WO2005107776A1 - METHOD OF ADMINISTERING PORCINE B-DOMAINLESS fVIII - Google Patents
METHOD OF ADMINISTERING PORCINE B-DOMAINLESS fVIII Download PDFInfo
- Publication number
- WO2005107776A1 WO2005107776A1 PCT/US2005/014760 US2005014760W WO2005107776A1 WO 2005107776 A1 WO2005107776 A1 WO 2005107776A1 US 2005014760 W US2005014760 W US 2005014760W WO 2005107776 A1 WO2005107776 A1 WO 2005107776A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- obi
- patient
- porcine
- ill
- hyate
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/36—Blood coagulation or fibrinolysis factors
- A61K38/37—Factors VIII
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/0005—Vertebrate antigens
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/02—Inorganic compounds
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/06—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite
- A61K47/08—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite containing oxygen, e.g. ethers, acetals, ketones, quinones, aldehydes, peroxides
- A61K47/12—Carboxylic acids; Salts or anhydrides thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/06—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite
- A61K47/16—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite containing nitrogen, e.g. nitro-, nitroso-, azo-compounds, nitriles, cyanates
- A61K47/18—Amines; Amides; Ureas; Quaternary ammonium compounds; Amino acids; Oligopeptides having up to five amino acids
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/06—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite
- A61K47/26—Carbohydrates, e.g. sugar alcohols, amino sugars, nucleic acids, mono-, di- or oligo-saccharides; Derivatives thereof, e.g. polysorbates, sorbitan fatty acid esters or glycyrrhizin
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/0012—Galenical forms characterised by the site of application
- A61K9/0019—Injectable compositions; Intramuscular, intravenous, arterial, subcutaneous administration; Compositions to be administered through the skin in an invasive manner
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/14—Particulate form, e.g. powders, Processes for size reducing of pure drugs or the resulting products, Pure drug nanoparticles
- A61K9/19—Particulate form, e.g. powders, Processes for size reducing of pure drugs or the resulting products, Pure drug nanoparticles lyophilised, i.e. freeze-dried, solutions or dispersions
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P43/00—Drugs for specific purposes, not provided for in groups A61P1/00-A61P41/00
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P7/00—Drugs for disorders of the blood or the extracellular fluid
- A61P7/04—Antihaemorrhagics; Procoagulants; Haemostatic agents; Antifibrinolytic agents
Definitions
- Hemophilia A is a disease characterized by a defect in blood clotting which results in a variety of clinical symptoms and is ultimately life-threatening.
- Standard treatment of the disease is administration of clotting factor VIII (fVIII), a 300 kDa plasma protein missing or deficient in Hemophilia A patients.
- fVIII clotting factor VIII
- the therapy does not cure the underlying disease, but it ameliorates the symptoms. Therefore, patients must receive repeated doses of fVIII over their lifetime.
- OBI-1 is also termed POL-1212 in U.S. Patent No. 6,458,563. Both names, OBI-1 and POL 1212, refer to the same substance, porcine A Ill having the B-domain deleted except for 12 amino acids at the N-terminal part of the B-domain and 12 amino acids at the C-terminal part of the B-domain. Previous studies [Doering, C.B. et al. (2002) J. Biol. Chem. 277:39345-38349] have documented that the B-domain of porcine fVIII can be deleted without loss of activity.
- 5,763,401 and 5,874,408 disclose a recombinant fVIII composition containing glycine, histidine, sucrose, sodium chloride, and calcium chloride.
- fVIII compositions having various salts, non-ionic surfactants and antioxidants (US Patent No. 5,962,650, US Patent No. 5,972,885, WO 89/09784, and WO 94/07510).
- WO 03/080108 describes a stable solid pharmaceutical composition devoid of amino acids which contain fVIII, a surfactant, calcium chloride, sucrose, sodium chloride, trisodium citrate, and a buffer and has a pH of 6-8 prior to lyophilization and after reconstitution in water for injection.
- the present invention relates to the surprising experimental findings that OBI-1 has 2-6 fold greater bioavailability compared to HYATE:C.
- Bioavailability refers to the blood levels achieved and maintained after administering a given dose. Bioavailability can be assessed by calculating the area under the curve (AUC) of blood levels plotted as a function of time after administration of a given dose. Consequently, compared to HYATE:C, OBI-1 can be administered at a substantially lower dose, expressed in Units/kg of body weight, to provide equivalent protection against serious bleeding episodes or in the prevention of bleeding episodes for hemophiliac patients who are in non-bleeding state.
- AUC area under the curve
- OBI-1 can be provided at the same dose as, or a similar dose to, HYAGE:C, but at a reduced frequency of administration compared to HYATE:C, bringing about more rapid control of bleeding and reducing the inconvenience associated with multiple administrations. Coupled with the fact that OBI-1 is available at a higher concentration in Units/ml than HYATE:C, the findings provide for a new method of administration that is highly advantageous for patients' well-being and quality of life. Current treatments with HYATE:C (100 Units/kg of body weight) typically require intravenous infusion of 280 ml of HYATE:C solution, at a rate of 2-5 ml per minute repeated every 6-8 hrs.
- OBI-1 can be administered as a single intravenous injection of about 10- 100 Units/kg body wt, e.g. 14 ml, requiring only 5-15 minutes to administer and may be required only one to four times, in order to halt a bleed, in contrast to HYATE:C, which takes a median of eight separate administrations over a two day period to halt a single bleeding episode, according to its package insert.
- HYATE:C which takes a median of eight separate administrations over a two day period to halt a single bleeding episode, according to its package insert.
- OBI-1 Using OBI-1 , faster control of bleeding is facilitated because higher fVIII levels can be achieved more rapidly.
- the actual dose administered to an individual depends on several individual factors including body weight, plasma volume, and residual antibody titer to OBI-1.
- the methods for calculating individual dosage have been well established from studies with HYATE:C.
- the methods for calculating OBI-1 dosage will, in addition, require taking into account the newly discovered greater in vivo efficacy and bioavailability of OBI-1.
- the present invention also provides pharmaceutical compositions and kits containing OBI-1 that are useful for treating a patient in need of fVIII in a more rapid and effective manner.
- Fig. 1 is a graph of activity recoveries of fVIII (Example 1), corrected for baseline Ill after a single injection of either HYATE:C or OBI-1 into cynomolgus monkeys at the indicated dose as described in Example 1.
