EP4091607A1 - Procédés de traitement de troubles du système nerveux central par l'activateur du récepteur muscarinique xanoméline et des antipsychotiques - Google Patents
Procédés de traitement de troubles du système nerveux central par l'activateur du récepteur muscarinique xanoméline et des antipsychotiques Download PDFInfo
- Publication number
- EP4091607A1 EP4091607A1 EP21206327.5A EP21206327A EP4091607A1 EP 4091607 A1 EP4091607 A1 EP 4091607A1 EP 21206327 A EP21206327 A EP 21206327A EP 4091607 A1 EP4091607 A1 EP 4091607A1
- Authority
- EP
- European Patent Office
- Prior art keywords
- salt
- xanomeline
- trospium
- composition
- antipsychotic
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Pending
Links
Images








Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/04—Centrally acting analgesics, e.g. opioids
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/13—Amines
- A61K31/135—Amines having aromatic rings, e.g. ketamine, nortriptyline
- A61K31/137—Arylalkylamines, e.g. amphetamine, epinephrine, salbutamol, ephedrine or methadone
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/21—Esters, e.g. nitroglycerine, selenocyanates
- A61K31/215—Esters, e.g. nitroglycerine, selenocyanates of carboxylic acids
- A61K31/22—Esters, e.g. nitroglycerine, selenocyanates of carboxylic acids of acyclic acids, e.g. pravastatin
- A61K31/222—Esters, e.g. nitroglycerine, selenocyanates of carboxylic acids of acyclic acids, e.g. pravastatin with compounds having aromatic groups, e.g. dipivefrine, ibopamine
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/40—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having five-membered rings with one nitrogen as the only ring hetero atom, e.g. sulpiride, succinimide, tolmetin, buflomedil
- A61K31/4025—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having five-membered rings with one nitrogen as the only ring hetero atom, e.g. sulpiride, succinimide, tolmetin, buflomedil not condensed and containing further heterocyclic rings, e.g. cromakalim
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/435—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with one nitrogen as the only ring hetero atom
- A61K31/44—Non condensed pyridines; Hydrogenated derivatives thereof
- A61K31/4427—Non condensed pyridines; Hydrogenated derivatives thereof containing further heterocyclic ring systems
- A61K31/4439—Non condensed pyridines; Hydrogenated derivatives thereof containing further heterocyclic ring systems containing a five-membered ring with nitrogen as a ring hetero atom, e.g. omeprazole
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/435—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with one nitrogen as the only ring hetero atom
- A61K31/46—8-Azabicyclo [3.2.1] octane; Derivatives thereof, e.g. atropine, cocaine
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/435—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with one nitrogen as the only ring hetero atom
- A61K31/47—Quinolines; Isoquinolines
- A61K31/472—Non-condensed isoquinolines, e.g. papaverine
- A61K31/4725—Non-condensed isoquinolines, e.g. papaverine containing further heterocyclic rings
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/495—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with two or more nitrogen atoms as the only ring heteroatoms, e.g. piperazine or tetrazines
- A61K31/496—Non-condensed piperazines containing further heterocyclic rings, e.g. rifampin, thiothixene or sparfloxacin
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/495—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with two or more nitrogen atoms as the only ring heteroatoms, e.g. piperazine or tetrazines
- A61K31/505—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim
- A61K31/519—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim ortho- or peri-condensed with heterocyclic rings
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/55—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole
- A61K31/551—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole having two nitrogen atoms, e.g. dilazep
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/55—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole
- A61K31/551—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole having two nitrogen atoms, e.g. dilazep
- A61K31/5513—1,4-Benzodiazepines, e.g. diazepam or clozapine
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/55—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole
- A61K31/554—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole having at least one nitrogen and one sulfur as ring hetero atoms, e.g. clothiapine, diltiazem
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/14—Drugs for disorders of the nervous system for treating abnormal movements, e.g. chorea, dyskinesia
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/14—Drugs for disorders of the nervous system for treating abnormal movements, e.g. chorea, dyskinesia
- A61P25/16—Anti-Parkinson drugs
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/18—Antipsychotics, i.e. neuroleptics; Drugs for mania or schizophrenia
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/24—Antidepressants
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/28—Drugs for disorders of the nervous system for treating neurodegenerative disorders of the central nervous system, e.g. nootropic agents, cognition enhancers, drugs for treating Alzheimer's disease or other forms of dementia
Definitions
- Schizophrenia and various mood disorders are thought to be caused by an excess of dopaminergic D2 and serotonergic 5-HT2A activity, resulting in overactivity of central mesolimbic pathways and mesocortical pathways, respectively.
- All currently approved antipsychotic drugs sometimes referred to as neuroleptics or major tranquilizers, work primarily by binding to and blocking dopamine D2 receptors.
- Antipsychotic medications have both a short-term sedative effect and the long-term effect of reducing the chances of psychotic episodes.
- Atypical antipsychotics such as risperidone, olanzapine, quetiapine, and aripiprazole, are currently the first-line agents in patients with psychotic symptoms of dementia. Nevertheless, these drugs exert detrimental effects and provide limited efficacy, such as excessive sedation, orthostatic hypotension, and related complications such as falls, extrapyramidal symptoms, cognitive slowing, cardiovascular complications, and anticholinergic side effects. Pertaining to the atypical antipsychotics, weight gain and metabolic dysfunction are prominent side-effects.
- Xanomeline an M1/M4 preferring muscarinic receptor agonist
- peripherally-mediated muscarinic agonist adverse events prevented its further development.
- a co-formulation of xanomeline together with the peripherally-restricted muscarinic antagonist trospium identified as KarXT was reported to be well-tolerated and efficacious in treating acute psychosis in patients with schizophrenia.
- Activating the muscarinic system through muscarinic agonists may treat several diseases, such as dementia-related psychosis, schizophrenia, Alzheimer's disease, Parkinson's disease, depression, movement disorders, drug addiction, pain, and other neurodegenerative disorders, such as tauopathies or synucleinopathies.
- Muscarinic cholinergic receptors are G-protein coupled receptors with five different receptor subtypes (M1-M5), each of which is found in the CNS with different tissue distributions. M1 and M4 subtypes have been of interest as therapeutic targets for various diseases. Genetic evidence directly links the muscarinic system to alcohol addiction and schizophrenia.
- central nervous system disorder including schizophrenia and its related symptoms, such as dementia, psychosis, agitation, and irritability, especially without the side effects associated with dopamine antagonism and off-target muscarinic activation.
- compositions and methods which are meant to be exemplary and illustrative, not limiting in scope.
- one or more of the above-described problems have been reduced or eliminated, while other embodiments are directed to other improvements.
- the present disclosure provides a method of treating a central nervous system disorder in a patient in need thereof, the method comprising administering a synergistic combination of a composition comprising xanomeline and/or a salt thereof and a composition comprising an antipsychotic.
- the present disclosure further provides a method of treating schizophrenia in a patient in need thereof, the method comprising administering a synergistic combination of a composition comprising xanomeline and/or a salt thereof and a composition comprising risperidone or aripiprazole.
- the present disclosure further provides a method of treating a central nervous system disorder in a patient in need thereof, the method comprising co-administering a first composition comprising xanomeline and/or a salt thereof and a composition comprising an antipsychotic, for example, wherein the first composition or the second composition or both are co-administered in a reduced amount compared to the first composition or the second composition used alone, such as in a subthreshold amount or in a lower dose.
- the first composition further comprises trospium chloride.
- the second composition comprises aripiprazole or risperidone.
- the present disclosure provides a method of treating a central nervous system disorder in a patient in need thereof.
- the method comprises administering a synergistic combination of a composition comprising xanomeline and/or a salt thereof and a composition comprising an antipsychotic.
- a method comprising administering a synergistic combination of a first composition comprising xanomeline and/or a salt thereof and trospium chloride, and a second composition comprising an antipsychotic.
- “Synergy” refers to the interaction or cooperation of two or more drugs that produce a combined effect in a subject that is greater than the sum of their separate effects in that subject. Synergy is more than merely additive, and it is greater than augmentation relative to any of the individual drugs. For example, if Drug A produces an effect of 2 units and Drug B produces an effect of 2 units, an augmented result is an effect of at least 3 units; an additive result is an effect equal to 4 units. A synergistic effect is greater than 4 units, the upper boundary of which is inherently unpredictable and only discernable through experimentation. An augmented result includes additive results and synergistic effects.
- Xanomeline and atypical antipsychotics target different receptor families; therefore, there is the potential for greater therapeutic benefit with adjunctive treatment.
- the administration of xanomeline with the atypical antipsychotic risperidone was investigated in mouse models predictive of antipsychotic activity to determine the potential for greater therapeutic benefit with adjunctive treatment.
