WO2023239937A1 - Gpcr inhibitors and uses thereof - Google Patents
Gpcr inhibitors and uses thereof Download PDFInfo
- Publication number
- WO2023239937A1 WO2023239937A1 PCT/US2023/024983 US2023024983W WO2023239937A1 WO 2023239937 A1 WO2023239937 A1 WO 2023239937A1 US 2023024983 W US2023024983 W US 2023024983W WO 2023239937 A1 WO2023239937 A1 WO 2023239937A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- cell
- cxcr4
- inhibitor
- beta
- subject
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/66—Phosphorus compounds
- A61K31/675—Phosphorus compounds having nitrogen as a ring hetero atom, e.g. pyridoxal phosphate
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/13—Amines
- A61K31/135—Amines having aromatic rings, e.g. ketamine, nortriptyline
- A61K31/138—Aryloxyalkylamines, e.g. propranolol, tamoxifen, phenoxybenzamine
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/18—Growth factors; Growth regulators
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/19—Cytokines; Lymphokines; Interferons
- A61K38/193—Colony stimulating factors [CSF]
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/39—Medicinal preparations containing antigens or antibodies characterised by the immunostimulating additives, e.g. chemical adjuvants
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/395—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K40/00—Cellular immunotherapy
- A61K40/50—Cellular immunotherapy characterised by the use of allogeneic cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2866—Immunoglobulins [IG], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against receptors for cytokines, lymphokines, interferons
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K2239/00—Indexing codes associated with cellular immunotherapy of group A61K40/00
- A61K2239/39—Indexing codes associated with cellular immunotherapy of group A61K40/00 characterised by a specific adjuvant, e.g. cytokines or CpG
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K2300/00—Mixtures or combinations of active ingredients, wherein at least one active ingredient is fully defined in groups A61K31/00 - A61K41/00
Definitions
- beta blockers appear to have potential to improve hematopoietic stem cell mobilization by restoring bone marrow function.
- CXCR4 antagonists like Burixafor (also referred to as GPC-100 or TG-0054), as well as Plerixafor (also referred to as AMD3100 or Mozobil), have been used clinically in combination with granulocyte-colony stimulating factor (G-CSF) for hematopoietic stem cell mobilization and subsequent autologous stem cell transplant in non-Hodgkin’s Lymphoma and multiple myeloma patients.
- G-CSF granulocyte-colony stimulating factor
- a G-CSF regimen involves repeated multi-day injections and is associated with adverse side effects like severe bone pain.
- FIG. 4 shows data for mice that were administered GPC100 after propranolol pretreatment, showing that white blood cells were mobilized to the extent that was comparable to those that received G-CSF.
- FIGS. 5A-5B show cumulative data of several experiments, showing a large variation in mobilization in white blood cells (FIG. 5A) and lymphocytes (FIG. 5B) from the combination treatment of G-CSF and AMD3100.
- FIGS. 6A-6B shows data for G-CSF enhanced mobilization by GPC100 with or without propranolol pretreatment in WBC (FIG. 6A) and progenitor cells (FIG. 6B).
- FIGS. 7A-7C show data pooled from four experiments indicating that when combined with G-CSF, GPC100 mobilized more WBC compared to AMD3100, with addition of propranolol not altering the overall WBC count for any groups (FIG. 7A), lymphocyte counts suggesting that propranolol enhanced their mobilization when added to the G-CSF and GPC100 combination (FIG. 7B), and distribution of WBC differential count showing that addition of propranolol increased lymphocyte trafficking into the peripheral blood (FIG. 7C).
- FIGS. 8A-8D show enhancement in mobilization of white blood cells (FIG. 8A), lymphocytes (FIG. 8B), neutrophils (FIG. 8C), and monocytes (FIG. 8D) by propranolol pretreatment.
- FIG. 9 shows data from three studies showing a significant increase in GPCIOO-induced mobilization after propranolol pretreatment.
- FIGS. 10A-10D show data demonstrating an increase in mobilized white blood cells (FIG. 10A), lymphocytes (FIG. 10B), neutrophils (FIG. 10C), and monocytes (FIG. 10D) from propranolol pretreatment mainly due to lymphocytes, as opposed to an SOC regimen mainly mobilizing neutrophils.
- FIG. 11 shows data demonstrating an increase in mobilized WBCs from propranolol pretreatment mainly due to lymphocytes, as opposed to an SOC regimen mainly mobilizing neutrophils.
- FIG. 14 shows data for determination of hematopoietic stem cell mobilization with the dosing regimen by flow cytometry, with no significant difference observed from the standard of care for LSK Cells.
- FIG. 15 shows data for determination of hematopoietic stem cell mobilization with the dosing regimen by flow cytometry, with no significant difference observed from the standard of care for Lin-CXCR4+ cells.
- FIG. 16 shows data demonstrating that the addition of propranolol to the combination of G-CSF and GPC100 caused maximum mobilization of WBCs, with a significant increase in mobilization compared to SOC or G-CSF and GPC100 combination treatment.
- FIGS. 17A-17C shows data demonstrating that the addition of propranolol to the combination of G-CSF and GPC100 caused maximum mobilization of neutrophils (FIG. 17A), lymphocytes (FIG. 17B), and monocytes (FIG. 17C), with a significant increase in mobilization compared to SOC or G-CSF and GPC100 combination treatment.
- FIG. 18 shows that GPC100 in combination with propranolol increased lymphocytes, while GPC100 in combination with G-CSF increased Neutrophils.
- FIGS. 19A-19B show that increased mobilized circulating WBCs (FIG. 19A) and Colony Formation Units (FIG. 19B) was observed in groups with G-CSF.
- FIG. 21 is a schematic of a study focused on mobilization into the peripheral blood.
- FIG. 22 shows data for GPCIOO-induced mobilization in white blood cells in mice.
- FIG. 23 shows data for time-dependent GPC 100-induced mobilization in white blood cells in mice.
- FIGS. 24A-24C show that 7-day administration of propranolol enhanced GPC 100 induced mobilization of white blood cells (FIG. 24A), lymphocytes (FIG. 24B), and neutrophils (FIG. 24C) but had no effect on blood counts when administered alone.
- FIGS. 25A-25C show that Nadolol enhanced GPC 100-induced mobilization of white blood cells (FIG. 25A), lymphocytes (FIG. 25B), and neutrophils (FIG. 25C).
- FIGS. 26A-26C show that 7-day beta-blocker administration with a single GPC100 did not increase LSK and Lin-CXCR4+ cells.
- FIGS. 27A-27C show that propranolol was observed to enhance GPCIOO-induced mobilization of white blood cells (FIG. 27A), lymphocytes (FIG. 27B), and neutrophils (FIG.
- FIG. 28 shows that lymphocytes increased with GPC 100 and beta blockers, while neutrophils increased with G-CSF + AMD3100.
- FIGS. 31A-31C show mobilization data for white blood cells (FIG. 31A), lymphocytes (FIG. 31B), and neutrophils (FIG. 31C) for the triple combination.
- FIG. 32 shows data of white blood cell populations for the triple combination.
- FIG. 34 is a schematic for a colony forming unit assay.
- FIG. 35 shows data showing that the triple combination mobilized the highest number of progenitor cells.
- FIGS. 36A-36B show data showing that the triple combination resulted in the highest number of colony-forming units (FIG. 36A) and burst-forming units (FIG. 36B).
- FIG. 37 shows images of BFU-E colonies (left) and CFU-GM colonies (right) from G- CSF and GPC-100 combination treatment (top), and G-CSF + AMD3100 combination treatment (bottom).
- FIGS. 38A-38B show data showing that the triple combination was associated with the maximum increase in circulating WBCs (FIG. 38A) as well as progenitor cells, measured by total colony forming units (FIG. 38B) compared to other drug groups.
- FIGS. 39A-39B show total CFU after G-CSF combination treatments (FIG. 39A) and treatment with GPC100 with and without propranolol (FIG. 39B).
- FIGS. 40A-40B show cumulative data from three studies regarding the effect of propranolol on GPC 100- induced mobilization of white blood cells (FIG. 40A) and lymphocytes (FIG. 40B).
- FIGS. 42A-42C show data from a study of GPC 100, AMD3100 or G-CSF induced WBC mobilization of white blood cells (FIG. 42A), lymphocytes (FIG. 42B), and neutrophils (FIG. 42C) using a single agent.
- FIGS. 43A-43B show data on the effect of propranolol on GPCIOO-induced mobilization in the absence or presence of G-CSF in comparison with standard of care (SOC) in WBC for study 4 (FIG. 43A) and study 5 (FIG. 43B).
- FIGS. 44A-44B show data on the effect of propranolol on GPCIOO-induced mobilization in the absence or presence of G-CSF in comparison with standard of care (SOC) in lymphocytes for study 4 (FIG. 44A) and study 5 (FIG. 44B).
- FIGS. 45A-45B show data on the effect of propranolol on GPCIOO-induced mobilization in the absence or presence of G-CSF in comparison with standard of care (SOC) in neutrophils for study 4 (FIG. 45A) and study 5 (FIG. 45B).
- FIGS. 46A-46C show data for a comparison study of mobilization of white blood cells (FIG. 46A), lymphocytes (FIG. 46B), and neutrophils (FIG. 46C) between GPC 100 and AMD3100.
- FIGS. 50A-50B show that the addition of propranolol to the G-CSF and GPC100 combination mobilized significantly more WBC (FIG. 50A) and lymphocytes (FIG. 50B) compared to the standard of care.
- FIGS. 51A-51B show combined data from six studies showing that 7-day propranolol treatment prior to GPC100 results in significantly enhanced WBC (FIG. 51A) and lymphocyte (FIG. 51B) cell counts in peripheral blood compared to GPC100 alone.
- FIGS. 52A-52B show that the standard of care regimen mobilized more WBCs (FIG. 52A) but not lymphocytes (FIG. 52B) compared to the propranolol and GPC100 combination.
- FIGS. 55A-55C show data for GPC100, AMD3100 or G-CSF induced WBC (FIG. 55A), lymphocyte (FIG. 55B), and neutrophil (FIG. 55C) mobilization.
- FIGS. 56A-56C show data for a comparison study of mobilization of white blood cells (FIG. 56A), lymphocytes (FIG. 56B), and neutrophils (FIG. 56C) between GPC100 and AMD3100.
- FIGS. 57A-57C show data showing the effect of propranolol on GPCIOO-induced mobilization of white blood cells (FIG. 57A), lymphocytes (FIG. 57B), and neutrophils (FIG. 57C) with or without G-CSF, in comparison with standard of care.
- FIGS. 58A-58B show combined data from three studies showing that when combined with G-CSF, GPC100 was observed to mobilize significantly more WBCs (FIG. 58A) and lymphocytes (FIG. 58B), compared to AMD3100.
- FIGS. 59A-59F shows that GPC100 inhibition of CXCR4 can be modulated by propranolol, in an in vitro activity assay (FIG. 59A), mobilization assay (FIG. 59B), co- localization of CXCR4 and B2AR in MDA-MB-231 cells expression CXCR4 and B2AR (FIG. 59C) and control cells expressing CXCR4 alone (FIG. 59D), and Ca2+ flux assays in MDA-MB- 231 inhibited with GPC-100 (FIG. 59E) or AMD3100 (FIG. 59F).