- Fig. 2 is a graph of results obtained from the experiment described in
- Example 5 Individual patient plasmas are arrayed along the horizontal axis. The vertical axis indicates U/ml of fVIII activity recovered from the individual plasmas after addition of fVIII as described in Example 5. The data for King George Biomedical plasmas are designated as "good” or "bad” based on anomalous behavior of the latter plasma (see Example 5).
- Fig. 3 is a graph showing the plasma concentrations of fVIII in six human patients after intravenous administration of OBI-1 or HYATE:C.
- the Y axis indicates U/ml of fVIII activity recovered from the individual plasmas as measured by the one-stage activity assay.
- Fig. 4 is a graph showing the plasma concentrations of fVIII in six human patients after intravenous administration of OBI-1 or HYATE:C.
- the Y axis indicates U/ml of fVIII activity recovered from the individual plasmas as measured by the chromogenic assay as described herein.
- physiologically acceptable carrier is an organic or inorganic composition which serves as a carrier/stabilizer of the active ingredient of the present invention, OBI-1 , in a pharmaceutical composition.
- physiologically acceptable carriers include but are not limited to water, phosphate-buffered saline, saline, aqueous solvents, where water is mixed with lower alkanols, vegetable oils, polyalkylene glycols, petroleum-based jelly, ethyl cellulose, ethyl oleate, carboxymethyl cellulose, polyvinylpyrrolidine, isopropyl myristate.
- Physiologically acceptable carriers further include albumin, an amino acid (e.g., glycine, histidine, or its salts), a detergent (ionic and non-ionic) such as polysorbate or TWEEN 80, a high ionic strength media consisting of sodium salts, calcium salts and/or histidine, mono-, di- or polysaccharides (e.g., sucrose) or sugar alcohols, and other diluents, additives or carriers known in the art.
- a detergent ionic and non-ionic
- a detergent ionic and non-ionic
- a high ionic strength media consisting of sodium salts, calcium salts and/or histidine, mono-, di- or polysaccharides (e.g., sucrose) or sugar alcohols, and other diluents, additives or carriers known in the art.
- a high ionic strength media consisting of sodium salts, calcium salts and/or histidine, mono-, di- or
- a pharmaceutical composition comprising OBI-1 is preferably a solid composition obtainable by lyophilization of a solution devoid of amino acids comprising OBI-1 , a surfactant or detergent, calcium chloride, sucrose, sodium chloride, trisodium citrate and a buffer.
- the solution has a pH of 6-8 prior to lyophilization and after reconstitution in water for injection.
- the surfactant is preferably a non-ionic surfactant such as polysorbates and block copolymers like poloxamers (i.e., copolymers of polyethylene and propylene glycol).
- a more preferred surfactant is a polysorbate having a mean polymerization degree from 20 to 100 monomer units (preferably about 80).
- the most preferred surfactant is polysorbate 80 derived from a plant.
- the buffer is preferably tris(hydroxymethyl)methylamine, commonly known as "tris.”
- the solid pharmaceutical composition is prepared by lyophilization from the solution containing OBI-1 at a concentration from 50 to 10,000 Units/mL, a surfactant at a concentration ranging from above critical micellar concentration to 1% v/v, calcium chloride at 0.5- 10 mM, sucrose at 5-50 mM, sodium chloride at 0.15-50 0.5 M, trisodium citrate at 1- 50 mM, and a buffer at 1-50 mM.
- the pH of the pharmaceutical composition prior to lyophilization and after reconstitution in water for injection is preferably about 6.5- 7.5, more preferably about 7.0.
- the solid pharmaceutical composition containing OBI-1 may be diluted with sterile water optionally containing sodium chloride before administering into a patient in need of fVIII.
- the administration of such composition is typically carried out intravenously.
- the optimal dose of composition to be administered will be determined by the treating physician based on the severity of the disease for each patient.
- WO 03/080108 which is incorporated herein as reference in its entirety, discloses detailed description of a method of preparing the solid pharmaceutical compositions comprising OBI-1 described herein.
- reducing blood clotting time refers to the reduced length of time for blood clotting to occur in a given patient having fVIII deficiency when OBI-1 is administered compared to when HYATE:C is administered, i.e., the difference in the length of time for blood clotting to occur in patients treated with OBI-1 and those treated with HYATE:C administration.
- the term, "therapeutically effective level or concentration of factor VIII” as used herein, means the level of fVIII in the plasma of a patient having fVIII deficiency, who has received a pharmaceutical composition of OBI-1 , that is sufficient to exhibit a measurable improvement or protective effect in the patient (e.g., to stop bleeding).
- the patients having fVIII deficiency are typically hemophilia A patients but also include those subjects diagnosed with "acquired hemophilia", a condition in which those who are not congenital hemophiliacs spontaneously develop inhibitory antibodies to their fVIII, creating a serious fVIII deficiency.
- the therapeutically effective level is estimated to be about 1 %, preferably about 10%, most preferably about 25-35% and above, of the fVIII level in a normal, non- hemophilia A subject.
- concentration range of fVIII in normal non-hemophilia A humans is defined as 50% to 200% of the fVIII activity found in a sample plasma pool derived from at least 20 normal donors.
- the level of fVIII in normal humans fluctuates through this normal range in response to various physiologic and non- physiologic stimuli.
- antibody-neutralizing dose of OBI-1 is used to indicate the amount of OBI-1 necessary to administer to neutralize the patient's preexisting antibodies directed against OBI-1.
- the level of a hemophilia A patient's antibody to porcine fVIII is different for each individual.
- the amount of anti-OBI-1 antibody present can be readily calculated by measuring the antibody titer, using standard methods known in the art, and from this value, the amount of OBI-1 required to neutralize the antibody can be estimated. Because of individually differing binding and inactivating characteristics of each patient's inhibitory antibody, the precise amount of OBI-1 required can only be estimated, and the exact amount to be administered must be empirically determined, (or "titrated")
- Human fVIII deficiency can be studied in fVIII-deficient mammals because the steps of blood clot formation are shared among all vertebrates, and fVIII proteins of several species are known to have a high degree of sequence homology. Bioavailability can also be assessed in non-hemophilic monkeys. After taking into account species variations in blood volume, basal fVIII levels and the like, results from animal studies are generally predictive of results in humans. The present invention was developed from results of experiments, described in detail below. Studies of four types were conducted: bioavailability studies in monkeys and hemophilic dogs, efficacy studies in hemophilic dogs and hemophilic mice, an in vitro activity recovery study in human plasma, and an in vivo bioavailability studies in six human subjects.
