4 pg/melanoma cell to about 4.48 pg/melanoma cell.
- an increased level of mRNA encoding a SERPINE2 polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) higher than a reference level of mRNA encoding a SERPINE2 polypeptide.
- an increased level of mRNA encoding a SERPINE2 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold greater than a reference level of mRNA encoding a SERPINE2 polypeptide.
- an altered level of a polypeptide can be a decreased level of a PARM1 polypeptide.
- PARM1 polypeptides and nucleic acid sequences encoding a PARM1 polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. Q6UWI2 (version Q6UWI2.1).
- a decreased level of a PARM1 polypeptide (or an mRNA encoding a PARM1 polypeptide) can be any level that is lower than a reference level of the PARM1 polypeptide (or a reference level of an mRNA encoding a PARM1 polypeptide).
- a reference level of a PARM1 polypeptide in humans can be a level of a PARM1 polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 1.7 pg/melanoma cell to about 3.0 pg/melanoma cell.
- a decreased level of a PARM1 polypeptide can be at least 5% (c.g, about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of a PARM1 polypeptide.
- a decreased level of a PARM1 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of a PARM1 polypeptide.
- a reference level of an mRNA encoding a PARM1 polypeptide in humans can be a level of such mRNA that is from about 0.93 pg/melanoma cell to about 1.65 pg/melanoma cell.
- a decreased level of mRNA encoding a PARM1 polypeptide can be a level that is at least 5% (c.g, about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of mRNA encoding a PARM1 polypeptide.
- a decreased level of mRNA encoding a PARM1 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of mRNA encoding a PARM1 polypeptide.
- an altered level of a polypeptide can be a decreased level of an EMP2 polypeptide.
- EMP2 polypeptides and nucleic acid sequences encoding a EMP2 polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. P54851 (version P54851.1).
- a decreased level of an EMP2 polypeptide (or an mRNA encoding an EMP2 polypeptide) can be any level that is lower than a reference level of the EMP2 polypeptide (or a reference level of an mRNA encoding an EMP2 polypeptide).
- a reference level of an EMP2 polypeptide in humans can be a level of an EMP2 polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 0.6 pg/melanoma cell to about 1.5 pg/melanoma cell.
- a decreased level of an EMP2 polypeptide can be at least 5% (c.g, about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of an EMP2 polypeptide.
- a decreased level of an EMP2 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of an EMP2 polypeptide.
- a reference level of an mRNA encoding an EMP2 polypeptide in humans can be a level of such mRNA that is from about 0.6 pg/melanoma cell to about 1.39 pg/melanoma cell.
- a decreased level of mRNA encoding an EMP2 polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of mRNA encoding an EMP2 polypeptide.
- a decreased level of mRNA encoding an EMP2 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of mRNA encoding an EMP2 polypeptide.
- an altered level of a polypeptide can be a decreased level of a PRKCB polypeptide.
- PRKCB polypeptides and nucleic acid sequences encoding a PRKCB polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. P05771 (version P05771.4).
- a decreased level of a PRKCB polypeptide (or an mRNA encoding a PRKCB polypeptide) can be any level that is lower than a reference level of the PRKCB polypeptide (or a reference level of an mRNA encoding a PRKCB polypeptide).
- a reference level of a PRKCB polypeptide in humans can be a level of a PRKCB polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 2.9 pg/melanoma cell to about 5.2 pg/melanoma cell.
- a decreased level of a PRKCB polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of a PRKCB polypeptide.
- a decreased level of a PRKCB polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of a PRKCB polypeptide.
- a reference level of an mRNA encoding a PRKCB polypeptide in humans can be a level of such mRNA that is about 1.05 pg/melanoma cell to about 1.89 pg/melanoma cell.
- a decreased level of mRNA encoding a PRKCB polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of mRNA encoding a PRKCB polypeptide.
- a decreased level of mRNA encoding a PRKCB polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of mRNA encoding a PRKCB polypeptide.
- an altered level of a polypeptide can be a decreased level of a CD IE polypeptide.
- Examples of CD IE polypeptides and nucleic acid sequences encoding a CD IE polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. P15812 (version P15812.2).
- a decreased level of a CD IE polypeptide (or an mRNA encoding a CD IE polypeptide) can be any level that is lower than a reference level of the CD IE polypeptide (or a reference level of an mRNA encoding a CD IE polypeptide).
- a reference level of a CD IE polypeptide in humans can be a level of a CD IE polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 5.9 pg/melanoma cell to about 7.7 pg/melanoma cell.
- a decreased level of a CD IE polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of a CD IE polypeptide.
- a decreased level of a CD IE polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of a CD1E polypeptide.
- a reference level of an mRNA encoding a CD IE polypeptide in humans can be a level of such mRNAthat is from about 0.89 pg/melanoma cell to about 1.17 pg/melanoma cell.
- a decreased level of mRNA encoding a CD IE polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of mRNA encoding a CD IE polypeptide.
- a decreased level of mRNA encoding a CD1E polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of mRNA encoding a CD IE polypeptide.
- an altered level of a polypeptide can be a decreased level of an ALDH2 polypeptide.
- ALDH2 polypeptides and nucleic acid sequences encoding an ALDH2 polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. P05091 (version P05091.2).
- a decreased level of an ALDH2 polypeptide (or an mRNA encoding an ALDH2 polypeptide) can be any level that is lower than a reference level of the ALDH2 polypeptide (or a reference level of an mRNA encoding an ALDH2 polypeptide).
- a reference level of an ALDH2 polypeptide in humans can be a level of an ALDH2 polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 4.8 pg/melanoma cell to about 11.4 pg/melanoma cell.
- a decreased level of an ALDH2 polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of an ALDH2 polypeptide.
- a decreased level of an ALDH2 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of an ALDH2 polypeptide.
- a reference level of an mRNA encoding an ALDH2 polypeptide in humans can be a level of such mRNA that is from about 2.87 pg/melanoma cell to about 6.76 pg/melanoma cell.
- a decreased level of mRNA encoding an ALDH2 polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of mRNA encoding an ALDH2 polypeptide.
- a decreased level of mRNA encoding an ALDH2 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of ALDH2 encoding an EMP2 polypeptide.
- an altered level of a polypeptide can be a decreased level of a CD200R1 polypeptide.
- CD200R1 polypeptides and nucleic acid sequences encoding a CD200R1 polypeptide include, without limitation, those set forth in the NCBI databases at, for example, accession no. Q8TD46 (version Q8TD46.3).