- the efficacy of xanomeline is augmented by the antipsychotic, such as risperidone and aripiprazole.
- the combined does of xanomeline and the antipsychotic significantly augmented the effect sizes of that observed for each agent alone, where the combined effect was statistically significant and more than additive.
- the adjunctive treatment with xanomeline and an antipsychotic provides greater therapeutic benefit to the patient in need thereof.
- antipsychotic refers to a drug that diminishes psychosis, hallucinations, or delusions.
- Antipsychotics include, but are not limited to haloperidol, droperidol, chlorpromazine, fluphenazine, perphenazine, prochlorperazine, thioridazine, trifluoperazine, mesoridazine, periciazine, promazine, triflupromazine, levomepromazine, promethazine, pimozide, chlorprothixene, flupentixol, thiothixene, zuclopenthixol, clozapine, olanzapine, risperidone, quetiapine, ziprasidone, amisulpride, asenapine, paliperidone, zotepine, aripiprazole, bifeprunox, and tetrabenazine.
- First-generation antipsychotics (“typical antipsychotics") are considered effective for managing the "positive" symptoms of schizophrenia, including hallucinations, hearing voices, aggression/hostility, disorganized speech, and psychomotor agitation.
- this class of drugs e.g. haloperidol and chlorpromazine.
- Potent dopamine-blockade of the D2 receptor induces these movement disorders, including drug-induced parkinsonism, akathisia, dystonia, tardive dyskinesia, and other side effects, such as sedation, weight gain, and prolactin changes.
- Low-potency antipsychotics block many receptors other than the primary target (dopamine receptors), such as cholinergic or histaminergic receptors, resulting in a higher incidence of side effects, such as sedation, weight gain, and hypotension.
- Second-generation antipsychotics also known as atypical antipsychotics, generally have a lower risk of extrapyramidal side effects and tardive dyskinesia than first-generation antipsychotics.
- Typical and atypical antipsychotic drugs are more comparable in their clinical efficacy, except for clozapine, an atypical antipsychotic with unique efficacy in treatment-resistant schizophrenia.
- Antipsychotic drugs differ from one another in dosing, route of administration, pharmacokinetics, side effect profile, and cost, factors that influence how to select an antipsychotic drug for individual patients.
- Typical antipsychotic drugs have largely been replaced with atypical antipsychotics, such as risperidone, olanzapine, clozapine, quetiapine, aripiprazole, and ziprasidone.
- Aripiprazole (Abilify TM ) is an atypical antipsychotic orally indicated for treating schizophrenia, bipolar I, major depressive disorder, irritability associated with autism, and Tourette's syndrome. It is also indicated as an injection for agitation associated with schizophrenia or bipolar mania. Aripiprazole exerts its effects through partial agonism of dopamine and 5-HT1A receptors and antagonism of alpha-adrenergic and 5-HT2A receptors. The dosing for aripiprazole approved by the US Food and Drug Administration (FDA) is shown in Table 1. Oral formulations are administered once daily without regard to meals.
- FDA US Food and Drug Administration
- Chlorpromazine (Thoraxine TM ) is a prototypical phenothiazine antipsychotic drug.
- the FDA-approved oral dosing for chlorpromazine for schizophrenia, psychoses, anxiety, and agitation is, to begin with, 25 mg three times daily or 75 mg at bedtime, increasing by daily amounts of 25 mg to an effective maintenance dose.
- the effective dose is usually between 75 and 300 mg daily, but some patients may require up to 1 g daily.
- Children under one year old should not use chlorpromazine unless it is lifesaving.
- Patients 1-5 years old should begin with 0.5 mg/kg bodyweight every 4-6 hours to a maximum recommended dose of 40 mg daily.
- Patients 6-12 years old should use a third to half of the adult dose to a maximum recommended dose of 75 mg daily.
- the elderly should start with a third to a half the usual adult dose with a more gradual increase in dosage.
- Intramuscular dosing in adults for acute relief of symptoms should be 25-50 mg every 6-8 hours. Patients 1-5 years old should dose at 0.5 mg/kg bodyweight every 6-8 hours, not to exceed 40 mg daily. Patients 6-12 years old should do at 0.5 mg/kg bodyweight every 6-8 hours, not to exceed 75 mg daily. For the elderly, doses in the lower range for adults should be sufficient to control symptoms, for example, 25 mg every 8 hours.
- Clozapine (Clozaril TM , Fazaclo TM , Versacloz TM ) is a tricyclic dibenzodiazepine, classified as an atypical antipsychotic.
- the FDA-approved dosing for clozapine is 12.5 mg once or twice daily and then be continued with daily dosage increments of 25-50 mg/day, if well-tolerated, to achieve a target dose of 300-450 mg/day by the end of two weeks. Subsequent dosage increments should be made no more than once or twice weekly, in increments not to exceed 100 mg.
- Flupentixol (Depixol TM , Fluanxol TM ) is an antipsychotic drug of the thioxanthene group.
- Flupentixol oral tablets are available at doses of 0.5 mg, 3 mg, and 5 mg.
- the dosage of flupentixol tablets should be individualized and adjusted according to the severity of symptoms and tolerance to the drug.
- the maintenance dose can usually be given as a single morning dose.
- Fluphenazine is a phenothiazine used to treat psychoses. Fluphenazine Decanoate Injection, USP is available as a clear, pale yellow solution for intramuscular (IM) or subcutaneous (SC, SQ) use providing 25 mg fluphenazine decanoate per mL in a sesame oil vehicle with 12 mg benzyl alcohol as a preservative. For most patients, a dose of 12.5 to 25 mg (0.5 to 1 mL) may initiate therapy.
- IM intramuscular
- SC, SQ subcutaneous
- Haloperidol is a highly potent typical antipsychotic and one of the most frequently used antipsychotic medications worldwide.
- the initial dosage for oral haloperidol in adults with moderate symptoms is 0.5 mg to 2 mg b.i.d. or t.i.d. and with severe symptoms 3 mg to 5 mg b.i.d. or t.i.d.
- higher doses may be required in some cases.
- the recommended doses for geriatric or debilitated patients is 0.5 mg to 2 mg b.i.d. or t.i.d.
- For chronic or resistant patients is 3 mg to 5 mg b.i.d. or t.i.d.
- Patients who remain severely disturbed or inadequately controlled may require dosage adjustment.
- Daily dosages up to 100 mg may be necessary in some cases for a response.
- oral haloperidol should begin at the lowest dose possible (0.5 mg per day). If required, the dose should be increased by 0.5 mg at 5 to 7-day intervals until the desired therapeutic effect is obtained.
- the total dose may be divided, to be given b.i.d. or t.i.d.
- the dosage for psychotic disorders is 0.05 mg/kg/day to 0.15 mg/kg/day.
- the recommended dosage is 0.05 mg/kg/day to 0.075 mg/kg/day.
- Haloperidol is available as a sterile parenteral form for intramuscular injection.
- the injection provides 5 mg haloperidol (lactate) and lactic acid for pH adjustment between 3.0-3.6.
- haloperidol decanoate is recommended to be 10-15 times the previous daily dose in oral haloperidol equivalents.
- Olanzapine (Zyprexa TM ) is a thienobenzodiazepine classified as an atypical antipsychotic. Recommended dosing is shown in Table 2. Table 2 - Recommended dosing of Olanzapine Indication Dosing Schizophrenia in adults Oral: Start at 5-10 mg once daily; Target: 10 mg/day within several days Schizophrenia in adolescents Oral: Start at 2.5-5 mg once daily; Target: 10 mg/day Bipolar I Disorder (manic or mixed episodes) in adults Oral: Start at 10 or 15 mg once daily Bipolar I Disorder (manic or mixed episodes) in adolescents Oral: Start at 2.5-5 mg once daily; Target: 10 mg/day Bipolar I Disorder (manic or mixed episodes) with lithium or valproate in adults Oral: Start at 10 mg once daily Agitation associated with Schizophrenia and Bipolar I Mania in adults IM: 10 mg (5 mg or 7.5 mg when clinically warranted) Assess for orthostatic hypotension before subsequent dosing (max.
- Depressive Episodes associated with Bipolar I Disorder in adults Oral in combination with fluoxetine Start at 5 mg of oral olanzapine and 20 mg of fluoxetine once daily Depressive Episodes associated with Bipolar I Disorder in children and adolescents Oral in combination with fluoxetine: Start at 2.5 mg of oral olanzapine and 20 mg of fluoxetine once daily Treatment-Resistant Depression in adults Oral in combination with fluoxetine: Start at 5 mg of oral olanzapine and 20 mg of fluoxetine once daily
- the lower starting dose is recommended in debilitated or pharmacodynamically sensitive patients, patients with a predisposition to hypotensive reactions, or with the potential for slowed metabolism.
