WO2024225457A1 - IgA腎症の判定方法 - Google Patents
IgA腎症の判定方法 Download PDFInfo
- Publication number
- WO2024225457A1 WO2024225457A1 PCT/JP2024/016523 JP2024016523W WO2024225457A1 WO 2024225457 A1 WO2024225457 A1 WO 2024225457A1 JP 2024016523 W JP2024016523 W JP 2024016523W WO 2024225457 A1 WO2024225457 A1 WO 2024225457A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- iga
- iga nephropathy
- determining
- nephropathy
- marker protein
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Images


Classifications
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/564—Immunoassay; Biospecific binding assay; Materials therefor for pre-existing immune complex or autoimmune disease, i.e. systemic lupus erythematosus, rheumatoid arthritis, multiple sclerosis, rheumatoid factors or complement components C1-C9
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6854—Immunoglobulins
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6893—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids related to diseases not provided for elsewhere
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/34—Genitourinary disorders
- G01N2800/347—Renal failures; Glomerular diseases; Tubulointerstitial diseases, e.g. nephritic syndrome, glomerulonephritis; Renovascular diseases, e.g. renal artery occlusion, nephropathy
Definitions
- the present invention relates to a method for determining the possibility of developing IgA nephropathy or disease activity by blood-mediated liquid biopsy.
- Immunoglobulin A (IgA) nephropathy is a chronic glomerulonephritis characterized by deposition of IgA1 and complement C3 in the mesangial region of the glomerulus, mesangial cell proliferation, and matrix proliferation. Autoantibodies are formed against glycosylated IgA1, and immune complexes containing galactose-deficient glycosylated IgA1 and its autoantibodies are formed in the blood. It is believed that the deposition of the formed immune complexes in the mesangial region of the glomerulus induces nephritis and leads to renal damage.
- IgA nephropathy is the most frequent primary glomerulonephritis, but approximately 20-40% of cases develop end-stage renal failure 20-30 years after renal biopsy, and it is a disease with a poor prognosis, requiring renal replacement therapy such as hemodialysis. For this reason, early diagnosis and treatment, as well as accurate evaluation of disease activity, are important for IgA nephropathy.
- the initial symptom of IgA nephropathy is mainly abnormal urine test results, and the disease is often discovered when hematuria or proteinuria is detected during a health check.
- a definitive diagnosis of IgA nephropathy requires a pathological diagnosis based on renal tissue findings from a renal biopsy, but renal biopsy requires hospitalization and is highly invasive. It is not easy to perform frequent renal biopsies on the same patient to evaluate disease activity. Meanwhile, the traditional methods of evaluating disease activity based on proteinuria, hematuria, or serum creatinine used in diagnosis are simple and useful methods, but there are limitations to their accuracy.
- IgA nephropathy the main treatments for IgA nephropathy are supportive therapy centered on RA (renin-angiotensin) system inhibitors, and aggressive therapy that includes supportive therapy plus immunosuppressants such as corticosteroids or tonsillectomy.
- RA renin-angiotensin
- immunosuppressants such as corticosteroids or tonsillectomy.
- simple tests such as serum tests, that can diagnose IgA nephropathy or evaluate disease activity, as a means of determining whether or not to perform aggressive treatment at the time of initial onset and recurrence.
- the complement pathways involved in IgA nephropathy are said to be the alternative pathway and the lectin pathway. It has been reported that the serum concentration of complement factor H-related protein 1 (FHRP1), one of the regulatory factors in the blood of the alternative pathway, tends to be increased in patients with IgA nephropathy compared to healthy individuals (Non-Patent Document 1). However, the difference in serum concentration between healthy individuals and patients with IgA nephropathy is slight, making it difficult to use clinically as a marker for the onset of IgA nephropathy.
- FHRP1 complement factor H-related protein 1
- the present invention aims to provide a method for determining the possibility of developing IgA nephropathy or disease activity by blood-mediated liquid biopsy, instead of the highly invasive renal biopsy or the conventionally used proteinuria or hematuria.
- the inventors conducted intensive research to solve the above problems, and as a result, they used a mass spectrometer to analyze samples from patients with IgA nephropathy and samples from people without IgA nephropathy, and succeeded in identifying a new protein that is specifically elevated in patients with IgA nephropathy. They discovered that by using this protein as a marker, it is possible to obtain useful information about the presence or absence of IgA nephropathy and the state of the disease, and thus completed the present invention.
- a method for determining a possibility of developing IgA nephropathy or disease activity in a test animal comprising: (a) measuring an IgA nephropathy marker protein contained in an IgA immune complex in a blood sample collected from the test animal; (b) determining the possibility of developing IgA nephropathy or disease activity of the subject animal based on the amount of the IgA nephropathy marker protein measured in the step (a); having A method for determining IgA nephropathy, wherein the IgA nephropathy marker protein is a protein contained in an IgA immune complex, and the amount of the protein contained in the IgA immune complex of a group of IgA nephropathy patients is greater than the amount contained in the IgA immune complex of a group of healthy subjects.
- the step (a) (c-1) separating serum or plasma from a blood sample collected from a subject animal; (c-2) recovering the IgA immune complexes contained in the serum or plasma obtained in the step (c-1); (c-3) measuring the IgA nephropathy marker protein in the IgA immune complex recovered in the step (c-2); The method for diagnosing IgA nephropathy according to [1] above, [3]
- the subject animal is an animal diagnosed as having IgA nephropathy, The method for determining IgA nephropathy according to any of [1] to [10] above, wherein, in the step (b), if the amount of the IgA nephropathy marker protein measured in the step (a) is lower than the amount of the IgA nephropathy marker protein contained in the IgA immune complex in a blood sample collected from the test animal before the blood sample provided in the step (a) was collected, it is determined that the pathological condition of the IgA nephropathy of the test animal has improved.
- a kit for determining the possibility of developing IgA nephropathy or disease activity in a test animal comprising:
- the present invention relates to a method for treating IgA nephropathy comprising the steps of:
- the subject animal is an animal diagnosed as having IgA nephropathy
- the method for determining IgA nephropathy according to the present invention can provide information useful for the presence or absence of IgA nephropathy or for evaluating treatment methods using blood as a sample. Since the method does not require a renal biopsy on a subject animal, it is expected that the burden on patients will be reduced and appropriate treatment can be provided to patients.
- the kit for diagnosing IgA nephropathy according to the present invention the method for diagnosing IgA nephropathy can be carried out more simply.
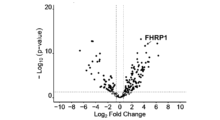
- FIG. 1 shows the results of comparing the relative abundance of proteins in IgA immune complexes between an IgA nephropathy group (supportive therapy group + aggressive therapy group) (at the time of kidney biopsy) and a healthy control group in Example 1.
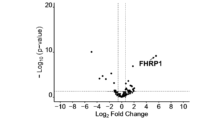
- FIG. 2 shows the results of comparing proteins in IgA immune complexes before and after treatment in the active IgA nephropathy treatment group in Example 1.
- FIG. 2 shows the measurement results of the amount of FHRP1 contained in IgA immune complexes (amount of FHRP1 contained per 10 ⁇ g of IgA [ng/10 ⁇ g of IgA]) in each group in Example 1.
- FIG. 1 shows the results of comparing the amount of FHRP1 (amount of FHRP1 contained per 10 ⁇ g of IgA [ng/IgA 10 ⁇ g]) before and after treatment in each group in Example 1.
- an "IgA nephropathy marker protein” is a protein contained in the IgA immune complex in the blood, and is contained in a greater amount in the IgA immune complex of a group of IgA nephropathy patients than in a group of healthy subjects.
