WO2022270099A1 - コレステロールリスク推定装置、コレステロールリスク推定方法及びプログラム - Google Patents
コレステロールリスク推定装置、コレステロールリスク推定方法及びプログラム Download PDFInfo
- Publication number
- WO2022270099A1 WO2022270099A1 PCT/JP2022/015093 JP2022015093W WO2022270099A1 WO 2022270099 A1 WO2022270099 A1 WO 2022270099A1 JP 2022015093 W JP2022015093 W JP 2022015093W WO 2022270099 A1 WO2022270099 A1 WO 2022270099A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- cholesterol
- risk
- cholesterol risk
- risk estimation
- information
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Images








Classifications
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H50/00—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics
- G16H50/30—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics for calculating health indices; for individual health risk assessment
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/145—Measuring characteristics of blood in vivo, e.g. gas concentration or pH-value ; Measuring characteristics of body fluids or tissues, e.g. interstitial fluid or cerebral tissue
- A61B5/14542—Measuring characteristics of blood in vivo, e.g. gas concentration or pH-value ; Measuring characteristics of body fluids or tissues, e.g. interstitial fluid or cerebral tissue for measuring blood gases
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/145—Measuring characteristics of blood in vivo, e.g. gas concentration or pH-value ; Measuring characteristics of body fluids or tissues, e.g. interstitial fluid or cerebral tissue
- A61B5/14546—Measuring characteristics of blood in vivo, e.g. gas concentration or pH-value ; Measuring characteristics of body fluids or tissues, e.g. interstitial fluid or cerebral tissue for measuring analytes not otherwise provided for, e.g. ions, cytochromes
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/145—Measuring characteristics of blood in vivo, e.g. gas concentration or pH-value ; Measuring characteristics of body fluids or tissues, e.g. interstitial fluid or cerebral tissue
- A61B5/1455—Measuring characteristics of blood in vivo, e.g. gas concentration or pH-value ; Measuring characteristics of body fluids or tissues, e.g. interstitial fluid or cerebral tissue using optical sensors, e.g. spectral photometrical oximeters
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/72—Signal processing specially adapted for physiological signals or for diagnostic purposes
- A61B5/7221—Determining signal validity, reliability or quality
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/72—Signal processing specially adapted for physiological signals or for diagnostic purposes
- A61B5/7235—Details of waveform analysis
- A61B5/7264—Classification of physiological signals or data, e.g. using neural networks, statistical classifiers, expert systems or fuzzy systems
- A61B5/7267—Classification of physiological signals or data, e.g. using neural networks, statistical classifiers, expert systems or fuzzy systems involving training the classification device
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/72—Signal processing specially adapted for physiological signals or for diagnostic purposes
- A61B5/7271—Specific aspects of physiological measurement analysis
- A61B5/7275—Determining trends in physiological measurement data; Predicting development of a medical condition based on physiological measurements, e.g. determining a risk factor
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H50/00—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics
- G16H50/20—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics for computer-aided diagnosis, e.g. based on medical expert systems
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H50/00—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics
- G16H50/70—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics for mining of medical data, e.g. analysing previous cases of other patients
Definitions
- the present invention relates to a cholesterol risk estimation device, a cholesterol risk estimation method and a program.
- Lipoproteins contained in blood can be classified into four types: chylomicrons, VLDL (Very Low Density Lipoprotein), LDL (Low Density Lipoprotein) cholesterol, and HDL (High Density Lipoprotein) cholesterol.
- HDL cholesterol is also called good cholesterol, and it is generally known that a lack of HDL cholesterol in the blood increases the risk of diseases such as arteriosclerosis. According to the criteria for blood tests established by the Society of Ningen Dock, if HDL cholesterol is 40 mg/dL or more, there is no abnormality, and if it is less than 40 mg/dL, it is determined that there is a risk.
- LDL cholesterol is also called bad cholesterol, and it is generally known that a large amount of LDL cholesterol in the blood increases the risk of diseases such as arteriosclerosis. According to the blood test criteria established by the Ningen Dock Society, if the LDL cholesterol is less than 120 mg/dL, there is no abnormality, and if it is 120 mg/dL or more, it is determined that there is a risk.
- Patent Document 1 A method described in Patent Document 1 is known as a noninvasive method for measuring lipids as whole lipoproteins.
- Patent Document 1 cannot estimate the concentration for each type of lipoprotein such as LDL and HDL, and whether or not there is a risk to health for each of LDL cholesterol and HDL cholesterol. It was difficult to make a determination of
- the present invention has been made in view of the circumstances as described above, and an object of the present invention is to estimate the risk of cholesterol, that is, LDL cholesterol or HDL cholesterol, to health from non-invasive biological information with extremely high accuracy. to provide a cholesterol risk estimation device, a cholesterol risk estimation method, and a program.
- a cholesterol risk estimation device includes an information acquisition unit that acquires predetermined user attribute information and non-invasive biological information, an estimation model storage unit that stores a cholesterol risk estimation model, and a cholesterol risk estimation model. and an estimation processor that calculates an estimated cholesterol risk value for a given user based on the given user's attribute information and/or non-invasive biometric information.