- Bioavailability was assessed by measuring recovery of activity at a specified time after administering a given dose. Efficacy was assessed by measuring the effect of a given dose on the cuticle bleeding time (CBT) in hemophilic dogs and by mortality in a tail-transection-bleeding model of hemophilic mice. Recoveries of OBI-1 and the HYATE:C were also measured in vitro by adding each substance to human hemophilic plasma samples and human hemophilic-inhibitor plasma samples. Bioavailability was further assessed in six human subjects by measuring recovery of activity at a specified time after administering a standard dose of 100 U/kg.
- OBI-1 and HYATE:C resulted in greater recovery of OBI-1 than HYATE:C based on a standard /Ill clotting assay.
- OBI-1 can be administered at a significantly lower effective dose than can HYATE:C, where the activity level of each has been measured by a standard A/Ill assay. It will be understood by those skilled in the art that the effective dose can be calibrated according to individual patient requirements, including residual levels of A/Ill existing in the patient's plasma and the level of inhibitory antibodies in the patient's plasma that must be neutralized.
- Recoveries of OBI-1 and the HYATE:C also were measured in vitro after adding each to a nominal concentration of 1 U/ml to human plasma samples from hemophilia patients with inhibitors. Recoveries of both OBI-1 and HYATE:C were lower than the nominal concentration, which was due in part to cross-reactive inhibitory antibodies. However, in 25 of 35 samples, recovered OBI-1 activity was greater than recovered HYATE:C activity, and in 18 of the 35 samples, recovered OBI-1 activity was more than 2-fold greater than recovered HYATE:C activity.
- Bioavailability studies were further carried out in six human subjects, with absent or minimal inhibitory antibodies to OBI-1 , in a randomized, double-blind, double-dummy, parallel-group blinded manner as described in Example 6. As shown in Table 8 and Figs. 3 and 4, the bioavailability of OBI-1 was much greater than HYATE:C when both were administered at 100 U/kg.
- OBI-1 is a recombinant product
- HYATE:C is a plasma derived product.
- human factor IX used in the treatment of hemophilia B
- the plasma derived product actually showed recoveries about two times greater than the recombinant derived product (1.71+/- 0.73 IU per dL per IU per kg compared to 0.86+/- 0.313 IU per dL per IU per kg [see Ewenstein BM et al. Transfusion (2002), 42:190].
- OBI-1 and HYATE:C are consistent with the pharmacokinetic data obtained using monkeys, hemophilic dogs, and hemophilic mice. These results further indicate that OBI-1 can be administered at a lower dose or equally important can be administered at a greatly reduced frequency of administration, compared to HYATE:C, to yield equivalent therapeutic effects in patients having A/Ill deficiency. The data also show that OBI-1 reaches peak and therapeutic levels much more rapidly than equivalent doses of HYATE:C, allowing for more rapid control of bleeding.
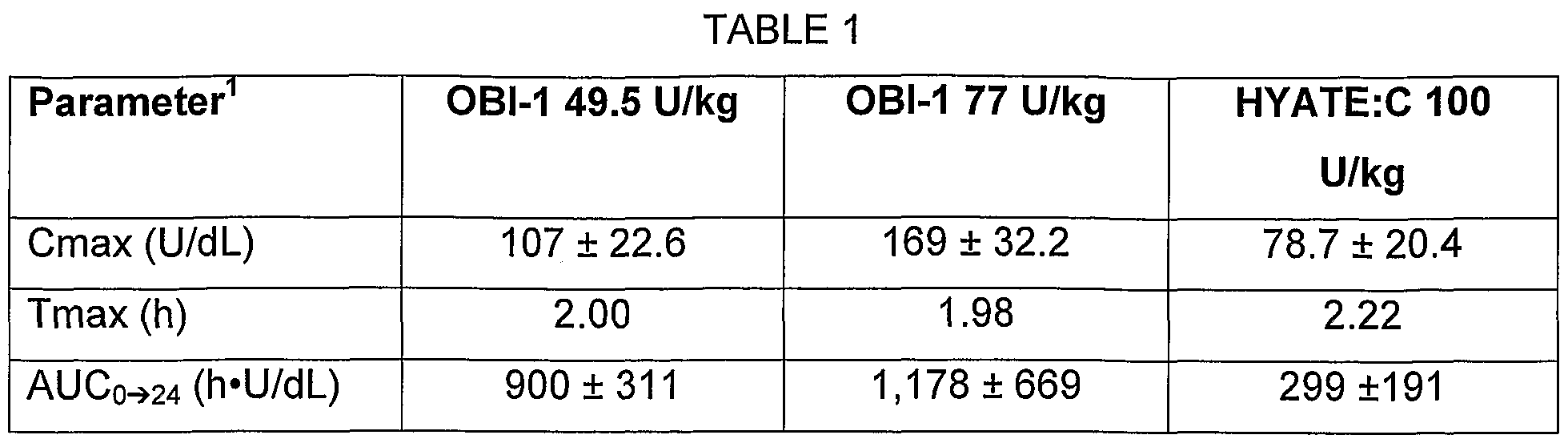
- Non-hemophilic cynomolgus monkeys were used to compare bioavailability of OBI-1 and HYATE:C. Groups of 4 monkeys were given one dose of either HYATE:C 100 U/kg, or OBI-1 at doses of either 49 or 77 U/kg. Blood samples were drawn at specified time points thereafter, and the A/Ill levels obtained were used to calculate pharmacokinetic parameters, including the activity levels integrated over time. The integrated value is referred to as area under the curve for the specified time period (AUC 0 ⁇ t).
- a 77 U/kg dose of OBI-1 provided about 5- fold greater AUC 0 ⁇ 24 than did 100 U/kg of HYATE:C. Similar results were obtained in a separate study using five monkeys receiving 40 U/kg OBI-1 , 5 monkeys receiving 100 U/kg OBI-1 and 6 monkeys receiving 100 U/kg HYATE:C. (Table 2.)