- a decreased level of a CD200R1 polypeptide (or an mRNA encoding a CD200R1 polypeptide) can be any level that is lower than a reference level of the CD200R1 polypeptide (or a reference level of an mRNA encoding a CD200R1 polypeptide).
- a reference level of a CD200R1 polypeptide in humans can be a level of a CD200R1 polypeptide in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the human of from about 1.1 pg/melanoma cell to about 1.8 pg/melanoma cell.
- a decreased level of a CD200R1 polypeptide can be at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of a CD200R1 polypeptide.
- a decreased level of a CD200R1 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of a CD200R1 polypeptide.
- a reference level of an mRNA encoding a CD200R1 polypeptide in humans can be a level of such mRNA that is from about 0.36 pg/melanoma cell to about 0.59 pg/melanoma cell.
- a decreased level of mRNA encoding a CD200R1 polypeptide can be a level that is at least 5% (e.g., about 5%, about 10%, about 20%, about 30%, about 40%, about 50%, about 60%, about 70%, about 80%, about 90%, about 95%, or more) lower than a reference level of mRNA encoding a CD200R1 polypeptide.
- a decreased level of mRNA encoding a CD200R1 polypeptide can be a level that is at least 2 (e.g., at least 5, at least 10, at least 15, at least 20, at least 25, at least 35, or at least 50) fold less than a reference level of mRNA encoding a CD200R1 polypeptide.
- any appropriate method can be used to identify the presence, absence, or level of a polypeptide or mRNA encoding that polypeptide.
- the presence, absence, or level of an mRNA encoding a polypeptide can be assessed by detecting and/or quantifying the mRNA encoding a polypeptide.
- methods that can be used to detect and/or quantify mRNA include, without limitation, RT-PCR techniques (e.g., quantitative RT-PCR techniques), and RNA sequencing methods.
- the presence, absence, or level of a polypeptide can be assessed by detecting and/or quantifying the polypeptide.
- Examples of methods that can be used to detect and/or quantify polypeptides include, without limitation, immunohistochemistry (IHC) techniques, mass spectrometry techniques (e.g., proteomicsbased mass spectrometry assays or targeted quantification-based mass spectrometry assays), western blotting techniques, and enzyme-linked immunoassay (ELISA).
- IHC immunohistochemistry
- mass spectrometry techniques e.g., proteomicsbased mass spectrometry assays or targeted quantification-based mass spectrometry assays
- ELISA enzyme-linked immunoassay
- a sample can be a biological sample.
- a sample can contain one or more cancer cells (e.g., melanoma cells).
- a sample can contain one or more biological molecules (e.g., nucleic acids such as DNA and RNA, polypeptides, carbohydrates, lipids, hormones, and/or metabolites).
- tissue samples e.g., tissue samples obtained by skin biopsy.
- a sample can be a fresh sample or a fixed sample (e.g., a formaldehyde-fixed sample or a formalin-fixed sample).
- one or more biological molecules can be isolated from a sample (e.g, from one or more cancer cells within the sample).
- nucleic acid can be isolated from a sample and can be assessed as described herein.
- polypeptides can be isolated from a sample and can be assessed as described herein.
- methods and materials for determining whether or not a melanoma e.g., a PCM
- determining a Breslow depth of the melanoma can be from about 0.1 mm to about 10 mm.
- a Breslow depth of greater than about 0.8 mm (e.g., from about 0.8 mm to about 10 mm, from about 0.8 mm to about 9 mm, from about 0.8 mm to about 8 mm, from about 0.8 mm to about 7 mm, from about 0.8 mm to about 6 mm, from about 0.8 mm to about 5 mm, from about 0.8 mm to about 4 mm, from about 0.8 mm to about 3 mm, from about 0.8 mm to about 2 mm, from about 0.8 mm to about 1 mm, from about 1 mm to about 10 mm, from about 2 mm to about 10 mm, from about 3 mm to about 10 mm, from about 4 mm to about 10 mm, from about 5 mm to about 10 mm, from about 6 mm to about 10 mm, from about 7 mm to about 10 mm, from about 8 mm to about 10 mm, from about 9 mm to about 10 mm, from about 1 mm to about 9 mm, from
- a Breslow depth of greater than about 0.8 mm in combination with the presence of an altered level (e.g., an increased level or a decreased level) of 4 or more polypeptides can indicate that a melanoma is likely to relapse.
- a Breslow depth of less than about 0.8 mm (e.g., from about 0.1 mm to about 0.7 mm, from about 0.1 mm to about 0.6 mm, from about 0.1 mm to about 0.5 mm, from about 0.1 mm to about 0.4 mm, from about 0.1 mm to about 0.3 mm, from about 0.1 mm to about 0.2 mm, from about 0.2 mm to about 0.8 mm, from about 0.3 mm to about 0.8 mm, from about 0.4 mm to about 0.8 mm, from about 0.5 mm to about 0.8 mm, from about 0.6 mm to about 0.8 mm, from about 0.7 mm to about 0.8 mm, from about 0.2 mm to about 0.7 mm, from about 0.3 mm to about 0.6 mm, from about 0.4 mm to about 0.5 mm, from about 0.2 mm to about 0.4 mm, from about 0.3 mm to about 0.5 mm, from about 0.4 mm to about 0.5 mm,
- a Breslow depth of less than about 0.8 mm in combination with the absence of an altered level (e.g., an increased level or a decreased level) of 4 or more polypeptides can indicate that a melanoma is not likely to relapse.
- Any appropriate method can be used to determine a Breslow depth of a melanoma (e.g., a PCM).
- a PCM a PCM
- tumor depth of a skin sample e.g., a skin sample obtained by excisional biopsy
- an ocular micrometer at a right angle to the skin e.g., a PCM
- measurements obtained from digitized slides using computer software can be used to determine a Breslow depth of a melanoma (e.g., a PCM).
- a mammal e.g., a human having a melanoma (e.g., a PCM) that is identified as not being likely to relapse (e.g, not likely to relapse following treatment) as described herein (e.g, based, at least in part, on the absence of an altered level of 4 or more polypeptides) can be selected to receive surgery to remove the melanoma.
- a mammal e.g., a human having a melanoma (e.g., a PCM) that is identified as not being likely to relapse (e.g, not likely to relapse following treatment) as described herein (e.g, based, at least in part, on the absence of an altered level of 4 or more polypeptides) can be selected to receive surgery to remove the melanoma.