- the cholesterol risk estimation device is characterized by further comprising a training data storage unit that stores a training data set, and a learning processing unit that generates a cholesterol risk estimation model by machine learning based on the training data set.
- the attribute information includes age and sex, or a combination thereof
- the non-invasive biometric information includes BMI, blood pressure, pulse wave data, electrocardiogram data, bioimpedance, or a combination thereof.
- the training dataset is characterized by including subject's attribute information, non-invasive biological information, and cholesterol measurement values measured from blood.
- the noninvasive biological information is characterized by further including oxygen saturation (SpO2).
- the estimation accuracy of the cholesterol risk estimate is characterized by the accuracy with which the presence or absence of risk can be classified with an ROC_AUC of 0.7 or more.
- the learning processing unit adds a label indicating the presence or absence of cholesterol risk based on the cholesterol measurement value measured from blood, and in the label, the number of cholesterol risk and the number of no cholesterol risk. It is characterized by increasing the sample data in the training data set so as to reduce the difference if the difference is equal to or greater than a predetermined value.
- the learning processing unit generates a first cholesterol risk estimation model and a second cholesterol risk estimation model by machine learning, respectively, based on different types of training data sets, and the estimation processing unit generates the first cholesterol risk estimation model and the second A cholesterol risk estimation model is used to calculate a cholesterol risk estimate for a given user.
- a biological information estimator for estimating at least one biological information selected from BMI, blood pressure, pulse wave data, electrocardiogram data, biological impedance, and oxygen saturation included in the biological information;
- the biometric information estimated by the estimation unit is obtained as the biometric information of the predetermined user.
- the cholesterol risk estimating device In addition to the cholesterol risk estimating device, it is characterized by further comprising a biological information measuring device that measures noninvasive biological information to constitute a noninvasive cholesterol risk estimating system.
- the method for estimating cholesterol risk in the present invention includes steps of storing a training data set including attribute information of a subject, noninvasive biological information, and cholesterol measured values measured from blood, and performing machine learning based on the training data set. and using the cholesterol risk estimation model to calculate a cholesterol risk estimate for a given user based on demographic information and/or non-invasive biometric information of the given user. characterized by comprising
- the program in the present invention comprises steps of storing a training data set including attribute information of a subject, non-invasive biological information, and cholesterol measurement values measured from blood; generating an estimation model; and using the cholesterol risk estimation model to calculate a cholesterol risk estimate for a given user based on demographic information and/or non-invasive biometric information of the given user. It is characterized by executing
- a cholesterol risk estimating device capable of extremely accurately estimating the health risk of cholesterol, that is, LDL cholesterol or HDL cholesterol, by machine learning using non-invasive biological information, cholesterol risk. It is to provide an estimation method and program.
- FIG. 1 is a block diagram showing a schematic configuration of a cholesterol risk estimation system; FIG. It is a figure for demonstrating ESG (Electroscangram). It is a hardware block diagram of a cholesterol risk estimation apparatus.
- 4 is a flow chart showing a procedure for generating an LDL cholesterol risk estimation model by machine learning; 4 is a flow chart showing an execution procedure of LDL cholesterol risk estimation processing; 4 is a flow chart showing a procedure for generating an HDL cholesterol risk estimation model by machine learning;
- FIG. 10 is a flow chart showing an execution procedure of HDL cholesterol risk estimation processing;
- FIG. 4 is an ROC_AUC curve of estimation results in Example 1.
- FIG. 10 is an ROC_AUC curve of estimation results in Example 2.
- FIG. 10 is a ROC_AUC curve of estimation results in Example 3.
- FIG. 10 is an ROC_AUC curve of estimation results in Example 1.
- FIG. 1 is a block diagram showing a schematic configuration of a cholesterol risk estimation system 1 according to this embodiment.
- the cholesterol risk estimation system 1 includes a terminal device 10 , a biological information measurement device 20 , a cholesterol risk estimation device 30 and a display device 39 .
- a "user” refers to a person who uses the cholesterol risk estimation system to non-invasively obtain an estimate of cholesterol risk.
- subjects are used in the cholesterol risk estimation system after obtaining prescribed procedures and consent, attribute information such as age and gender, non-invasive biological information, and cholesterol measured from blood.
- the terminal device 10 is an information terminal capable of inputting user attribute information (name, ID, age, gender, etc.) and outputting the input information to the cholesterol risk estimation device 30 via a wired or wireless communication network.
- Any information terminal may be used as long as it is. Examples include tablet terminals, smart phones, mobile terminals including wearable terminals, and PCs (Personal Computers).
- the height, weight, and the like may be measured by the biological information measuring device 20, which will be described later.
- the biological information measuring device 20 measures the user's non-invasive biological information.
- non-invasive biometric information is biometric information obtained by a method that does not require the insertion of instruments into the skin or into body orifices.
- Non-invasive biological information can be measured using commercially available stature scales, weight scales, sphygmomanometers, pulse oximeters, pulse wave meters, electrocardiographs, impedance measuring devices, galvanic skin measuring devices, and the like.
- ESTEC BC-3 which can simultaneously measure pulse wave data, electrocardiogram data, bioimpedance, and oxygen saturation (SpO2), can also be used. These devices can noninvasively measure biometric data without imposing a psychological or physical burden on the user.