- FIGS. 59A-59F shows that GPC100 inhibition of CXCR4 can be modulated by propranolol, in an in vitro activity assay (FIG. 59A), mobilization assay (FIG. 59B), co- localization of CXCR4 and B2AR in MDA-MB-231 cells expression CXCR4 and B2AR (FI
- FIG. 62 shows mobilization of hematopoietic stem cells as measured by LSK cells by flow cytometry.
- FIG. 65 shows induction of mobilization by GPC-100 and propranolol combination compared with the standard of care, G-CSF.
- FIG. 66 shows that WBC mobilization was significantly greater compared to the increased WBC count by G-CSF alone (4.5-fold) or G-CSF plus AMD3100 (6.6-fold).
- FIG. 67A-67D shows total CFUs (CFU-GM + BFU) (FIG. 67A), BFUs (FIG. 67C), and both CFU-GM (clear bars) and BFUs (solid bars) (FIG. 67B) as well as WBC migration (FIG. 67D) after triple combination.
- AML acute myeloid leukemia
- ADORA3 Adenosine A3 Receptor
- AD0RA2B Adenosine Receptor A2b
- AdHTS adenovirus high-throughput system
- AdHTS AdHTS
- ADCYAP1R1 Adrenoceptor Alpha 1A
- ADRB2 Adrenoceptor Beta 2
- APLNR Apelin Receptor
- APLNR Atypical chemokine receptor 3
- BiFC bimolecular fluorescence complementation
- BRET Bioluminescence Resonance Energy Transfer
- BRET Bioluminescence Resonance Energy Transfer
- BRET Bioluminescence Resonance Energy Transfer
- BRET Bioluminescence Resonance Energy Transfer
- BRET Bioluminescence Resonance Energy Transfer
- BRET Bioluminescence Resonance Energy Transfer
- BRET Bioluminescence Resonance Energy Transfer
- BRET Bioluminescence Resonance Energy Transfer
- BRET bovine serum albumin
- CALCR Calciton
- White blood cells play a crucial part in maintaining the health and viability of animals, including humans.
- White blood cells part of the body’s immune system that help the body fight infection and other diseases, include granulocytes (neutrophils, eosinophils and basophils/mast cells), monocytes/macrophages, as well the lymphocytes (T and B cells) of the immune system.
- White blood cells are continuously replaced via the hematopoietic system, by the action of colony stimulating factor (CSF) and various cytokines on stem cells and progenitor cells in hematopoietic tissues.
- CSF colony stimulating factor
- Mature blood cells are derived from hematopoietic precursor (progenitor) cells and stem cells present in specific hematopoietic tissues including bone marrow. Within these environments hematopoietic cells proliferate and differentiate prior to entering the circulation.
- chemokine receptor CXCR4 and its natural ligand stromal cell derived factor- 1 appear to be important in this process (for reviews, see Maekawa, T., et al., Internal Med. (2000) 39:90-100; Nagasawa, T., et al., Int. I. Hematol. (2000) 72:408-411). This is demonstrated by reports that CXCR4 or SDF-1 knock-out mice exhibit embryonic lethality and hematopoietic defects (Ma, Q., et al., Proc. Natl. Acad.
- CD34+ progenitor cells express CXCR4 and require SDF-1 produced by bone marrow stromal cells for chemo attraction and engraftment (Peled, A., et al., Science (1999) 283:845-848). It is also known that, in vitro, SDF-1 is chemotactic for both CD34+ cells (Aiuti, A., et al., J. Exp. Med.
- SDF-1 is also an important chemoattractant, signaling via the CXCR4 receptor, for several other more committed progenitors and mature blood cells including T-lymphocytes and monocytes (Blcul, C., ct al., J. Exp. Med. (1996) 184:1101-1109), pro-and pre-B lymphocytes (Fedyk, E. R., et al., J. Leukoc.
- SDF-1 is able to control the positioning and differentiation of cells bearing CXCR4 receptors whether these cells are stem cells (i.e., cells which are CD34+) and/or progenitor cells (which, being either CD34+ or CD34-, can result in the formation of specified types of colonies in response to particular stimuli) or cells that are somewhat more differentiated.
- stem cells i.e., cells which are CD34+
- progenitor cells which, being either CD34+ or CD34-, can result in the formation of specified types of colonies in response to particular stimuli
- cells that are somewhat more differentiated are somewhat more differentiated.
- CD34+ cells mobilized in the pool of peripheral blood progenitor cells used for autologous stem cell transplantation.
- the CD34+ population is the component thought to be primarily responsible for the improved recovery time after chemotherapy and the cells most likely responsible for long-term engraftment and restoration of hematopoiesis (Croop, J.
- CD34+ cells re-engraft may be due to the chemotactic effects of SDF-1 on CXCR4 expressing cells (Voermans, C. Blood, 2001, 97, 799- 804; Ponomaryov, T., et al., J. Clin. Invest. (2000) 106:1331-1339).
- adult hematopoietic stem cells were shown to be capable of restoring damaged cardiac tissue in mice (Jackson, K., et al., J. Clin. Invest. (2001) 107:1395-1402; Kocher, A., et al., Nature Med. (2001) 7:430-436).
- the role of the CXCR4 receptor in managing cell positioning and differentiation has assumed considerable significance.
- progenitor cells refers to cells that, in response to certain stimuli, can form differentiated hematopoietic or myeloid cells.
- the presence of progenitor cells can be assessed by the ability of the cells in a sample to form colony-forming units of various types, including, for example, CFU-GM (colony-forming units, granulocyte-macrophage); CFU- GEMM (colony-forming units, multipotential); BFU-E (burst-forming units, erythroid); HPP-CFC (high proliferative potential colony-forming cells); or other types of differentiated colonies which can be obtained in culture using known protocols.
- CFU-GM colony-forming units, granulocyte-macrophage
- CFU- GEMM colony-forming units, multipotential
- BFU-E burst-forming units, erythroid
- HPP-CFC high proliferative potential colony-forming cells
- stem cells are less differentiated forms of progenitor cells. Typically, such cells arc often positive for CD34. Some stem cells do not contain this marker, however. These CD34+ cells can be assayed using fluorescence activated cell sorting (FACS) and thus their presence can be assessed in a sample using this technique. In general, CD34+ cells are present only in low levels in the blood, but are present in large numbers in bone marrow. While other types of cells such as endothelial cells and mast cells also may exhibit this marker, CD34 is considered an index of stem cell presence.
- FACS fluorescence activated cell sorting
- CXCR4 refers to C-X-C Motif Chemokine Receptor 4, also identified by unique database identifiers (IDs) and alternate names as shown in Table 1 (Chatterjee et al., 2014; Debnath et al., 2013; Domanska et al., 2013; Guo et al., 2016; Peled et al., 2012; Roccaro et al., 2014; Walenkamp et al., 2017). Table 1 also provides the nomenclature of CXCR4 and GPCRx that form heteromers with CXCR4 and synergistically enhance Ca2+ response upon co- stimulation with both agonists.
- GPCRx refers to GPCRs that were used in this study to investigate if these GPCRs interact with CXCR4 and show properties distinct from those of individual protomers, including ADCYAP1R1 (ADCYAP Receptor Type I), ADORA2B (Adenosine A2b Receptor), AD0RA3 (Adenosine A3 Receptor), ADRB2 (Adrenoceptor Beta 2), APLNR (Apelin Receptor), C5AR1 (Complement C5a Receptor 1), CALCR (Calcitonin Receptor), CCR5 (Chemokine (C-C Motif) Receptor 5), CHRM1 (Cholinergic Receptor Muscarinic 1), GALR1 (Galanin Receptor 1), EDNRB (Endothelin Receptor Type B), HRH1 (Histamine Receptor Hl), MLNR (Motilin Receptor), NTSR1 (Neu).
- inhibitor refers to molecule that inhibits or suppresses the enhanced function of a CXCR4, a beta-adrenergic receptor, a GPCR, a heteromer of CXCR4 and a beta-adrenergic receptor, and/or a CXCR4-GPCRx heteromer.
- Non-limiting examples of the inhibitor of the invention that can be used for mobilization of cells include GPCRx antagonist, GPCRx inverse agonist, GPCRx positive and negative allosteric modulator, CXCR4-GPCRx heteromer- specific antibody or its antigen biding portions including single-domain antibody-like scaffolds, bivalent ligands which have a pharmacophore selective for CXCR4 joined by a spacer arm to a pharmacophore selective for GPCRx, bispecific antibody against CXCR4 and GPCRx, radiolabeled CXCR4 ligand linked with GPCRx ligand, and small molecule ligands that inhibit heteromer- selective signaling.
- Antagoni t refers to a type of receptor ligand or drug that blocks or dampens a biological response by binding to and blocking a receptor, also called blockers. Antagonists have affinity but no efficacy for their cognate receptors, and their binding disrupts the interaction and inhibit the function of an agonist or inverse agonist at the cognate receptors. Certain examples of antagonists against GPCRx that form heteromers with CXCR4 and enhance Ca2+ response upon co-stimulation with both agonists are listed in Table 2.
- heteromer refers to macromolecular complex composed of at least two GPCR units [protomers] with biochemical properties that are demonstrably different from those of its individual components. Heteromerization can be evaluated by in situ hybridization, immunohistochemistry, RNAseq, Reverse transcription-quantitative PCR (RT- qPCR, realtime PCR), microarray, proximity ligation assay (PLA), time-resolved FRET (TR- FRET), whole -body Single-photon emission computed tomography (SPECT) or Positron Emission Tomography /Computed Tomography (PET/CT).
- the phrase "effective amount” as used herein refers to an amount sufficient to effect beneficial or desired results.
- An effective amount can be administered in one or more administrations, applications or dosages. Such delivery is dependent on a number of variables including the time period for which the individual dosage unit is to be used, the bioavailability of the agent, the route of administration, etc.
- the phrase “therapeutically effective amount” as used herein refers to the amount of a therapeutic agent (c.g., an inhibitor, an antagonist, or any other therapeutic agent provided herein) which is sufficient to reduce, ameliorate, and/or prevent the severity and/or duration of a cancer and/or a symptom related thereto.
- a therapeutically effective amount of a therapeutic agent can be an amount necessary for the reduction, amelioration, or prevention of the advancement or progression of a cancer, reduction, amelioration, or prevention of the recurrence, development or onset of a cancer, and/or to improve or enhance the prophylactic or therapeutic effect of another therapy (e.g., a therapy other than the administration of a inhibitor, an antagonist, or any other therapeutic agent provided herein).
- another therapy e.g., a therapy other than the administration of a inhibitor, an antagonist, or any other therapeutic agent provided herein.
- a therapeutic agent refers to any agent that can be used in the treatment, amelioration, prevention, or management of a cancer and/or a symptom related thereto.
- a therapeutic agent refers to an inhibitor of CXCR4-GPCRx heteromer of the invention.
- a therapeutic agent can be an agent which is well known to be useful for, or has been or is currently being used for the treatment, amelioration, prevention, or management of a cancer and/or a symptom related thereto.
- intracellular Ca2+ assay refers to cell-based assay to measure the calcium flux associated with GPCR activation or inhibition.
- the method utilizes a calcium sensitive fluorescent dye that is taken up into the cytoplasm of most cells. The dye binds the calcium released from intracellular store and its fluorescence increases. The change in the fluorescence intensity is directly correlated to the amount of intracellular calcium that is released into cytoplasm in response to ligand activation of the receptor of interest.