- a melanoma e.g., a PCM
- a mammal having a melanoma that is identified as lacking an increased level of a HJURP polypeptide (or mRNA encoding a HJURP polypeptide), an increased level of a NUF2 polypeptide (or mRNA encoding a NUF2 polypeptide), an increased level of a PPP1R9A polypeptide (or mRNA encoding a PPP 1R9 A polypeptide), an increased level of a SRSF11 polypeptide (or mRNA encoding a SRSF11 polypeptide), an increased level of a NT5DC3 polypeptide (or mRNA encoding a NT5DC3 polypeptide), an increased level of SERPINE2 polypeptide (or mRNA encoding a SERPINE2 polypeptide), a decreased level of a PARM1 polypeptide (or mRNA encoding a PARM1 polypeptide), a decreased level of
- a mammal e.g., a human having a melanoma (e.g., a PCM) that is identified as being likely to relapse (e.g., likely to relapse following treatment) as described herein (e.g., based, at least in part, on the presence of an altered level of 4 or more polypeptides) can be selected to receive surgery to remove the melanoma and can be selected for increased monitoring.
- a mammal e.g., a human having a melanoma (e.g., a PCM) that is identified as being likely to relapse (e.g., likely to relapse following treatment) as described herein (e.g., based, at least in part, on the presence of an altered level of 4 or more polypeptides) can be selected to receive surgery to remove the melanoma and can be selected for increased monitoring.
- a melanoma e.g., a PCM
- a mammal having a melanoma that is identified as having the presence of an altered level of 4 or more polypeptides in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the mammal can be selected to receive one or more (e.g., one, two, three, four, five, or more) tests that can be used to identify whether or not a melanoma (e.g., PCM) has relapsed.
- a sample e.g., a tissue sample containing one or more melanoma cells
- a mammal e.g, a human having a melanoma (e.g., a PCM) that is identified as being likely to relapse (e.g., likely to relapse following treatment) as described herein (e.g., based, at least in part, on the presence of an altered level of 4 or more polypeptides) can be selected to receive surgery to remove the melanoma and can be selected for treatment with one or more adjuvant therapies.
- a mammal e.g, a human having a melanoma (e.g., a PCM) that is identified as being likely to relapse (e.g., likely to relapse following treatment) as described herein (e.g., based, at least in part, on the presence of an altered level of 4 or more polypeptides)
- a mammal e.g., a human
- a melanoma e.g., a PCM
- a mammal having a melanoma that is identified as having the presence of an altered level of 4 or more polypeptides in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the mammal can be selected to undergo surgery to remove the melanoma and to receive one or more (e.g., one, two, three, four, five, or more) adjuvant therapies.
- a sample e.g., a tissue sample containing one or more melanoma cells
- This document also provides methods for treating a mammal (e.g., a human) having melanoma (e.g., a PCM).
- a mammal e.g., a human
- a mammal having a melanoma e.g., a PCM
- that is assessed as described herein e.g., to determine whether or not the melanoma is likely to relapse based, at least in part, on the presence or absence of an altered level of 4 or more polypeptides in a sample obtained from the mammal
- a mammal having melanoma e.g., a PCM
- a mammal having melanoma can be administered or instructed to self-administer one or more cancer treatments selected based, at least in part, on whether or not the melanoma is likely to relapse (e.g., based, at least in part, on the presence or absence of an altered level of 4 or more polypeptides in a sample obtained from the mammal).
- a cancer treatment for melanoma can include any appropriate melanoma cancer treatment.
- a cancer treatment for melanoma e.g., a PCM
- a cancer treatment can include administering one or more anti-cancer drugs (e.g., chemotherapeutic agents, targeted cancer drugs, and immunotherapy drugs) to a mammal in need thereof.
- anti-cancer drugs e.g., chemotherapeutic agents, targeted cancer drugs, and immunotherapy drugs
- examples of anti-cancer drugs that can be administered to a mammal having melanoma can include, without limitation, nivolumab (e.g., OPDIVO®), ipilimumab (e.g., YERVOY®), pembrolizumab (e.g., KEYTRUDA®), talimogene laherparepvec (T-VEC; e.g., IMLYGIC®), vemurafenib (e.g., ZELBORAF®), dabrafenib (e.g., TAFINLAR®), encorafenib (e.g., BRAFTOVI
- a mammal e.g., a human
- a melanoma e.g., a PCM
- the mammal can undergo surgery (e.g., local reexcision surgery) to remove the melanoma.
- a mammal having a melanoma that is identified as lacking an increased level of a HJURP polypeptide (or mRNA encoding a HJURP polypeptide), an increased level of a NUF2 polypeptide (or mRNA encoding a NUF2 polypeptide), an increased level of a PPP 1R9 A polypeptide (or mRNA encoding a PPP1R9A polypeptide), an increased level of a SRSF11 polypeptide (or mRNA encoding a SRSF11 polypeptide), an increased level of a NT5DC3 polypeptide (or mRNA encoding a NT5DC3 polypeptide), an increased level of SERPINE2 polypeptide (or mRNA encoding a SERPINE2 polypeptide), a decreased level of a PARM1 polypeptide (or mRNA encoding a PARM1 polypeptide), a decreased level of
- the surgery can be the sole cancer treatment used to treat the mammal.
- a mammal e.g., a human
- a melanoma e.g., a PCM
- the surgery can be the sole cancer treatment used to treat the mammal.
- a mammal having a melanoma that is identified as lacking an increased level of a HJURP polypeptide (or mRNA encoding a HJURP polypeptide), an increased level of a NUF2 polypeptide (or mRNA encoding a NUF2 polypeptide), an increased level of a PPP1R9A polypeptide (or mRNA encoding a PPP1R9A polypeptide), an increased level of a SRSF11 polypeptide (or mRNA encoding a SRSF11 polypeptide), an increased level of a NT5DC3 polypeptide (or mRNA encoding a NT5DC3 polypeptide), an increased level of SERPINE2 polypeptide (or mRNA encoding a SERPINE2 polypeptide), a decreased level of a PARM1 polypeptide (or mRNA encoding a PARM1 polypeptide), a decreased level of
- a mammal e.g., a human
- a melanoma e.g., a PCM
- the mammal can undergo surgery to remove the melanoma and can be administered or instructed to self-administer one or more adjuvant therapies.
- a mammal having a melanoma that is identified as having the presence of an altered level of 4 or more polypeptides in a sample (e.g., a tissue sample containing one or more melanoma cells) obtained from the mammal can undergo surgery to remove the melanoma and can be administered or instructed to self-administer one or more (e.g., one, two, three, four, five, or more) adjuvant therapies.
- An adjuvant therapy can be any appropriate cancer treatment.