- the non-invasive biological information includes BMI (body mass index), blood pressure, pulse wave data, electrocardiogram data, and bioimpedance, or a combination thereof, and oxygen saturation (SpO2 ) may be included.
- Pulse wave data is obtained by irradiating red light ( ⁇ 660 nm) from a Red LED and near-infrared light ( ⁇ 905 nm) from an IR LED to a protruding part of the body, such as a finger, using a pulse wave meter or pulse oximeter. is obtained by measuring the phototransistor.
- Pulse wave data include pulse, elastic index, peripheral vascular resistance, accelerogram, b/a, e/a, -d/a, Takazawa accelerometer aging index, ejection fraction, LVET, DEI elastic index), or a combination thereof.
- the elastic index is a numerical value obtained by dividing the height by the time from the systolic peak to the diastolic peak detected in the finger plethysmogram.
- Peripheral vascular resistance is determined by mean arterial pressure/cardiac output ⁇ 80.
- DEI depleted elastic index
- 0.3 to 0.7 is normal, 0.3 or less suggests hypertension or arteriosclerosis, and 0.7 or more suggests acute anxiety.
- the acceleration pulse wave is a second derivative of photoplethysmogram (SDPTG) of finger plethysmogram (photoplethysmogram: PTG).
- Acceleration pulse wave includes early positive wave (a-wave), early negative wave (b-wave), mid-systolic re-rising wave (c-wave), late-systolic re-descending wave (d-wave), and diastolic early positive wave (e-wave).
- the above b/a, e/a, and -d/a are calculated from the ratio of each wave height.
- vascular aging is evaluated using the Takazawa acceleration pulse wave aging index (bcde)/a. be able to.
- Ejection fraction is the fraction of blood ejected from the ventricle with each heartbeat and is proportional to the Accelerometer Plethysmographic Aging Index.
- LVET is Left Ventricular Ejection Time, the time for blood in the left ventricle to be ejected into the aorta after the aortic valve opens.
- Electrocardiogram data can be measured by electrode electrocardiography (ECG) or photoplethysmography (PPG).
- ECG data includes respiratory rate, heart rate, RR interval, standard deviation of RR interval, MxDMn ratio, power spectrum of low frequency band, power spectrum of high frequency band, heart rate variability index LF/HF, total power, or combinations thereof.
- the RR interval is the interval from one QRS wave to the next QRS wave in an electrocardiogram.
- the MxDMn ratio is the ratio of the longest RR interval to the shortest RR interval in time and is an index of irregular heartbeats.
- the total power is the calculated value of the total power of the power spectrum of frequencies 0 to 0.4 Hz (VLF, LF, HF) measured for 2 minutes.
- This value reflects the total autonomic nervous system activity dominated by sympathetic activity.
- the high frequency power spectral ratio (0.1875 to 0.50 Hz: HF)
- the low frequency power spectral ratio (0.05 to 0.1875 Hz: LF)
- the LF/HF ratio the power spectrum ratio of the very low frequency band (0-0.05 Hz: VLF)
- the impedance (conductance) of a living body can be measured, for example, by passing weak electricity between two of the six electrodes on both legs, both hands, and left and right forehead.
- ⁇ S anode/cathode conductance
- ⁇ S cathode/anode conductance
- ⁇ S/m electrical conductivity
- muscle mass, body fat mass, total water content, phase angle, and resistance value can be measured at the same time.
- the dielectric constant ( ⁇ Si) when the current is applied between the right hand and the left hand and between the right forehead and the left forehead is also possible. It is preferable to measure the impedance (conductance) of the living body using 22 patterns of conductivity from six electrodes.
- Bioimpedance includes body fat mass (kg), body fat mass (%), lean mass, lean mass, muscle mass, total water content (kg), total water content (%), intracellular water content (% ), cardiac output, 1 left forehead-2 left hand/SCR A, 1 left left-2 left hand/delta SCR C-SCR A, 5 left hand-6 left foot/SCR A, 5 left hand-6 left foot/delta SCR C- SCR A, 13 left foot - 14 right foot / SCR C, 13 left foot - 14 right foot / SCR A, 15 right hand - 16 left forehead / Delta SCR C - SCR A, 15 right hand - 16 left forehead SCR C, 19 right foot - 20 left hand / Delta SCR C-SCR A, ESG2+4+15+17 ( ⁇ S/m), ESG6+13+19 (%), ESG 6+8+19+21 (%), ESG6+8+19+21 ( ⁇ S/m), ESG 9+10 ( ⁇ S/m), ESG9+10
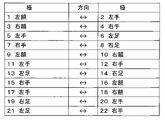
- ESG is an abbreviation for electroscangram.
- the "+" in ESG2+4+15+17 means which electrode attached to the body was used to measure.
- ESG 2 + 4 + 15 + 17, as shown in Fig. 2 is the left hand when electricity is applied from the left hand to the left forehead, the right hand when electricity is applied from the right hand to the right forehead, the right hand when electricity is applied from the right hand to the left forehead, and the left hand to the right forehead. It means the average value of the conductance measured with the left hand when the current is applied.
- Non-Patent Document 1 has a detailed description of these conductances.