- proximity-based assay refers to biophysical and biochemical techniques that are able to monitor proximity and/or binding of two protein molecules in vitro (in cell lysates) and in live cells, including bioluminescence resonance energy transfer (BRET), fluorescence resonance energy transfer (FRET), bimolecular fluorescence complementation (BiFC), Proximity ligation assay (PLA), cysteine crosslinking, and co-immunoprecipitation (Ferre et al., 2009; Gomes et al., 2016).
- BRET bioluminescence resonance energy transfer
- FRET fluorescence resonance energy transfer
- BiFC bimolecular fluorescence complementation
- PHA Proximity ligation assay
- cysteine crosslinking cysteine crosslinking
- co-immunoprecipitation Ferre et al., 2009; Gomes et al., 2016.
- the cell is a stem cell. In some embodiments, the cell is an immune cell. In some embodiments, the mobilizing a cell in a subject comprises blocking CXCR4. Tn some embodiments, the mobilizing a cell in a subject comprises blocking a beta-adrenergic receptor. In some embodiments, the mobilizing a cell in a subject comprises blocking a GPCR. In some embodiments, the mobilizing a cell in a subject comprises blocking CXCR4 and a beta-adrenergic receptor. In some embodiments, the mobilizing a cell in a subject comprises blocking CXCR4 and a GPCR. In some embodiments, the mobilizing a cell in a subject comprises blocking a CXCR4- GPCR heteromer.
- a cell in a subject comprising: blocking CXCR4 signaling and beta-adrenergic receptor signaling in the subject.
- methods of inducing cell mobilization in a subject comprising: blocking CXCR4 signaling and beta-adrenergic receptor signaling in the subject.
- the blocking beta-adrenergic receptor signaling is performed before the blocking CXCR4 signaling.
- the blocking beta-adrenergic receptor signaling is performed at a first specific time interval before the blocking CXCR4 signaling.
- the first specific time interval is between 5 minutes to 10 minutes, 10 minutes to 20 minutes, 20 minutes to 30 minutes, 30 minutes to 40 minutes, 40 minutes to 50 minutes, 50 minutes to 1 hour, 1 hour to 2 hours, 2 hours to 3 hours, 3 hours to 4 hours, 4 hours to 5 hours, 5 hours to 6 hours, 6 hours to 12 hours, 12 hours to 24 hours, 1 day to 2 days, 2 days to 3 days, 3 days to 4 days, 4 days to 5 days, 5 days to 6 days, 6 days to 7 days, 7 days to 8 days, 8 days to 9 days, 9 days to 10 days, 10 days to 11 days, 11 days to 12 days, 12 days to 13 days, 13 days to 14 days, or 14 days or more.
- the blocking beta-adrenergic receptor signaling continues after the blocking CXCR4 signaling is terminated. In some embodiments, the blocking beta-adrenergic receptor signaling continues for a second specific time interval after the blocking CXCR4 signaling is terminated.
- the second specific time interval is between 5 minutes to 10 minutes, 10 minutes to 20 minutes, 20 minutes to 30 minutes, 30 minutes to 40 minutes, 40 minutes to 50 minutes, 50 minutes to 1 hour, 1 hour to 2 hours, 2 hours to 3 hours, 3 hours to 4 hours, 4 hours to 5 hours, 5 hours to 6 hours, 6 hours to 12 hours, 12 hours to 24 hours, 1 day to 2 days, 2 days to 3 days, 3 days to 4 days, 4 days to 5 days, 5 days to 6 days, 6 days to 7 days, 7 days to 8 days, 8 days to 9 days, 9 days to 10 days, 10 days to 11 days, 11 days to 12 days, 12 days to 13 days, 13 days to 14 days, or 14 days or more.
- the blocking CXCR4 signaling comprises administering a CXCR4 inhibitor to the subject.
- a stem cell in a subject comprising: administering a beta-adrenergic receptor inhibitor and a CXCR4 inhibitor to the subject.
- methods of inducing stem cell mobilization in a subject comprising: administering a beta-adrenergic receptor inhibitor and a CXCR4 inhibitor to the subject.
- the administering the beta-adrenergic receptor inhibitor is performed before the administering the CXCR4 inhibitor.
- the administering the beta-adrenergic receptor inhibitor is performed at a first specific time interval before the administering the CXCR4 inhibitor.
- the administering the beta-adrenergic receptor inhibitor continues after the administering the CXCR4 inhibitor is terminated. In some embodiments, the administering the beta-adrenergic receptor inhibitor continues for a second specific time interval after the administering the CXCR4 inhibitor is terminated.
- the second specific time interval is between 5 minutes to 10 minutes, 10 minutes to 20 minutes, 20 minutes to 30 minutes, 30 minutes to 40 minutes, 40 minutes to 50 minutes, 50 minutes to 1 hour, 1 hour to 2 hours, 2 hours to 3 hours, 3 hours to 4 hours, 4 hours to 5 hours, 5 hours to 6 hours, 6 hours to 12 hours, 12 hours to 24 hours, 1 day to 2 days, 2 days to 3 days, 3 days to 4 days, 4 days to 5 days, 5 days to 6 days, 6 days to 7 days, 7 days to 8 days, 8 days to 9 days, 9 days to 10 days, 10 days to 11 days, 11 days to 12 days, 12 days to 13 days, 13 days to 14 days, or 14 days or more.
- the beta-adrenergic receptor inhibitor is an ADRB2 inhibitor.
- the beta-adrenergic receptor inhibitor is selected from the group consisting of alprenolol, atenolol, betaxolol, bupranolol, butoxamine, carazolol, carvedilol, CGP 12177, cicloprolol, ICT 118551, ICYP, labetalol, levobetaxolol, levobunolol, LK 204-545, metoprolol, nadolol, NIHP, NIP, propafenone, propranolol, sotalol, SR59230A, and timolol.
- the CXCR4 inhibitor is selected from the group consisting of ALX40- 4C, AMD070 (AMD11070, X4P-001), AMD3100 (plerixafor), AMD3465, ATI 2341, BKT140 (BL-8040; TF14016; 4F-Benzoyl-TN 14003), CTCE-9908, CX549 gratisD-[Lys3] GHRP-6, FC122, FC131, GMI-1359, GSK812397, GST-NT21MP, isothiourea- la, isothiourea- It (ITlt), KRH- 1636, KRH-3955, LY2510924, MSX-122, N-[l lC]Methyl-AMD3465, POL6326, SDF-1 1- 9[P2G] dimer, SDF1 P2G, T134, T140, T22, TC 14012, TG-0054 (Burixafor), USL31
- Burixafor is also referred to as GPC-100 or TG-0054.
- Plerixafor is also referred to as AMD3100 or Mozobil.
- the CXCR4 inhibitor is selected from the group consisting of AD-214, AMD070 (AMD11070, X4P-001), AMD3100 (plerixafor), BKT140 (BL- 8040; TF14016; 4F-Benzoyl-TN 14003), CTCE-9908, LY2510924, LY2624587, T140, TG-0054 (Burixafor), PF-06747143, POL6326, and ulocuplumab (MDX1338/BMS-936564).
- the method further comprises administering G-CSF to the subject.
- the administering the beta-adrenergic receptor inhibitor and the CXCR4 inhibitor to the subject is performed in the absence of G-CSF.
- methods of mobilizing a stem cell in a subject comprising: administering a CXCR4 inhibitor and G-CSF to the subject, in the absence of a beta-adrenergic receptor inhibitor.
- methods of inducing stem cell mobilization in a subject comprising: administering a CXCR4 inhibitor and G-CSF to the subject, in the absence of a beta-adrenergic receptor inhibitor.
- the administering the CXCR4 inhibitor to the subject comprises administering TG-0054 (burixafor) and propranolol. In embodiments, the administering the CXCR4 inhibitor to the subject comprises administering AMD3100 (plerixafor) and propranolol. In embodiments, the administering the CXCR4 inhibitor to the subject comprises administering ulocuplumab (MDX1338/BMS-936564) and propranolol.
- the enhanced amount of cell mobilization relative to the amount of cell mobilization induced by the CXCR4 inhibitor only is between 5% - 10% more, 10%-20% more, 20%-30% more, 30%-40% more, 40%-50% more, 50%-60% more, 60%-70% more, 70%-80% more, 80%-90% more, 90%-100% more, 100%-120% more, 120%-140% more, 140%-160% more, 160%-180% more, 180%-200% more, 200%-250% more, 250%-300% more, 300%-400% more, 400%-500% more, 500%-750% more, 750%-1000% more, or 1000% or more.
- the administering a combination of the CXCR4 inhibitor, the beta- adrenergic receptor inhibitor, and the G-CSF induces an enhanced amount of cell mobilization relative to the amount of cell mobilization induced by the CXCR4 inhibitor and the beta-adrenergic receptor inhibitor only.
- the administering a combination of the CXCR4 inhibitor, the beta-adrenergic receptor inhibitor, and the G-CSF mobilizes a cell by an amount enhanced relative to the amount of cell mobilization induced by the CXCR4 inhibitor and the beta-adrenergic receptor inhibitor only.
- the administering a combination of TG-0054 (burixafor) and the G-CSF induces an enhanced amount of cell mobilization relative to the amount of cell mobilization induced by AMD3100 (plerixafor) and the G-CSF.
- the administering a combination of the TG-0054 (burixafor) and the G-CSF mobilizes a cell by an amount enhanced relative to the amount of cell mobilization induced by the AMD3100 (plerixafor) and the G-CSF.
- the enhanced amount of cell mobilization relative to the amount of cell mobilization induced by the CXCR4 inhibitor only is between 1.1-fold to 1.2-fold
- the stem cell is selected from the group consisting of a hematopoietic stem cell, a hematopoietic progenitor cell, a mesenchymal stem cell, an endothelial progenitor cell, a neural stem cell, an epithelial stem cell, a skin stem cell, and a cancer stem cell.
- the stem cell is a hematopoietic stem cell or a hematopoietic progenitor cell.
- the hematopoietic stem cell or the hematopoietic progenitor cell is mobilized from bone marrow to peripheral blood.
- the mobilized hematopoietic stem cell or hematopoietic progenitor cell is collected for transplantation to a patient having cancer.
- the cancer is selected from the group consisting of lymphoma, leukemia, and myeloma.
- the cancer is non-Hodgkin lymphoma (NHL), acute myeloid leukemia (AML), acute lymphoblastic leukemia (ALL), or multiple myeloma (MM).
- the stem cell is a mesenchymal stem cell.
- the mesenchymal stem cell is mobilized from bone marrow to peripheral blood.
- the mesenchymal stem cell is mobilized for treatment of a condition selected from the group consisting of neurological disorder, cardiac ischemia, myocardial infarction, diabetes, tissue repair, bone and cartilage disease, autoimmune disease, graft versus host disease, Crohn's disease, multiple sclerosis, systemic lupus erythematosus, and systemic sclerosis.
- the stem cell is a cancer stem cell.
- the cancer stem cell is mobilized into blood.
- the cancer stem cell is mobilized for treatment of a cancer.
- the cell is an immune cell.
- the immune cell is a white blood cell.
- the white blood cell is a lymphocyte.
- the lymphocyte is selected from the group consisting of a T cell, a B cell, and a natural killer (NK) cell. In embodiments, the lymphocyte is a T cell. In embodiments, the lymphocyte is a natural killer (NK) cell.
- the white blood cell is a granulocyte. In embodiments, the granulocyte is selected from the group consisting of a neutrophile, an eosinophile, and a basophile. In embodiments, the granulocyte is a neutrophile. In embodiments, the white blood cell is a monocyte.