- radiation therapy can be used as an adjuvant therapy with surgery to treat a mammal having a melanoma (e.g., a PCM) that is identified as being likely to relapse as described herein.
- a cancer treatment that can be used as an adjuvant therapy with surgery to treat a mammal having a melanoma (e.g., a PCM) that is identified as being likely to relapse as described herein can include administering one or more anti-cancer drugs (e.g., chemotherapeutic agents, targeted cancer drugs, and immunotherapy drugs) to the mammal.
- anti-cancer drugs e.g., chemotherapeutic agents, targeted cancer drugs, and immunotherapy drugs
- anti-cancer drugs that can be administered to a mammal having melanoma (e.g., a PCM) can include, without limitation, nivolumab (e.g., OPDIVO®), ipilimumab (e.g., YERVOY®), pembrolizumab (e.g., KEYTRUDA®), talimogene laherparepvec (T-VEC; e.g., IMLYGIC®), vemurafenib (e.g., ZELBORAF®), dabrafenib (e.g., TAFINLAR®), encorafenib (e.g., BRAFTOVI®), trametinib (e.g.,MEKINIST®), cobimetinib (e.g., COTELLIC®), binimetinib (e.g., MEKTOVI®), atezolizumab (e.g.,
- the treatment when treating a mammal (e.g., a human) having melanoma (e.g., PCM) as described herein, the treatment can be effective to treat the melanoma.
- the number of cancer cells present within a mammal can be reduced using the methods and materials described herein.
- the methods and materials described herein can be used to reduce the number of cancer cells present within a mammal having melanoma by, for example, 10, 20, 30, 40, 50, 60, 70, 80, 90, 95, or more percent. In some cases, the number of cancer cells present within a mammal does not increase.
- the size (e.g., volume) of one or more tumors present within a mammal can be reduced using the methods and materials described herein.
- the methods and materials described herein can be used to reduce the size of one or more tumors present within a mammal having melanoma (e.g., PCM) by, for example, 10, 20, 30, 40, 50, 60, 70, 80, 90, 95, or more percent.
- the size (e.g., volume) of one or more tumors present within a mammal does not increase.
- the treatment when treating a mammal (e.g., a human) having melanoma (e.g., PCM) as described herein, the treatment can be effective to treat the melanoma while minimizing the risk of relapse.
- the number of cancer cells present within a mammal can be reduced using the methods and materials described herein.
- the methods and materials described herein can be used to reduce the number of cancer cells present within a mammal having melanoma by, for example, 10, 20, 30, 40, 50, 60, 70, 80, 90, 95, or more percent. In some cases, the number of cancer cells present within a mammal does not increase.
- the size (e.g., volume) of one or more tumors present within a mammal can be reduced using the methods and materials described herein.
- the methods and materials described herein can be used to reduce the size of one or more tumors present within a mammal having melanoma (e.g., PCM) by, for example, 10, 20, 30, 40, 50, 60, 70, 80, 90, 95, or more percent.
- the size (e.g., volume) of one or more tumors present within a mammal does not increase.
- the treatment when treating a mammal (e.g., a human) having melanoma (e.g., PCM) as described herein, the treatment can be effective to improve survival of the mammal.
- the methods and materials described herein can be used to improve disease-free survival (e.g., relapse-free survival).
- the methods and materials described herein can be used to improve overall survival.
- the methods and materials described herein can be used to improve the survival of a mammal having melanoma (e.g., PCM) by, for example, 10, 20, 30, 40, 50, 60, 70, 80, 90, 95, or more percent.
- the methods and materials described herein can be used to improve the survival of a mammal having melanoma (e.g., PCM) by, for example, at least 6 months (e.g., about 6 months, about 8 months, about 10 months, about 1 year, about 1.5 years, about 2 years, about 2.5 years, or about 3 years).
- a mammal having melanoma e.g., PCM
- at least 6 months e.g., about 6 months, about 8 months, about 10 months, about 1 year, about 1.5 years, about 2 years, about 2.5 years, or about 3 years.
- the treatment when treating a mammal (e.g., a human) having melanoma (e.g., PCM) as described herein, the treatment can be effective to improve survival of the mammal while minimizing the risk of relapse.
- the methods and materials described herein can be used to improve disease-free survival (e.g., relapse-free survival).
- the methods and materials described herein can be used to improve overall survival.
- the methods and materials described herein can be used to improve the survival of a mammal having melanoma (e.g., PCM) by, for example, 10, 20, 30, 40, 50, 60, 70, 80, 90, 95, or more percent.
- the methods and materials described herein can be used to improve the survival of a mammal having melanoma (e.g., PCM) by, for example, at least 6 months (e.g., about 6 months, about 8 months, about 10 months, about 1 year, about 1.5 years, about 2 years, about 2.5 years, or about 3 years).
- a mammal having melanoma e.g., PCM
- at least 6 months e.g., about 6 months, about 8 months, about 10 months, about 1 year, about 1.5 years, about 2 years, about 2.5 years, or about 3 years.
- the treatment when treating a mammal (e.g., a human) having melanoma (e.g., PCM) as described herein, the treatment can be effective to reduce or eliminate one or more symptoms of the melanoma.
- symptoms of melanoma e.g., PCM
- Examples of symptoms of melanoma (e.g., PCM) that can be reduced or eliminated using the methods and materials described herein can include, without limitation, changes in one or more existing moles, development of a new pigmented and/or unusual-looking growth on the skin, sores that don’t heal, redness and/or swelling that spreads outside the border of a spot to the surrounding skin, itchiness, tenderness, pain, blurry vision, partial loss of sight, and dark spots in the iris.
- the methods and materials described herein can be used to reduce one or more symptoms of melanoma (e.g., PCM) within a mammal having melanoma by, for example, 10, 20, 30, 40, 50, 60, 70, 80, 90, 95, or more percent.
- melanoma e.g., PCM
- the treatment when treating a mammal (e.g., a human) having melanoma (e.g., PCM) as described herein, the treatment can be effective to reduce or eliminate one or more symptoms of the melanoma while minimizing the risk of relapse.
- a mammal e.g., a human
- melanoma e.g., PCM
- Examples of symptoms of melanoma that can be reduced or eliminated using the methods and materials described herein can include, without limitation, changes in one or more existing moles, development of a new pigmented and/or unusual-looking growth on the skin, sores that don’t heal, redness and/or swelling that spreads outside the border of a spot to the surrounding skin, itchiness, tenderness, pain, blurry vision, partial loss of sight, and dark spots in the iris.
- the methods and materials described herein can be used to reduce one or more symptoms of melanoma (e.g., PCM) within a mammal having melanoma by, for example, 10, 20, 30, 40, 50, 60, 70, 80, 90, 95, or more percent.