- IgA nephropathy marker proteins can be identified by the following method. First, blood samples are taken from a group of IgA nephropathy patients who have been definitively diagnosed with IgA nephropathy by other means such as kidney biopsy, and a group of healthy individuals, and the amount of each protein contained in the IgA immune complex in the blood samples is measured. The average amount of protein contained in the IgA immune complex is calculated for the IgA nephropathy patients and healthy individuals, and proteins whose average value for the IgA nephropathy patients is significantly higher than the average value for the healthy individuals can be identified as IgA nephropathy marker proteins.
- IgA nephropathy marker proteins include alpha-1-antitrypsin, apolipoprotein C-1, FHRP1 (Complement factor H related protein 1), cathepsin G, SLC13A4 (Solute carrier family 13 member 4), alpha-2-macroglobulin, myeloperoxidase, C1QB (Complement C1q subcomponent subunit B), RhoGAP42 (Rho GTPase-activating protein 42), and C1QC (Complement C1q subcomponent subunit C).
- the method for determining IgA nephropathy is a method for determining the possibility of developing IgA nephropathy or disease activity in a test animal, and comprises the following steps: (a) measuring an IgA nephropathy marker protein contained in an IgA immune complex in a blood sample collected from a test animal; (b) determining the possibility of developing IgA nephropathy or disease activity of the subject animal based on the amount of the IgA nephropathy marker protein measured in the step (a).
- the above steps (a) and (b) are steps carried out in vitro.
- the IgA nephropathy marker protein used in the present invention may be one type, or two or more types may be used in combination.
- the IgA nephropathy marker protein may be one or more types selected from the group consisting of alpha 1-antitrypsin, apolipoprotein C-1, FHRP1, cathepsin G, SLC13A4, alpha 2-macroglobulin, myeloperoxidase, C1QB, RhoGAP42, and C1QC.
- FHRP1 as the IgA nephropathy marker protein.
- step (a) the IgA nephropathy marker protein contained in the IgA immune complex in a blood sample collected from the subject animal is measured.
- the method for determining IgA nephropathy according to the present invention makes it possible to accurately determine whether or not a subject animal has developed IgA nephropathy.
- the method for determining IgA nephropathy according to the present invention provides information useful for evaluating disease activity in cases where the subject has IgA nephropathy.
- the method for measuring the amount of IgA nephropathy marker protein contained in the IgA immune complex in a blood sample collected from a test animal is not particularly limited.
- serum or plasma can be prepared from the blood sample, the IgA immune complex contained therein can be recovered, and the IgA nephropathy marker protein in the recovered IgA immune complex can be measured.
- the measurement of the IgA nephropathy marker protein in the IgA immune complex in the step (a) can be carried out, for example, by the following steps (c-1) to (c-3).
- (c-1) separating serum or plasma from a blood sample collected from a subject animal;
- (c-2) recovering the IgA immune complexes contained in the serum or plasma obtained in the step (c-1);
- (c-3) A step of measuring an IgA nephropathy marker protein in the IgA immune complex recovered in the step (c-2).
- the subject animal is not particularly limited as long as it is an animal that has kidneys.
- mammals are preferred, and experimental animals such as humans, mice, rats, and monkeys, and livestock or pets such as rabbits, dogs, cats, cows, horses, and sheep are more preferred, and humans are particularly preferred.
- the subject animal in the method for determining IgA nephropathy according to the present invention is preferably an animal suspected of developing nephropathy.
- animals suspected of developing nephropathy include animals in which an increase in the amount of protein in the urine or pathologies observed in nephropathy, such as hematuria, have been confirmed, and in particular, animals diagnosed with hematuria or proteinuria are preferred.
- the amount of protein in the urine is 0.15 g/day or more in terms of creatinine, the onset of nephropathy is suspected, and therefore such animals are suitable as subject animals in the method for determining IgA nephropathy according to the present invention.
- the preparation of plasma or serum from blood collected from a subject animal can be carried out by a conventional method.
- blood can be collected from a subject animal in a blood collection tube that has already contained an anticoagulant such as sodium citrate, heparin, EDTA, or sodium fluoride, and then the blood collection tube can be centrifuged to precipitate blood cell components and recover the supernatant, which is plasma.
- the blood can be coagulated and then centrifuged to precipitate blood cell components and recover the supernatant, which is serum.
- the blood collected from a subject animal, or the plasma or serum prepared from it can be used to recover IgA immune complexes immediately after preparation, or can be used to recover IgA immune complexes after a predetermined period of storage.
- the plasma or serum can be stored in a refrigerator or freezer, at room temperature, or as a frozen powder after freeze-drying.
- the plasma or serum can be diluted with an appropriate buffer or various additives can be added as a pretreatment.
- additives include surfactants, protease inhibitors, nuclease inhibitors, pH adjusters, and pH indicators.
- the recovery of IgA immune complexes contained in serum or plasma can be carried out by various methods that can increase the concentration of IgA immune complexes compared to before recovery.
- the anti-IgA antibody is not particularly limited as long as it is an antibody that can selectively bind to IgA in the IgA immune complexes, and various anti-IgA antibodies can be used.
- an antibody that specifically recognizes IgA with abnormal glycosylation such as galactose-deficient IgA
- galactose-deficient IgA can also be used as the anti-IgA antibody in the present invention, and can be used to recover IgA immune complexes.
- the method for measuring the IgA nephropathy marker protein in the collected IgA immune complex is not particularly limited as long as it is a method that can generally measure the concentration of the target protein.
- the IgA nephropathy marker protein can be measured by an immunological method using an antibody against the IgA nephropathy marker protein.
- immunological methods include ELISA (enzyme-linked immunosorbent assay), latex agglutination, and immunochromatography. These methods can be performed by standard methods using an antibody against the IgA nephropathy marker protein.
- the IgA nephropathy marker protein can also be measured by a method that utilizes mass spectrometry, such as liquid chromatography mass spectrometry.
- the "amount of IgA nephropathy marker protein in IgA immune complexes” may be the value obtained by quantifying the IgA nephropathy marker protein itself, but it is preferable to use a "relative value to the amount of IgA protein in IgA immune complexes" since this allows for more accurate comparison of the amount of IgA nephropathy marker protein between samples. Specifically, it is preferable to carry out step (a) in the following steps (c-1) to (c-5). Steps (c-1) to (c-3) can be carried out in the same manner as described above.
- c-1) separating serum or plasma from a blood sample collected from a subject animal; (c-2) recovering the IgA immune complexes contained in the serum or plasma obtained in the step (c-1); (c-3) measuring the IgA nephropathy marker protein in the IgA immune complex recovered in the step (c-2); (c-4) measuring the IgA protein in the IgA immune complexes recovered in the step (c-2); (c-5) a step of calculating the amount of IgA nephropathy marker protein contained in the IgA immune complex in the blood sample collected from the test animal by dividing the amount of IgA nephropathy marker protein measured in the step (c-3) by the amount of IgA protein measured in the step (c-4) ([amount of IgA nephropathy marker protein in IgA immune complex]/[amount of IgA protein in IgA immune complex]).
- the measurement of IgA protein in step (c-4) can be carried out, for example, by an immunological method using an anti-IgA antibody or a method using mass spectrometry such as liquid chromatography mass spectrometry.
- immunological methods include ELISA, latex agglutination, and immunochromatography.
- step (c-4) the amount of IgA protein in step (c-4) by the same method as that used to measure the amount of IgA nephropathy marker protein in step (c-3).
- step (b) the presence or absence of onset of IgA nephropathy in a test animal, or the possibility of onset, is determined based on the amount of IgA nephropathy marker protein measured in step (a).
- the amount of the IgA nephropathy marker protein used in the present invention contained in IgA immune complexes in the blood tends to be significantly higher in patients with IgA nephropathy than in healthy subjects.
- the amount of the IgA nephropathy marker protein contained in IgA immune complexes in the blood of the test animal can be used to determine the presence or absence of onset of IgA nephropathy in a test animal, or the possibility of onset.