- Quetiapine (Seroquel TM ) is an atypical antipsychotic used to treat schizophrenia, major depression, and bipolar disorder. Recommended doses are shown in Table 3. Table 3 - Recommended doses for quetiapine Indication Initial Dose Recommended Dose Maximum Dose Schizophrenia-Adults 25 mg twice daily 150-750 mg/day 750 mg/day Schizophrenia-Adolescents (13-17 years) 25 mg twice daily 400-800 mg/day 800 mg/day Bipolar Mania-Adults Monotherapy or as an adjunct to lithium or divalproex 50 mg twice daily 400- 800 mg/day 800 mg/day Bipolar Mania-Children and Adolescents (10 to 17 years), Monotherapy 25 mg twice daily 400-600 mg/day 600 mg/day Bipolar Depression-Adults 50 mg once daily at bedtime 300 mg/day 300 mg/day
- Risperidone (Perseris TM , Risperdal TM ) is an atypical antipsychotic medication for treating several mood and mental health conditions, including schizophrenia and bipolar disorder. Another commonly used atypical antipsychotic is paliperidone, the primary active metabolite of risperidone (i.e., 9-hydroxyrisperidone). Recommended dosing is shown in Table 4.
- Methods of treatment comprising a synergistic combination of two agents, such as a synergistic combination of xanomeline or a salt thereof and an antipsychotic, typically use lower dosages of one or both agents in the synergistic combination.
- the dose for the xanomeline or the antipsychotic or both is reduced compared to what the patient would receive for each agent alone.
- the doses of one agent or both agents can be reduced by such as by at least 10%, at least 20%, at least 30%, at least 40%, at least 50%, at least 60%, at least 70%, at least 80%, or at least 90%. These lower doses reduce toxicity and harmful side effects.
- synergistic combinations of xanomeline or a salt thereof and an antipsychotic provide superior safety and efficacy than monotherapies or combinations of therapies that do not act synergistically.
- the combinations of xanomeline with an antipsychotic offer several advantages.
- the therapeutically effective dose of each can be lowered, thus avoiding side effects from each the xanomeline and the antipsychotic.
- the combination provides the advantage of achieving efficacy at a subthreshold dose.
- the combination provides the advantage of greater tolerability.
- the combination provides the advantage of fewer side effects.
- the ratio of xanomeline to antipsychotic is between 3:1 and 1:3, such as 3:1, 2:1, 1:1, 1:2, or 1:3. In certain embodiments, the ratio of xanomeline to antipsychotic is 3:1. In certain embodiments, the ratio of xanomeline to antipsychotic is 1:1. In certain embodiments, the ratio of xanomeline to antipsychotic is 1:3. In certain embodiments, the ratio of xanomeline to antipsychotic is between 1:0.03 and 1:0.3, such as between 1:0.03 and 1:0.05, between 1:0.05 and 1:0.1, between 1:0.1 and 1:0.2, or between 1:0.2 and 1:0.3. In certain embodiments, the ratio of xanomeline to antipsychotic is 1:0.03. In certain embodiments, the ratio of xanomeline to antipsychotic is 1:0.1. In certain embodiments, the ratio of xanomeline to antipsychotic is 1:0.3.
- the ratio of xanomeline to aripiprazole is between 3:1 and 1:3, such as 3:1, 2:1, 1:1, 1:2, or 1:3. In certain embodiments, the ratio of xanomeline to aripiprazole is 3:1. In certain embodiments, the ratio of xanomeline to aripiprazole is 1:1. In certain embodiments, the ratio of xanomeline to aripiprazole is 1:3. In certain embodiments, the ratio of xanomeline to aripiprazole is between 1:0.03 and 1:0.3, such as between 1:0.03 and 1:0.05, between 1:0.05 and 1:0.1, between 1:0.1 and 1:0.2, or between 1:0.2 and 1:0.3.
- the ratio of xanomeline to aripiprazole is 1:0.03. In certain embodiments, the ratio of xanomeline to aripiprazole is 1:0.1. In certain embodiments, the ratio of xanomeline to aripiprazole is 1:0.3.
- the ratio of xanomeline to risperidone is 1:3. In certain embodiments, the ratio of xanomeline to risperidone is between 1:0.03 and 1:0.3, such as between 1:0.03 and 1:0.05, between 1:0.05 and 1:0.1, between 1:0.1 and 1:0.2, or between 1:0.2 and 1:0.3. In certain embodiments, the ratio of xanomeline to risperidone is 1:0.03. In certain embodiments, the ratio of xanomeline to risperidone is 1:0.1. In certain embodiments, the ratio of xanomeline to risperidone is 1:0.3.
- the xanomeline and antipsychotic were co-administered on a per weight basis of mg/kg/day.
- the average body mass, globally, is 136 pounds (62 kg). In North America, which has the highest average body mass of any continent, the number is 178 pounds (80.7 kg). Based on these numbers, one of skill in the art can convert the daily mg/kg dosing to total daily doses in mg and select available drug products for dosing.
- Table 5 based on the method from Reagan-Shaw et al., The FASEB Journal, 22(3), 659-661 .
- mice Converted to dosage in humans For 60-kg patient For 80-kg patient 0.03 mg/kg 0.0024 mg/kg 0.14 mg 0.19 mg 0.10 mg/kg 0.0081 mg/kg 0.49 mg 0.64 mg 0.30 mg/kg 0.024 mg/kg 1.5 mg 1.9 mg 1.0 mg/kg 0.081 mg/kg 4.9 mg 6.5 mg 3.0 mg/kg 0.24 mg/kg 15mg 19 mg
- xanomeline was tested at 1 mg/kg/day in mice, which corresponds to 0.081 mg/kg for humans (4.9-6.5 mg per day) or 3 mg/kg/day in mice which (15-19 mg per day).
- the amounts of xanomeline tested in the clinic without an antipsychotic are between 25 and 225 mg per day, what are far higher than in the present examples.
- Risperidone was tested at 0.03-0.3 mg/kg/day (0.14-1.9 mg).
- the effective dose range for monotherapy is 4-16 mg per day.
- Aripiprazole was tested over a wider range, including dosing of 0.1-0.3 mg/kg/day (0.14-1.9 mg).
- the recommended daily dose of aripiprazole monotherapy is 10-15 mg and the maximum daily dose of 30 mg.
- a synergistic amount of the composition comprising xanomeline and/or a salt thereof and the composition comprising an antipsychotic is a specific concentration of the composition comprising xanomeline and/or a salt thereof and the composition comprising the antipsychotic. In some embodiments, a synergistic amount of the composition comprising xanomeline and/or a salt thereof and the composition comprising the antipsychotic is a specific ratio of the composition comprising xanomeline and/or a salt thereof to the composition comprising the antipsychotic.
- co-administer and “co-administration” and variants thereof mean the administration of at least two drugs to a patient either subsequently, simultaneously, or consequently proximate in time to one another (e.g., within the same day, or week or period of 30 days, or sufficiently proximate that each of the at least two drugs can be simultaneously detected in the blood plasma).
- two or more active agents can be co-formulated as part of the same composition or administered as separate formulations. This also may be referred to herein as "concomitant" administration or variants thereof.
- the synergistic effect of the composition comprising xanomeline and/or a salt thereof and the composition comprising an antipsychotic may include, but is not limited to an effect of treating a central nervous system disorder, e.g., by reduced dementia, psychosis, agitation, irritability, a change from Baseline in Positive and Negative Syndrome Scale (PANSS) Total Score or Positive Score or Negative Score, the number of participants with each Clinical Global Impression - Severity (CGI-S) Score at baseline, change from baseline in the PANSS Marder Factor Score, and the percentage of participants who were CGI-S responders.
- a central nervous system disorder e.g., by reduced dementia, psychosis, agitation, irritability
- PANSS Positive and Negative Syndrome Scale
- CGI-S Clinical Global Impression - Severity
- the composition comprising xanomeline and/or a salt thereof further comprises an anticholinergic agent.
- the anticholinergic agent is a muscarinic antagonist.
- the muscarinic antagonist is chosen from trospium, tolterodine, darifenacin, solifenacin, fesoterodine, scopolamine, N-methylscopolamine, and a salt thereof.
- the muscarinic agonist is trospium chloride.
- xanomeline combined with trospium chloride and an antipsychotic treats an animal.
- the animal is a mammal.
- the mammal is a human being.
- trospium chloride decreases the side effects associated with xanomeline.
- side effects include, but are not limited to, GI side effects, cardiac side effects, excessive sweating, and excessive salivation.
- the use of trospium with xanomeline allows the xanomeline to be used clinically when the xanomeline would not otherwise be used clinically due to its side effects.