- melanoma e.g., PCM
- a course of treatment the number of cancer cells present within a mammal and/or the severity of one or more symptoms related to the melanoma (e.g., PCM) can be monitored.
- Any appropriate method can be used to determine whether or not the number of cancer cells present within a mammal is reduced.
- imaging techniques can be used to assess the number of cancer cells present within a mammal.
- Example 1 A prognostic gene expression signature for primary cutaneous melanoma
- This Example describes the identification of a gene expression signature for primary cutaneous melanoma that can be used to predict whether or not a melanoma patient is at a higher risk of relapse.
- Eligibility was based on histopathology data derived from patient medical records and established by two or more board-certified dermatopathologists. Inclusion was determined by institutional practice guidelines for recommending SLNb, which were based on Breslow thickness, ulceration, mitoses, and patient age. Patients were eligible for this study if they met one of the following three conditions: 1) Breslow thickness greater than 1.0 mm; 2) Breslow thickness of 0.75-0.99 mm and presence of ulceration, mitoses, or patient age less than 40 years; or 3) Breslow thickness of 0.50-0.74 mm and presence of at least two of the following: ulceration, mitoses and patient age less than 40 years.
- Exclusion criteria were as follows: Ml disease within 90 days of primary diagnosis; insufficient primary tumor diagnostic biopsy tissue; inadequate RNA harvested and, denial of access to medical records for research purposes. Patients were not excluded based on histologic type, but histologic type was recorded as a clinicopathologic variable.
- RNA sequencing data which was used for the discovery of the disclosed CP-GEP classifier, was derived from a subset of 382 of the 837 patients: o 384 samples were selected from the 837-patient cohort based on RNA quality, i.e., RIN scores, DV200 scores, concentration, fragment sizes, and the presence of primer dimers.
- RES Relapse-free survival
- RNA libraries were prepared according to the manufacturer's instructions for the TruSeq® RNA Exome Library Prep Kit by Illumina (San Diego, CA). o Coding regions of the transcriptome were captured by pooling four of the cDNA libraries at 200 ng each, following the TruSeq® RNA Exome Library Prep Kit instructions. o Libraries were multiplexed at 96 samples per flow cell, following Illumina’s standard protocol for the Illumina NovaSeqTM 6000 and S4 flow cell. The flow cells were sequenced as 100 X 2 paired-end reads using the NovaSeqTM S4 sequencing kit and NovaSeqTM Control Software vl.6.0. Base-calling was performed using Illumina’s RTA version 3.4.4. o An S4 flow cell’s total output is nine billion single-end reads, or 18 billion paired- end reads passing filters (about 94 million single-end reads per sample).
- the primary endpoint here was time to relapse after initial diagnosis of melanoma. Subjects who died, were lost to follow-up, or reached the end of the study period without relapse were censored at those respective time points.
- the q-value is an adjusted p-value, taking in to account the false discovery rate (FDR).
- Multivariate analysis association of gene expression with relapse-free survival
- Multivariate each expression association is adjusted for the independent effects of patient age at diagnosis, sex, ulcerations, Breslow depth and mitotic rate level.
- the Merlin genes are not the highest performing genes in the dataset.
- Example 2 CP-GEP models for predicting relapse
- the R glmnet package (version 4.1-1) was used to fit the LASSO models. Briefly, this method fits a penalized partial likelihood estimation algorithm to a Cox model (/
- ) L, (/) exp ⁇ A// ⁇ , subject to S
- ? 7 j ⁇ .s. Conditioning on the penalty term s allows for both parameter estimation and feature selection, as variables whose parameter estimates are shrunk to 0 are effectively removed from the prediction model. The number of relapses in the study (N 95) prohibited us from splitting the study set into training and testing sets. An alternative solution to this external validation approach is to internally validate the model by repeated cross-validation and average the predictive performance across the multiple test sets.
- This double loop cross-validation approach was as described elsewhere (Bellomo et al., JCO Precision Oncology, 2020:319-34 (2020)).
- this approach (1) randomly sorts the study set; (2) uses 10-fold cross-validation to estimate the LASSO penalty term; and (3) uses 3 -fold cross-validation and the penalty term from (2) to build/train a predictive model on two-thirds of the data and test the model on the remaining one-third, resulting in 3 predictive models. This process is repeated 100 times, generating a total of 300 predictive models. Due to the way the 3 -fold cross-validation approach assigns subjects to training and testing sets, each subject is included in exactly 100 of the 300 model test sets.
- Final time-specific relapse probability estimates for a given subject are then calculated by averaging their survival estimates at various times post-diagnosis across the 100 test set models.
- the overall predictive capability of the model was assessed using a survival-based concordance (c-) statistic, and time-specific predictive capabilities were assessed at various years postdiagnosis using receiver operating characteristics (ROC curves).
- the variables most predictive of relapse were determined based on the proportion of times they were included in the 300 LASSO models.
- One final model was then created by fitting these most predictive variables with Cox LASSO regression using a penalty term equal to the average of the penalty terms from the 100 loops. Gene filtering approach.
- Clinical variables includes:
- TMBV tumor mutational burden
- HJURP polypeptide an increased level of a HJURP polypeptide, an increased level of a NUF2 polypeptide, an increased level of a PPP1R9A polypeptide, an increased level of a SRSF11 polypeptide, an increased level of a NT5DC3 polypeptide, a decreased level of a PARM1 polypeptide, a decreased level of an EMP2 polypeptide, a decreased level of a PRKCB polypeptide, and a decreased level of a CD IE polypeptide in melanoma cells of a mammal having melanoma can be used to identify that mammal as being likely to relapse.
- Example 3 A prognostic gene expression signature for primary cutaneous melanoma
- the study cohort was derived from a previously published cohort of 854 patients diagnosed with stage I-III malignant melanoma who had an SLNb performed within 90 days of their diagnosis (Quattrocchi et al., Int. J. Dermatol., 59:1241-8 (2020)). Briefly, patients with primary cutaneous melanoma with known SLN status were retrospectively identified by electronic searches of pathology reports. Charts were then reviewed for eligibility criteria (see next paragraph), and if met, diagnostic biopsy tissue was requested. Patients underwent SLNb. Patients who presented with stage IV disease or who developed stage IV disease within 90 days of melanoma diagnosis were excluded from the cohort.
- all patients included were with stage LIIA disease (patients with early-stage primaries and no evidence of metastasis).