- Non-Patent Documents 2 and 3 The details of the ESG (electroscangram) measurement method are described in Non-Patent Documents 2 and 3.
- “1 left side -2 left hand/SCR A” is the conductance (or conductivity) of the path measured when electricity flows so that "1 left side” is the cathode and "2 left hand” is the anode direction.
- “5 left hand - 6 left foot / delta SCR C-SCR A” is the difference in conductance measured when current is applied between "5 left hand” and "6 left foot” so that anode-cathode, cathode-anode. be.
- BMI and blood pressure can be measured using a height weight scale and a blood pressure monitor.
- the non-invasive biological information may also include oxygen delivery calculated from SpO2 and cardiac output.
- the measured noninvasive biological information is output to the cholesterol risk estimation device 30 through a wired or wireless communication network.
- the biological information measuring device 20 may be a built-in measuring device or a portable measuring device such as a wearable terminal.
- the cholesterol risk estimation device 30 includes a first acquisition unit 31, a second acquisition unit 32, a user data storage unit 33, a training data storage unit 34, a learning processing unit 35, an estimation model storage unit 36, and an estimation process.
- a section 37 and an estimated data storage section 38 are provided.
- the first acquisition unit 31 acquires user attribute information from the terminal device 10 .
- the second acquisition unit 32 acquires non-invasive biological information of the user from the biological information measuring device 20 .
- the user data storage unit 33 stores user attribute information and non-invasive biological information acquired from the first acquisition unit 31 and the second acquisition unit 32 .
- the training data storage unit 34 stores, as a training data set for machine learning, attribute information of a plurality of subjects acquired in advance, non-invasive biological information, and cholesterol obtained from blood tests (LDL cholesterol or HDL cholesterol ) are stored.
- the specimen test information may further include test information obtained from blood, urine, stool, and the like.
- the learning processing unit 35 acquires the training data set stored in the training data storage unit 34 and creates a cholesterol risk estimation model using the training data set. Specifically, when estimating LDL cholesterol risk, machine learning using gradient boosting such as XGBoost is performed on the obtained training dataset to learn the relationship between attribute information and non-invasive biometric information and LDL cholesterol risk. In addition, when estimating HDL cholesterol risk, the obtained training data set is standardized or normalized, and the relationship between attribute information and non-invasive biometric information and HDL cholesterol risk is learned by machine learning using logistic regression.
- the estimated model storage unit 36 stores the cholesterol risk estimated model generated by the learning processing unit 35 .
- the non-invasive biometric information includes BMI, blood pressure, pulse wave data, electrocardiogram data, bioimpedance, or a combination thereof. Additionally, oxygen saturation (SpO2) is included as needed.
- the estimation processing unit 37 uses the estimation model generated by the learning processing unit 35 to estimate the user's cholesterol risk based on predetermined user attribute information and/or non-invasive biological information. The estimated cholesterol risk value is then stored in the estimated data storage unit 38 .
- the display device 39 can display the estimated cholesterol risk value together with the user's attribute information and non-invasive biological information. These data may be displayed on the terminal device 10 owned by the user.
- FIG. 3 is a hardware configuration diagram of the cholesterol risk estimation device 30.
- cholesterol risk estimation device 30 is configured by computer 300 having one or more processors 301 , memory 302 , storage 303 , input/output port 304 and communication port 305 .
- the processor 301 performs processing related to cholesterol estimation according to this embodiment by executing a program.
- the memory 302 temporarily stores programs and computation results of the programs.
- Storage 303 stores a program for executing processing by cholesterol risk estimation device 30 .
- the storage 303 may be of any kind as long as it is readable by a computer, for example, various recording media such as a recording medium (magnetic disk, optical disk, etc.), random access memory, flash type memory, read-only memory, etc. can be used.
- the input/output port 304 inputs information from the terminal device 10 and the biological information measuring device 20 and outputs estimated cholesterol values to the display device 39 .
- a communication port 305 transmits and receives data to and from an information terminal such as another computer (not shown). As a communication method, wireless communication or wired communication can be used.
- the cholesterol risk estimating device 30 can be implemented by a commercially available desktop PC or notebook PC, and it takes several seconds to calculate the cholesterol risk estimated value using the estimation model.
- the processor 301 of the cholesterol risk estimation device 30 the first acquisition unit 31, the second acquisition unit 32, the learning processing unit 35, the estimation processing unit 37, etc. function when operating.
- Cholesterol estimation model is generated by machine learning based on non-invasive biological data including BMI (body mass index), blood pressure, pulse wave data, electrocardiogram data, bioimpedance, etc. to estimate cholesterol without blood test. becomes possible. Moreover, as shown below, it is possible to determine whether or not cholesterol is normal even when the number of each data included in the noninvasive biological data is limited.
- BMI body mass index
- blood pressure blood pressure
- pulse wave data pulse wave data
- electrocardiogram data electrocardiogram data
- bioimpedance bioimpedance
- FIG. 4 is a flow chart showing a procedure for generating an LDL cholesterol risk estimation model by machine learning.