- EXAMPLE 2 Bioavailability in Hemophilic Dogs [0033] Originally discovered as a spontaneous mutation, dogs with hemophilia A have been maintained in a protected colony for over twenty years. The colony housed at the Queens University in Springfield, Ontario, is in its tenth generation. They have no circulating A Ill activity or protein and their phenotypic picture is analogous to severe hemophilia A in humans, with recurrent severe spontaneous soft tissue and joint bleeds and chronic joint deformities. They require frequent injections of canine-derived plasma or cryoprecipitate to control their bleeding.
- FVIII levels were determined against a porcine A/Ill standard designated HY98P. Although these hemophilic dogs have no measurable canine Ill activity, and no A/Ill antigen present in their blood, they were found to have measurable A Ill activity at baseline (0.1 to 0.3 U/ml) when tested against a porcine A/Ill standard.
- This porcine standard was made by adding varying amounts of the actual test product HYATE:C or OBI-1 (in 1 % bovine serum albumin/imidazole buffer) to factor VIII deficient human hemophilic plasma. For purposes of determining pharmacokinetic parameters, therefore, the baseline activity measured was subtracted from the measured activity at each time point and the difference in A/Ill activity was entered for all calculations. For both products tested, there was substantial variability in the pharmacokinetic values obtained from the dogs tested at each dose level.
- CBT Efficacy in Hemophilic Dogs
- the time it takes for bleeding to stop after the dog's toenail cuticle is cut is a useful measure of efficacy in hemophilia dogs.
- the cuticle In the untreated dog with hemophilia, the cuticle usually stops bleeding in approximately 2 minutes, does not bleed for a brief time and then re-bleeds steadily for at least 12 minutes or until the lesion is cauterized.
- the normal CBT is defined as 5 or fewer minutes of bleeding and no need for cauterization.
- CBT in dogs with congenital hemophilia has been used widely as a measure of the efficacy of investigational A/Ill products.
- Table 5 demonstrates the individual changes in the CBT results for each dog for each injection.
- mice have been created by targeted disruption of exon
- the E16 mice have undetectable A/Ill activity, occasional spontaneous bleeding, and prolonged bleeding and increased mortality after tail transection or laceration of the tail vein.
- An efficacy model has been developed in which the ability of A/Ill to decrease the mortality in E16 mice following transection of the distal 2 cm of tail is assessed.
- mice Male or female hemophilia A mice, aged 9 to 10 weeks, were injected by tail vein with various concentrations of OBI-1 or control buffer. The mice were anesthetized and, 15 min after injection, the distal 2 cm of tail was transected and allowed to bleed freely. This injury reportedly is fatal within 24 h in most E16 hemophilia A mice.
- Units/kg is effective in preventing death in this model. Combining the data at 0.4 and 1.2 Units/kg, there are 14/14 survivors compared to 6/38 survivors in the control (untreated) group. An estimated dose conferring 50% survival (ED 50 ) was 0.044 U/kg. Furthermore, every mouse receiving at least 0.4 U/kg survived.
- mice Prior to tail vein injections of HYATE:C (0 to 100 A lll Units/kg), or placebo (saline), mice were warmed under a 60-watt lamp for 2 minutes to dilate the tail veins. Fifteen minutes after injection, mice were anesthetized with Metofane and the distal 2 cm of the tail was amputated. Mice were placed into clean cages with paper towels in place of litter and observed for 24 hours to determine survival. Well- moistened food was placed inside each cage in addition to the usual water bottle and dry pellets. Survivors were terminated after 24 hours using Metofane followed by cervical dislocation.
- the estimated ED 50 for HYATE:C was 0.2 U/kg, 4-5 times greater than that estimated for OBI-1 , predicting greater efficacy of OBI-1. Overall, the comparative efficacy of HYATE:C and OBI-1 has not been rigorously studied in hemophilia A mice.
- A/lll-deficient plasma human hemophilia A plasma, product no. 0800
- Human hemophilia A plasma, product no. 0800 were purchased from George King Bio-medical, Inc. They were stored at -70°C.
- Activated partial thromboplastin time (aPTT) reagent (product No. 35513) was purchased from Organon Teknika Corp. It was stored in a lyophilized state at 4°C.
- OBI-1 Vehicle, Lot No. 214-02-001 was reconstituted with 1 ml Water for Injection per vial (60 vials total).
- Four vials of OBI-1 Lot No. 214-01-001 , were each reconstituted with 1 ml Water for Injection, yielding an expected concentration of 550 U/ml according to the manufacturer's label.
- OBI-1 was diluted 15.9-fold further by addition of 59.6 ml of reconstituted OBI-1 vehicle, yielding a predicted concentration of 34.6 U/ml.
- HYATE:C was sub-aliquoted into 120 aliquots of 0.5 ml each and frozen at -70°C.
- OBI-1 was sub-aliquoted into 127 aliquots of 0.5 ml each and frozen at -70 °C.
- Citrated plasmas from patients with inhibitory antibodies to A/Ill were shipped on dry ice to Emory University from several hemophilia treatment centers. Samples were frozen at -70°C until used. From 58 plasmas that were obtained, 25 were randomly selected for study.
- aPTT reagent was solubilized in 3 ml H 2 O according to the manufacturer's instructions and kept at room temperature until used.
- FACT and A lll-deficient plasma were stored on ice after rapid thawing in a 37 °C water bath.
- FVIII-deficient plasma 50 ⁇ l was added to sample cuvettes and allowed to warm for 30-45 seconds before addition of the remaining reagents. Dilutions of the A/Ill standard or sample (5 ⁇ l) were added, followed by addition of 50 ⁇ l aPTT reagent and incubation for 250 seconds.
- Clotting was initiated by addition of 50 ⁇ l pre-warmed CaCI 2 solution using a cabled pipette. The addition activates an internal timer and records the clotting time in seconds.
- a standard curve was prepared using four dilutions of FACT into Hank's Buffered Saline: undiluted, 1/3, 1/11 , and 1/21.
- the A/Ill concentration of undiluted FACT is approximately 1 U/ml and ranged from 1.04 to 1.09 U/ml according to the manufacturer.
- the clotting time was plotted versus the logarithm of the A/Ill concentration and the standard curve was calculated by linear regression.
- the A/Ill concentration of samples was measured by interpolation on the standard curve, except in the case of analysis of stock solutions of OBI-1 and HYATE:C, for which more extensive measurements were made, as described in Results.