- a threshold value for distinguishing between IgA nephropathy sufferers and non-affected individuals is set in advance, the amount of IgA nephropathy marker protein contained in the IgA immune complexes in the blood of the test animal is measured, and it is determined whether the amount of said protein is equal to or greater than the threshold value set in advance for distinguishing between IgA nephropathy patients and healthy subjects. If the measured amount of IgA nephropathy marker protein is equal to or greater than the specified threshold, it is determined that there is a high possibility that the test animal has developed (has) IgA nephropathy.
- the threshold value for separating the group of IgA nephropathy patients from the group of healthy individuals can be experimentally set, taking into consideration the method for measuring the IgA nephropathy marker protein, etc.
- the IgA nephropathy determination method according to the present invention can be performed on blood collected from a group known not to have IgA nephropathy and blood collected from a group known to have IgA nephropathy, measuring the amount of IgA nephropathy marker protein contained in the IgA immune complexes in each blood sample, and comparing the measured values for both groups, thereby appropriately setting the threshold value.
- the amount of IgA nephropathy marker protein contained in the IgA immune complex in the blood tends to decrease rapidly after active treatment. From this, it is expected that the amount of IgA nephropathy marker protein contained in the IgA immune complex in the blood is positively correlated with the disease activity of IgA nephropathy. Therefore, by setting an appropriate threshold, it is possible to accurately evaluate not only the presence or absence or possibility of onset of IgA nephropathy, but also the disease activity of IgA nephropathy, and it is preferable that the obtained evaluation is provided to a physician as information useful for formulating a treatment plan.
- the disease activity of IgA nephropathy can also be determined.
- the disease activity of IgA nephropathy in a test animal can also be evaluated by measuring the amount of IgA nephropathy marker protein contained in IgA immune complexes in blood samples collected from the same test animal over time and comparing these amounts.
- the amount of IgA nephropathy marker protein measured in step (a) is lower than the amount of IgA nephropathy marker protein contained in IgA immune complexes in a blood sample collected from the same test animal before the blood sample used for the measurement was collected, it can be determined that the disease activity of IgA nephropathy in the test animal has decreased and the pathological condition has improved.
- the obtained evaluation is preferably provided to a doctor as information useful for formulating a treatment plan.
- subject animals assessed as having a high probability of developing IgA nephropathy and subject animals assessed as having high disease activity have a high amount of IgA nephropathy marker protein contained in IgA immune complexes in their blood. Therefore, aggressive treatment such as corticosteroid therapy and tonsillectomy is predicted to be effective for subject animals assessed as having a high probability of developing IgA nephropathy or having high disease activity in the method for assessing IgA nephropathy according to the present invention.
- the method for assessing IgA nephropathy according to the present invention can be performed on IgA nephropathy patients diagnosed with IgA nephropathy in order to obtain information for selecting a treatment method.
- FHRP1 is one of the control factors of the complement pathway, such as the alternative pathway or the lectin pathway
- the IgA nephropathy marker protein contained in the IgA immune complex in the blood is high
- the IgA nephropathy that the subject develops is likely to be caused by complement activation. Therefore, in the method for determining IgA nephropathy according to the present invention, it is predicted that treatment with a complement inhibitor targeting the alternative pathway or the lectin pathway will be effective for subject animals that are evaluated as having a high possibility of developing IgA nephropathy or high disease activity.
- the method for determining IgA nephropathy according to the present invention can provide useful information for selecting patients who will use complement treatment drugs and predicting the effectiveness of treatment.
- Examples of complement treatment drugs for the alternative pathway include LNP023 (manufactured by Novartis), and examples of complement treatment drugs for the lectin pathway include Narsoprimab (manufactured by Omeros).
- the method for determining IgA nephropathy according to the present invention can be carried out more easily by preparing a kit including reagents and devices used for recovering IgA immune complexes and quantifying IgA nephropathy marker proteins and IgA proteins.
- a kit for determining the possibility of developing IgA nephropathy or disease activity in a subject animal preferably contains an anti-IgA antibody and an antibody against the IgA nephropathy marker protein.
- the kit for determining the disease activity of IgA nephropathy in a test animal according to the present invention can be used to predict the effectiveness of treatment for a patient with IgA nephropathy.
- the present invention provides the use of an anti-IgA antibody and an antibody against an IgA nephropathy marker protein to manufacture a kit for predicting the efficacy of treatment for an IgA nephropathy patient.
- the present invention provides an anti-IgA antibody and an antibody against an IgA nephropathy marker protein for predicting the efficacy of treatment for an IgA nephropathy patient.
- the present invention may include other steps in addition to steps (a) and (b).
- steps (a) and (b) include (c) treating a patient with IgA nephropathy based on the evaluation results of the possibility of developing IgA nephropathy or disease activity determined in step (b).
- step (c) is further included in addition to steps (a) and (b)
- the method of this embodiment may be a method for treating a patient with IgA nephropathy.
- a treatment plan for IgA nephropathy can be determined based on the evaluation results of the likelihood of developing IgA nephropathy or disease activity.
- Treatment for IgA nephropathy patients who are evaluated as having a high likelihood of developing IgA nephropathy or high disease activity may be complement inhibitor therapy targeting the alternative pathway or lectin pathway, or active treatment such as corticosteroid therapy and tonsillectomy. Of these, either or both of complement inhibitor therapy targeting the alternative pathway or lectin pathway and corticosteroid therapy are preferred.
- a method for treating a patient with IgA nephropathy comprising: (a) measuring an IgA nephropathy marker protein contained in an IgA immune complex in a blood sample collected from a test animal; (b) determining the possibility of developing IgA nephropathy or disease activity of the subject animal based on the amount of the IgA nephropathy marker protein measured in the step (a); (c) treating a patient with IgA nephropathy based on the evaluation result of the possibility of developing IgA nephropathy or disease activity determined in the step (b); having A method for treating patients with IgA nephropathy, wherein the IgA nephropathy marker protein is a protein contained in an IgA immune complex, and the amount of the protein contained in the IgA immune complex of a group of IgA nephropathy patients is greater than the amount contained in the IgA immune complex of a group of healthy subjects.
- Example 1 In order to identify novel biomarker candidate proteins that can diagnose IgA nephropathy and determine disease activity by measuring blood levels without performing renal biopsy in patients with IgA nephropathy, we performed proteomic analysis of IgA immune complexes in the blood to search for proteins that are specifically increased in patients with IgA nephropathy.
- the supportive care group included cases in which renal dysfunction had already progressed, cases in which tissue obtained by renal biopsy showed few acute lesions, or cases in which urinalysis findings were mild.
- Treatment consisted of conservative therapy centered on RA system inhibitors.
- aggressive treatment group consisted of patients treated with tonsillectomy and steroid pulse therapy (the method of Pozzi et al.). This group included patients with histological acute lesions and severe urinalysis findings.
- IgA immune complexes Separation and purification of IgA immune complexes from serum IgA immune complexes were separated and purified from 100 ⁇ L of each serum by affinity chromatography using a cyanogen bromide-activated Sepharose column bound with anti-human IgA antibody (product number: 0855068, manufactured by Cappel Laboratories). Specifically, 100 ⁇ L of serum and 1 mL of phosphate buffered saline were added, filtered through a 0.45 ⁇ m filter, and then adsorbed onto the affinity column. After washing the affinity column with phosphate buffered saline, the IgA immune complexes were eluted with 0.1 M glycine hydrochloride buffer (pH 2.7). The eluted solution was neutralized with 1.0 M Tris-HCl buffer (pH 9.0).
- the separated and purified IgA immune complexes were concentrated using an ultrafiltration membrane (product name: Ultra-4 30K Centrifugal Filter Units, Amicon) by centrifugation at 2330 x g and 4°C for 20 minutes.