- the learning processing unit 35 preprocesses input data (for example, the training data set described above). Specifically, the learning processing unit 35 converts the LDL cholesterol obtained from the blood test to 0 (no risk) when the LDL cholesterol is less than 120 mg/dl and 1 (with risk) when the LDL cholesterol is 120 mg/dl or more. In addition, when the number of people classified as 0 and the number of people classified as 1 are unbalanced, the learning processing unit 35 applies SMOTE (Chawla, NV. et al.
- Training samples may be generated artificially. That is, in the input data (training data set), a label indicating the presence or absence of LDL cholesterol risk (for example, 0 or 1 described above) is added based on LDL cholesterol obtained by a blood test, and in the label, LDL cholesterol risk If the difference between the number of positive (label: 1) and the number of no LDL cholesterol risk (label: 0) is greater than or equal to a predetermined value, increase (generate) the sample data in the training dataset to reduce this difference ).
- the learning processing unit 35 performs machine learning using a gradient boosting decision tree.
- Machine learning using gradient boosted regression trees can use software libraries such as XGBoost, CatBoost, and LightBGM.
- the risk value (0: no risk, 1: risk) obtained by comparing the LDL cholesterol level obtained from a blood test with a predetermined threshold was compared with the LDL cholesterol risk value estimated by machine learning.
- each parameter of XGBoost max_depth, subsample, colsample_bytree, learning_rate
- max_depth is the depth of the decision tree
- subsample is the proportion of randomly sampled samples in each tree
- colsample_bytree is the proportion of randomly sampled columns in each tree
- learning_rate indicates the learning rate.
- the learning processing unit 35 stores the LDL cholesterol risk estimation model generated by the learning process described above in the estimation model storage unit 36 . It should be noted that the machine learning algorithms described above are merely examples, and the present invention is not limited to these.
- step ST201 the first acquisition unit 31 of the cholesterol risk estimation device 30 acquires user attribute information from the terminal device 10.
- step ST202 the second acquisition unit 32 of the cholesterol risk estimation device 30 acquires non-invasive biological information of the user. Then, the user's attribute information and non-invasive biological information are stored in the user data storage unit 33 .
- step ST203 using the LDL cholesterol risk estimation model stored in the estimation model storage unit 36, the estimation processing unit 37 determines the probability of belonging to class 0 (no risk) or class 1 (with risk), that is, LDL cholesterol. Calculate risk estimates.
- step ST204 the calculated LDL cholesterol risk estimated value is stored in the estimated data storage unit 38, and in step ST205, the LDL cholesterol risk estimated value is output to an external terminal such as the display device 39 for display.
- FIG. 6 is a flow chart showing a procedure for generating an HDL cholesterol risk estimation model by machine learning.
- the learning processing section 35 preprocesses the input data. Specifically, the learning processing unit 35 converts HDL cholesterol of 40 mg/dl or more into 0 (no risk) and less than 40 mg/dl of HDL cholesterol obtained by a blood test into 1 (with risk). In addition, when the number of people classified as 0 and the number of people classified as 1 are unbalanced, the learning processing unit 35 applies SMOTE (Chawla, NV. et al. 2002) to the learning data, Training samples may be generated artificially.
- SMOTE Chowla, NV. et al. 2002
- a label indicating the presence or absence of HDL cholesterol risk (e.g., 0 or 1 above) is added based on HDL cholesterol obtained by a blood test, and in the label, HDL cholesterol risk If the difference between the number of cases with HDL cholesterol risk (label: 1) and the number of cases without HDL cholesterol risk (label: 0) is greater than or equal to a predetermined value, increase (generate) the sample data in the training dataset to reduce this difference. ). Further standardize and normalize the data.
- the learning processing unit 35 performs machine learning by logistic regression.
- Logistic Regression provided by Scikit-learn, which is an open source machine learning library for Python, can be used. Also, if necessary, the number of dimensions may be compressed by principal component analysis.
- the risk value (0: no risk, 1: risk) obtained by comparing the HDL cholesterol level obtained from a blood test with a predetermined threshold was compared with the HDL cholesterol risk value estimated by machine learning.
- each parameter of Logistic Regression (C, regularization method, max_iter, solver) was adjusted to maximize the f1 score to generate an HDL cholesterol risk estimation model.
- C is a trade-off parameter that determines the strength of regularization, and the larger the value, the weaker the strength of regularization.
- Regularization method means L1 regularization or L2 regularization, which is selected.
- max_iter is the maximum number of iterations to learn.
- the solver chooses a convergence method (eg L-BFGS method, Newton CG method, liblinear, sag and saga) that minimizes the cross-entropy error. In Examples 2 and 3 below, the liblinear method was selected.
- the learning processing unit 35 stores the HDL cholesterol risk estimation model generated by the learning process described above in the estimation model storage unit 36 . It should be noted that the machine learning algorithms described above are merely examples, and the present invention is not limited to these.
- step ST401 the first acquisition unit 31 of the cholesterol risk estimation device 30 acquires user attribute information from the terminal device 10.
- step ST402 the second acquiring unit 32 of the cholesterol risk estimating device 30 acquires non-invasive biological information of the user. Then, the user's attribute information and non-invasive biological information are stored in the user data storage unit 33 . Then, in step ST403, using the HDL cholesterol risk estimation model stored in the estimation model storage unit 36, the estimation processing unit 37 determines the probability of belonging to class 0 (no risk) or class 1 (with risk), that is, HDL cholesterol. Calculate risk estimates.