- HYATE:C was measured in 33 of the available inhibitor plasma samples (Fig. 2). In all cases, the plasmas were spiked to a predicted A Ill activity of 0.9 U/ml. Additionally, two hemophilia A plasmas obtained from George King were included, and are shown at the far right in the figure. "Good” plasma corresponds to commercially available reagent plasma in which recovery of A/Ill in HYATE:C and OBI-1 had previously been found to be in the expected range. "Bad” plasma corresponds to plasma in which recovery of A Ill in HYATE:C had previously been found to be less than 10% of expected at Ipsen.
- HYATE:C in human subjects, the following randomized, parallel-group blinded comparison study was carried out with nine human patients. Of these 9 patients, five had no detectable anti-porcine inhibitor at baseline (i.e. less than 0.8 Bethesda units) and one (assigned to the OBI-1 group) had a very low inhibitor of 1.0 Bethesda units. Of the six patients with either no preexisting inhibitor or a very low inhibitor to porcine A Ill, three received HYATE:C and three received OBI-1. The three patients with significantly higher levels of inhibitors were excluded from the bioavailability assessment, as the presence of such inhibitors depresses bioavailability, thereby confounding the analysis.
- OBI-1 was provided in sterile vials containing 535 Units of A/Ill activity per vial. Each vial was reconstituted with 1.0 ml Sterile Water for Injection USP to a final concentration of 535 U/ml.
- HYATE:C was provided in sterile vials containing 541 IU of A/Ill per vial. Each vial was reconstituted with 20 ml Sterile Water for Injection USP to a final concentration of 27 lU/ml. The dose of each product administered was 100 lU/kg regardless of subject antibody titer.
- the pharmacokinetic parameters measured in this study include Clearance (CL, ml/h/kg), Area Under the Curve (AUC, U/dL), Maximum Concentration (Cmax, U/ml), Volume of distribution (Vz), mean time to maximum concentration (Tmax, h), and half-time (T 1 2 , h).
- the AUC values for OBI-1 were about 2-2.5 times greater than that for HYATE:C.
- the difference in AUC between OBI-1 and HYATE:C was more pronounced in the chromogenic assay than the one-stage activity assay.
- Maximum concentration (Cmax) in the blood for OBI-1 was about 3 times greater than for HYATE:C (151 vs 53 by the chromogenic assay).
- the mean time to Maximum Concentration (Tmax) was approximately 2.5 to 3 times shorter for OBI-1 than it was for HYATE:C.
- OBI-1 has much greater bioavailability compared to HYATE:C. Therefore, OBI-1 can be administered at a lower dose or be administered at a reduced frequency of administration, compared to HYATE:C, to yield equivalent therapeutic effects in A/Ill deficient patients. And OBI-1 at equivalent doses to Hyate:C can bring more rapid control of bleeding.
- the A/Ill concentration in normal non-hemophilia A subjects is approximately 100 Units/dL.
- a typical bleeding episode is very likely to be controlled if the plasma level of A/Ill is reached at about 25% and 35% of the normal level and maintained for several hours (Roberts H and Hoffman M, "Hemophilia A and Hemophilia B," Chapter 123 in Beutler E, Lichtman M, Coller B, Kipps T and Seligsohn U (Eds), Williams Hematology, 6 th edition (2001): pages 1639-1657; McGraw-Hill, New York).
- Example 6 The combined data of Examples 1-6 demonstrate the unexpected finding that OBI-1 behaves differently from HYATE:C in human and animal plasma.
- OBI-1 recombinant porcine A lll
- HYATE:C plasma-derived porcine A Ill
- This surprising result is precisely the opposite of what was seen with factor IX, where the plasma-derived concentrate had significantly greater recovery and bioavailability that the recombinant factor IX product (Ewenstein et al. supra).
- the greater bioavailability of OBI-1 compared to HYATE:C was also surprising, in light of the report by Kessler et al.
- OBI-1 may be administered to a patient at as little as 1/6 the standard activity dose in units/kg recommended for HYATE:C.
- the recommended dose for HYATE:C is 100 lU/kg of body wt in excess of the dose required to neutralize any patient antibody to porcine A/Ill.
- the level of a patient's antibody to porcine A/Ill is different for each individual.
- the dose of OBI-1 required to neutralize the patient's antibodies can be estimated from measurement of antibody titer, using standard methods known in the art. Accordingly, for a given patient, one can administer OBI-1 in place of HYATE:C at a dose about as little as 10-20 U/kg of body wt in excess of the neutralizing dose. If a hemophilia A patient has an inhibitory antibody against A/Ill, it would require more OBI to neutralize the inhibitory antibodies.
- OBI-1 can be administered in a fraction of the volume of solution required for administering a dose of HYATE:C, not only because OBI-1 can be prepared in more concentrated form, but also because a smaller dose of OBI-1 can yield a recovery of activity comparable to a 2 to 6 fold higher dose of HYATE:C.
- HYATE:C required a median of eight infusions to halt a single bleeding episode over a two day period
- OBI-1 may require only 1-4 such infusions, a dramatic advance in patient treatment.
- OBI-1 dosage can bring about more rapid control of bleeding and therefore is likely both more effective and safer than Hyate:C. It is also advantageous for patient comfort and quality of life, as well as providing a reduced risk of infection and of side effects from contaminants. Therapeutic levels of A/Ill can be achieved more rapidly by infusing the concentrated OBI-1 product.
- Another aspect of the invention provides a therapeutic protocol that includes a step of measuring OBI-1 recovery as part of the process for establishing an optimal dose in an individual patient.