- the use of trospium chloride with the xanomeline allows for the xanomeline to achieve a higher maximum tolerated dose than xanomeline would otherwise achieve, with or without co-administration with a composition comprising an antipsychotic.
- animal models demonstrate the efficacy of new therapeutics for schizophrenia, including pharmacological models (e.g., ketamine model) and genetic models (e.g., DISCI mouse).
- pharmacological models e.g., ketamine model
- genetic models e.g., DISCI mouse
- animal models including rodents, dogs, and non-human primates, demonstrate the side effect profile of pharmacological agents.
- Animal models are an experimental proxy for humans but may suffer from deficiencies in the physiological differences between humans and animals and may have limited predictive power for human experiments, particularly for central nervous system disorders.
- Standard measures based on patient self-report can be used by those skilled in the art to assess various side effects such as GI discomfort.
- objective physiological measures e.g., EKGs
- a set of standard measures has also been developed to assess schizophrenia symptoms, including the Brief Psychiatric Rating Scale (BPRS), the Positive and Negative Syndrome Scale (PANSS), and Clinical Global Impression (CGI).
- BPRS Brief Psychiatric Rating Scale
- PANSS Positive and Negative Syndrome Scale
- CGI Clinical Global Impression
- clinical trials are double-blinded, where one group of patients receives an inactive placebo, and the other group the active intervention.
- the Positive and Negative Syndrome Scale is a medical scale used for measuring symptom severity of patients with schizophrenia.
- the name refers to the two types of symptoms in schizophrenia, as defined by the American Psychiatric Association: positive symptoms, which refer to an excess or distortion of normal functions (e.g., hallucinations and delusions), and negative symptoms, which represent a diminution or loss of normal functions. Some of these functions which may be lost include normal thoughts, actions, the ability to tell sexualies from reality, and the ability to properly express emotions
- the PANSS is a relatively brief interview of about 45 to 50 minutes. The interviewer must be trained to a standardized level of reliability. The patient is rated from 1 to 7 on 30 different symptoms in three categories based on the interview and reports of family members or primary care hospital workers.
- PANSS Marder factor score is the sum of five negative scales and two general scales (N1. Blunted affect; N2. Emotional withdrawal; N3. Poor rapport; N4. Passive/apathetic social withdrawal; N6. Lack of spontaneity; G7. Motor retardation; and G16. Active social avoidance). If a patient has a PANSS assessment recorded, but any of the items are missing, the last non-missing score for the individual item from previous assessments will be carried forward. If more than 30% of the items are missing at a particular visit, the respective positive score is not calculated. It is treated as missing data in the analysis.
- the Positive and Negative Syndrome Scale (PANSS) total score for the subject decreases by at least 10 points than the placebo, for example, after five treatment weeks.
- the PANSS positive subscore decreases by at least 3 points than the placebo, for example, after five treatment weeks.
- the PANSS negative subscore decreases by at least 2 points than the placebo, for example, after five treatment weeks.
- CGI-S Clinical Global Impression - Severity scale
- This 7-point scale requires the clinician to rate the severity of the patient's illness at the time of assessment relative to the clinician's experience with patients who have the same diagnosis. Possible ratings are (1) Normal, not at all ill; (2) Borderline mentally ill; (3) Mildly ill, (4) Moderately ill; (5) Markedly ill; (6) Severely ill, and (7) Among the most extremely ill patients.
- schizophrenia patients changes in the CGI-S follow a consistent pattern relative to more objective PANSS scoring.
- patients Before co-administering the disclosed combinations, patients may have a lead-in period from one to 28 days, during which lead-in period trospium chloride and/or the antipsychotic is given alone.
- the trospium chloride and/or antipsychotic are co-administered for one or more dose periods before co-administering xanomeline to accumulate trospium chloride and/or antipsychotic in the body or for the trospium chloride and/or antipsychotic to reach or approach steady-state exposure levels. This accumulation or higher exposure levels of the trospium chloride increases the blockade of muscarinic receptors outside of the brain and reduces adverse events when xanomeline is administered.
- this accumulation or higher exposure levels to the antipsychotics increase the blockade of D2 receptors and simplifies the process for titrating to the synergistic amount of xanomeline and/or a salt thereof.
- the trospium chloride and/or antipsychotic are co-administered for one or more days before xanomeline.
- the patient was already taking a steady-state dose of an antipsychotic before beginning treatment with KarXT.
- the dose of the antipsychotic may be titrated down to account for its synergistic effect with KarXT.
- the dose of KarXT may be titrated down to account for its synergistic effect with the antipsychotic.
- the total daily dose is 5 mg a salt of trospium.
- the total daily dose is 10 mg a salt of trospium.
- the total daily dose is 15 mg a salt of trospium.
- the total daily dose is 17.5 mg a salt of trospium.
- the total daily dose is 20 mg a salt of trospium.
- the total daily dose is 30 mg a salt of trospium.
- the total daily dose is 25 mg xanomeline and/or the salt thereof.
- the total daily dose is 50 mg xanomeline and/or the salt thereof.
- the total daily dose is 75 mg xanomeline and/or the salt thereof.
- the total daily dose is 100 mg xanomeline and/or the salt thereof.
- the total daily dose is 150 mg xanomeline and/or the salt thereof.
- the total daily dose is 175 mg xanomeline and/or the salt thereof.
- the total daily dose is 200 mg xanomeline and/or the salt thereof.
- the total daily dose is 25 mg xanomeline and/or the salt thereof and 5 mg a salt of trospium.
- the total daily dose is 50 mg xanomeline and/or the salt thereof and 10 mg a salt of trospium.
- the total daily dose is 50 mg xanomeline and/or the salt thereof and 20 mg a salt of trospium.
- the total daily dose is 75 mg xanomeline and/or the salt thereof and 15 mg a salt of trospium.
- the total daily dose is 75 mg xanomeline and/or the salt thereof and 30 mg a salt of trospium.
- the total daily dose is 100 mg xanomeline and/or the salt thereof and 17.5 mg a salt of trospium.
- the total daily dose is 100 mg xanomeline and/or the salt thereof and 20 mg a salt of trospium.
- the total daily dose is 100 mg xanomeline and/or the salt thereof and 40 mg a salt of trospium.
- the total daily dose is 150 mg xanomeline and/or the salt thereof and 20 mg a salt of trospium.
- the total daily dose is 150 mg xanomeline and/or the salt thereof and 30 mg a salt of trospium.
- the total daily dose is 150 mg xanomeline and/or the salt thereof and 40 mg a salt of trospium.
- the total daily dose is 175 mg xanomeline and/or the salt thereof and 30 mg a salt of trospium.
- the total daily dose is 175 mg xanomeline and/or the salt thereof and 40 mg a salt of trospium.
- the total daily dose is 200 mg xanomeline and/or the salt thereof and 30 mg a salt of trospium.
- the total daily dose is 200 mg xanomeline and/or the salt thereof and 40 mg a salt of trospium.
- xanomeline and trospium chloride are administered to a patient 6 times during a 24-hour period. In another embodiment, xanomeline and trospium chloride are administered to a patient 5 times during a 24-hour period. In another embodiment, xanomeline and trospium chloride are administered to a patient 4 times during a 24-hour period. In an embodiment, xanomeline and trospium chloride are administered to a patient 3 times during a 24-hour period. In another embodiment, xanomeline and trospium chloride are administered to a patient twice during a 24-hour period. In another embodiment, xanomeline and trospium chloride are administered to a patient once during a 24-hour period.
- the administration comprises a dosing schedule of 25 mg xanomeline and/or the salt thereof and 5 mg a salt of trospium twice daily.
- the administration comprises a dosing schedule of 25 mg xanomeline and/or the salt thereof and 5 mg a salt of trospium thrice daily.
- the administration comprises a dosing schedule of 25 mg xanomeline and/or the salt thereof and 5 mg a salt of trospium twice daily, and 50 mg xanomeline and/or the salt thereof and 7.5 mg a salt of trospium once daily.
- the administration comprises a dosing schedule of 25 mg xanomeline and/or the salt thereof and 10 mg a salt of trospium twice daily.
- the administration comprises a dosing schedule of 50 mg xanomeline and/or the salt thereof and 7.5 mg a salt of trospium twice daily, and 50 mg xanomeline and/or the salt thereof and 5 mg a salt of trospium once daily.
- the administration comprises a dosing schedule of 50 mg xanomeline and/or the salt thereof and 10 mg a salt of trospium twice daily.
- the administration comprises a dosing schedule of 50 mg xanomeline and/or the salt thereof and 10 mg a salt of trospium thrice daily.