- the immune cell is mobilized from bone marrow to peripheral blood. In embodiments, the immune cell is mobilized from lymph node to peripheral blood.
- Enhancing mobilization of the stem and/or progenitor cells to peripheral blood is helpful in treatments to alleviate the effects of protocols that adversely affect the bone marrow, such as those that result in leukopenia, which are known side effects of chemotherapy and radiotherapy.
- the agents inhibiting the binding of SDF-1 to CXCR4 also enhance the success of bone marrow transplantation, enhance wound healing and bum treatment, and aid in restoration of damaged organ tissue. They also combat bacterial infections that are prevalent in leukemia. They are used to mobilize and harvest CD34+ cells via apheresis with and without combinations with other mobilizing factors. The harvested cells are used in treatments requiring stem cell transplantations.
- mobilizing a stem cell in a subject comprises blocking a CXCR4-GPCR heteromer.
- CXCR4-GPCR heteromers with distinct physiological and pharmacological properties have been reported, but their roles in stem cell mobilization or possibilities for developing stem cell mobilization therapeutics targeting CXCR4- GPCR heteromers have not been clearly understood or appreciated.
- GPCRs were believed to function as monomers that interact with hetero-trimeric G proteins upon ligand binding, and drugs were developed based on monomeric or homomeric GPCRs (Milligan 2008). Recently, this view changed drastically based on discoveries that GPCRs can form heteromers, and that heteromerization is obligatory for some GPCRs. GPCR heteromerization is known to alter GPCR maturation and cell surface delivery, ligand binding affinity, signaling intensity and pathways, as well as receptor desensitization and recycling (Terrillon and Bouvier 2004; Ferre et al., 2010; Rozenfeld and Devi 2010; Gomes et al., 2016; Farran 2017).
- Apheresis is a standard practice to obtain a larger number of immune cells as starting material for Adoptive Cell Therapy (ACT), which is a treatment based on transferring cells into a patient (1-3).
- ACT Adoptive Cell Therapy
- Apheresis may involve passing the blood of a patient through an apparatus that separates out one particular constituent and returns the remainder to the blood circulation of the patient. Apheresis is thus an extracorporeal therapy.
- different processes are employed in apheresis. If separation by density is required, centrifugation is the most common method. Other methods involve absorption onto beads coated with an absorbent material and filtration. The centrifugation method can be divided into two basic categories: continuous flow centrifugation (CFC) and intermittent flow centrifugation.
- CFC continuous flow centrifugation
- intermittent flow centrifugation intermittent flow centrifugation
- CFC historically required two venipunctures as the “continuous” means that the blood was collected, spun, and returned simultaneously. Newer systems can use a single venipuncture.
- the main advantage of CFC is the low extracorporeal volume (calculated by volume of the apheresis chamber, the donor’s hematocrit, and total blood volume of the donor) used in the procedure, which may be advantageuous in the elderly and for children. Intermittent flow centrifugation works in cycles, taking blood, spinning/ processing the blood, then giving back the unused parts to the donor in a bolus.
- the main advantage is a single venipuncture site. To stop the blood from coagulating, anticoagulant is automatically mixed with the blood as it is punped from the body into the apheresis machine.
- apheresis techniques may be used whenever the removed constituent is causing severe symptoms of disease in a patient. Generally, apheresis has to be performed fairly often and is an invasive procedure. It is therefore generally employed if other means to control a particular disease have failed, or if the symptoms are of such a nature that waiting for medication to become effective would cause suffering or risk of complications.
- Apheresis techniques include: (1) plasma exchange - removal of the liquid portion of blood to remove harmful substances, where the plasma is replaced with a replacement solution; (2) LDL apheresis - removal of low density lipoprotein in patients with familial hypercholesterolemia; (3) photopheresis - used to treat graft- versus-host disease, cutaneous T-cell lymphoma, and rejection in heart transplantation; (4) immunoadsorbtion with Staphylococcal protein A-agarose column - removal of allo- and autoantibodies (in autoimmune diseases, transplant rejection, hemophilia) by directing plasma through protein A-agarose columns (Protein A is a cell wall component produced by several strains of Staphylococcus aureus which binds to the Fc region of IgG); (5) leukocytapheresis - removal of malignant white blood cells in people with leukemia and very high white blood cell counts causing symptoms; (6) erythrocytapheresis -
- ACTs including CAR-T, CAR-NK, Tumor- Infiltrating Lymphocyte (TIL), and engineered T cell receptor (TCR)
- TIL Tumor- Infiltrating Lymphocyte
- TCR engineered T cell receptor
- Enhanced stem cell mobilization (SCM) or cell mobilization methods as disclosed herein can further augment or facilitate the conventional apheresis procedure.
- enhanced stem cell mobilization (SCM) or cell mobilization is particularly beneficial for the apheresis technique of leukapheresis.
- administering a CXCR4 antagonist to a subject further enhances apheresis by augmenting SCM or cell mobilization.
- administering a beta-adrenergic receptor antagonist in conjunction with a CXCR4 antagonist to a subject further enhances apheresis by augmenting SCM or cell mobilization, and/or replacing the G-CSF component of the treatment regime with a non-selective beta-blocker, such as propranolol.
- the augmentation of SCM in turn benefits HSCT (Hematopoietic Stem Cells Transplantation) or manufacturing of CAR-T cells for cancer immunotherapy.
- CXCR4 inhibitors such as plerixafor (Mozobil) which have been approved as stem cell mobilizers, are being used together with G-CSF as the standard of care to provide enriched hematopoietic stem cells and progenitor cells from healthy donors, marketed as the product “mobilized leukopaks.”
- enhancing apheresis in a subject comprising: blocking CXCR4 signaling and beta-adrenergic receptor signaling in the subject. Also disclosed herein are methods of enhancing apheresis by inducing cell mobilization in a subject, the method comprising: blocking CXCR4 signaling and beta-adrenergic receptor signaling in the subject. Further disclosed herein are methods of enhancing apheresis by mobilizing a cell in a subject, the method comprising: blocking CXCR4 signaling and beta-adrenergic receptor signaling in the subject. In embodiments, the blocking beta-adrenergic receptor signaling is performed before the blocking CXCR4 signaling.
- the blocking beta-adrenergic receptor signaling is performed at a first specific time interval before the blocking CXCR4 signaling.
- the first specific time interval is between 5 minutes to 10 minutes, 10 minutes to 20 minutes, 20 minutes to 30 minutes, 30 minutes to 40 minutes, 40 minutes to 50 minutes, 50 minutes to 1 hour, 1 hour to 2 hours, 2 hours to 3 hours, 3 hours to 4 hours, 4 hours to 5 hours, 5 hours to 6 hours, 6 hours to 12 hours, 12 hours to 24 hours, 1 day to 2 days, 2 days to 3 days, 3 days to 4 days, 4 days to 5 days, 5 days to 6 days, 6 days to 7 days, 7 days to 8 days, 8 days to 9 days, 9 days to 10 days, 10 days to 11 days, 11 days to 12 days, 12 days to 13 days, 13 days to 14 days, or 14 days or more.
- the blocking beta-adrenergic receptor signaling continues after the blocking CXCR4 signaling is terminated. In some embodiments, the blocking beta- adrenergic receptor signaling continues for a second specific time interval after the blocking CXCR4 signaling is terminated.
- the blocking CXCR4 signaling comprises administering a CXCR4 inhibitor to the subject.
- the second specific time interval is between 5 minutes to 10 minutes, 10 minutes to 20 minutes, 20 minutes to 30 minutes, 30 minutes to 40 minutes, 40 minutes to 50 minutes, 50 minutes to 1 hour, 1 hour to 2 hours, 2 hours to 3 hours, 3 hours to 4 hours, 4 hours to 5 hours, 5 hours to 6 hours, 6 hours to 12 hours, 12 hours to 24 hours, 1 day to 2 days, 2 days to 3 days, 3 days to 4 days, 4 days to 5 days, 5 days to 6 days, 6 days to 7 days, 7 days to 8 days, 8 days to 9 days, 9 days to 10 days, 10 days to 11 days, 11 days to 12 days, 12 days to 13 days, 13 days to 14 days, or 14 days or more.
- the beta-adrenergic receptor inhibitor is selected from the group consisting of propranolol, nadolol, and ICI 118551. In embodiments, the beta-adrenergic receptor inhibitor is propranolol.
- the CXCR4 inhibitor is selected from the group consisting of ALX40- 4C, AMD070 (AMD11070, X4P-001), AMD3100 (plerixafor), AMD3465, ATI 2341, BKT140 (BL-8040; TF14016; 4F-Benzoyl-TN 14003), CTCE-9908, CX549 gratisD-[Lys3] GHRP-6, FC122, FC131, GMI-1359, GSK812397, GST-NT21MP, isothiourea- la, isothiourea- It (ITlt), KRH- 1636, KRH-3955, LY2510924, MSX-122, N-[l lC]Methyl-AMD3465, POL6326, SDF-1 1- 9[P2G] dimer, SDF1 P2G, T134, T140, T22, TC 14012, TG-0054 (Burixafor), USL31
- the CXCR4 inhibitor is selected from the group consisting of AD-214, AMD070 (AMD11070, X4P-001), AMD3100 (plerixafor), BKT140 (BL-8040; TF14016; 4F-Benzoyl-TN14003), CTCE-9908, LY2510924, LY2624587, T140, TG-0054 (Burixafor), PF-06747143, POL6326, and ulocuplumab (MDX1338/BMS-936564).
- the CXCR4 inhibitor is TG-0054 (burixafor).
- the CXCR4 inhibitor is AMD3100 (plerixafor).
- the CXCR4 inhibitor is ulocuplumab (MDX1338/BMS-936564).
- the method further comprises administering G-CSF to the subject.
- the administering the beta-adrenergic receptor inhibitor and the CXCR4 inhibitor to the subject is performed in the absence of G-CSF.
- methods of enhancing apheresis in a subject comprising: administering a CXCR4 inhibitor and G-CSF to the subject, in the absence of a beta-adrenergic receptor inhibitor.
- methods of enhancing apheresis by inducing cell mobilization in a subject the method comprising: administering a CXCR4 inhibitor and G-CSF to the subject, in the absence of a beta-adrenergic receptor inhibitor.
- Also disclosed herein are methods of enhancing apheresis by mobilizing a cell in a subject comprising: administering a CXCR4 inhibitor and G-CSF to the subject, in the absence of a beta-adrenergic receptor inhibitor.
- the administering a combination of the CXCR4 inhibitor and the G-CSF induces an enhanced amount of apheresis relative to the amount of apheresis induced by the CXCR4 inhibitor only.
- the administering a combination of the CXCR4 inhibitor and the beta-adrenergic receptor inhibitor induces an enhanced amount of apheresis relative to the amount of apheresis induced by the CXCR4 inhibitor only.
- the enhanced amount of cell mobilization relative to the amount of cell mobilization induced by the CXCR4 inhibitor only is between 1.1-fold to 1.2-fold, 1.2-fold to 1.3-fold, 1.3 -fold to 1.4-fold, 1.4-fold to 1.5-fold, 1.5-fold to 1.6-fold, 1.6-fold to 1.7-fold, 1.7-fold to 1.8-fold, 1.8-fold to 1.9- fold, 1.9-fold to 2-fold, 2-fold to 2.5-fold, 2.5-fold to 3-fold, 3-fold to 4-fold, 4-fold to 5-fold, 5- fold to 10-fold, or 10-fold or more.