- OBI-1 recovery can be measured essentially as described in Example 5, by adding a measured amount of OBI-1 activity to a sample of a patient's plasma, then measuring the activity recovered from the sample after a short time interval. A series of such tests can establish an OBI-1 dose suitable for each patient. Alternatively, individual recovery data can be measured directly in a patient.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- General Health & Medical Sciences (AREA)
- Veterinary Medicine (AREA)
- Medicinal Chemistry (AREA)
- Public Health (AREA)
- Pharmacology & Pharmacy (AREA)
- Animal Behavior & Ethology (AREA)
- Epidemiology (AREA)
- Engineering & Computer Science (AREA)
- Bioinformatics & Cheminformatics (AREA)
- General Chemical & Material Sciences (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Oil, Petroleum & Natural Gas (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Immunology (AREA)
- Hematology (AREA)
- Gastroenterology & Hepatology (AREA)
- Dermatology (AREA)
- Zoology (AREA)
- Organic Chemistry (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Mycology (AREA)
- Biochemistry (AREA)
- Molecular Biology (AREA)
- Microbiology (AREA)
- Inorganic Chemistry (AREA)
- Diabetes (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
- Medicines Containing Material From Animals Or Micro-Organisms (AREA)
- Peptides Or Proteins (AREA)
- Medicinal Preparation (AREA)
Abstract
Description








Claims
Priority Applications (12)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2007511442A JP2007536230A (en) | 2004-05-03 | 2005-04-28 | Method for administering porcine B domain deficient fVIII |
| ES05740319.8T ES2449044T3 (en) | 2004-05-03 | 2005-04-28 | Administration procedure of fVIII without porcine B domain |
| EP05740319.8A EP1750733B1 (en) | 2004-05-03 | 2005-04-28 | METHOD OF ADMINISTERING PORCINE B-DOMAINLESS fVIII |
| PL05740319T PL1750733T3 (en) | 2004-05-03 | 2005-04-28 | METHOD OF ADMINISTERING PORCINE B-DOMAINLESS fVIII |
| SI200531828T SI1750733T1 (en) | 2004-05-03 | 2005-04-28 | METHOD OF ADMINISTERING PORCINE B-DOMAINLESS fVIII |
| HK07108636.6A HK1100900B (en) | 2004-05-03 | 2005-04-28 | Method of administering porcine b-domainless fviii |
| DK05740319.8T DK1750733T3 (en) | 2004-05-03 | 2005-04-28 | PROCEDURE FOR SUBMITTING PIG-B DOMAIN WITHOUT VVIII |
| US11/549,049 US7576181B2 (en) | 2004-05-03 | 2006-10-12 | Method of administering porcine B-domainless fVIII |
| US12/496,516 US8101718B2 (en) | 2004-05-03 | 2009-07-01 | Methods of administering porcine B-domainless fVIII |
| US13/356,437 US8501694B2 (en) | 2004-05-03 | 2012-01-23 | Method of administering porcine B-domainless fVIII |
| US13/959,523 US20140193441A1 (en) | 2004-05-03 | 2013-08-05 | Method of Administering Porcine B-domainless fVIII |
| US15/179,343 US20170119857A1 (en) | 2004-05-03 | 2016-06-10 | Method of Administering Porcine B-Domainless fVIII |
Applications Claiming Priority (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US56801504P | 2004-05-03 | 2004-05-03 | |
| US60/568,015 | 2004-05-03 | ||
| US56900004P | 2004-05-07 | 2004-05-07 | |
| US60/569,000 | 2004-05-07 |
Related Child Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| US11/549,049 Continuation-In-Part US7576181B2 (en) | 2004-05-03 | 2006-10-12 | Method of administering porcine B-domainless fVIII |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2005107776A1 true WO2005107776A1 (en) | 2005-11-17 |
Family
ID=35320037
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2005/014760 Ceased WO2005107776A1 (en) | 2004-05-03 | 2005-04-28 | METHOD OF ADMINISTERING PORCINE B-DOMAINLESS fVIII |
Country Status (10)
| Country | Link |
|---|---|
| US (5) | US7576181B2 (en) |
| EP (1) | EP1750733B1 (en) |
| JP (1) | JP2007536230A (en) |
| CY (1) | CY1114809T1 (en) |
| DK (1) | DK1750733T3 (en) |
| ES (1) | ES2449044T3 (en) |
| PL (1) | PL1750733T3 (en) |
| PT (1) | PT1750733E (en) |
| SI (1) | SI1750733T1 (en) |
| WO (1) | WO2005107776A1 (en) |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US7560107B2 (en) | 1996-06-26 | 2009-07-14 | Emory University | Modified factor VIII |
| US7576181B2 (en) | 2004-05-03 | 2009-08-18 | Ipsen Biopharm Limited | Method of administering porcine B-domainless fVIII |
| US8623824B2 (en) | 2007-02-23 | 2014-01-07 | Biomethodes | VIII factors for the treatment of type A hemophilia |
| US9150637B2 (en) | 2010-11-05 | 2015-10-06 | Baxalta Inc. | Variant of antihemophilic factor VIII having increased specific activity |
Families Citing this family (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10654911B1 (en) | 2019-04-02 | 2020-05-19 | Beijing Neoletix Biological Technology Co., Ltd. | Vector co-expressing truncated von Willebrand factor and factor VIII |
Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US6458563B1 (en) * | 1996-06-26 | 2002-10-01 | Emory University | Modified factor VIII |
| WO2003080108A1 (en) * | 2002-03-26 | 2003-10-02 | Societe De Conseils De Recherches Et D'applications Scientifiques (S.C.R.A.S.) | Stable pharmaceutical composition containing factor viii |
Family Cites Families (37)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4348384A (en) * | 1980-10-17 | 1982-09-07 | Dainippon Pharmaceutical Co., Ltd. | Pharmaceutical composition for oral administration containing coagulation factor VIII or IX |
| US4757006A (en) * | 1983-10-28 | 1988-07-12 | Genetics Institute, Inc. | Human factor VIII:C gene and recombinant methods for production |
| EP0182448A3 (en) | 1984-08-24 | 1987-10-28 | Genetics Institute, Inc. | Production of factor viii and related products |
| ATE72838T1 (en) * | 1985-04-12 | 1992-03-15 | Genetics Inst | NEW PROCOAGULATION PROTEINS. |