- PCR Quantitative polymerase chain reaction
- the primary endpoint for the study was time to relapse after initial diagnosis of melanoma. Subjects who died, were lost to follow-up, or reached the end of the study period without relapse were censored at those respective timepoints. Gene expression was examined using normalized cycle threshold values (ACt values). All continuous variables were modeled assuming a log-linear association with time to relapse.
- Multivariate models to predict time to relapse were built using Cox proportional hazards, least absolute shrinkage and selection operator (LASSO) regression with a double loop cross-validation (DLCV) component.
- the R glmnet package (version 4.1-1) was used to fit the LASSO models (Tibshirani et al., J. R. Stat. Soc., 58:267-88 (1996); and Tibshirani et al., Stat. Med., 16:385-95 (1997)). Briefly, this method fits a penalized partial likelihood estimation algorithm to a Cox model ⁇ (t ⁇ x) — (t) exp(A ? ⁇ , subject to £ ⁇ s.
- this approach (1) randomly sorts the study set; (2) uses 10-fold cross-validation to estimate the LASSO penalty term; and (3) uses 3-fold cross-validation and the penalty term from (2) to build/train a predictive model on two-thirds of the data and test the model on the remaining one-third, resulting in 3 predictive models. This process is repeated 100 times, generating a total of 300 predictive models. Due to the way the 3 -fold cross-validation approach assigns subjects to training and testing sets, each subject is included in exactly 100 of the 300 model test sets. Final time-specific relapse probability estimates for a given subject are then calculated by averaging their survival estimates at various times post-diagnosis across the 100 test set models.
- the overall predictive capability of the model was assessed using a survival-based concordance (c-)statistic, and time-specific predictive capabilities were assessed at various years post-diagnosis using receiver operating characteristics (ROC curves).
- the variables most predictive of relapse were determined based on the proportion of times they were included in the 300 LASSO models.
- One final model was then created by fitting these most predictive variables with Cox LASSO regression using a penalty term equal to the average of the penalty terms from the 100 loops.
- HJURP polypeptide and mRNA encoding a HJURP polypeptide
- NUF2 polypeptide and mRNA encoding a NUF2 polypeptide
- PPP1R9A polypeptide and mRNA encoding a PPP1R9A polypeptide
- SRSF11 polypeptide and mRNA encoding a SRSF11 polypeptide
- NT5DC3 polypeptide and mRNA encoding a NT5DC3 polypeptide
- SERPINE2 polypeptide and mRNA encoding a SERPINE2 polypeptide
- PARM1 polypeptide and mRNA encoding a PARM1 polypeptide
- EMP2 polypeptide and mRNA encoding an EMP2 polypeptide
- PRKCB polypeptide and mRNA encoding a PRKCB polypeptide
- CD IE polypeptide and mRNA IE polypeptide
- a tissue sample containing one or more melanoma cells is obtained from a human having PCM.
- the obtained sample is examined for the presence or absence of an altered level of a HJURP polypeptide, a NUF2 polypeptide, a PPP 1R9A polypeptide, a SRSF11 polypeptide, a NT5DC3 polypeptide, a SERPINE2 polypeptide, a PARMl polypeptide, an EMP2 polypeptide, a PRKCB polypeptide, a CD IE polypeptide, an ALDH2 polypeptide, a CD200R polypeptide.
- the PCM is identified as being likely to relapse (e.g., likely to relapse following treatment)
- the human is subjected to surgery to remove the PCM and
- the surgery in combination with the one or more adjuvant therapies can reduce number of cancer cells within the human while minimizing the risk of relapse.
- a tissue sample containing one or more melanoma cells is obtained from a human having PCM.
- the obtained sample is examined for the presence or absence of an altered level of a HJURP polypeptide, a NUF2 polypeptide, a PPP 1R9A polypeptide, a SRSF11 polypeptide, a NT5DC3 polypeptide, a SERPINE2 polypeptide, a PARMl polypeptide, an EMP2 polypeptide, a PRKCB polypeptide, a CD IE polypeptide, an ALDH2 polypeptide, a CD200R polypeptide.
- the PCM is identified as not being likely to relapse (e.g., likely to relapse following treatment), and the human is subjected to surgery to remove the PCM without any adjuvant therapy.
- the surgery can reduce number of cancer cells within the human while sparing the human from unnecessary toxicities and/or expenses of adjuvant therapies.
- a tissue sample containing one or more melanoma cells is obtained from a human having PCM.
- the obtained sample is examined for the level of a nucleic acid (e.g., an mRNA) encoding a HJURP polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a NUF2 polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a PPP 1R9A polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a SRSF11 polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a NT5DC3 polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a SERPINE2 polypeptide, the level of a nucleic acid (e.g., an mRNA) en
- the level of a nucleic acid (e.g., an mRNA) encoding a HJURP polypeptide is greater than 0.3 pg/melanoma cell
- the level of a nucleic acid (e.g., an mRNA) encoding a NUF2 polypeptide is greater than 0.19 pg/melanoma cell
- the level of a nucleic acid (e.g., an mRNA) encoding a PPP1R9A polypeptide is greater than 0.77 pg/melanoma cell
- the level of a nucleic acid (e.g., an mRNA) encoding a SRSF11 polypeptide is greater than 1.71 pg/melanoma cell
- the level of a nucleic acid (e.g., an mRNA) encoding a NT5DC3 polypeptide is greater than 3.28 pg/melanoma cell
- the surgery in combination with the one or more adjuvant therapies can reduce number of cancer cells within the human while minimizing the risk of relapse.
- a tissue sample containing one or more melanoma cells is obtained from a human having PCM.
- the obtained sample is examined for the level of a nucleic acid (e.g., an mRNA) encoding a HJURP polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a NUF2 polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a PPP 1R9A polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a SRSF11 polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a NT5DC3 polypeptide, the level of a nucleic acid (e.g., an mRNA) encoding a SERPINE2 polypeptide, the level of a nucleic acid (e.g., an mRNA) en
- the level of a nucleic acid (e.g., an mRNA) encoding a HJURP polypeptide is from about 0.17 pg/melanoma cell to about 0.3 pg/melanoma cell
- the level of a nucleic acid (e.g., an mRNA) encoding a NUF2 polypeptide is from about 0.11 pg/melanoma cell to about 0.19 pg/melanoma cell
- the level of a nucleic acid tAf is from about 0.11 pg/melanoma cell to about 0.19 pg/melanoma cell.