- the administration comprises a dosing schedule of 50 mg xanomeline and/or the salt thereof and 10 mg a salt of trospium twice daily, and 75 mg xanomeline and/or the salt thereof and 10 mg a salt of trospium once daily.
- the administration comprises a dosing schedule of 75 mg xanomeline and/or the salt thereof and 10 mg a salt of trospium twice daily, and 50 mg xanomeline and/or the salt thereof and 10 mg a salt of trospium once daily.
- the low doses are split TID rather than BID.
- BID keeps the trospium dose as low as possible with a minimum amount of 10 mg of trospium per capsule.
- a starting dose of 50/5 mg or 50/7.5 mg xanomeline/trospium is split TID so the individual dose 17/2.5 mg xanomeline/trospium.
- Treatment may be initiated with smaller dosages. After that, small increments may increase the dosage until a balance between therapeutic effect and side effects is attained.
- the patient's health may be monitored by measuring one or more of the relevant indices at predetermined times during the treatment period. Treatment, including composition, amounts, administration, and formulation times, may be adjusted per such monitoring. The patient may be periodically reevaluated to determine improvement by measuring the same parameters. Adjustments to the disclosed composition administered and possibly to the administration time may be made based on these reevaluations.
- the patient has a diagnosis of schizophrenia. In certain embodiments, the patient has acute psychosis. In certain embodiments, the patient has psychosis associated with Alzheimer's disease. In certain embodiments, the patient has a schizo-affective disorder. In certain embodiments, the patient has psychosis. In certain embodiments, the patient has a delusional disorder. In certain embodiments, the patient has psychosis associated with Parkinson's disease. In certain embodiments, the patient has psychotic depression. In certain embodiments, the patient has bipolar disorder. In certain embodiments, the patient has bipolar disorder with psychosis. In certain embodiments, the patient has Huntington's disease. In certain embodiments, the patient has Lewy Body dementia. In certain embodiments, the patient has dementia-related psychosis (DRP).
- DRP dementia-related psychosis
- the patient previously had been administered one or more antipsychotics.
- the patient was an inadequate responder to such administration.
- the patient was treatment-resistant.
- an oral pharmaceutical composition comprising a plurality of xanomeline beads comprising xanomeline or a salt thereof; and a plurality of trospium beads comprising a salt of trospium.
- the salt of trospium is chosen from trospium chloride, trospium bromide, trospium iodide, and trospium saccharinate.
- the therapeutically effective amount of the composition comprising xanomeline and/or a salt thereof comprises a synergistically effective amount of the composition comprising xanomeline and/or a salt thereof.
- the composition comprising xanomeline and/or a salt thereof and the composition comprising an antipsychotic exhibit synergy. Synergy between the composition comprising xanomeline and/or a salt thereof and the composition comprising an antipsychotic can be measured using the methods described herein.
- the oral pharmaceutical composition comprises a plurality of xanomeline beads comprising xanomeline or a salt thereof. In certain embodiments, the oral pharmaceutical composition comprises a plurality of trospium beads comprising a salt of trospium.
- the plurality of xanomeline beads has a core comprising xanomeline or a salt thereof.
- the plurality of trospium beads has a core comprising a salt of trospium.
- a capsule shell comprising hydroxypropyl methylcellulose (HPMC) containing separate populations of drug beads containing xanomeline tartrate or trospium chloride wherein the drug beads are of comparable size and release the actives rapidly and at substantially similar rates.
- HPMC hydroxypropyl methylcellulose
- the drug beads may dissolve in the stomach or pass through the pyloric valve into the duodenum intact or partially intact. Still, the two drugs' ratio, both in dissolved form and in undissolved form, remains relatively constant in the gastrointestinal tract until the drugs are absorbed.
- a capsule comprises 50 mg xanomeline as the tartrate salt and 10 mg trospium chloride. Fifty mg xanomeline as a free base corresponds to about 76 mg xanomeline tartrate.
- the trospium beads are formulated with a lower drug load. Effective doses of trospium and xanomeline are contained in roughly equivalent numbers of beads. Despite the differences in drug loads in certain embodiments, the trospium and xanomeline beads release at roughly similar rates. For example, if the dissolution of the capsules is assessed using a United States Pharmacopeia (USP) dissolution apparatus, the percentage of xanomeline dissolved is substantially equivalent to the percentage of dissolved trospium chloride, such as at 10 min, 20 min, or 30 min.
- USP United States Pharmacopeia
- the medicament may also include one or more pharmaceutically acceptable salts.
- the medicament may include one or more pharmaceutically-acceptable carriers.
- the medicament may be administered orally.
- the medicament may be delivered orally using tablets, troches, liquids, emulsions, suspensions, drops, capsules, caplets or gel caps, and other methods of oral administration known to one skilled in the art.
- the medicament may be in a dosage form that immediately releases the drug.
- the medicament may have a controlled release dosage form.
- the medicament may be in dosage forms that use other controlled-release formulations known to one in the art.
- the medicament is combined with one or more therapies, including psychotherapy and drugs.
- Therapeutic agents include, but are not limited, to antipsychotics, anxiolytics, anti-depressants, sedatives, tranquilizers, analgesics, and other pharmacological interventions known to one skilled in the art.
- a therapeutic agent may fall under the category of more than one drug.
- benzodiazepines can be considered anxiolytics, sedatives, and tranquilizers.
- an element means one element or more than one element.
- ranges set forth herein include all possible subsets of ranges and any combinations of such subset ranges.
- ranges include the stated endpoints, unless stated otherwise, where a range of values is provided, each intervening value between the upper and lower limit of that range and any other stated or intervening value in that stated range is encompassed within the disclosure.
- the upper and lower limits of these smaller ranges may independently be included in the smaller ranges and encompassed within the disclosure, subject to any specifically excluded limit in the stated range. Where the stated range includes one or both limits, ranges excluding either or both of those included limits are also contemplated to be part of the disclosure.
- wt.% is the weight percent based on the total weight, e.g., of the core, or enteric coating, or total bead, as described in context. Unless stated otherwise, the wt.% is intended to describe the weight percent based on dry weight (e.g., for a core following drying).
- controlled release is defined as a prolonged-release pattern of one or more drugs, such that the drugs are released over a period.
- a controlled release formulation has release kinetics that results in measurable serum levels of the drug over a period longer than what would be possible following intravenous injection or following administration of an immediate release oral dosage form. Controlled release, slow-release, sustained-release, extended-release, prolonged-release, and delayed-release have the same definitions.
- mammals include humans, primates, bovines, porcines, canines, felines, and rodents (e.g., mice and rats).
- a "patient,” “subject,” or “host” to be treated by the subject method means either a human or non-human mammal.
- pharmaceutically-acceptable carrier refers to a pharmaceutically-acceptable material, composition or vehicle, such as a liquid or solid filler, diluent, excipient, solvent, or encapsulating material, involved in carrying or transporting any subject composition or component thereof from one organ, or portion of the body, to another organ, or portion of the body.
- a pharmaceutically-acceptable material such as a liquid or solid filler, diluent, excipient, solvent, or encapsulating material, involved in carrying or transporting any subject composition or component thereof from one organ, or portion of the body, to another organ, or portion of the body.
- Each carrier must be “acceptable” in the sense of being compatible with the subject composition and its components and not injurious to the patient.
- materials that may serve as pharmaceutically acceptable carriers include sugars, such as lactose, glucose, and sucrose; starches, such as corn starch and potato starch; cellulose and its derivatives, such as sodium carboxymethyl cellulose, ethylcellulose, and cellulose acetate; powdered tragacanth; malt; gelatin; talc; excipients, such as cocoa butter and suppository waxes; oils, such as peanut oil, cottonseed oil, safflower oil, sesame oil, olive oil, corn oil, and soybean oil; glycols, such as propylene glycol; polyols, such as glycerin, sorbitol, mannitol, and polyethylene glycol; esters, such as ethyl oleate and ethyl laurate; agar; buffering agents, such as magnesium hydroxide and aluminum hydroxide; alginic acid; pyrogen-free water; isotonic saline; Ringer
- salt refers to a salt prepared from relatively nontoxic acids or bases, including inorganic acids and bases and organic acids and bases, including, for example, those contained in compositions of the present disclosure.
- Suitable non-toxic acids include inorganic and organic acids such as acetic, benzenesulfonic, benzoic, camphorsulfonic, citric, ethenesulfonic, fumaric, gluconic, glutamic, hydrobromic, hydrochloric, isethionic, lactic, maleic, malic, mandelic, methanesulfonic, mucic, nitric, pamoic, pantothenic, phosphoric, saccharinate, succinic, sulfuric, tartaric acid, p-toluenesulfonic, hydrochloric, hydrobromic, phosphoric, and sulfuric acids and the like.