- the absorbance at a wavelength of 280 nm was then measured using a Nano Vue spectrophotometer (GE) to calculate the protein concentration.
- trypsin product name: V528A, manufactured by Promega
- 100 mM ammonium bicarbonate solution pH 8.3
- enzyme treatment was performed again overnight at 37° C.
- the entire sample after enzyme treatment was desalted using a C18 spin column (product name: 89870, manufactured by Thermo Fisher Scientific). Finally, the sample was dried using a SpeedVac.
- the dried measurement samples were dissolved in 20 ⁇ L of 0.1% formic acid, and the protein concentration was adjusted to 0.1 ⁇ g/L and the final concentration of DTT to 20 mM. Measurements were performed using liquid chromatography-high resolution mass spectrometry (LC-HRMS) and comprehensive analysis was performed using a label-free quantitative method.
- LC-HRMS liquid chromatography-high resolution mass spectrometry
- Mass spectrometry was performed using an EASY-nLC 1000 system and an Orbitrap Fusion mass spectrometer (both manufactured by Thermo Fisher Scientific). Liquid chromatography was performed using a concentration gradient of acetonitrile from 0% to 35%, with elution at a flow rate of 300 nL/min over 120 minutes.
- Figure 1 shows the results of comparing the relative abundance of proteins in IgA immune complexes between the IgA nephropathy group (supportive care group + active treatment group) (at the time of kidney biopsy) and the healthy control group.
- the horizontal axis shows the logarithm of the relative ratio of protein abundance in the IgA nephropathy group/healthy control group [Log2 (Fold change)], and the vertical axis shows the P value [-Log10 (P value)].
- Black circles shifted in the positive direction of the logarithm [Log2 (Fold change)] indicate proteins that were abundant in IgA nephropathy, and black circles shifted in the negative direction indicate proteins that were abundant in healthy control subjects.
- FHRP1 was present in higher amounts in IgA immune complexes compared to healthy control subjects. Proteins that were significantly more abundant in IgA nephropathy patients, including FHRP1, are shown in Table 4.
- Figure 2 shows the results of comparing proteins in IgA immune complexes before and after treatment in the aggressive IgA nephropathy treatment group.
- the horizontal axis shows the logarithm [Log2 (Fold change)] of the relative ratio of protein abundance before/after treatment (approximately 2 years later) in the aggressive IgA nephropathy treatment group
- the vertical axis shows the P value [-Log10 (P value)].
- Black circles shifted in the positive direction of the logarithm [Log2 (Fold change)] indicate proteins that were abundant before treatment
- black circles shifted in the negative direction indicate proteins that were abundant after treatment.
- FHRP1 was found to be a protein that is significantly more abundant in IgA nephropathy patients than in healthy subjects, and that is significantly reduced by aggressive treatment ( Figures 1 and 2).
- the IgA concentration of the IgA immune complex solution collected in (2) above was calculated using a commercially available ELISA kit for measuring IgA (product name: "IgA Human Uncoated ELISA kit", manufactured by Thermo Fischer Scientific). Using this measured value, the IgA concentration was adjusted to 10 ⁇ g/mL, and the FHRP1 concentration was measured using a commercially available ELISA kit for measuring human CFHR (product name: "RayBio (registered trademark) Human CFHR1 ELISA kit", manufactured by RayBiotech) according to the procedure provided with the kit.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Engineering & Computer Science (AREA)
- Immunology (AREA)
- Hematology (AREA)
- Molecular Biology (AREA)
- Chemical & Material Sciences (AREA)
- Biomedical Technology (AREA)
- Urology & Nephrology (AREA)
- Cell Biology (AREA)
- Analytical Chemistry (AREA)
- Biotechnology (AREA)
- Pathology (AREA)
- Food Science & Technology (AREA)
- Medicinal Chemistry (AREA)
- Physics & Mathematics (AREA)
- Microbiology (AREA)
- Biochemistry (AREA)
- General Health & Medical Sciences (AREA)
- General Physics & Mathematics (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Rehabilitation Therapy (AREA)
- Rheumatology (AREA)
- Investigating Or Analysing Biological Materials (AREA)
Abstract
Description
本願は、2023年4月26日に、日本に出願された特願2023-072454号に基づき優先権を主張し、その内容をここに援用する。