- an enhanced amount of cell mobilization or aphcrcsis is measured by a method selected from the group consisting of complete blood count (CBC) analysis, flow cytometry, and colony forming unit (CFU) assay.
- the enhanced amount of cell mobilization or apheresis is measured by flow cytometry.
- the flow cytometry is performed on (Lin-Scal+c-Kit+) LSK cells.
- the enhanced amount of cell mobilization or apheresis is measured by colony forming unit (CFU) assay.
- ADRB2 signaling in the cardiac myocyte is modulated by interactions with CXCR4 (LaRocca et al., 2010). Norepinephrine attenuates CXCR4 expression and the corresponding invasion of MDA-MB-231 breast cancer cells via ADRB2 (Wang et al., 2015a). ADRB2 is expressed in several cancers such as pancreatic, prostate (Braadland et al., 2014; Xu et al., 2017), renal and breast cancer (Choy et al., 2016).
- Radioligand Binding Assays (Bushlin et al., 2012; Pfeiffer et al., 2002); Cell Surface Biotinylation and Immunoblotting (He et al., 2011); immunostaing (Bushlin et al., 2012; Decaillot et al., 2008); immunoelectron microscopy (Fernandez-Duenas et al., 2015); [35S]GTP > S Binding assays (Bushlin et al., 2012); Calcuim imaging or assays using dyes such as Fura 2-acetomethoxy ester (Molecular Probes), Fluo-4 NW calcium dye (Thermo Fisher Scientific), or FLIPR5 dye (Molecular Devices); cAMP assays using radioimmunoassay
- protein-protein interaction inhibitor refers to any molecules that can interfere with protein-protein interactions.
- Protein-protein interaction unlike enzyme-substrate interaction involving well-defined binding pockets, is a transient interaction or association between proteins over relatively large areas and is often driven by electrostatic interactions, hydrophobic interactions, hydrogen bonds, and/or Van der Waals forces.
- PPI inhibitors may include, but not limited to, membrane-permeable peptides or lipid fused to a peptide sequence that disrupts the GPCR heteromeric interface, for example, transmembrane helix, intracellular loop, or C-terminal tail of GPCRx.
- the PPI inhibitor of the CXCR4-GPCRx heteromer may be a membrane-permeable peptide or cell-penetrating peptide (CPP) conjugated with peptide that targets the CXCR4-GPCRx heteromeric interface(s), or may be a cellpenetrating lipidated peptide targeting the CXCR4-GPCRx heteromeric interface(s).
- CPP cell-penetrating peptide
- CXCR4-GPCRx heteromers To identify novel CXCR4-GPCRx heteromers, recombinant adenoviruses encoding 143 GPCRs fused with N-terminal fragments of yellow fluorescent protein Venus (VN) and 147 GPCRs fused with C-terminal fragment of Venus (VC) were made as described in Song et al. (Song et al., 2014; SNU patent; Song, thesis). CXCR4-GPCR heteromers were identified using bimolecular fluorescence complementation (BiFC) assay (FIG. 1), in which two complementary VN and VC fragments of Venus reconstitute a fluorescent signal only when both fragments are close enough through interaction between two different proteins to which they are fused (Hu et al., 2002).
- BiFC bimolecular fluorescence complementation
- the preclinical study evaluated the ability of the non- selective beta adrenergic receptor blocker propranolol to improve GPCIOO-induced stem cell mobilization following a seven-day treatment in a mouse model. These effects were further assessed by the addition of G-CSF to GPC100, as well as in comparison with the current standard of care treatments for stem cell mobilization such as G-CSF alone or in combination with AMD3100.
- Propranolol (MedChem Express, Princeton, NJ) was intraperitoneally (IP) administered at 20 mg/kg for seven days once in a day.
- Recombinant murine G-CSF (Peprotech, Cranbury, NJ) was administered subcutaneously (SC) two times a day for five days at 0.1 mg/kg/dose.
- AMD3100 (MedChem Express, Princeton, NJ) was administered subcutaneously once on day 7 at 5 mg/kg.
- GPC100 was administered intravenously (IV) once on day 7 at 30 mg/kg.
- GPC100 was acquired by GPCR Therapeutics from TaiGen Biotechnology, Taiwan. All compounds were reconstituted in PBS. Vehicle controls received PBS intravenously, intraperitoneally or subcutaneously depending on the drug combination used in the study.
- mice Male, 6-9 weeks old were purchased from Jackson Laboratory and maintained on a 12-h light/dark cycle with free access to food and water. All mice were housed at the laboratory animal facility that had been accredited by A AALAC (Association for Assessment and Accreditation of Laboratory Animal Care International) and the IACUC (Institutional Animal Care and Use Committee) of Crown Bioscience (San Diego, CA) or Explora Biolabs (San Carlos, CA).
- AALAC Association for Assessment and Accreditation of Laboratory Animal Care International
- IACUC Instituteional Animal Care and Use Committee
- Crown Bioscience San Diego, CA
- Explora Biolabs San Carlos, CA
- mice were administered a single dose of GPC100 (30 mg/kg, IV) or vehicle (IV) and blood was collected one hour later.
- Another group of C57/BL6 mice received a single dose of GPC100 (30 mg/kg, IV) and blood was collected at 30 min, 1 hour and 2 hours post- injection.
- the time point for sample collection post-GPCIOO was established at 2 hours based on the maximum WBC mobilization (FIG. IB). All subsequent studies were performed in C57/BL6 female mice as this mouse strain is more critically evaluated in stem cell mobilization studies.
- mice received vehicle (IP) or propranolol (20 mg/kg, IP) for seven days.
- IP vehicle
- GPC100 (30 mg/kg, IV) was co-administered (Table 3).
- mice were treated with propranolol or vehicle for seven days; GPC100 or vehicle was co-adminstered on day 7 to determine the effects of propranolol alone, GPC100 alone or their combination on total blood cell count in peripheral blood (Table 3).
- mice were administered G-CSF (0.1 mg/kg, SC, BID) for five days (day 2 to day 6) with or without propranolol.
- GPC100 (30 mg/kg, IV) was co-administered with propranolol or alone on day 7 (Table 5).
- mice treated with vehicle showed mean WBC count of 3.4 +/- 1.8 x 10 3 cells/uL and lymphocyte count of 2.6 +/- 1.2 x 10 3 cells/uL of peripheral blood. Vehicle treated mice were included in all studies as a control despite not presented in data graphs.
- GPC100 (30 mg/kg) resulted in the rapid increase of circulating WBCs in C57/BL6 and Balb/c mice, which is reflective of stem cell mobilization (FIG. 1A).
- GPC-100 (30 mg/kg) was administered intravenously in naive C57/B16 mice, and peripheral blood was collected at time points 0.5-, 1- and 2-hours post-injection in different groups. Time dependent increase in WBC count was observed and a 2-hour post-injection sample collection was selected for subsequent studies (FIG. IB).
- T lymphocytes are critical in the manufacturing process of CAR-T cells.
- Some CAR-T products that are being clinically investigated or are commercially available rely on autologous patient-derived T cells. T cells from patients might be insufficient in number or affected by several lines of pretreatment and/or actual disease related treatment (for example, progressive AML) (Fesnak et al Transfus Med Rev 2016). This suggests that lymphocyte mobilization is significant both for allogenic hematopoietic stem cell transplant to reduce GVHD risk, as well as for strategies designed to mobilize both effector and regulatory lymphocyte populations for adoptive cellular therapies.
- the phenotypic profile of immune cells including the lymphocytes that are mobilized by propranolol and GPC100 combination treatments is being further investigated.
- the results from the study disclosed herein will provide more information on the type of lymphocyte subsets that can be harvested by GPC100 and propranolol combination treatment and their importance in therapeutic development.
- the subjects of the study were C57/BL6 Female mice. Peripheral blood was collected 2 hours after vehicle or GPC 100, and 1 hour after AMD3100 by terminal cardiac puncture. Complete blood count was determined by hematology analyzer.
- mice treated with GPC100 and/or propranolol no change in the number of platelets, RBCs or hemoglobin levels was observed compared to those treated with the standard of care treatment or vehicle.
- hematopoietic stem cells are devoid of lineage markers (Lin-) and express Seal and cKit markers (LSK cell profile). CXCR4 is also expressed on hematopoietic stem cells. Data are shown for LSK Cells (FIG. 14) and for Lin-CXCR4+ cells (FIG. 15).
- the combined blockade of the two signaling pathways is investigated for its ability to drive CXCR4 and beta-adrenergic receptors.
- the CXCR4 blockade will be determined by administration of both B urixafor and Plerixafor.
- the effects of a combination of propranolol + Plerixafor AND propranolol + G-CSF + Plerixafor will also be studied.
- GPC-100 & G-CSF resulted in a higher number of mobilized circulating WBCs and progenitor cells as compared to AMD3100 & G-CSF.
- the triple combination resulted in highest number of mobilized WBCs and progenitor cells.
- G-CSF was administered two times daily for five days at 0.1 mg/kg, SC; twelve-hours after the last injection of G-CSF, GPC100 was administered alone at 30 mg/kg, IV. Samples were collected 2 hours after GPC100 administration (Table 9).
- Propranolol was administered once daily for 7 days; G-CSF was administered twice daily for five days starting on the second day; twelve hours after the last injection of G-CSF, GPC100 was co-administered with propranolol; samples were collected 2 hours after GPC100 administration (Table 10).
- CXCR4 antagonists like Plerixafor (AMD3100) and Burixafor (GPC100) arc clinically approved in the U.S and Europe for use in combination with G- CSF for hematopoietic stem cell mobilization and subsequent autologous stem cell transplant in Non-Hodgkin’s Lymphoma and multiple myeloma patients.
- G-CSF regimen involves repeated multi-day injections and is associated with adverse side effects like severe bone pain. Poor mobilization has also been reported in up to 40% patients. Therefore, an alternate approach to improve hematopoietic stem cell mobilization by CXCR4 antagonists is needed.
- mice were selected over Balb/c for future studies as HSC mobilization has been critically evaluated in this mouse strain (Broxmeyer et al 2005).
- GPC-100 (30 mg/kg, TV) alone induces time-dependent WBC Mobilization (FIG. 23).
- a future study will employ sample collection at 2 hours post-GPC administration. The planned time-course study will be as follows: 0.5, 1, 2, 3, 4 hours post-GPCIOO administration. Dose response with IV GPC100 administration will be performed (doses TBD).
- G-CSF + AMD3100 [00187] A study was performed to study compare with G-CSF + AMD3100 (Table 14). Propranolol (20 mg/kg IP) was administered once daily for 7 days. On day 7, GPC 100 (30 mg/kg IV) was co-administered with propranolol. Peripheral blood was collected 2 hours post-injection by cardiac puncture. This outcome was compared with the current standard of care for mobilization i.e., the combination treatment with G-CSF and AMD3100 (Plerixafor). G-CSF (0.1 mg/kg SC) was administered for 5 days two times a day, followed by a single injection of AMD3100 (5 mg/kg SC) on day 6 after 12 hours. Peripheral blood was collected 1-hour post- AMD3100 based on the literature reports (Hoggatt et al 2018).
- Propranolol was observed to enhance GPCIOO-induced mobilization (FIGs. 27A-C). This effect was comparable with the standard of care (G-CSF + AMD3100/Plerixafor). The Propranolol + GPC100 combination was observed to mobilize more lymphocytes. It was also observed that SOC mobilized more neutrophils (G-CSF driven).