- inorganic and organic acids such as acetic, benzenesulfonic, benzoic, camphorsulfonic, citric, ethenesulfonic, fumaric, gluconic, glutamic, hydrobromic, hydrochloric, isethionic, lactic, maleic, malic, mandelic,
- treating is art-recognized and refers to curing as well as ameliorating at least one symptom of any condition or disorder.
- therapeutic agent refers to any chemical moiety that is a biologically, physiologically, or pharmacologically active substance acting locally or systemically in a subject.
- therapeutic agents also referred to as "drugs,” are described in well-known literature references such as the Merck Index (14th editi on), the Physicians'Desk Reference (64th editi on), and The Pharmacological Basis of Therapeutics (12th editi on).
- These therapeutic agents include without limitation medicaments; vitamins; mineral supplements; substances used for the treatment, prevention, diagnosis, cure, or mitigation of a disease or illness; substances that affect the structure or function of the body, or pro-drugs, which become biologically active or more active after they have been placed in a physiological environment.
- psychotherapy refers to non-pharmacological therapies.
- Those skilled in the art use various techniques involving verbal and other interactions with a patient to affect a positive therapeutic outcome. Such techniques include, but are not limited to, behavior therapy, cognitive therapy, psychodynamic therapy, psychoanalytic therapy, group therapy, family counseling, art therapy, music therapy, vocational therapy, humanistic therapy, existential therapy, transpersonal therapy, client-centered therapy (also called person-centered therapy), Gestalt therapy, biofeedback therapy, rational emotive behavioral therapy, reality therapy, response-based therapy, Sandplay therapy, status dynamics therapy, hypnosis, and validation therapy.
- Psychotherapy may involve combining two or more techniques. A therapist can select and adjust the techniques based on the individual patient's needs and responses.
- musclecarinic disorder refers to any disease or condition ameliorated by activating the muscarinic system.
- diseases include ones in which direct activation of muscarinic receptors themselves or inhibition of cholinesterase enzymes has produced a therapeutic effect.
- disorders related to schizophrenia include, but are not limited to, schizo-affective disorder, psychosis, including acute psychosis, delusional disorders, psychosis associated with Alzheimer's disease, psychosis associated with Parkinson's disease, psychotic depression, bipolar disorder, bipolar with psychosis, Huntington's disease, Lewy Body dementia, or any other disease with psychotic features.
- Psychosis refers to an abnormal condition of the mind that results in difficulties determining what is real and not. Symptoms of psychosis include, but are not limited to, false beliefs (delusions), seeing or hearing things that others do not see or hear (hallucinations), incoherent speech, behavior that is inappropriate for the situation, sleep problems, social withdrawal, lack of motivation, and difficulties carrying out daily activities.
- Acute psychosis refers to the quick or strong onset of psychotic symptoms in a patient, for example, as defined in "Acute and Transient Psychotic Disorder” (International Classification of Diseases-10) and “Brief Psychosis”(DSM-IV). A sharp striking delusion with quick changes in the structure occurs in the individual who has acute psychosis after a short preliminary period of anxiety, insomnia, and confusion. Acute psychosis can include acute psychotic exacerbation when a patient may respond to hallucinations or delusions. Acute psychosis lasts for a short time, typically from one to two weeks.
- activator means a molecule described as an agonist, partial agonist, co-agonist, physiological agonist, potentiator, stimulator, allosteric potentiator, positive allosteric modulator, allosteric agonist, or a molecule that increases the activity or signaling of receptors directly or indirectly.
- inhibitor means a molecule described as an antagonist, partial antagonist, competitive antagonist, non-competitive antagonist, uncompetitive antagonist, silent antagonist, inverse agonist, reversible antagonist, physiological antagonist, irreversible antagonist, inhibitor, reversible inhibitor, irreversible inhibitor, negative allosteric modulator, allosteric antagonist, or a molecule that decreases the activity or signaling of receptors directly or indirectly.
- an "adverse event” is any untoward medical occurrence associated with treatment with a pharmaceutical composition described herein.
- a “mild adverse event” is easily tolerated by the subject, causes minimal discomfort, and does not interfere with everyday activities.
- a “moderate adverse event” is sufficiently discomforting to interfere with everyday activities; intervention may be needed.
- a “severe adverse event” prevents everyday activities; treatment or other intervention is usually needed.
- a “serious adverse event” results in death; is life-threatening (immediate risk of death from the event as it occurred); requires or prolongs inpatient hospitalization; results in persistent or significant disability/incapacity; or results in a congenital anomaly/disability, cancer, or drug overdose.
- An adverse event is incapacitating or disabling if it results in a substantial or permanent disruption of the subject's ability to carry out normal life functions.
- a patient is said to "tolerate" a dose of a compound if administering that dose to that patient does not result in an unacceptable adverse event or an unacceptable combination of adverse events.
- tolerance is a subjective measure and that what may be tolerable to one patient may not be tolerable to a different patient. For example, one patient may not be able to tolerate a headache. In contrast, a second patient may find headaches tolerable but is not able to tolerate vomiting. For a third patient, either headache alone or vomiting alone is tolerable. Still, the patient cannot tolerate the combination of headache and vomiting, even if the severity of each is less than when experienced alone.
- maximum tolerated dose means the highest dose of a drug or therapeutic that a patient can take without the patient experiencing intolerable side effects.
- the maximum tolerated dose is typically determined empirically in clinical trials.
- muscarinic receptors refers to G-protein linked receptors that bind the neurotransmitter acetylcholine. To date, five subtypes of the muscarinic receptor have been identified. “M1” means the subtype one muscarinic receptor. “M2” means the subtype two muscarinic receptor. “M3” means the subtype three muscarinic receptor. “M4" means the subtype four muscarinic receptor. “M5" means the subtype five muscarinic receptor.
- anxiolytics refers to drugs that reduce anxiety, fear, panic, or related feelings.
- drugs include, but are not limited to, benzodiazepines (e.g., alprazolam, chlordiazepoxide, clonazepam, clorazepate, diazepam, lorazepam), buspirone, barbiturates (e.g., amobarbital, pentobarbital, secobarbital, phenobarbital), and hydroxyzine.
- anti-depressants refers to drugs that alleviate depression and related conditions (e.g., dysthymia).
- drugs include, but are not limited to, selective serotonin-reuptake inhibitors (SSRIs, e.g., citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline), serotonin-norepinephrine reuptake inhibitors (SNRIs, e.g., desvenlafaxine, duloxetine, milnacipran, venlafaxine), mianserin, mirtazapine, norepinephrine reuptake inhibitors (e.g., atomoxetine, mazindol, reboxetine, viloxazine), bupropion, tianeptine, agomelatine, tricyclic antidepressants (e.g., amitriptyline, clomipramine, doxepin, imipramine, trimipra
- sedatives or “tranquilizers” refer to drugs that induce somnolence, promote a feeling of being tired or desire to sleep, or promote a state of unconsciousness.
- drugs include, but are not limited to, benzodiazepines, barbiturates (e.g., amobarbital, pentobarbital, secobarbital, phenobarbital), eszopiclone, zaleplon, zolpidem, and zopiclone.
- Example 1 Rodent models of psychosis demonstrated synergy between xanomeline dosed with risperidone or aripiprazole.
- mice were tested for drug effects using conditioned avoidance response (CAR) and MK-801-induced locomotor activity (LMA) tests.
- CAR conditioned avoidance response
- LMA locomotor activity
- mice were first trained to avoid a foot shock (i.e., crossing from one side of a shuttle box to another within 10 secs) to a performance criterion of >85% avoidance responses. A repeated-measures, counterbalanced design was used.
- Two experiments evaluated the effects of blocking central (with scopolamine) vs. peripheral (with N -methylscopolamine) muscarinic receptors.
- Additional experiments evaluated augmentation and synergy by combining dosing subthreshold doses of xanomeline plus risperidone or aripiprazole.
- “Subthreshold” of "sub-efficacious” refers to doses that are lower than the therapeutically effective amount for monotherapy but which could be effective in synergy with the antipsychotics tested.
- Xanomeline, risperidone, and aripiprazole dose-dependently reduced conditioned avoidance responding were analyzed separately via one-way repeated-measures ANOVA.
- a Dunnett post-hoc test was performed and that dose group significance was only assessed against Vehicle.
- Xanomeline [F(2.8, 55.4) 30.62, p ⁇ 0.0001]
- N 9;
- RIS low dose risperidone
- Xan subthreshold xanomeline
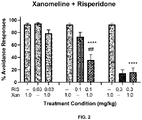
- N 17.
- Data are planned comparisons vs. xanomeline alone ( ⁇ ) and risperidone dose alone (#).
- Table 6 shows that actual avoidance responses were significantly higher than expected if the effects of xanomeline alone and risperidone alone were added together.