[1] 被験動物のIgA腎症の発症可能性又は疾患活動性を判定する方法であって、(a)被験動物から採取された血液試料中のIgA免疫複合体に含まれているIgA腎症マーカータンパク質を測定する工程と、
(b)前記工程(a)において測定された前記IgA腎症マーカータンパク質の量に基づいて、前記被験動物のIgA腎症の発症可能性又は疾患活動性を判定する工程と、
を有し、
前記IgA腎症マーカータンパク質は、IgA免疫複合体に含まれているタンパク質であって、IgA腎症罹患者群のIgA免疫複合体に含まれている量が、健常者群のIgA免疫複合体に含まれている量よりも多いタンパク質である、IgA腎症の判定方法。
[2] 前記工程(a)を、
(c-1)被験動物から採取された血液試料から血清又は血漿を分離する工程と、
(c-2)前記工程(c-1)において得られた血清又は血漿に含まれているIgA免疫複合体を回収する工程と、
(c-3)前記工程(c-2)において回収されたIgA免疫複合体中のIgA腎症マーカータンパク質を測定する工程と、
により行う、前記[1]のIgA腎症の判定方法。
[3] 前記工程(a)を、
(c-1)被験動物から採取された血液試料から血清又は血漿を分離する工程と、
(c-2)前記工程(c-1)において得られた血清又は血漿に含まれているIgA免疫複合体を回収する工程と、
(c-3)前記工程(c-2)において回収されたIgA免疫複合体中のIgA腎症マーカータンパク質を測定する工程と、
(c-4)前記工程(c-2)において回収されたIgA免疫複合体中のIgAタンパク質を測定する工程と、
(c-5)前記工程(c-3)で測定されたIgA腎症マーカータンパク質の量を、前記工程(c-4)で測定されたIgAタンパク質の量で除した値を、前記被験動物から採取された血液試料中のIgA免疫複合体に含まれているIgA腎症マーカータンパク質の量として求める工程と、
により行う、前記[1]のIgA腎症の判定方法。
[4] 前記工程(c-2)において、IgA免疫複合体の回収を、抗IgA抗体を用いたアフィニティークロマトグラフィーにより行う、前記[2]又は[3]のIgA腎症の判定方法。
[5] IgA免疫複合体中の前記IgA腎症マーカータンパク質の測定を、前記IgA腎症マーカータンパク質に対する抗体を用いた免疫学的手法により行う、前記[1]~[4]のいずれかのIgA腎症の判定方法。
[6] 前記免疫学的手法が、ELISA法、ラテックス凝集法、又はイムノクロマトグラフィー法である、前記[5]のIgA腎症の判定方法。
[7] IgA免疫複合体中の前記IgA腎症マーカータンパク質の測定を、液体クロマトグラフ質量分析法により行う、前記[1]~[4]のいずれかのIgA腎症の判定方法。
[8] 前記IgA腎症マーカータンパク質が、アルファ1-アンチトリプシン、アポリポプロテインC-1、FHRP1、カテプシンG、SLC13A4、アルファ2-マクログロブリン、ミエロペルオキシダーゼ、C1QB、RhoGAP42、及びC1QCからなる群より選択される1種以上である、前記[1]~[7]のいずれかのIgA腎症の判定方法。
[9] 前記工程(b)において、前記工程(a)において測定された前記IgA腎症マーカータンパク質の量が、IgA腎症患者群と健常者群を鑑別するための予め設定された閾値よりも多い場合に、前記被験動物はIgA腎症を発症している可能性が高いと判定する、前記[1]~[8]のいずれかのIgA腎症の判定方法。
[10] 前記被験動物がIgA腎症を発症している可能性が高いと判定された場合に、前記被験動物は、副腎皮質ステロイド治療が有効であると予測する、前記[9]のIgA腎症の判定方法。
[11] 前記被験動物がIgA腎症を発症している可能性が高いと判定された場合に、前記被験動物は、副経路又はレクチン経路を標的とした補体阻害薬治療が有効であると予測する、前記[9]のIgA腎症の判定方法。
[12] 前記被験動物が、腎症の発症が疑われている動物である、前記[1]~[11]のいずれかのIgA腎症の判定方法。
[13] 前記被験動物が、血尿又はタンパク質尿と診断された動物である、前記[1]~[12]のいずれかのIgA腎症の判定方法。
[14] 前記被験動物がIgA腎症を発症していると診断された動物であり、
前記工程(b)において、前記工程(a)において測定された前記IgA腎症マーカータンパク質の量が、前記工程(a)において供された血液試料が採取された時点以前に前記被験動物から採取された血液試料中のIgA免疫複合体に含まれている前記IgA腎症マーカータンパク質の量よりも低下している場合に、前記被験動物のIgA腎症の病態が改善したと判定する、前記[1]~[10]のいずれかのIgA腎症の判定方法。
[15] 被験動物のIgA腎症の発症可能性又は疾患活動性を判定するためのキットであって、
抗IgA抗体と、IgA腎症マーカータンパク質に対する抗体とを備え、
前記IgA腎症マーカータンパク質は、IgA免疫複合体に含まれているタンパク質であって、IgA腎症罹患者群のIgA免疫複合体に含まれている量が、健常者群のIgA免疫複合体に含まれている量よりも多いタンパク質である、IgA腎症の判定用キット。
[16] 前記IgA腎症マーカータンパク質が、アルファ1-アンチトリプシン、アポリポプロテインC-1、FHRP1、カテプシンG、SLC13A4、アルファ2-マクログロブリン、ミエロペルオキシダーゼ、C1QB、RhoGAP42、及びC1QCからなる群より選択される1種以上である、前記[15]のIgA腎症の判定用キット。
[17] 前記被験動物のIgA腎症の発症可能性を判定するために用いられる、前記[15]又は[16]のIgA腎症の判定用キット。
[18] 前記被験動物がIgA腎症を発症していると診断された動物であり、
前記被験動物の治療法の選択のための情報を得るために用いられる、前記[15]又は[16]のIgA腎症の判定用キット。
本発明に係るIgA腎症の判定用キットを用いることにより、前記IgA腎症の判定方法をより簡便に実施することができる。
(a)被験動物から採取された血液試料中のIgA免疫複合体に含まれているIgA腎症マーカータンパク質を測定する工程と、
(b)前記工程(a)において測定された前記IgA腎症マーカータンパク質の量に基づいて、前記被験動物のIgA腎症の発症可能性又は疾患活動性を判定する工程。
上記工程(a)及び(b)は、in vitroで行われる工程である。
(c-1)被験動物から採取された血液試料から血清又は血漿を分離する工程と、
(c-2)前記工程(c-1)において得られた血清又は血漿に含まれているIgA免疫複合体を回収する工程と、
(c-3)前記工程(c-2)において回収されたIgA免疫複合体中のIgA腎症マーカータンパク質を測定する工程。
(c-2)前記工程(c-1)において得られた血清又は血漿に含まれているIgA免疫複合体を回収する工程と、
(c-3)前記工程(c-2)において回収されたIgA免疫複合体中のIgA腎症マーカータンパク質を測定する工程と、
(c-4)前記工程(c-2)において回収されたIgA免疫複合体中のIgAタンパク質を測定する工程と、
(c-5)前記工程(c-3)で測定されたIgA腎症マーカータンパク質の量を、前記工程(c-4)で測定されたIgAタンパク質の量で除した値([IgA免疫複合体中のIgA腎症マーカータンパク質の量]/[IgA免疫複合体中のIgAタンパク質の量])を、前記被験動物から採取された血液試料中のIgA免疫複合体に含まれているIgA腎症マーカータンパク質の量として求める工程。
本発明に係る被験動物のIgA腎症の疾患活動性を判定するためのキットは、IgA腎症患者に対する治療の有効性を予測するために用いることができる。
IgA腎症患者に対する治療方法であって、
(a)被験動物から採取された血液試料中のIgA免疫複合体に含まれているIgA腎症マーカータンパク質を測定する工程と、
(b)前記工程(a)において測定された前記IgA腎症マーカータンパク質の量に基づいて、前記被験動物のIgA腎症の発症可能性又は疾患活動性を判定する工程と、
(c)前記工程(b)において判定されたIgA腎症の発症可能性又は疾患活動性の評価結果に基づいて、IgA腎症患者に対して治療する工程と、
を有し、
前記IgA腎症マーカータンパク質は、IgA免疫複合体に含まれているタンパク質であって、IgA腎症罹患者群のIgA免疫複合体に含まれている量が、健常者群のIgA免疫複合体に含まれている量よりも多いタンパク質である、IgA腎症患者に対する治療方法。
IgA腎症患者に腎生検を行うことなく、血液を測定することによりIgA腎症の診断及び疾患活動性の判断ができる新規バイオマーカー候補タンパク質を同定するために、血液中のIgA免疫複合体をプロテオーム解析することにより、IgA腎症患者で特異的に増加しているタンパク質を探索した。
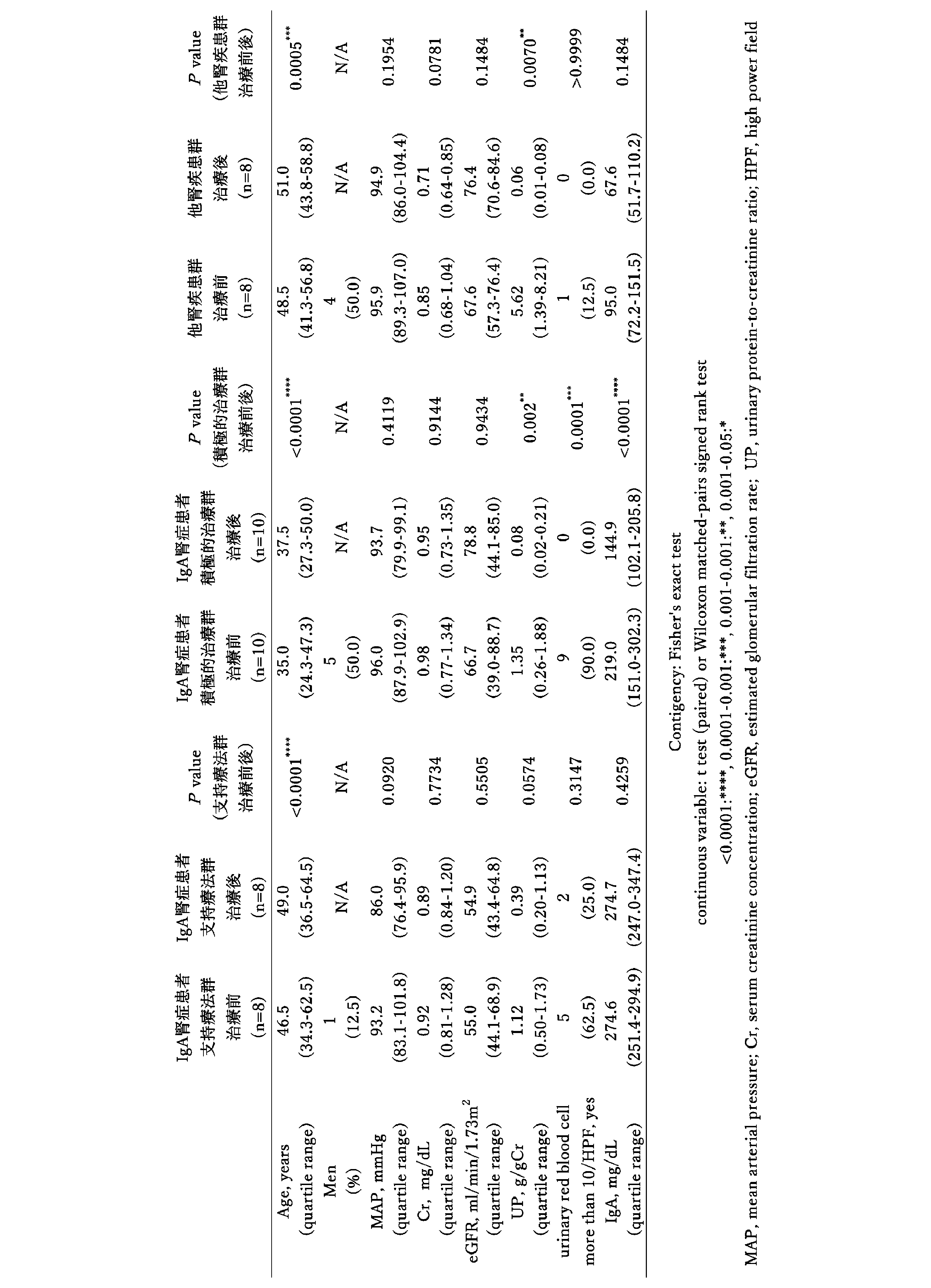
健常者(n=20)、膜性腎症や微小変化型ネフローゼ症候群の他腎疾患(IgA腎症以外)患者群(n=8)、IgA腎症患者の支持療法群(n=8)、及び、IgA腎症患者の積極的治療群(n=24)から血清を回収した(表1)。IgA腎症患者の支持療法群と積極的治療群の分類は、藤田医科大学の治療アルゴリズムに基づき、分類した。
支持療法群は、すでに腎機能障害が進行した症例、腎生検で得られた組織において急性病変に乏しい症例、あるいは検尿所見が軽微である症例が含まれる。治療は、RA系阻害薬を中心とした保存療法が行われた。一方、積極的治療群は、扁桃摘出とステロイドパルス療法(Pozziらの方式)で治療した患者群である。組織学的急性病変が認められ、検尿所見が重度である患者がこれに該当する。


各血清100μLから、抗ヒトIgA抗体(製品番号:0855068、Cappel Labporatories社製)を結合した臭化シアン活性化セファロースカラムを用いたアフィニティークロマトグラフィー法により、IgA免疫複合体を分離・精製した。具体的には、血清100μLとリン酸緩衝食塩水1mLを加え、0.45μmフィルターで濾過した後、アフィニティーカラムに吸着させた。当該アフィニティーカラムをリン酸緩衝食塩水で洗浄した後、IgA免疫複合体を0.1M グリシン塩酸緩衝液(pH2.7)で溶出した。溶出した溶液は、1.0M トリス塩酸緩衝液(pH9.0)を用いて中和した。