- an mRNA) encoding a PPP1R9A polypeptide is from about 0.37 pg/melanoma cell to about 0.77 pg/melanoma cell
- the level of a nucleic acid (e.g., an mRNA) encoding a SRSF11 polypeptide is from about 0.79 pg/melanoma cell to about 1.71 pg/melanoma cell
- the level of a nucleic acid (e.g., an mRNA) encoding a NT5DC3 polypeptide is from about 1.5 pg/melanoma cell to about 3.28 pg/melanoma cell
- the level of a nucleic acid (e.g., an mRNA) encoding a SERPINE2 polypeptide is from about 0.4 pg/melanoma cell to about 4.48 pg/melanoma cell
- the surgery can reduce number of cancer cells within the human while sparing the human from unnecessary toxicities and/or expenses of adjuvant therapies.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Engineering & Computer Science (AREA)
- Immunology (AREA)
- Molecular Biology (AREA)
- Pathology (AREA)
- Analytical Chemistry (AREA)
- Urology & Nephrology (AREA)
- Biomedical Technology (AREA)
- Hematology (AREA)
- Organic Chemistry (AREA)
- General Health & Medical Sciences (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Physics & Mathematics (AREA)
- Biochemistry (AREA)
- Microbiology (AREA)
- Biotechnology (AREA)
- Medicinal Chemistry (AREA)
- Genetics & Genomics (AREA)
- Wood Science & Technology (AREA)
- Zoology (AREA)
- Food Science & Technology (AREA)
- General Physics & Mathematics (AREA)
- Cell Biology (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Oncology (AREA)
- Biophysics (AREA)
- Hospice & Palliative Care (AREA)
- Tropical Medicine & Parasitology (AREA)
- Physiology (AREA)
- General Engineering & Computer Science (AREA)
- General Chemical & Material Sciences (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Dermatology (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Pharmacology & Pharmacy (AREA)
- Animal Behavior & Ethology (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
Abstract
Description







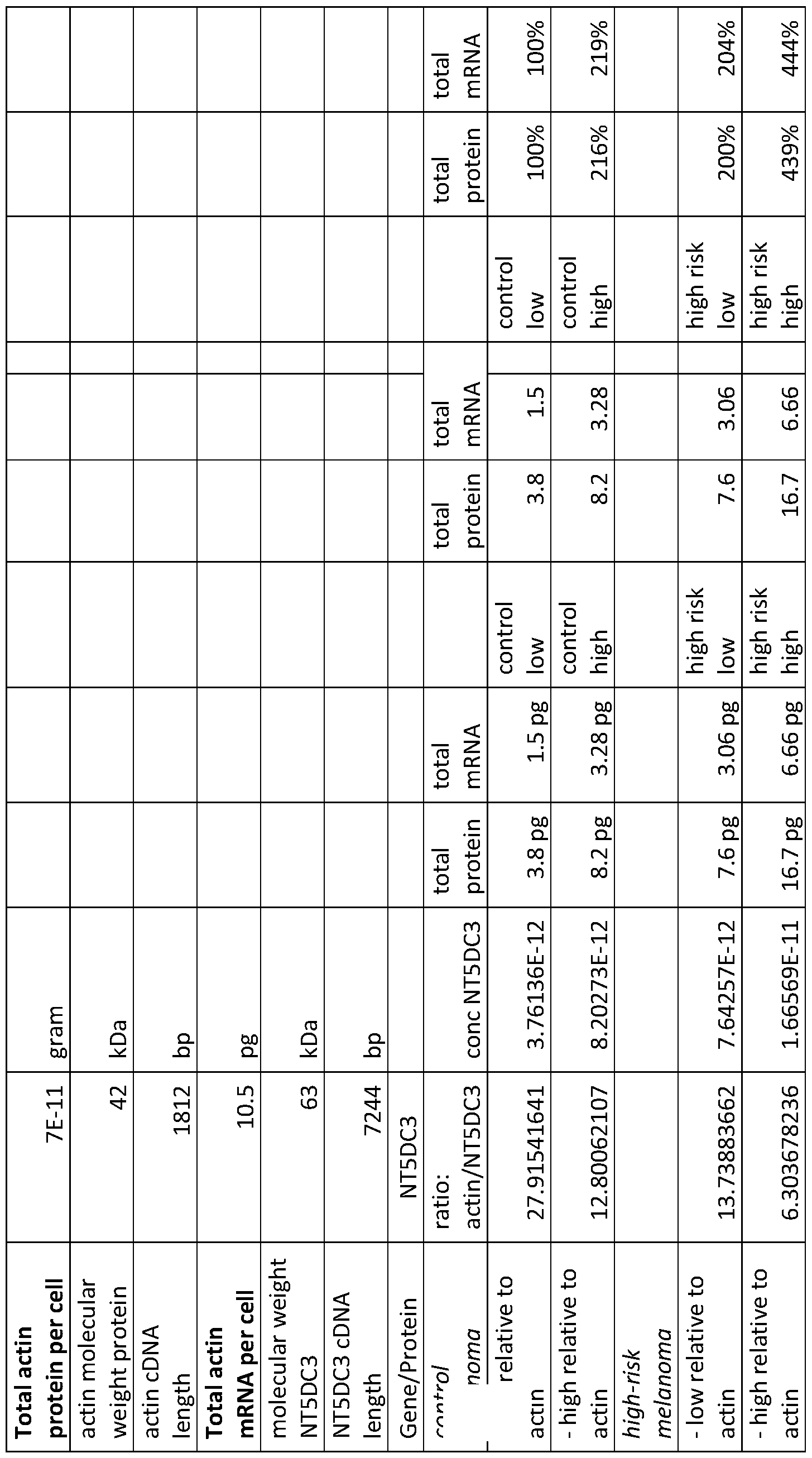







Claims
Priority Applications (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| AU2022406744A AU2022406744A1 (en) | 2021-12-08 | 2022-12-01 | Assessing and treating melanoma |
| US18/717,252 US20250043359A1 (en) | 2021-12-08 | 2022-12-01 | Assessing and treating melanoma |
| CA3240376A CA3240376A1 (en) | 2021-12-08 | 2022-12-01 | Assessing and treating melanoma |
| EP22904935.8A EP4445142A4 (en) | 2021-12-08 | 2022-12-01 | ASSESSMENT AND TREATMENT OF MELANOMAS |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US202163287217P | 2021-12-08 | 2021-12-08 | |
| US63/287,217 | 2021-12-08 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2023107328A1 true WO2023107328A1 (en) | 2023-06-15 |
Family
ID=86731047
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2022/051517 Ceased WO2023107328A1 (en) | 2021-12-08 | 2022-12-01 | Assessing and treating melanoma |
Country Status (5)
| Country | Link |
|---|---|
| US (1) | US20250043359A1 (en) |
| EP (1) | EP4445142A4 (en) |
| AU (1) | AU2022406744A1 (en) |
| CA (1) | CA3240376A1 (en) |
| WO (1) | WO2023107328A1 (en) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP4445137A4 (en) * | 2021-12-08 | 2025-12-10 | Mayo Found Medical Education & Res | ASSESSMENT AND TREATMENT OF MELANOMAS |
Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20080113360A1 (en) * | 2006-09-07 | 2008-05-15 | Riker Adam I | Melanoma Gene Signature |
| US20140271545A1 (en) * | 2013-03-14 | 2014-09-18 | Castle Biosciences, Inc. | Methods for predicting risk of metastasis in cutaneous melanoma |
| US20170107577A1 (en) * | 2014-03-11 | 2017-04-20 | The Council Of The Queensland Institute Of Medical Research | Determining Cancer Aggressiveness, Prognosis and Responsiveness to Treatment |
| US20210301353A1 (en) * | 2018-07-25 | 2021-09-30 | Skylinedx B.V. | Gene signatures for predicting metastasis of melanoma and patient prognosis |
Family Cites Families (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20140302042A1 (en) * | 2011-07-01 | 2014-10-09 | Dana-Farber Cancer Institute, Inc. | Methods of predicting prognosis in cancer |
-
2022
- 2022-12-01 CA CA3240376A patent/CA3240376A1/en active Pending
- 2022-12-01 EP EP22904935.8A patent/EP4445142A4/en active Pending
- 2022-12-01 US US18/717,252 patent/US20250043359A1/en active Pending
- 2022-12-01 WO PCT/US2022/051517 patent/WO2023107328A1/en not_active Ceased
- 2022-12-01 AU AU2022406744A patent/AU2022406744A1/en active Pending
Patent Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20080113360A1 (en) * | 2006-09-07 | 2008-05-15 | Riker Adam I | Melanoma Gene Signature |