- step ST404 the calculated HDL cholesterol risk estimated value is stored in the estimated data storage section 38, and in step ST405, the HDL cholesterol risk estimated value is output to an external terminal such as the display device 39 and displayed.
- LDL cholesterol risk estimation An example of LDL cholesterol risk estimation is described below.
- Attribute information includes ID, name, age, gender, or a combination thereof
- non-invasive biometric information includes BMI, blood pressure, pulse wave data, electrocardiogram data, bioimpedance, and oxygen saturation. (SpO2), or combinations thereof.
- Height and weight which are the criteria for calculating BMI, were measured using a height scale and weight scale, respectively, and blood pressure was measured using a sphygmomanometer.
- Pulse wave data, electrocardiogram data, bioimpedance, and oxygen saturation (SpO2) were measured with Estech BC-3 (Ryobi Systems).
- the non-invasive biometric information may be acquired using a predetermined wearable terminal.
- Bioimpedance (conductance) was measured by passing a weak electric current between two of six electrodes on both feet, both hands, and left and right forehead. The voltage and current were 1.28 V, 200 ⁇ A and the conductance was measured for 32 milliseconds per second. Current was applied to two of the six electrodes, and (1) anode/cathode conductance ( ⁇ S), (2) cathode/anode conductance ( ⁇ S), (3) conductance measured in (1) above.
- Estec BC-3 measured pulse wave data, electrocardiogram data, bioimpedance, and oxygen saturation (SpO2) for 2 minutes for each subject.
- a device equipped with electrocardiogram, pulse wave monitor, and pulse oximeter functions was attached to the subject's left index finger, and two electrodes were attached to the forehead. placed on top.
- ⁇ Learning model 1> In learning model 1, as shown in FIG. 4, machine learning was performed using a gradient boosting decision tree. At this time, the following data were selected and used as attribute information and non-invasive biological data.
- A Attribute information/Age
- B Non-invasive biological data
- Blood pressure diastolic blood pressure
- Pulse wave data elastic index
- Electrocardiogram data heart rate, standard deviation of RR interval Bioimpedance ⁇ Body fat mass (kg), muscle mass, total water content (%), cardiac output, 5 left hand-6 left leg/SCRA, ESG2+4+15+17 ( ⁇ S/m), ESG 9+10 ( ⁇ S/m), ESG9+10 (%), R ( ⁇ )
- ESG9+10 is the average impedance value measured at the site shown in FIG.
- the non-invasive biometric data further includes cardiac output included in bioimpedance and oxygen delivery estimated from oxygen saturation (SpO2).
- Example 1 In Example 1, (1) attribute information of 712 subjects, (2) height and weight scale, sphygmomanometer, and noninvasive biological information measured by Estech BC-3, and (3) noninvasive biological information measurement and An LDL cholesterol risk estimation model was generated through machine learning of learning model 1 above using a training data set of LDL cholesterol obtained from a blood test performed on the same day. Then, the estimated accuracy of the LDL cholesterol risk estimation model was evaluated by the ROC_AUC curve. As a result, ROC_AUC showed 0.71, which exceeded 0.7 indicating that good classification was achieved.
- FIG. 8 shows the ROC_AUC curve of the estimation result of Example 1. As shown in FIG.
- Attribute information includes ID, name, age, gender, or a combination thereof
- non-invasive biometric information includes BMI, blood pressure, pulse wave data, electrocardiogram data, bioimpedance, and oxygen saturation. (SpO2), or combinations thereof.
- Height and weight which are the criteria for calculating BMI, were measured using a height scale and weight scale, respectively, and blood pressure was measured using a sphygmomanometer.
- Pulse wave data, electrocardiogram data, bioimpedance, and oxygen saturation (SpO2) were measured with Estech BC-3 (Ryobi Systems).
- the non-invasive biometric information may be acquired using a predetermined wearable terminal.
- Bioimpedance (conductance) was measured by passing a weak electric current between two of six electrodes on both feet, both hands, and left and right forehead. The voltage and current were 1.28 V, 200 ⁇ A and the conductance was measured for 32 milliseconds per second. Current was applied to two of the six electrodes, and (1) anode/cathode conductance ( ⁇ S), (2) cathode/anode conductance ( ⁇ S), (3) conductance measured in (1) above.
- Estec BC-3 measured pulse wave data, electrocardiogram data, bioimpedance, and oxygen saturation (SpO2) for 2 minutes for each subject.
- a device equipped with electrocardiogram, pulse wave monitor, and pulse oximeter functions was attached to the subject's left index finger, and two electrodes were attached to the forehead. placed on top.
- ⁇ Learning model 2> In learning model 2, as shown in FIG. 6, machine learning was performed by logistic regression. At this time, the following data were selected and used as attribute information and non-invasive biological data.
- A Attribute information/Gender
- B Non-invasive biological data/Blood pressure
- Pulse pressure/Pulse wave data ...Peripheral vascular resistance, pulse rate, e/a, acceleration pulse wave aging index/Electrocardiogram data... ⁇ LF/HF ⁇ Bioimpedance ⁇ Fat-free percentage (%), 15 right hand-16 left forehead/SCRC, ESG 9+10 ( ⁇ S/m), permittivity of forehead path ⁇ Pulse oximeter ⁇ SpO2
- the noninvasive biological data further includes cardiac output included in bioimpedance, oxygen delivery estimated from oxygen saturation (SpO2), and pulse pressure/pulse calculated from pulse and pulse pressure.