IgA免疫複合体5μgを、冷却したアセトンを用いて沈殿させた。その沈殿を250mM リン酸ナトリウムバッファー(pH6.0)で溶解させ、シアリダーゼA(製品名:GK80040、Prozyme社製)を2.5mU添加して、37℃で一晩の酵素処理を行った。その後、ジチオスレイトール(DTT)を終濃度20mMで添加して、室温で15分間還元処理を行った。還元後のサンプルに、100mM 炭酸水素アンモニウム溶液(pH8.3)で溶解したトリプシン(製品名:V528A、Promega社製)0.1gを添加して、再び37℃で一晩の酵素処理を行った。酵素処理後のサンプル全量に対して、C18スピンカラム(製品名:89870、Thermo Fisher Scientific社製)を用いて、脱塩処理を行った。最後に、SpeedVacを用いて、サンプルを乾固させた。
Proteome Discovererで同定されたタンパク質の相対存在量を、Perseus (version 1.6.15.0)を用いて、差違解析した。タンパク質の相対存在量をLog2変換し、各サンプルの中央値を差し引いて正規化した。欠損値に関しては、正規分布に基づいて補完した(width = 0.3、downshift = 1.8)。統計学的有意差は、Student’s t-testで検定し、P-value<0.05 かつLog2(Fold change)絶対値>0.58を満たすタンパク質を、有意差のあるタンパク質とした。

免疫学的な手法であるELISAを用いて、健常者、IgA腎症患者、他腎疾患患者(サンプル量不足のためn=7)のIgA免疫複合体中に含まれるFHRP1量を測定した。FHRP1の測定は、IgA濃度を揃えて測定し、IgA10μgあたりに含まれるFHRP1量(ng/IgA10μg)を算出した。測定値を、Kruskal Wallis testにて検定し(P<0.0001)、その後の検定をDunn’s multiple comparisons testにて行った。
Claims (11)
- 被験動物のIgA腎症の発症可能性又は疾患活動性を判定する方法であって、
(a)被験動物から採取された血液試料中のIgA免疫複合体に含まれているIgA腎症マーカータンパク質を測定する工程と、
(b)前記工程(a)において測定された前記IgA腎症マーカータンパク質の量に基づいて、前記被験動物のIgA腎症の発症可能性又は疾患活動性を判定する工程と、
を有し、
前記IgA腎症マーカータンパク質は、IgA免疫複合体に含まれているタンパク質であって、IgA腎症罹患者群のIgA免疫複合体に含まれている量が、健常者群のIgA免疫複合体に含まれている量よりも多いタンパク質である、IgA腎症の判定方法。 - 前記工程(a)を、
(c-1)被験動物から採取された血液試料から血清又は血漿を分離する工程と、
(c-2)前記工程(c-1)において得られた血清又は血漿に含まれているIgA免疫複合体を回収する工程と、
(c-3)前記工程(c-2)において回収されたIgA免疫複合体中のIgA腎症マーカータンパク質を測定する工程と、
により行う、請求項1に記載のIgA腎症の判定方法。 - 前記工程(c-2)において、IgA免疫複合体の回収を、抗IgA抗体を用いたアフィニティークロマトグラフィーにより行う、請求項2に記載のIgA腎症の判定方法。
- IgA免疫複合体中の前記IgA腎症マーカータンパク質の測定を、前記IgA腎症マーカータンパク質に対する抗体を用いた免疫学的手法により行う、請求項1~3のいずれか一項に記載のIgA腎症の判定方法。
- 前記IgA腎症マーカータンパク質が、アルファ1-アンチトリプシン、アポリポプロテインC-1、FHRP1、カテプシンG、SLC13A4、アルファ2-マクログロブリン、ミエロペルオキシダーゼ、C1QB、RhoGAP42、及びC1QCからなる群より選択される1種以上である、請求項1~3のいずれか一項に記載のIgA腎症の判定方法。
- 前記工程(b)において、前記工程(a)において測定された前記IgA腎症マーカータンパク質の量が、IgA腎症患者群と健常者群を鑑別するための予め設定された閾値よりも多い場合に、前記被験動物はIgA腎症を発症している可能性が高いと判定する、請求項1~3のいずれか一項に記載のIgA腎症の判定方法。
- 前記被験動物がIgA腎症を発症している可能性が高いと判定された場合に、前記被験動物は、副腎皮質ステロイド治療が有効であると予測する、請求項6に記載のIgA腎症の判定方法。
- 前記被験動物がIgA腎症を発症している可能性が高いと判定された場合に、前記被験動物は、副経路又はレクチン経路を標的とした補体阻害薬治療が有効であると予測する、請求項6に記載のIgA腎症の判定方法。
- 前記被験動物がIgA腎症を発症していると診断された動物であり、
前記工程(b)において、前記工程(a)において測定された前記IgA腎症マーカータンパク質の量が、前記工程(a)において供された血液試料が採取された時点以前に前記被験動物から採取された血液試料中のIgA免疫複合体に含まれている前記IgA腎症マーカータンパク質の量よりも低下している場合に、前記被験動物のIgA腎症の疾患活動性が低下したと判定する、請求項1~3のいずれか一項に記載のIgA腎症の判定方法。 - 被験動物のIgA腎症の疾患活動性を判定するためのキットであって、
抗IgA抗体と、IgA腎症マーカータンパク質に対する抗体とを備え、
前記IgA腎症マーカータンパク質は、IgA免疫複合体に含まれているタンパク質であって、IgA腎症罹患者群のIgA免疫複合体に含まれている量が、健常者群のIgA免疫複合体に含まれている量よりも多いタンパク質である、IgA腎症の判定用キット。 - 前記IgA腎症マーカータンパク質が、アルファ1-アンチトリプシン、アポリポプロテインC-1、FHRP1、カテプシンG、SLC13A4、アルファ2-マクログロブリン、ミエロペルオキシダーゼ、C1QB、RhoGAP42、及びC1QCからなる群より選択される1種以上である、請求項10に記載のIgA腎症の判定用キット。
Priority Applications (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| CN202480027514.8A CN121013988A (zh) | 2023-04-26 | 2024-04-26 | IgA肾病的判定方法 |
| KR1020257035465A KR20250172593A (ko) | 2023-04-26 | 2024-04-26 | IgA 신병증의 판정 방법 |
| JP2025516934A JPWO2024225457A1 (ja) | 2023-04-26 | 2024-04-26 | |
| EP24797200.3A EP4703729A1 (en) | 2023-04-26 | 2024-04-26 | Method for determining iga nephropathy |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2023-072454 | 2023-04-26 | ||
| JP2023072454 | 2023-04-26 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2024225457A1 true WO2024225457A1 (ja) | 2024-10-31 |
Family
ID=93256861
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2024/016523 Ceased WO2024225457A1 (ja) | 2023-04-26 | 2024-04-26 | IgA腎症の判定方法 |
Country Status (5)
| Country | Link |
|---|---|
| EP (1) | EP4703729A1 (ja) |
| JP (1) | JPWO2024225457A1 (ja) |
| KR (1) | KR20250172593A (ja) |
| CN (1) | CN121013988A (ja) |
| WO (1) | WO2024225457A1 (ja) |
Citations (15)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPS61117456A (ja) * | 1984-11-13 | 1986-06-04 | Sumitomo Seiyaku Kk | IgA腎症診断用試薬 |
| JPH04326062A (ja) * | 1991-04-25 | 1992-11-16 | Green Cross Corp:The | IgA測定用試薬 |
| WO1996005853A1 (en) * | 1994-08-19 | 1996-02-29 | Peptide Therapeutics Limited | TREATMENT OF IgA NEPHROPATHY |
| JP2592121B2 (ja) * | 1987-05-08 | 1997-03-19 | ビオカルブ・エイビー | IgA腎臓病の診断のための方法及びキツト |
| JP2000241431A (ja) * | 1999-02-17 | 2000-09-08 | Nissho Corp | 免疫グロブリンa−フィブロネクチン複合体の免疫学的測定試薬および測定法 |
| JP2004061357A (ja) * | 2002-07-30 | 2004-02-26 | Fuso Pharmaceutical Industries Ltd | IgA腎症治療薬のスクリーニング方法 |
| JP2007010540A (ja) * | 2005-07-01 | 2007-01-18 | Univ Nagoya | IgA腎症関連抗体の検出法 |
| WO2009147998A1 (ja) * | 2008-06-02 | 2009-12-10 | エーザイ・アール・アンド・ディー・マネジメント株式会社 | IgA腎症の検査方法及び検査キット |