- FIG. 29A-B For LSK flow, propranolol + GPC100 combination was comparable with SOC. Future studies will repeat this experiment with more blood volume and added G-CSF.
- a Colony Forming Unit Assay was performed (FIG. 33 and FIG. 34).
- the CFU assay is based on the ability of hematopoietic progenitors to proliferate and differentiate into colonies in a semi-solid media in response to cytokine stimulation.
- Number and types of colonies counted in a CFU assay provide information about the frequency and types of progenitor cells present in the original cell population and their ability to proliferate and differentiate.
- the triple combination mobilized the highest number of progenitor cells (FIG. 35, FIGs. 36A-36B and FIG. 37). Furthermore, the triple combination was associated with the maximum increase in circulating WBCs as well as progenitor cells compared to other drug groups (FIGs. 38A-38B).
- GPC100 + G-CSF mobilized more WBCs and progenitors compared to AMD3100 + G-CSF. No difference was observed between vehicle group vs. GPC100 +/- propranolol.
- the CFU assay was only designed for myeloid progenitors, and not lymphoid (FIGs. 39A-39B).
- G-CSF was observed to mobilize myeloid progenitors and the assay was observed to be dependent on G-CSF.
- FIGs. 40A-40B Data regarding the effect of propranolol on GPCIOO-induced mobilization from 3 studies (studies 1, 3, 4) are shown in FIGs. 40A-40B. It was observed that Propranolol enhanced GPC100 induced mobilization in 3 studies.
- GPC 100, AMD3100 or G-CSF induced WBC mobilization was studied (FIGs. 42A-42C). Maximum mobilization was observed with G-CSF, while GPC100 mobilized more lymphocytes than AMD3100 or G-CSF. Furthermore, GPC 100 mobilized more WBCs than AMD3100 and G-CSF mobilized more neutrophils than GPC 100 or AMD3100.
- FIGs. 46A-C A comparison study between GPC100 and AMD3100 was performed (FIGs. 46A-C). This was the first study to show the effect of propranolol and triple combination with AMD3100. Propranolol was observed to slightly increase AMD3100-induced mobilization of lymphocytes.
- FIGs. 49 A- B Data from 4 studies in which standard of care group was added are shown in FIGs. 49 A- B. It was observed that the standard of care regimen mobilized more WBCs compared to the propranolol and GPC100 combination. However, there was no difference in lymphocyte mobilization. The standard of care group also showed high variability, which reflects the mobilization patient response in the clinic.
- FIGs. 50A-B Data from 3 studies in which G-CSF combination group was added are shown in FIGs. 50A-B . It was observed that addition of propranolol to G-CSF and GPC 100 combination mobilized significantly more WBC and lymphocytes compared to the standard of care. When combined with G-CSF, GPC 100 was observed to mobilize significantly more WBCs, compared to AMD3100. However, with addition of propranolol there was significantly more mobilization of lymphocytes.
- CXCR4 antagonists like Plerixafor (AMD3100) and Burixafor (GPC 100) are clinically approved in the U.S and Europe for use in combination with G-CSF for hematopoietic stem cell mobilization and subsequent autologous stem cell transplant in Non-Hodgkin’s Lymphoma and multiple myeloma patients.
- G-CSF regimen involves repeated multi-day injections and is associated with adverse side effects like severe bone pain. Poor mobilization has also been reported in up to 40% patients.
- Lymphocyte Mobilization High T-cell content was associated with rapid hematopoietic reconstitution, decreased relapse, increased discasc-frcc survival in patients receiving peripheral blood stem cell transplants compared to those receiving bone marrow transplants highlighting the importance of lymphocyte mobilization (Stem Cell Trialists' Collaborative Group J Clin One 2005).
- a study in non-human primates showed that single injection of the CXCR4 antagonist AMD3100 resulted in enhanced lymphocyte count in peripheral blood that included effector T cells, as well as Treg and Tern, which are associated with GVHD-protective properties (Kean et al Blood 2014).
- allogeneic stem cell grafts harvested in healthy donors following a single dose of AMD3100 contained higher numbers of both effector and regulatory T-cells as compared to grafts harvested following G-CSF. (Greef et al Blood 2014). This is significant both for allo-HSCT as well as for strategies designed to mobilize both effector and regulatory lymphocyte populations for adoptive cellular therapies.
- Previous studies have documented CXCL12/CXCR4-mediated lymphocyte homing in the bone marrow, lymph nodes, high endothelial venules, small blood vessels, thymus, and gastrointestinal tract (Bunting et al Immunol Cell Biol 2011).
- Efficient leukapheresis providing a sufficient amount of T lymphocytes is a critical step in the manufacturing process of CAR-T cells.
- Some CAR-T cell products under current investigation are based on allogeneic T cells from healthy donors, while some CAR-T products that are clinically investigated or are commercially available rely on autologous patient derived T cells.
- T cells from patients might be decreased in number or hampered by several lines of pretreatment and actual disease related treatment (for example, progressive AML) (Fesnak et al Transfus Med Rev 2016).
- FIGs. 51A-B Combined data from all 6 studies are shown in FIGs. 51A-B. 7-day propranolol treatment prior to GPC100 was observed to result in significantly enhanced WBC and lymphocyte cell counts in peripheral blood compared to GPC100 alone.
- GPC 100, AMD3100 or G-CSF induced WBC mobilization was studied (FIGs. 55A-C). Maximum mobilization was observed with G-CSF.
- GPC 100 mobilized more lymphocytes than AMD3100 or G-CSF, while GPC100 mobilized more WBCs than AMD3100, and G-CSF mobilized more neutrophils than GPC100 or AMD3100.
- GPC 100 In vitro activity of GPC 100 was investigated in cell-based assays (FIGs. 59A-59B). In the FRET ligand binding assay in HEK cells, GPC 100 more potently inhibited binding of CXCL12 to CXCR4 than AMD3100 with a ⁇ 30-fold better binding affinity (Ki of 1.6 vs 40 nM, respectively). Potent inhibition of CXCR4 was recapitulated in cell migration assays using a multiple myeloma cell line MMES, where GPC 100 inhibited CXCL12-mediated migration with IC50 of 30 nM compared to the AMD3100 IC50 of 80 nM.
- BBs like Pro can shift bone marrow-derived cells to differentiate away from a myeloid bias to a phenotype consistent with CD34+ stem cells and genes associated with stem cells (Knight et al., Blood Adv 2020).
- MM Multiple myeloma
- ASCT Autologous Stem Cell Transplant
- HSC hematopoietic stem cells
- BM bone marrow
- PB peripheral blood
- HSCs are phenotypically characterized by the expression of CD34.
- a minimum of around 2 x 10 6 CD34 + cells/kg are used for HSC harvest, whereas the prefered numbers for improved engraftment and survival is >5-6 x 10 6 CD34 + cells/kg (Toor et al., 2004; Tricot et al., 1995).
- G-CSF Granulocyte-colony stimulating factor
- CXCR4 is a member of the chemokine G protein-coupled receptor (GPCR) family and is expressed on HSCs (Wu et al., 2010; Mezzapelle et al., 2022; Guo et al., 2016).
- CXCR4 signaling mediated by its natural ligand CXCL12, plays a role in cellular chemotaxis, as well as retention and survival of HSCs in BM (Guo et al., 2016).
- GPC-100 also known as Burixafor or TG-0054, is a novel small molecule antagonist of CXCR4 with a high binding affinity for CXCR4.
- GPC-100 in combination with G-CSF, has been tested clinically in MM patients as an HSC mobilizer (NCT02104427) (Schuster, 2021), and was shown to elicit a increase in HSCs with >5.0 x 10 6 CD34 + cells/kg in 1-2 leukapheresis sessions (Setia et al., 2015). This result was comparable with the historical results from G-CSF plus AMD3100 treatment.
- the MM microenvironment is known to cause dysregulation of HSC function leading to changes in gene expression and altered hematopoietic differentiation (Bruns et al., 2012; Knight et al., 2020).
- a Phase II biomarker-driven randomized study showed that in MM patients, the FDA-approved non-selective beta blocker propranolol shifted cell differentiation away from the myeloid-lineage bias to an upregulation of CD34 + cells and enhanced engraftment (Knight et al., 2020).
- CFU Colony Forming Unit
- GPC- 100 and propranolol were compared with G-CSF alone for WBC mobilization.
- G-CSF was administered for 5 days, two times daily.
- a triple combination with G-CSF, GPC-100 and propranolol was investigated in comparison with G-CSF plus AMD3100 for WBC and stem cell mobilization in a phenotypic analysis and colony forming unit assay.
- blood was collected 2 hours after GPC-100, 1 hour after AMD3100 and 12 hours after G-CSF.
- CFU assay was conducted to measure the mobilized HSPCs based on their ability to form CFU-GM and BFU-E colonies.
- the triple combination produced a 47 -fold increase in CFUs over vehicle control compared to a 35-fold and 27-fold increase over vehicle from G-CSF plus GPC-100 and G-CSF plus AMD3100 treatments, respectively (FIG. 67A-67D).
- GPC-100 is a potent hematopoietic mobilizer, and its mobilizing effect is enhanced by propranolol.
- the studies also also show that GPC-100-induced increase in the mobilization by G-CSF is superior to the combination of G-CSF and AMD3100. Addition of propranolol to G-CSF and GPC-100 mobilized significantly more hematopoietic stem cells capable of differentiating into multipotent progenitors.
- a method of mobilizing a cell in a subject comprising: blocking CXCR4 signaling and beta-adrenergic receptor signaling in the subject.
- Tn an embodiment, disclosed herein is a method of inducing cell mobilization in a subject, the method comprising: blocking CXCR4 signaling and beta-adrenergic receptor signaling in the subject.
- a method of enhancing apheresis by inducing cell mobilization in a subject comprising: blocking CXCR4 signaling and beta-adrenergic receptor signaling in the subject.
- a method of enhancing apheresis by mobilizing a cell in a subject comprising: blocking CXCR4 signaling and beta-adrenergic receptor signaling in the subject.
- the blocking beta-adrenergic receptor signaling is performed before the blocking CXCR4 signaling.
- the blocking beta-adrenergic receptor signaling continues after the blocking CXCR4 signaling is terminated.
- the blocking CXCR4 signaling comprises administering a CXCR4 inhibitor to the subject.
- the blocking beta-adrenergic receptor signaling comprises administering a beta-adrenergic receptor inhibitor to the subject.
- the cell is a stem cell.
- the cell is a stem cell.
- a method of mobilizing a stem cell in a subject comprising: administering a beta-adrenergic receptor inhibitor and a CXCR4 inhibitor to the subject.
- a method of inducing stem cell mobilization in a subject comprising: administering a beta-adrenergic receptor inhibitor and a CXCR4 inhibitor to the subject.
- Tn an embodiment, disclosed herein is a method of enhancing apheresis in a subject, the method comprising: administering a beta-adrenergic receptor inhibitor and a CXCR4 inhibitor to the subject.
- a method of enhancing apheresis by inducing cell mobilization in a subject comprising: administering a beta-adrenergic receptor inhibitor and a CXCR4 inhibitor to the subject.
- a method of enhancing apheresis by mobilizing a cell in a subject comprising: administering a beta-adrenergic receptor inhibitor and a CXCR4 inhibitor to the subject.