| JPH0387173A (en) | 1987-09-10 | 1991-04-11 | Teijin Ltd | Preparation of human active natural type factor viii c and transformant using the same |
| US5605884A (en) * | 1987-10-29 | 1997-02-25 | Rhone-Poulenc Rorer Pharmaceuticals Inc. | Factor VIII formulations in high ionic strength media |
| WO1989009784A1 (en) | 1988-04-08 | 1989-10-19 | Commonwealth Serum Laboratories Commission | Production of heat-stable factor viii concentrate |
| DK162233C (en) | 1989-11-09 | 1992-03-16 | Novo Nordisk As | PROCEDURE FOR INSULATING FACTOR VIII FROM BLOOD PLASMA AND PHARMACEUTICAL PREPARATION CONTAINING THE ASSOCIATED PHATAR VIII |
| DE4111393A1 (en) * | 1991-04-09 | 1992-10-15 | Behringwerke Ag | STABILIZED FACTOR VIII PREPARATIONS |
| US5888974A (en) * | 1992-04-07 | 1999-03-30 | Emory University | Hybrid human/animal factor VIII |
| US5744446A (en) * | 1992-04-07 | 1998-04-28 | Emory University | Hybrid human/animal factor VIII |
| US6180371B1 (en) | 1996-06-26 | 2001-01-30 | Emory University | Modified factor VIII |
| US5364771A (en) * | 1992-04-07 | 1994-11-15 | Emory University | Hybrid human/porcine factor VIII |
| US6376463B1 (en) * | 1992-04-07 | 2002-04-23 | Emory University | Modified factor VIII |
| US5663060A (en) * | 1992-04-07 | 1997-09-02 | Emory University | Hybrid human/animal factor VIII |
| US5859204A (en) * | 1992-04-07 | 1999-01-12 | Emory University | Modified factor VIII |
| DE69329795T2 (en) * | 1992-10-02 | 2001-07-05 | Genetics Institute, Inc. | COMPOSITION CONTAINING COAGULATION FACTOR VIII; METHOD FOR THE PRODUCTION THEREOF AND THE USE OF A SURFACE-ACTIVE SUBSTANCE AS A STABILIZER |
| US5563045A (en) | 1992-11-13 | 1996-10-08 | Genetics Institute, Inc. | Chimeric procoagulant proteins |
| US5348384A (en) * | 1992-12-31 | 1994-09-20 | Hull Harold L | Apparatus for supporting a title counter cap |
| SE9301581D0 (en) * | 1993-05-07 | 1993-05-07 | Kabi Pharmacia Ab | PROTEIN FORMULATION |
| CA2162497A1 (en) * | 1993-06-10 | 1994-12-22 | Sheila Connelly | Adenoviral vectors for treatment of hemophilia |
| SE504074C2 (en) * | 1993-07-05 | 1996-11-04 | Pharmacia Ab | Protein preparation for subcutaneous, intramuscular or intradermal administration |
| IL113010A0 (en) * | 1994-03-31 | 1995-10-31 | Pharmacia Ab | Pharmaceutical formulation comprising factor VIII or factor ix with an activity of at least 200 IU/ml and an enhancer for improved subcutaneous intramuscular or intradermal administration |
| US6818439B1 (en) * | 1994-12-30 | 2004-11-16 | Chiron Corporation | Methods for administration of recombinant gene delivery vehicles for treatment of hemophilia and other disorders |
| AU6291896A (en) | 1995-07-11 | 1997-02-10 | Chiron Corporation | Novel factor viii:c polypeptide analogs comprising factor v domains or subdomains |
| WO1997003193A1 (en) | 1995-07-11 | 1997-01-30 | Chiron Corporation | Novel factor viii:c polypeptide analogs with altered metal-binding properties |
| US7560107B2 (en) * | 1996-06-26 | 2009-07-14 | Emory University | Modified factor VIII |
| US5763401A (en) * | 1996-07-12 | 1998-06-09 | Bayer Corporation | Stabilized albumin-free recombinant factor VIII preparation having a low sugar content |
| WO1999029848A1 (en) | 1997-12-05 | 1999-06-17 | The Immune Response Corporation | Novel vectors and genes exhibiting increased expression |
| US6200560B1 (en) * | 1998-10-20 | 2001-03-13 | Avigen, Inc. | Adeno-associated virus vectors for expression of factor VIII by target cells |
| US6759216B1 (en) * | 1998-11-06 | 2004-07-06 | Emory University | Glycosylated, low antigenicity low immunogenicity factor VIII |
| KR100638184B1 (en) * | 2000-09-19 | 2006-10-26 | 에모리 유니버시티 | Modified Factor Ⅷ |
| WO2003031598A2 (en) * | 2001-10-05 | 2003-04-17 | Emory University | Nucleic acid and amino acid sequences encoding high-level expressor factor viii polypeptides and methods of use |
| AU2002364509A1 (en) * | 2001-11-30 | 2003-06-17 | Emory University | Factor viii c2 domain variants |
| US7105745B2 (en) * | 2002-12-31 | 2006-09-12 | Thomas & Betts International, Inc. | Water resistant electrical floor box cover assembly |
| US20050123997A1 (en) * | 2003-10-30 | 2005-06-09 | Lollar John S. | Modified fVIII having reduced immunogenicity through mutagenesis of A2 and C2 epitopes |
| SI1750733T1 (en) * | 2004-05-03 | 2014-03-31 | Emory University | METHOD OF ADMINISTERING PORCINE B-DOMAINLESS fVIII |
-
2005
- 2005-04-28 SI SI200531828T patent/SI1750733T1/en unknown
- 2005-04-28 ES ES05740319.8T patent/ES2449044T3/en not_active Expired - Lifetime
- 2005-04-28 PT PT57403198T patent/PT1750733E/en unknown
- 2005-04-28 JP JP2007511442A patent/JP2007536230A/en active Pending
- 2005-04-28 EP EP05740319.8A patent/EP1750733B1/en not_active Expired - Lifetime
- 2005-04-28 WO PCT/US2005/014760 patent/WO2005107776A1/en not_active Ceased
- 2005-04-28 DK DK05740319.8T patent/DK1750733T3/en active
- 2005-04-28 PL PL05740319T patent/PL1750733T3/en unknown
-
2006
- 2006-10-12 US US11/549,049 patent/US7576181B2/en not_active Expired - Lifetime
-
2009
- 2009-07-01 US US12/496,516 patent/US8101718B2/en not_active Expired - Lifetime
-
2012
- 2012-01-23 US US13/356,437 patent/US8501694B2/en not_active Expired - Lifetime
-
2013
- 2013-08-05 US US13/959,523 patent/US20140193441A1/en not_active Abandoned
-
2014
- 2014-02-05 CY CY20141100088T patent/CY1114809T1/en unknown
-
2016
- 2016-06-10 US US15/179,343 patent/US20170119857A1/en not_active Abandoned
Patent Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US6458563B1 (en) * | 1996-06-26 | 2002-10-01 | Emory University | Modified factor VIII |
| WO2003080108A1 (en) * | 2002-03-26 | 2003-10-02 | Societe De Conseils De Recherches Et D'applications Scientifiques (S.C.R.A.S.) | Stable pharmaceutical composition containing factor viii |
Non-Patent Citations (3)
| Title |
|---|