- ⁇ Learning model 3> In learning model 3, as shown in FIG. 6, machine learning was performed by logistic regression. At this time, the following data were selected and used as attribute information and non-invasive biological data.
- A Attribute information/Sex
- B Non-invasive biometric data/BMI/ECG data: RR interval, bioimpedance: cardiac output, 13 left leg-14 right leg/SCRC, R ( ⁇ )
- noninvasive biometric data further includes cardiac output included in bioimpedance and oxygen delivery estimated from oxygen saturation (SpO2).
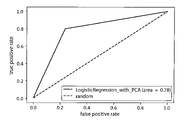
- Example 2 In Example 2, (1) attribute information of 321 subjects, (2) height and weight scale, sphygmomanometer, and noninvasive biological information measured by Estec BC-3, and (3) noninvasive biological information measurement and An HDL cholesterol risk estimation model was generated through machine learning of learning model 2 above using a training data set of HDL cholesterol obtained from a blood test performed on the same day. Then, the estimated accuracy of the HDL cholesterol risk estimation model was evaluated by the ROC_AUC curve. As a result, ROC_AUC showed 0.78, which exceeded 0.7 indicating that good classification was achieved.
- FIG. 9 shows the ROC_AUC curve of the estimation result of Example 2. As shown in FIG.
- Example 3 In Example 3, (1) attribute information of a total of 712 subjects, (2) height and weight scale, sphygmomanometer, and noninvasive biological information measured by Estec BC-3, and (3) noninvasive biological information An HDL cholesterol risk estimation model was generated through machine learning of learning model 3 above using a training data set of HDL cholesterol obtained from a blood test performed on the same day as the measurement. Then, the estimated accuracy of the HDL cholesterol risk estimation model was evaluated by the ROC_AUC curve. As a result, ROC_AUC showed 0.87, exceeding 0.8 indicating that very good classification was achieved.
- FIG. 10 shows the ROC_AUC curve of the estimation result of Example 3.
- HDL cholesterol risk may be estimated using a plurality of learning models. This enables more accurate estimation than estimating the HDL cholesterol risk using one learning model.
- BMI is generally not obtained by wearable terminals, etc., but is obtained from the height and weight entered by the user, but by estimating the BMI and obtaining only biological information, the above-mentioned cholesterol risk is obtained. Therefore, convenience for the user is improved.
- the method of estimating BMI is not particularly limited, for example, BMI is known to be correlated with the inclination of the user's abdomen (at a predetermined position).
- a predetermined acceleration sensor is provided on the abdomen of the user (or a wristband-type wearable terminal equipped with an acceleration sensor is applied to the abdomen), and the inclination of the abdomen is calculated based on the data output from the acceleration sensor. may be obtained and estimated BMI.
- pulse wave data and oxygen saturation may also be estimated using a wristband-type wearable terminal equipped with a pulse wave sensor or medium oxygen concentration sensor, as described above.
- blood pressure may also be estimated using a wristband-type wearable terminal or the like in the same manner as described above. Since it is known that there is a correlation between the speed of the pulse wave sent through the artery by the heartbeat and the blood pressure, using a predetermined sensor that measures the speed of the pulse wave sent through the artery by the heartbeat, Blood pressure may be estimated.
- electrocardiogram data may also be estimated using a wristband-type wearable terminal or the like in the same manner as described above.
- the electrocardiogram data can be estimated based on the data obtained from the electrodes provided on the surface opposite to the display surface of the wristband wearable terminal and the electrodes provided on the display surface side.
- the wrist of a hand for example, left hand wearing a wristband-type wearable terminal is in contact with the electrode provided on the opposite side, and the hand attached to the electrode provided on the display surface side
- Electrocardiogram data may be estimated from data obtained by contacting the fingertips of the opposite hand (eg, right hand).
- bioimpedance may also be estimated using a wristband-type wearable terminal or the like equipped with various electrodes.
- bioimpedance may be estimated based on biometric information obtained from the chest and wrist using a wristband-type wearable terminal or the like.
- biometric information that can be acquired by the wearable terminal and the biometric information to be estimated (BMI, blood pressure, pulse wave data, electrocardiogram data, and biometric information of at least one or more of bioimpedance and oxygen saturation)
- BMI blood pressure
- pulse wave data pulse wave data
- electrocardiogram data electrocardiogram data
- biometric information of at least one or more of bioimpedance and oxygen saturation As teacher data, classifiers generated using various machine learning algorithms may be used to estimate the biometric information of the estimation target described above.
- the above-described second acquisition unit may acquire the estimated biological information.
- the series of processes described above can be executed by hardware or by software.
- the functional configuration described above is merely an example and is not particularly limited. In other words, it is sufficient for the information processing system to have a function capable of executing the series of processes described above as a whole, and what kind of functional block is used to realize this function is not particularly limited to the example described above.
- the locations of the functional blocks are not particularly limited to those shown in FIG. 1, and may be arbitrary.