- the administering the beta-adrenergic receptor inhibitor is performed before the administering the CXCR4 inhibitor.
- the administering the beta-adrenergic receptor inhibitor continues after the administering the CXCR4 inhibitor is terminated.
- the method further comprises administering G-CSF to the subject.
- a method of mobilizing a stem cell in a subject comprising: administering a CXCR4 inhibitor and G-CSF to the subject, in the absence of a beta-adrenergic receptor inhibitor.
- the beta-adrenergic receptor inhibitor is selected from the group consisting of propranolol, nadolol, and ICI 118551.
- the CXCR4 inhibitor is AMD3100 (plerixafor).
- the administering the CXCR4 inhibitor to the subject comprises administering TG-0054 (burixafor) and propranolol.
- the administering the CXCR4 inhibitor to the subject comprises administering AMD3100 (plerixafor) and propranolol.
- the administering a combination of the CXCR4 inhibitor and the G- CSF induces an enhanced amount of apheresis relative to the amount of apheresis induced by the CXCR4 inhibitor only.
- the administering a combination of the CXCR4 inhibitor and the beta- adrenergic receptor inhibitor induces an enhanced amount of cell mobilization relative to the amount of cell mobilization induced by the CXCR4 inhibitor only.
- the administering a combination of the CXCR4 inhibitor and the beta- adrenergic receptor inhibitor mobilizes a cell by an amount enhanced relative to the amount of cell mobilization induced by the CXCR4 inhibitor only.
- the administering a combination of the CXCR4 inhibitor and the beta- adrenergic receptor inhibitor induces an enhanced amount of apheresis relative to the amount of apheresis induced by the CXCR4 inhibitor only.
- the administering a combination of the CXCR4 inhibitor and the beta- adrenergic receptor inhibitor, and the G-CSF induces an enhanced amount of apheresis relative to the amount of apheresis induced by the CXCR4 inhibitor and the beta-adrenergic receptor inhibitor only.
- the administering a combination of TG-0054 (burixafor) and the G- CSF induces an enhanced amount of cell mobilization relative to the amount of cell mobilization induced by AMD3100 (plerixafor) and the G-CSF.
- the administering a combination of the TG-0054 (burixafor) and the G-CSF mobilizes a cell by an amount enhanced relative to the amount of cell mobilization induced by the AMD3100 (plerixafor) and the G-CSF.
- the administering a combination of the TG-0054 (burixafor) and the G-CSF induces an enhanced amount of apheresis relative to the amount of apheresis induced by the AMD3100 (plerixafor) and the G-CSF.
- an enhanced amount of cell mobilization or apheresis is measured by a method selected from the group consisting of complete blood count (CBC) analysis, flow cytometry, and colony forming unit (CFU) assay.
- CBC complete blood count
- CFU colony forming unit
- the enhanced amount of cell mobilization or apheresis is measured by flow cytometry.
- the flow cytometry is performed on (Lin-Scal+c-Kit+) LSK cells.
- the enhanced amount of cell mobilization or apheresis is measured by colony forming unit (CFU) assay.
- CFU colony forming unit
- the subject has a CXCR4 protomer in the cell.
- the subject has an ADRB2 protomer in the cell.
- the subject has a CXCR4 protomer and an ADRB2 protomer in the cell.
- the subject has a CXCR4-ADRB2 heteromer in the cell.
- the CXCR4-ADRB2 heteromer has an enhanced amount of downstream calcium mobilization relative to downstream calcium mobilization from a CXCR4 protomer or ADRB2 protomer; and ii) the administered combination of inhibitors suppresses the enhanced downstream calcium mobilization from said CXCR4-ADRB2 heteromer in the stem cell.
- the cell is a stem cell.
- the hematopoietic stem cell or the hematopoietic progenitor cell is mobilized from bone marrow to peripheral blood.
- the cancer is selected from the group consisting of lymphoma, leukemia, and myeloma.
- the cancer is non-Hodgkin lymphoma (NHL), acute myeloid leukemia (AML), acute lymphoblastic leukemia (ALL), or multiple myeloma (MM).
- NHL non-Hodgkin lymphoma
- AML acute myeloid leukemia
- ALL acute lymphoblastic leukemia
- MM multiple myeloma
- the stem cell is a mesenchymal stem cell.
- the mesenchymal stem cell is mobilized from bone marrow to peripheral blood.
- the mesenchymal stem cell is mobilized for treatment of a condition selected from the group consisting of neurological disorder, cardiac ischemia, myocardial infarction, diabetes, tissue repair, bone and cartilage disease, autoimmune disease, graft versus host disease, Crohn's disease, multiple sclerosis, systemic lupus erythematosus, and systemic sclerosis.
- a condition selected from the group consisting of neurological disorder, cardiac ischemia, myocardial infarction, diabetes, tissue repair, bone and cartilage disease, autoimmune disease, graft versus host disease, Crohn's disease, multiple sclerosis, systemic lupus erythematosus, and systemic sclerosis.
- the stem cell is a cancer stem cell.
- the cancer stem cell is mobilized into blood.
- the cancer stem cell is mobilized for treatment of a cancer.
- the cell is an immune cell.
- the immune cell is a white blood cell.
- the white blood cell is a lymphocyte.
- the lymphocyte is selected from the group consisting of a T cell, a B cell, and a natural killer (NK) cell.
- the lymphocyte is a T cell.
- the lymphocyte is a natural killer (NK) cell.
- the granulocyte is selected from the group consisting of a neutrophile, an eosinophile, and a basophile. [00329] Tn an embodiment, the granulocyte is a neutrophile.
- the white blood cell is a monocyte.
- the immune cell is mobilized from bone marrow to peripheral blood.
- the immune cell is mobilized from lymph node to peripheral blood.
- the mobilized immune cell is used for adoptive cell therapy (ACT).
- ACT adoptive cell therapy
- the adoptive cell therapy is chimeric antigen receptor (CAR) T cell therapy.
- the adoptive cell therapy is netural killer (NK) cell therapy.
- the adoptive cell therapy is tumor-infiltrating lymphocyte (TIL) therapy.
- TIL tumor-infiltrating lymphocyte
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- General Health & Medical Sciences (AREA)
- Medicinal Chemistry (AREA)
- Veterinary Medicine (AREA)
- Public Health (AREA)
- Animal Behavior & Ethology (AREA)
- Pharmacology & Pharmacy (AREA)
- Epidemiology (AREA)
- Immunology (AREA)
- Organic Chemistry (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Engineering & Computer Science (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- General Chemical & Material Sciences (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Zoology (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Gastroenterology & Hepatology (AREA)
- Microbiology (AREA)
- Mycology (AREA)
- Biochemistry (AREA)
- Biophysics (AREA)
- Genetics & Genomics (AREA)
- Molecular Biology (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
- Pharmaceuticals Containing Other Organic And Inorganic Compounds (AREA)
- Medicines Containing Material From Animals Or Micro-Organisms (AREA)
- Acyclic And Carbocyclic Compounds In Medicinal Compositions (AREA)
Abstract
Description
















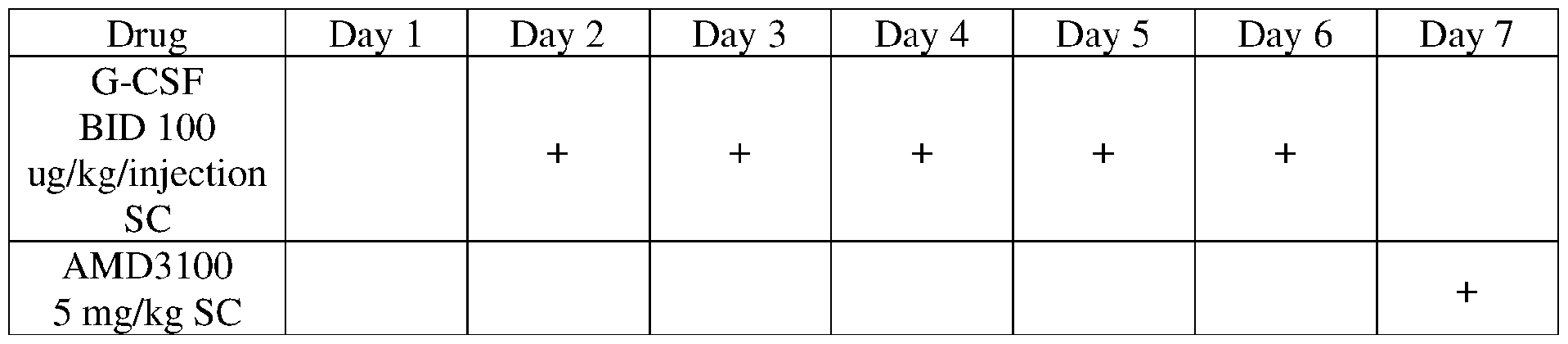

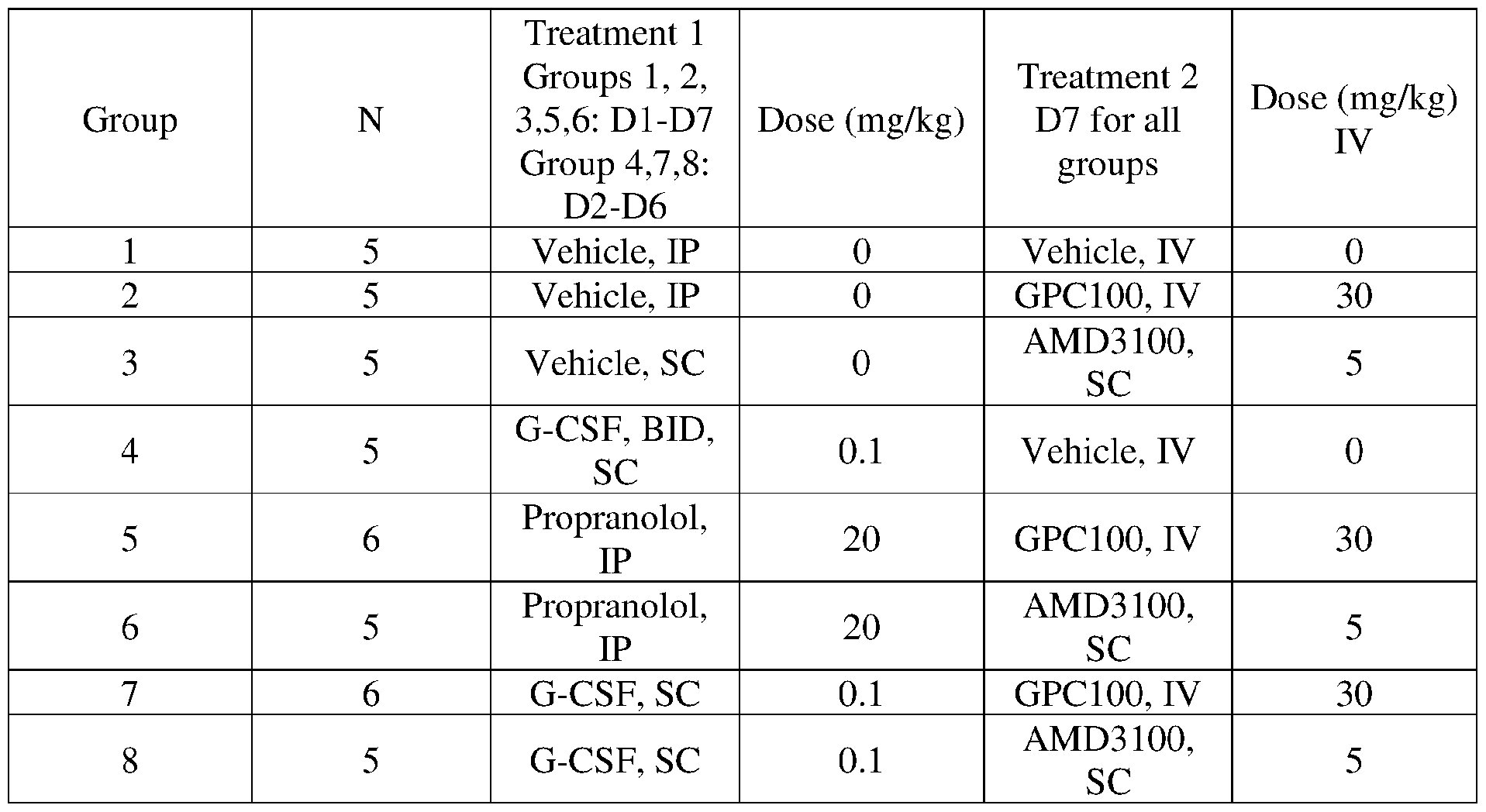






Claims
Priority Applications (7)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| AU2023285050A AU2023285050A1 (en) | 2022-06-10 | 2023-06-09 | Gpcr inhibitors and uses thereof |
| KR1020257001078A KR20250023521A (en) | 2022-06-10 | 2023-06-09 | GPCR inhibitors and uses thereof |
| EP23820497.8A EP4536239A4 (en) | 2022-06-10 | 2023-06-09 | GPCR inhibitors and their uses |
| US18/873,710 US20250360149A1 (en) | 2022-06-10 | 2023-06-09 | Gpcr inhibitors and uses thereof |
| CN202380053854.3A CN119562815A (en) | 2022-06-10 | 2023-06-09 | GPCR inhibitors and their uses |
| JP2024572376A JP2025519561A (en) | 2022-06-10 | 2023-06-09 | GPCR inhibitors and uses thereof |
| CA3258771A CA3258771A1 (en) | 2022-06-10 | 2023-06-09 | Gpcr inhibitors and uses thereof |
Applications Claiming Priority (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US202263351101P | 2022-06-10 | 2022-06-10 | |
| US63/351,101 | 2022-06-10 | ||
| US202263369738P | 2022-07-28 | 2022-07-28 | |
| US63/369,738 | 2022-07-28 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2023239937A1 true WO2023239937A1 (en) | 2023-12-14 |