| PARKER E.T ET AL: "Comparative Immunogeneticity of Recombinant B Domain-deleted Porcine Factor VIIIand Hyate: C in Hemophilia A Mice Presensitized to Human Factor VIII", J. THROMBOSIS AND HAEMOSTASIS, vol. 2, April 2004 (2004-04-01), pages 605 - 611, XP002992201 * |
| PARKER E.T. ET AL: "Comparative Immunogenicity of Recombinant B Domain-deleted Porcine Factor VIII and Hyate: C in Hemophilia A Mice Presensitized to Human Factor VIII", J. BLOOD, vol. 102, no. 11, 16 November 2003 (2003-11-16), pages 798A, XP008054758 * |
| See also references of EP1750733A4 * |
Cited By (8)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US7560107B2 (en) | 1996-06-26 | 2009-07-14 | Emory University | Modified factor VIII |
| US8951515B2 (en) | 1996-06-26 | 2015-02-10 | Emory University | Modified factor VIII |
| US7576181B2 (en) | 2004-05-03 | 2009-08-18 | Ipsen Biopharm Limited | Method of administering porcine B-domainless fVIII |
| US8101718B2 (en) | 2004-05-03 | 2012-01-24 | Emory University | Methods of administering porcine B-domainless fVIII |
| US8501694B2 (en) | 2004-05-03 | 2013-08-06 | Emory University | Method of administering porcine B-domainless fVIII |
| US8623824B2 (en) | 2007-02-23 | 2014-01-07 | Biomethodes | VIII factors for the treatment of type A hemophilia |
| US9150637B2 (en) | 2010-11-05 | 2015-10-06 | Baxalta Inc. | Variant of antihemophilic factor VIII having increased specific activity |
| US10053500B2 (en) | 2010-11-05 | 2018-08-21 | Baxalta Incorporated | Variant of antihemophilic factor VIII having increased specific activity |
Also Published As
| Publication number | Publication date |
|---|---|
| EP1750733B1 (en) | 2013-12-11 |
| SI1750733T1 (en) | 2014-03-31 |
| US8501694B2 (en) | 2013-08-06 |
| US20090270329A1 (en) | 2009-10-29 |
| EP1750733A1 (en) | 2007-02-14 |
| HK1100900A1 (en) | 2007-10-05 |
| EP1750733A4 (en) | 2009-06-17 |
| US8101718B2 (en) | 2012-01-24 |
| ES2449044T3 (en) | 2014-03-18 |
| US20120270788A1 (en) | 2012-10-25 |
| CY1114809T1 (en) | 2016-12-14 |
| US20070173446A1 (en) | 2007-07-26 |
| US7576181B2 (en) | 2009-08-18 |
| US20170119857A1 (en) | 2017-05-04 |
| JP2007536230A (en) | 2007-12-13 |
| US20140193441A1 (en) | 2014-07-10 |
| PL1750733T3 (en) | 2014-05-30 |
| DK1750733T3 (en) | 2014-01-20 |
| PT1750733E (en) | 2014-02-14 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| CA2742328C (en) | Factor viii formulations | |
| EP1016673A1 (en) | Composition comprising coagulation factor VIII formulation, process for its preparation and use of a surfactant as stabilizer | |
| JP2007262090A (en) | Highly concentrated, lyophilized, and liquid factor ix formulation | |
| JP2018505209A (en) | Pharmaceutical composition containing plasminogen and use thereof | |
| US20170119857A1 (en) | Method of Administering Porcine B-Domainless fVIII | |
| US12016904B2 (en) | Treatment of gastrointestinal bleeding in patients with severe von Willebrand disease by administration of recombinant VWF | |
| NO324064B1 (en) | Pharmaceutical composition comprising vWF propeptide and method of preparation and use thereof | |
| WO2023246680A1 (en) | Activators of coagulation factor x and formulations thereof for treating bleeding disorders | |
| JP2026500069A (en) | Formulations Comprising ActRIIA Protein Variants | |
| HK1100900B (en) | Method of administering porcine b-domainless fviii | |
| RU2774720C2 (en) | TREATMENT OF GASTROINTESTINAL BLEEDING IN PATIENTS WITH SEVERE VON WILLEBRAND DISEASE BY ADMINISTRATION OF RECOMBINANT vWF | |
| HK40115617A (en) | Treatment of gastrointestinal bleeding in patients with severe von willebrand disease by administration of recombinant vwf | |
| AU677797C (en) | Composition comprising coagulation factor viii formulation, process for its preparation and use of a surfactant as stabilizer | |
| HK40029176B (en) | Treatment of gastrointestinal bleeding in patients with severe von willebrand disease by administration of recombinant vwf | |
| HK40029176A (en) | Treatment of gastrointestinal bleeding in patients with severe von willebrand disease by administration of recombinant vwf | |
| PL175177B1 (en) | A pharmaceutical composition containing recombinant coagulation factor VIII I54) and a method of producing a pharmaceutical composition containing recombinant coagulation factor VIII |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| AK | Designated states |
Kind code of ref document: A1 Designated state(s): AE AG AL AM AT AU AZ BA BB BG BR BW BY BZ CA CH CN CO CR CU CZ DE DK DM DZ EC EE EG ES FI GB GD GE GH GM HR HU ID IL IN IS JP KE KG KM KP KR KZ LC LK LR LS LT LU LV MA MD MG MK MN MW MX MZ NA NI NO NZ OM PG PH PL PT RO RU SC SD SE SG SK SL SM SY TJ TM TN TR TT TZ UA UG US UZ VC VN YU ZA ZM ZW |
|
| AL | Designated countries for regional patents |
Kind code of ref document: A1 Designated state(s): BW GH GM KE LS MW MZ NA SD SL SZ TZ UG ZM ZW AM AZ BY KG KZ MD RU TJ TM AT BE BG CH CY CZ DE DK EE ES FI FR GB GR HU IE IS IT LT LU MC NL PL PT RO SE SI SK TR BF BJ CF CG CI CM GA GN GQ GW ML MR NE SN TD TG |
|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application | ||
| WWE | Wipo information: entry into national phase |
Ref document number: 11549049 Country of ref document: US |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2007511442 Country of ref document: JP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| WWW | Wipo information: withdrawn in national office |
Country of ref document: DE |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2005740319 Country of ref document: EP |
|
| WWP | Wipo information: published in national office |
Ref document number: 2005740319 Country of ref document: EP |
|
| WWP | Wipo information: published in national office |
Ref document number: 11549049 Country of ref document: US |