| US20140271545A1 (en) * | 2013-03-14 | 2014-09-18 | Castle Biosciences, Inc. | Methods for predicting risk of metastasis in cutaneous melanoma |
| US20170107577A1 (en) * | 2014-03-11 | 2017-04-20 | The Council Of The Queensland Institute Of Medical Research | Determining Cancer Aggressiveness, Prognosis and Responsiveness to Treatment |
| US20210301353A1 (en) * | 2018-07-25 | 2021-09-30 | Skylinedx B.V. | Gene signatures for predicting metastasis of melanoma and patient prognosis |
Non-Patent Citations (2)
| Title |
|---|
| EGGERMONT ALEXANDER M.M.; BELLOMO DOMENICO; ARIAS-MEJIAS SUZETTE M.; QUATTROCCHI ENRICA; SOMINIDI-DAMODARAN SINDHUJA; BRIDGES ALIN: "Identification of stage I/IIA melanoma patients at high risk for disease relapse using a clinicopathologic and gene expression model", EUROPEAN JOURNAL OF CANCER, ELSEVIER, AMSTERDAM NL, vol. 140, 5 October 2020 (2020-10-05), Amsterdam NL , pages 11 - 18, XP086335435, ISSN: 0959-8049, DOI: 10.1016/j.ejca.2020.08.029 * |
| See also references of EP4445142A4 * |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP4445137A4 (en) * | 2021-12-08 | 2025-12-10 | Mayo Found Medical Education & Res | ASSESSMENT AND TREATMENT OF MELANOMAS |
Also Published As
| Publication number | Publication date |
|---|---|
| CA3240376A1 (en) | 2023-06-15 |
| US20250043359A1 (en) | 2025-02-06 |
| AU2022406744A1 (en) | 2024-07-11 |
| EP4445142A1 (en) | 2024-10-16 |
| EP4445142A4 (en) | 2025-11-26 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| JP6351112B2 (en) | Gene expression profile algorithms and tests to quantify the prognosis of prostate cancer | |
| Sanchez‐Palencia et al. | Gene expression profiling reveals novel biomarkers in nonsmall cell lung cancer | |
| JP6140202B2 (en) | Gene expression profiles to predict breast cancer prognosis | |
| WO2019222657A1 (en) | Cell-free dna for assessing and/or treating cancer | |
| US20060199210A1 (en) | Methods and kits for monitoring Barrett's metaplasia | |
| CN103459597A (en) | Marker for predicting prognosis of gastric cancer and method for predicting prognosis of gastric cancer | |
| JP7239477B2 (en) | Algorithms and methods for evaluating late-stage clinical endpoints in prostate cancer | |
| CN113234818A (en) | Prostate cancer marker gene combination and application | |
| CN113039289B (en) | Gene signatures for predicting melanoma metastasis and patient prognosis | |
| US20250043359A1 (en) | Assessing and treating melanoma | |
| Schummer et al. | Comparison of breast cancer to healthy control tissue discovers novel markers with potential for prognosis and early detection | |
| BR112020012280A2 (en) | compositions and methods for diagnosing lung cancers using gene expression profiles | |
| JP2022512634A (en) | Preoperative risk stratification based on PDE4D7 and DHX9 expression | |
| EP4445137A1 (en) | Assessing and treating melanoma | |
| CA3090743A1 (en) | Patient classification and prognostic method | |
| CN110914453B (en) | Biomarkers of atherosclerotic cardiovascular disease | |
| WO2023089146A1 (en) | Prognostic and treatment response predictive method | |
| JP7313374B2 (en) | Postoperative risk stratification based on PDE4D mutation expression and postoperative clinical variables, selected by TMPRSS2-ERG fusion status | |
| RU2593020C2 (en) | Method for prediction of sensitivity to chemotherapy in patients suffering from lymphoproliferative diseases | |
| JP2017118841A (en) | Effect prediction marker for immunotherapy | |
| EP4616197A2 (en) | Methods and materials for assessing and treating cutaneous squamous cell carcinoma | |
| JP2024546521A (en) | Method for predicting prognosis of breast cancer treatment based on cell-free DNA in blood | |
| Dobrovic | P1. 16-11 Monitoring of Early Stage Lung Cancer Using Liquid Biopsies | |
| CN121215234A (en) | Models for predicting the response of glucocorticoids to SLE treatment and their applications | |
| Kashani-Sabet | Melanoma Genomics |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 22904935 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 3240376 Country of ref document: CA |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2022406744 Country of ref document: AU Ref document number: AU2022406744 Country of ref document: AU |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2022904935 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2022904935 Country of ref document: EP Effective date: 20240708 |