- Administration of either risperidone or aripiprazole alone did not significantly differ from vehicle-vehicle control conditions (data not shown). No incidence of escape failures was significant across any treatment condition.
- Table 7 shows that actual avoidance responses were significantly higher than expected if the effects of xanomeline alone and aripiprazole alone were added together. These comparative data are also displayed at FIGS. 7-10 . Table 7 - Average avoidance response percentages for xanomeline and aripiprazole combination therapy.
- FIG. 11 shows xanomeline's (Xan) effect following blockade of central and peripheral muscarinic receptors by scopolamine (SCOP) and by peripheral-only muscarinic receptors by N-methyl-scopolamine (NMS).
- FIG. 11 confirms that xanomeline depends on central muscarinic receptors. SCOP dose-dependently blocked xanomeline's effects, but NMS had no effect. A maximally active dose of xanomeline was used in this study. The 0.3 mg/kg dose of SCOP that fully blocks the activity of xanomeline has no activity alone in CAR.
- FIG. 12 shows that risperidone does not depend on central muscarinic receptors for its activity. Xanomeline and risperidone differ mechanistically from each other. Including trospium is not expected to affect xanomeline's therapeutic activity.
- NMS is an anticholinergic agent that lacks or has minimal penetration in the brain, thus blocking unwanted peripheral muscarinic activation from xanomeline, but allowing xanomeline to activate central muscarinic receptors.
- Suitable examples of other muscarinic antagonists include, but are not limited to, trospium, tolterodine, darifenacin, solifenacin, fesoterodine, and a salt thereof. These other muscarinic antagonists can be used in in-vitro or animal models or human clinical investigations with xanomeline and a composition comprising an antipsychotic.
- NMDA N-methyl-D-aspartate
- FIG. 13 and 14 depict the effects of risperidone doses alone against MK-801 induced activity ( FIG 13 ) and when combined with xanomeline ( FIG 14 ).
- Inactive doses of xanomeline (1 mg/kg) and risperidone (0.001 mg/kg) when combined resulted in almost a 70% reduction in MK-801 stimulated activity.
- Data are mean ( ⁇ SEM) total distance traveled.
- One-way ANOVAF(9,90) 7.34, p ⁇ 0.001.
- the 0.001 mg/kg risperidone + xanomeline group exhibited an augmented blockade of activity compared to the brain levels of xanomeline alone.
- MK-801 brain levels in the 0.1 mg/kg risperidone group were elevated compared to MK-801 alone, but MK-801 was unaffected in the risperidone + xanomeline groups. Exposures of risperidone or xanomeline alone groups were not measured.
- BLD below level of detection; 0.2 ng/mL for risperidone and MK-801; 0.4 ng/mL for xanomeline.
- Technical limitations prevented measuring risperidone at the active doses.
- Example 2 Aripiprazole formulation increased response alone in the Mouse CAR Assay
- Example 1 used a co-formulation of xanomeline and aripiprazole to deliver a single subcutaneous injection. This formulation limited aripiprazole exposure levels.
- This Example 2 used a formulation that enhanced aripiprazole absorption, resulting in a more robust response for aripiprazole alone. Also, in Example 2, compounds were delivered as two sequential subcutaneous injections rather than one. As a result, aripiprazole was evaluated at 10-fold lower doses in Example 2 than used in Example 1.
- Example 2 a 5% vehicle solution was prepared from 1.0 mL Tween-80 dissolved in 19.0 mL saline. To aid the solubility of the aripiprazole, three drops of 1.0-N HCl (15 ⁇ L) were added and vortexed. The average pH was 3.8 and compound was dosed at a 10 mL/kg bodyweight volume. Drug solutions were prepared fresh on each dosing day before testing. All solutions were mixed or vortexed thoroughly before injections.
- mice were male C57BL/6J, purchased from Jackson Labs, and successfully trained for CAR. Mice were first tested in an aripiprazole dose response study comprised of VEH, 0.3, 1, 3, and 10 mg/kg (data not shown). Dose order was randomly assigned for each mouse. Mice were returned to their home cages for 30 minutes following injection to allow the drug to take effect before testing began.
- Aripiprazole was effective at disrupting CAR performance in a dose-related manner.
- the 0.3 mg/kg dose best approximated the ED 50 . Escape failures were not evident at any doses.
- a relatively high concentration aripiprazole stock was first made and then diluted to the target concentrations for dosing.
- a 5% Tween-80 solution was prepared from 2.0 mL Tween-80 dissolved in 38.0 mL of saline.
- a 3.0 mg/kg aripiprazole solution as a stock was prepared from 3.0 mg aripiprazole dissolved in 5.0 mL 5% Tween-80, giving a concentration of 0.6 mg/mL.
- a dosing volume 5 mL/kg, equaling 3.0 mg/kg.
- aripiprazole To aid the solubility of the aripiprazole, three drops of 1.0-N HCl (15 ⁇ L) were added and vortexed. The average pH was 6.2. For 0.3 mg/kg aripiprazole, 0.6 mL of the 3 mg/kg aripiprazole stock was diluted in 5.4 mL of 5% Tween-80. For 0.1 mg/kg aripiprazole, 0.2 mL of the 3 mg/kg aripiprazole stock was dissolved in 5.8 mL of 5% Tween-80.
- the 1.0 mg/kg xanomeline solution was prepared from 3.05 mg xanomeline dissolved in 10.0 mL of sterile water, giving a concentration of 0.2 mg/mL. At a dosing volume of 10 mL/kg, this equals 1.0 mg/kg. (The drug mass adjustment factor between xanomeline free base and xanomeline tartrate is 1.5262.) The average pH was 4.4.
- mice were tested in CAR until all mice had completed the dosing regimen (see Table 9 below). Dose order was randomly assigned for each mouse. Injection 1 and Injection 2 occurred in sequence, with no gap time. Mice were returned to their home cages for 30 minutes following injection to allow the drugs to take effect before testing began. Mice were injected with vehicle (saline at 10 mL/kg SC and Tween-80 at 5 mL/kg IP) the day before dosing days. Mice were only dosed if their average percent avoidance values for the previous two non-dose days was > 85%.
- vehicle saline at 10 mL/kg SC and Tween-80 at 5 mL/kg IP
- the percent avoidance was analyzed via a two-way repeated-measures ANOVA with aripiprazole dose (vehicle, 0.1, or 0.3 and xanomeline dose (vehicle or 1.0) as factors. Planned comparisons of with or without xanomeline at the vehicle, 0.1, and 0.3 mg/kg aripiprazole (Bonferroni multiple comparisons corrected); ⁇ p ⁇ .05 versus without xanomeline.
- the aripiprazole solution was prepared as before.
- a dosing volume of 5 mL/kg this equals 0.3 mg/kg.
- the average pH of this solution was 7.3.
- mice were tested in CAR until all mice had completed the dosing regimen (Table 11). Dose order was randomly assigned for each mouse. Injection 1 was administered 15 minutes before Injection 2. During the interim, mice were returned to their home cages for 30 minutes following the final injection to allow the drugs to take effect before testing began. Mice were injected with vehicle (saline at 5 mL/kg S.C. and Tween-80 at 5 mL/kg I.P.) the day before dosing days. Mice were only dosed if their average percent avoidance values for the previous two non-dose days was > 85%.
- vehicle saline at 5 mL/kg S.C. and Tween-80 at 5 mL/kg I.P.
- avoidance behavior was analyzed via a one-way repeated measures ANOVA.
- N 15.
- a 3 mg/kg dose of aripiprazole had robust effects on CAR activity endpoints.
- Scopolamine had a slight, but statistically significant effect in reducing the activity of aripiprazole.
- robust activity of the scopolamine + aripiprazole combination was observed relative to vehicle control.
- xanomeline exhibited antipsychotic-like activity.
- This result indicates synergy between the xanomeline and the other two compounds.
- Central muscarinic receptors mediated xanomeline's efficacy in these animal models of psychosis.
- compositions are described as including components or materials, it is contemplated that the compositions can also consist essentially of, or consist of, any combination of the recited components or materials, unless described otherwise.
- methods are described as including steps, it is contemplated that the methods can also consist essentially of, or consist of, any combination of the recited steps, unless described otherwise.
- the disclosure illustratively disclosed herein suitably may be practiced in the absence of any element or step not specifically disclosed herein.