| WO2009147999A1 (ja) * | 2008-06-02 | 2009-12-10 | エーザイ・アール・アンド・ディー・マネジメント株式会社 | IgA腎症の検査方法及び検査キット |
| JP4636225B2 (ja) * | 2002-11-30 | 2011-02-23 | 司甫 横山 | 検査試薬キット |
| US20110236913A1 (en) * | 2008-10-01 | 2011-09-29 | Kyungpook National University Industry-Academic Cooperation Foundation | Compostion and kit for diagnosing immunoglobulin a nephropathy and tgbm nephropathy |
| WO2019098328A1 (ja) * | 2017-11-17 | 2019-05-23 | 学校法人帝京大学 | IgA腎症診断用キット |
| WO2021152371A1 (en) * | 2020-01-31 | 2021-08-05 | Warszawski Uniwersytet Medyczny | Method of differentiating of a chronic kidney disease or glomerulopathy, method of monitoring a response to treatment of a chronic kidney disease or glomerulopathy in a subject and a method of treatment of a chronic kidney disease or glomerulopathy |
| WO2022124219A1 (ja) * | 2020-12-07 | 2022-06-16 | 学校法人順天堂 | IgA腎症に関連する自己抗体 |
| JP2023072454A (ja) | 2021-11-12 | 2023-05-24 | トヨタ自動車株式会社 | 車両用表示装置、車両、車両用表示システム、車両用表示方法及びプログラム |
-
2024
- 2024-04-26 KR KR1020257035465A patent/KR20250172593A/ko active Pending
- 2024-04-26 EP EP24797200.3A patent/EP4703729A1/en active Pending
- 2024-04-26 WO PCT/JP2024/016523 patent/WO2024225457A1/ja not_active Ceased
- 2024-04-26 CN CN202480027514.8A patent/CN121013988A/zh active Pending
- 2024-04-26 JP JP2025516934A patent/JPWO2024225457A1/ja active Pending
Patent Citations (15)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPS61117456A (ja) * | 1984-11-13 | 1986-06-04 | Sumitomo Seiyaku Kk | IgA腎症診断用試薬 |
| JP2592121B2 (ja) * | 1987-05-08 | 1997-03-19 | ビオカルブ・エイビー | IgA腎臓病の診断のための方法及びキツト |
| JPH04326062A (ja) * | 1991-04-25 | 1992-11-16 | Green Cross Corp:The | IgA測定用試薬 |
| WO1996005853A1 (en) * | 1994-08-19 | 1996-02-29 | Peptide Therapeutics Limited | TREATMENT OF IgA NEPHROPATHY |
| JP2000241431A (ja) * | 1999-02-17 | 2000-09-08 | Nissho Corp | 免疫グロブリンa−フィブロネクチン複合体の免疫学的測定試薬および測定法 |
| JP2004061357A (ja) * | 2002-07-30 | 2004-02-26 | Fuso Pharmaceutical Industries Ltd | IgA腎症治療薬のスクリーニング方法 |
| JP4636225B2 (ja) * | 2002-11-30 | 2011-02-23 | 司甫 横山 | 検査試薬キット |
| JP2007010540A (ja) * | 2005-07-01 | 2007-01-18 | Univ Nagoya | IgA腎症関連抗体の検出法 |
| WO2009147998A1 (ja) * | 2008-06-02 | 2009-12-10 | エーザイ・アール・アンド・ディー・マネジメント株式会社 | IgA腎症の検査方法及び検査キット |
| WO2009147999A1 (ja) * | 2008-06-02 | 2009-12-10 | エーザイ・アール・アンド・ディー・マネジメント株式会社 | IgA腎症の検査方法及び検査キット |
| US20110236913A1 (en) * | 2008-10-01 | 2011-09-29 | Kyungpook National University Industry-Academic Cooperation Foundation | Compostion and kit for diagnosing immunoglobulin a nephropathy and tgbm nephropathy |
| WO2019098328A1 (ja) * | 2017-11-17 | 2019-05-23 | 学校法人帝京大学 | IgA腎症診断用キット |
| WO2021152371A1 (en) * | 2020-01-31 | 2021-08-05 | Warszawski Uniwersytet Medyczny | Method of differentiating of a chronic kidney disease or glomerulopathy, method of monitoring a response to treatment of a chronic kidney disease or glomerulopathy in a subject and a method of treatment of a chronic kidney disease or glomerulopathy |
| WO2022124219A1 (ja) * | 2020-12-07 | 2022-06-16 | 学校法人順天堂 | IgA腎症に関連する自己抗体 |
| JP2023072454A (ja) | 2021-11-12 | 2023-05-24 | トヨタ自動車株式会社 | 車両用表示装置、車両、車両用表示システム、車両用表示方法及びプログラム |
Non-Patent Citations (7)
| Title |
|---|
| CEDERHOLM BO, WIESLANDER JORGEN, HEINEGARDT DICK: "Circulating complexes containing IgA and fibronectin in patients with primary IgA nephropathy (collagen/Berger disease)", PROCEEDINGS OF THE NATIONAL ACADEMY OF SCIENCES OF THE UNITED STATES OF AMERICA, vol. 85, no. 13, 1 July 1988 (1988-07-01), pages 4865 - 4868, XP093227834 * |
| CHOWDHURY, B. ZHANG, Z. MUKHERJEE, A.B.: "Uteroglobin interacts with the heparin-binding site of fibronectin and prevents fibronectin-IgA complex formation found in IgA-nephropathy", FEBS LETTERS, ELSEVIER, AMSTERDAM., NL, vol. 582, no. 5, 1 February 2008 (2008-02-01), NL , pages 611 - 615, XP022495793, ISSN: 0014-5793, DOI: 10.1016/j.febslet.2008.01.025 * |
| FENG ZHENG , GOPAL C. KUNDU, ZHONGJIAN ZHANG, JERROLD WARD, FRANCESCO DEMAYO, ANIL B. MUKHERJEE: "Uteroglobin is essential in preventing immunoglobulin A nephropathy in mice", NATURE MEDICINE, vol. 5, no. 9, 1 September 1999 (1999-09-01), pages 1018 - 1025, XP093227838 * |
| MATOUSOVIC KAREL, NOVAK JAN, YANAGIHARA TAKESHI, TOMANA MILAN, MOLDOVEANU ZINA, KULHAVY ROSE, JULIAN BRUCE A., KONECNY KAREL, MEST: "IgA-containing immune complexes in the urine of IgA nephropathy patients", NEPHROLOGY DIALYSIS TRANSPLANTATION, OXFORD UNIVERSITY PRESS, GB, vol. 21, no. 9, 1 September 2006 (2006-09-01), GB , pages 2478 - 2484, XP093227835, ISSN: 0931-0509, DOI: 10.1093/ndt/gfl240 * |