Family
ID=89118957
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2023/024983 Ceased WO2023239937A1 (en) | 2022-06-10 | 2023-06-09 | Gpcr inhibitors and uses thereof |
Country Status (8)
| Country | Link |
|---|---|
| US (1) | US20250360149A1 (en) |
| EP (1) | EP4536239A4 (en) |
| JP (1) | JP2025519561A (en) |
| KR (1) | KR20250023521A (en) |
| CN (1) | CN119562815A (en) |
| AU (1) | AU2023285050A1 (en) |
| CA (1) | CA3258771A1 (en) |
| WO (1) | WO2023239937A1 (en) |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2025231332A1 (en) * | 2024-05-02 | 2025-11-06 | Dana-Farber Cancer Institute, Inc. | Methods of modulating erythropoiesis using beta-2 adrenergic receptor antagonists |
| WO2026020039A1 (en) * | 2024-07-18 | 2026-01-22 | Gpcr Therapeutics, Inc. | Cxcr4 inhibitors and/or beta adrenergic receptor inhibitors for mobilization of lymphocytes andimmune cells |
Citations (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20070190023A1 (en) * | 2006-01-25 | 2007-08-16 | Michela Battista | Methods and compositions for modulating the mobilization of stem cells |
| US20170355959A1 (en) * | 2014-12-19 | 2017-12-14 | Imperial Innovations Limited | Methods for mobilising populations of stem cells |
| US20210268069A1 (en) * | 2017-12-19 | 2021-09-02 | Gpcr Therapeutics, Inc. | Gpcr heteromer inhibitors and uses thereof |
| WO2021217143A1 (en) * | 2020-04-24 | 2021-10-28 | Emory University | Aminopiperidine amides, derivatives, compositions, and uses related to cxcr4 modulation |
| WO2022064075A1 (en) * | 2020-09-28 | 2022-03-31 | Ermium Therapeutics | Cyclic isothiourea derivatives as cxcr4 modulators |
Family Cites Families (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN111712262A (en) * | 2017-12-06 | 2020-09-25 | 美真达治疗公司 | Dosing regimen for mobilization of hematopoietic stem and progenitor cells |
| BR112021022887A2 (en) * | 2019-05-17 | 2022-01-18 | Gpcr Therapeutics Inc | Gpcr heteromer inhibitors and uses thereof |
-
2023
- 2023-06-09 CA CA3258771A patent/CA3258771A1/en active Pending
- 2023-06-09 KR KR1020257001078A patent/KR20250023521A/en active Pending
- 2023-06-09 CN CN202380053854.3A patent/CN119562815A/en active Pending
- 2023-06-09 WO PCT/US2023/024983 patent/WO2023239937A1/en not_active Ceased
- 2023-06-09 US US18/873,710 patent/US20250360149A1/en active Pending
- 2023-06-09 AU AU2023285050A patent/AU2023285050A1/en active Pending
- 2023-06-09 EP EP23820497.8A patent/EP4536239A4/en active Pending
- 2023-06-09 JP JP2024572376A patent/JP2025519561A/en active Pending
Patent Citations (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20070190023A1 (en) * | 2006-01-25 | 2007-08-16 | Michela Battista | Methods and compositions for modulating the mobilization of stem cells |
| US20170355959A1 (en) * | 2014-12-19 | 2017-12-14 | Imperial Innovations Limited | Methods for mobilising populations of stem cells |
| US20210268069A1 (en) * | 2017-12-19 | 2021-09-02 | Gpcr Therapeutics, Inc. | Gpcr heteromer inhibitors and uses thereof |
| WO2021217143A1 (en) * | 2020-04-24 | 2021-10-28 | Emory University | Aminopiperidine amides, derivatives, compositions, and uses related to cxcr4 modulation |
| WO2022064075A1 (en) * | 2020-09-28 | 2022-03-31 | Ermium Therapeutics | Cyclic isothiourea derivatives as cxcr4 modulators |
Non-Patent Citations (1)
| Title |
|---|
| See also references of EP4536239A4 * |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2025231332A1 (en) * | 2024-05-02 | 2025-11-06 | Dana-Farber Cancer Institute, Inc. | Methods of modulating erythropoiesis using beta-2 adrenergic receptor antagonists |
| WO2026020039A1 (en) * | 2024-07-18 | 2026-01-22 | Gpcr Therapeutics, Inc. | Cxcr4 inhibitors and/or beta adrenergic receptor inhibitors for mobilization of lymphocytes andimmune cells |
Also Published As
| Publication number | Publication date |
|---|---|
| US20250360149A1 (en) | 2025-11-27 |
| KR20250023521A (en) | 2025-02-18 |
| CN119562815A (en) | 2025-03-04 |
| AU2023285050A1 (en) | 2025-01-23 |
| CA3258771A1 (en) | 2023-12-14 |
| JP2025519561A (en) | 2025-06-26 |
| EP4536239A4 (en) | 2026-04-22 |
| EP4536239A1 (en) | 2025-04-16 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Luker et al. | At the Bench: Pre-clinical evidence for multiple functions of CXCR4 in cancer | |
| US20240115612A1 (en) | Articles of manufacture and methods for treatment using adoptive cell therapy | |
| Deutsch et al. | Megakaryocyte development and platelet production | |
| Hogstad et al. | RAF/MEK/extracellular signal–related kinase pathway suppresses dendritic cell migration and traps dendritic cells in Langerhans cell histiocytosis lesions | |
| Schatteman et al. | Biology of bone marrow-derived endothelial cell precursors | |
| AU2019218271B2 (en) | Anti-cancer regimen using anti-CD47 and anti-CD20 antibodies | |
| Ratajczak et al. | A novel perspective on stem cell homing and mobilization: review on bioactive lipids as potent chemoattractants and cationic peptides as underappreciated modulators of responsiveness to SDF-1 gradients | |
| Merli et al. | The role of interferon‐gamma and its signaling pathway in pediatric hematological disorders | |
| Karpova et al. | Continuous blockade of CXCR4 results in dramatic mobilization and expansion of hematopoietic stem and progenitor cells | |
| RU2645069C2 (en) | Compositions and methods for inhibition of stem cells and precursor cells binding with lymphoid tissue and for regeneration of germinal centers in lymph tissues | |
| CA3120869A1 (en) | Methods for treatment using adoptive cell therapy | |
| US11779631B2 (en) | CD47 blockade therapy by HDAC inhibitors | |
| Cunin et al. | Megakaryocytes compensate for Kit insufficiency in murine arthritis | |
| Wittwer et al. | High CD123 levels enhance proliferation in response to IL-3, but reduce chemotaxis by downregulating CXCR4 expression | |
| US20250360149A1 (en) | Gpcr inhibitors and uses thereof | |
| JP2014519480A (en) | Anti-IL-1R1 inhibitor used in cancer | |
| JP2021535083A (en) | CD80 extracellular domain FC fusion protein administration regimen | |
| Labanca et al. | Talquetamab in multiple myeloma: efficacy, safety, and future directions | |
| WO2019152516A1 (en) | Methods and compositions for treating inflammatory or autoimmune diseases or conditions using calcitonin receptor activators | |
| Sukhtankar et al. | GPC-100, a novel CXCR4 antagonist, improves in vivo hematopoietic cell mobilization when combined with propranolol | |
| EP3273984B1 (en) | Use of kit inhibitors to condition subjects for a hematopoietic stem cell (hsc) transplantation | |
| Fang et al. | A novel small molecule CXCR4 antagonist potently mobilizes hematopoietic stem cells in mice and monkeys | |
| AU2024334309A1 (en) | Gpcr inhibitors and uses thereof | |
| EP3302710A1 (en) | Mobilizing agents and uses therefor | |
| Brozowski et al. | Targeting the molecular and cellular interactions of the bone marrow niche in immunologic disease |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 23820497 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2024572376 Country of ref document: JP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 18873710 Country of ref document: US |
|
| WWE | Wipo information: entry into national phase |
Ref document number: AU2023285050 Country of ref document: AU |
|
| ENP | Entry into the national phase |
Ref document number: 20257001078 Country of ref document: KR Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 1020257001078 Country of ref document: KR Ref document number: 2023820497 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2023820497 Country of ref document: EP Effective date: 20250110 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 202380053854.3 Country of ref document: CN |
|
| ENP | Entry into the national phase |
Ref document number: 2023285050 Country of ref document: AU Date of ref document: 20230609 Kind code of ref document: A |
|
| WWP | Wipo information: published in national office |
Ref document number: 1020257001078 Country of ref document: KR |
|
| WWP | Wipo information: published in national office |
Ref document number: 202380053854.3 Country of ref document: CN |
|
| WWP | Wipo information: published in national office |
Ref document number: 2023820497 Country of ref document: EP |
|
| WWP | Wipo information: published in national office |
Ref document number: 18873710 Country of ref document: US |