Landscapes
- Health & Medical Sciences (AREA)
- Animal Behavior & Ethology (AREA)
- Public Health (AREA)
- Pharmacology & Pharmacy (AREA)
- Chemical & Material Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Veterinary Medicine (AREA)
- General Health & Medical Sciences (AREA)
- Medicinal Chemistry (AREA)
- Epidemiology (AREA)
- Engineering & Computer Science (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Neurosurgery (AREA)
- Biomedical Technology (AREA)
- Neurology (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Chemical Kinetics & Catalysis (AREA)
- General Chemical & Material Sciences (AREA)
- Organic Chemistry (AREA)
- Psychiatry (AREA)
- Emergency Medicine (AREA)
- Psychology (AREA)
- Pain & Pain Management (AREA)
- Hospice & Palliative Care (AREA)
- Pharmaceuticals Containing Other Organic And Inorganic Compounds (AREA)
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US202163190136P | 2021-05-18 | 2021-05-18 | |
| US202163195524P | 2021-06-01 | 2021-06-01 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| EP4091607A1 true EP4091607A1 (fr) | 2022-11-23 |
Family
ID=78516695
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| EP21206327.5A Pending EP4091607A1 (fr) | 2021-05-18 | 2021-11-03 | Procédés de traitement de troubles du système nerveux central par l'activateur du récepteur muscarinique xanoméline et des antipsychotiques |
Country Status (1)
| Country | Link |
|---|---|
| EP (1) | EP4091607A1 (fr) |
Cited By (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2024114781A1 (fr) * | 2022-12-02 | 2024-06-06 | 上海日馨医药科技股份有限公司 | Agoniste de tpk et son procédé d'utilisation pour traiter des maladies neurodégénératives |
| CN120983394A (zh) * | 2025-08-21 | 2025-11-21 | 广州共禾医药科技有限公司 | 一种具有多层核壳结构的双药共载口服微丸制剂及其制备方法与应用 |
| AU2025242171B1 (en) * | 2025-03-26 | 2025-12-11 | Beigene Switzerland Gmbh | A Medicament and Method of Treatment of Central Nervous System and/or Neuropsychiatric Disorders |
Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2002003684A2 (fr) * | 2000-06-30 | 2002-01-10 | Eli Lilly And Company | Therapie de combinaison pour le traitement des psychoses |
| US20110020423A1 (en) * | 2009-07-22 | 2011-01-27 | Puretech Ventures | Methods and compositions for treatment of disorders ameliorated by muscarinic receptor activation |
| WO2022182733A1 (fr) * | 2021-02-24 | 2022-09-01 | Karuna Therapeutics, Inc. | Méthodes de traitement de troubles améliorés par activation des récepteurs muscariniques |
-
2021
- 2021-11-03 EP EP21206327.5A patent/EP4091607A1/fr active Pending
Patent Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2002003684A2 (fr) * | 2000-06-30 | 2002-01-10 | Eli Lilly And Company | Therapie de combinaison pour le traitement des psychoses |
| US20110020423A1 (en) * | 2009-07-22 | 2011-01-27 | Puretech Ventures | Methods and compositions for treatment of disorders ameliorated by muscarinic receptor activation |
| WO2022182733A1 (fr) * | 2021-02-24 | 2022-09-01 | Karuna Therapeutics, Inc. | Méthodes de traitement de troubles améliorés par activation des récepteurs muscariniques |
Non-Patent Citations (4)
| Title |
|---|
| "The Pharmacological Basis of Therapeutics" |
| ANONYMOUS DOWNLOAD: "PureTech Affiliate Karuna Therapeutics Announces KarXT Met Primary Endpoint in Phase 2 Clinical Trial of Acute Psychosis in Patients with Schizophrenia | PureTech Health", 19 November 2019 (2019-11-19), XP093303315, Retrieved from the Internet <URL:https://news.puretechhealth.com/news-releases/news-release-details/puretech-affiliate-karuna-therapeutics-announces-karxt-met> * |
| BRANNAN STEPHEN: "Karxt: A M1/M4 preferring muscarinic agonist for the treatment of schizophrenia", 1 April 2019 (2019-04-01), XP093303319, Retrieved from the Internet <URL:https://pmc.ncbi.nlm.nih.gov/articles/PMC6455874/pdf/sbz019.386.pdf> * |
| REAGAN-SHAW ET AL., THE FASEB JOURNAL, vol. 22, no. 3, pages 659 - 661 |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2024114781A1 (fr) * | 2022-12-02 | 2024-06-06 | 上海日馨医药科技股份有限公司 | Agoniste de tpk et son procédé d'utilisation pour traiter des maladies neurodégénératives |
| AU2025242171B1 (en) * | 2025-03-26 | 2025-12-11 | Beigene Switzerland Gmbh | A Medicament and Method of Treatment of Central Nervous System and/or Neuropsychiatric Disorders |
| AU2025275131B2 (en) * | 2025-03-26 | 2026-01-22 | Beigene Switzerland Gmbh | A Medicament and Method of Treatment of Central Nervous System and/or Neuropsychiatric Disorders |
| CN120983394A (zh) * | 2025-08-21 | 2025-11-21 | 广州共禾医药科技有限公司 | 一种具有多层核壳结构的双药共载口服微丸制剂及其制备方法与应用 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Madari et al. | Pharmacological management of insomnia | |
| US20240100039A1 (en) | Methods and compositions for treatment of disorders ameliorated by muscarinic receptor activation | |
| EP4091607A1 (fr) | Procédés de traitement de troubles du système nerveux central par l'activateur du récepteur muscarinique xanoméline et des antipsychotiques | |
| US10265311B2 (en) | Methods and compositions for treatment of disorders ameliorated by muscarinic receptor activation | |
| HK1209323A1 (en) | Esketamine for the treatment of treatment-refractory or treatment-resistant depression | |
| ES2673956T3 (es) | Régimen de dosificación, envase de dispensación de la medicación y usos de los mismos para el tratamiento del trastorno depresivo mayor | |
| US11000519B2 (en) | Pridopidine for treating drug induced dyskinesias | |
| US20240156802A1 (en) | Methods for treating disorders ameliorated by muscarinic receptor activation | |
| US20220370454A1 (en) | Methods for treating central nervous system disorders with muscarinic receptor activation and antipsychotics | |
| US20120010242A1 (en) | Low dose pipamperone in treating mood disorders | |
| CN114585354A (zh) | 用芬氟拉明治疗癫痫患者的方法 | |
| US9066949B2 (en) | Compositions and methods for the treatment of catatonia | |
| WO2010135441A1 (fr) | Méthode de traitement des troubles obsessionnels compulsifs au moyen de l'ondansétron | |
| ZA200509904B (en) | Asenapine for the treatment of schizophrenia in a patient with overweight or predisposition for overweight | |
| EP2236157A1 (fr) | Pipampérone et un agent ultérieur pour le traitement des troubles de l'humeur et de l'anxiété | |
| HK40084241A (en) | Methods for treating central nervous system disorders with muscarinic receptor activator xanomeline and antipsychotics | |
| Green | Focus on amisulpride | |
| Kang et al. | Psychosis in nursing home patients with Parkinson's disease | |
| de Miranda et al. | Mood Stabilizers: Quetiapine | |
| Casaer et al. | Risperidone in the treatment of childhood autistic disorder: an open pilot study | |
| CN117529318A (zh) | 治疗阿尔茨海默病的方法 | |
| Rowles et al. | Antipsychotic agents | |
| HK1228453A1 (en) | Compositions for treatment of disorders ameliorated by muscarinic receptor activation | |
| WO2012075288A1 (fr) | Procédé de traitement d'un trouble obsessionnel compulsif par l'ondansétron |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| PUAI | Public reference made under article 153(3) epc to a published international application that has entered the european phase |
Free format text: ORIGINAL CODE: 0009012 |
|
| STAA | Information on the status of an ep patent application or granted ep patent |
Free format text: STATUS: THE APPLICATION HAS BEEN PUBLISHED |
|
| AK | Designated contracting states |
Kind code of ref document: A1 Designated state(s): AL AT BE BG CH CY CZ DE DK EE ES FI FR GB GR HR HU IE IS IT LI LT LU LV MC MK MT NL NO PL PT RO RS SE SI SK SM TR |
|
| STAA | Information on the status of an ep patent application or granted ep patent |
Free format text: STATUS: REQUEST FOR EXAMINATION WAS MADE |
|
| 17P | Request for examination filed |
Effective date: 20230523 |
|
| RBV | Designated contracting states (corrected) |
Designated state(s): AL AT BE BG CH CY CZ DE DK EE ES FI FR GB GR HR HU IE IS IT LI LT LU LV MC MK MT NL NO PL PT RO RS SE SI SK SM TR |
|
| REG | Reference to a national code |
Ref country code: HK Ref legal event code: DE Ref document number: 40084241 Country of ref document: HK |
|
| STAA | Information on the status of an ep patent application or granted ep patent |
Free format text: STATUS: EXAMINATION IS IN PROGRESS |
|
| 17Q | First examination report despatched |
Effective date: 20250813 |