| MEDJERAL-THOMAS ET AL., KIDNEY INTERNATIONAL, vol. 92, no. 4, 2017, pages 942 - 952 |
| NIHEI YOSHIHITO, HANIUDA KEI, HIGASHIYAMA MIZUKI, ASAMI SHOHEI, IWASAKI HIROYUKI, FUKAO YUSUKE, NAKAYAMA MAIKO, SUZUKI HITOSHI, KI: "Identification of IgA autoantibodies targeting mesangial cells redefines the pathogenesis of IgA nephropathy", SCIENCE ADVANCES, AMERICAN ASSOCIATION FOR THE ADVANCEMENT OF SCIENCE, US, vol. 9, no. 12, 24 March 2023 (2023-03-24), US , XP093227832, ISSN: 2375-2548, DOI: 10.1126/sciadv.add6734 * |
| See also references of EP4703729A1 |
Also Published As
| Publication number | Publication date |
|---|---|
| CN121013988A (zh) | 2025-11-25 |
| KR20250172593A (ko) | 2025-12-09 |
| EP4703729A1 (en) | 2026-03-04 |
| JPWO2024225457A1 (ja) | 2024-10-31 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| EP2310861B1 (en) | Healthy kidney biomarkers | |
| RU2765212C2 (ru) | Гистоны и/или proadm в качестве маркеров, свидетельствующих о неблагоприятном событии | |
| EP3497450B1 (en) | Histones and/or proadm as markers indicating organ dysfunction | |
| JP4516124B2 (ja) | 肝線維症の診断方法 | |
| US20190170770A1 (en) | Diagnostic Test to Exclude Significant Renal Injury | |
| US12174201B2 (en) | Prognosis and progression biomarkers for chronic kidney disease | |
| TWI822802B (zh) | 腎病變蛋白生物標記及其應用 | |
| EP3012634B1 (en) | Biomarker for rheumatoid arthritis diagnosis or activity evaluation | |
| Elnokeety et al. | Cell cycle arrest biomarkers for the early detection of acute allograft dysfunction and acute rejection in living donor kidney transplantation: A cross-sectional study from Egypt | |
| EP4703729A1 (en) | Method for determining iga nephropathy | |
| JP7307479B2 (ja) | IgA腎症診断用キット | |
| JP2007163151A (ja) | 対象生物の生理状態を判定する方法 | |
| US20180275135A1 (en) | Biomarker panel to identify steroid resistance in childhood idiopathic nephrotic syndrome | |
| CN118897083A (zh) | 尿液mt蛋白及其多肽片段在痛风中的应用 | |
| CN117836629A (zh) | 用于检测肾小管间质损伤的生物标志物及其用途 | |
| CN112147329A (zh) | Atp柠檬酸裂解酶作为脓毒症诊断标志物的用途 | |
| WO2017067821A1 (en) | A method for determining presence or risk of hemostasis disorder | |
| Class et al. | Patent application title: DIAGNOSTIC TEST TO EXCLUDE SIGNIFICANT RENAL INJURY Inventors: Lars Otto Uttenthal (Salamanca, ES) Antibodyshop A/s (Gentofte, DE) Kristian Bangert (Holte, DE) Assignees: AntibodyShop A/S | |
| HK40006968A (en) | Histones and/or proadm as markers indicating an adverse event | |
| HK40006968B (en) | Histones and/or proadm as markers indicating an adverse event |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 24797200 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 2025516934 Country of ref document: JP Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2025516934 Country of ref document: JP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: CN2024800275148 Country of ref document: CN |
|
| ENP | Entry into the national phase |
Ref document number: 1020257035465 Country of ref document: KR Free format text: ST27 STATUS EVENT CODE: A-0-1-A10-A15-NAP-PA0105 (AS PROVIDED BY THE NATIONAL OFFICE) |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2024797200 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2024797200 Country of ref document: EP Effective date: 20251126 |
|
| ENP | Entry into the national phase |
Ref document number: 2024797200 Country of ref document: EP Effective date: 20251126 |
|
| ENP | Entry into the national phase |
Ref document number: 2024797200 Country of ref document: EP Effective date: 20251126 |
|
| ENP | Entry into the national phase |
Ref document number: 2024797200 Country of ref document: EP Effective date: 20251126 |
|
| ENP | Entry into the national phase |
Ref document number: 2024797200 Country of ref document: EP Effective date: 20251126 |
|
| ENP | Entry into the national phase |
Ref document number: 2024797200 Country of ref document: EP Effective date: 20251126 |
|
| ENP | Entry into the national phase |
Ref document number: 2024797200 Country of ref document: EP Effective date: 20251126 |
|
| ENP | Entry into the national phase |
Ref document number: 2024797200 Country of ref document: EP Effective date: 20251126 |
|
| ENP | Entry into the national phase |
Ref document number: 2024797200 Country of ref document: EP Effective date: 20251126 |
|
| WWP | Wipo information: published in national office |
Ref document number: 2024797200 Country of ref document: EP |