- the functional blocks of the server may be transferred to another terminal, device, or the like.
- functional blocks of other terminals or devices may be transferred to a server or the like.
- one functional block may be composed of hardware alone, software alone, or a combination thereof.
- the computer may be a computer built into dedicated hardware. Also, the computer may be a computer capable of executing various functions by installing various programs, such as a server, a general-purpose smart phone, or a personal computer.
- a recording medium containing such a program not only consists of a removable medium (not shown) that is distributed separately from the device main body in order to provide the program to the user, etc., but is also preinstalled in the device main body and stored in the user's memory. It is composed of a recording medium etc. provided for Since the program can be distributed via a network, the recording medium may be installed in or accessible to a computer connected or connectable to the network.
- the steps of writing a program recorded on a recording medium are not necessarily processed chronologically according to the order, but may be executed in parallel or individually. It also includes the processing to be performed.
- the term "system” means an overall device composed of a plurality of devices, a plurality of means, or the like.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Engineering & Computer Science (AREA)
- Public Health (AREA)
- Medical Informatics (AREA)
- Physics & Mathematics (AREA)
- Biomedical Technology (AREA)
- Pathology (AREA)
- General Health & Medical Sciences (AREA)
- Molecular Biology (AREA)
- Biophysics (AREA)
- Heart & Thoracic Surgery (AREA)
- Surgery (AREA)
- Animal Behavior & Ethology (AREA)
- Veterinary Medicine (AREA)
- Artificial Intelligence (AREA)
- Signal Processing (AREA)
- Psychiatry (AREA)
- Physiology (AREA)
- Computer Vision & Pattern Recognition (AREA)
- Databases & Information Systems (AREA)
- Optics & Photonics (AREA)
- Data Mining & Analysis (AREA)
- Epidemiology (AREA)
- Primary Health Care (AREA)
- Fuzzy Systems (AREA)
- Mathematical Physics (AREA)
- Evolutionary Computation (AREA)
- Spectroscopy & Molecular Physics (AREA)
- Measurement Of The Respiration, Hearing Ability, Form, And Blood Characteristics Of Living Organisms (AREA)
- Measuring And Recording Apparatus For Diagnosis (AREA)
Abstract
Description
HDLコレステロールは善玉コレステロールとも称され、血中に不足すると動脈硬化などの疾患リスクが上昇することが一般的に知られている。人間ドック学会が制定する血液検査での判定基準によると、HDLコレステロールが40mg/dL以上であれば異常なし、40mg/dL未満であればリスク有と判定される。
また、LDLコレステロールは悪玉コレステロールとも称され、血中に多く存在すると動脈硬化などの疾患リスクが上昇することが一般的に知られている。人間ドック学会が制定する血液検査での判定基準によると、LDLコレステロールが120mg/dL未満であれば異常なし、120mg/dL以上であればリスク有と判定される。
図1~図7を参照して、本実施形態に係るコレステロールリスク推定システム1およびコレステロールリスク推定装置30を説明する。図1は、本実施形態に係るコレステロールリスク推定システム1の概略構成を示すブロック図である。コレステロールリスク推定システム1は、端末装置10と、生体情報測定装置20と、コレステロールリスク推定装置30と、表示装置39とを備える。
ここで、「ユーザ」とは、非侵襲にコレステロールリスクの推定値を得るために、コレステロールリスク推定システムを利用する人をいう。また、「被験者」とは、所定の手続きと同意を得た上で、年齢や性別等の属性情報、非侵襲な生体情報、および血液から測定されたコレステロール測定値を、コレステロールリスク推定システムにおいて利用される訓練データセットとして提供する人をいう。
BMI=w/ h2 [kg/m2]
脈圧は下記の式により計算される。
脈圧=収縮期血圧―拡張期血圧
平均動脈圧は下記の式により計算される。
平均動脈圧=拡張期血圧+脈圧×1/3
脈波データには、脈拍、弾性指数、末梢血管抵抗、加速度脈波、b/a、e/a、-d/a、高沢式加速度脈波加齢指数、駆出率、LVET、DEI(重拍弾性指数)のいずれか、またはこれらの組み合わせが含まれる。
ここで弾性指数とは、身長を、指尖容積脈波において収縮期のピークから拡張期のピークが検出されるまでの時間で割って得られる数値である。末梢血管抵抗は、平均動脈圧/心拍出量×80によって求められる。DEI(重拍弾性指数)は、拡張期血管の弾性を示す指標であり、PWV測定装置により測定可能である。0.3~0.7が正常、0.3以下で高血圧または動脈硬化の可能性があり、0.7以上では急性不安神経症の可能性が示唆される。
加速度脈波は、指尖容積脈波(photoplethysmogram:PTG)の二次微分波(second derivative of photoplethysmogram:SDPTG)である。加速度脈波は、初期陽性波(a波)、初期陰性波(b波)、収縮中期再上昇波(c波)、収縮後期再降下波(d波)、および拡張初期陽性波(e波)より構成され、上記b/a、e/a、-d/aは、各波高の割合より計算される。加齢に伴ってb/aの上昇およびc/a、d/a、e/aの低下が認められるため、高沢式加速度脈波加齢指数(b-c-d-e)/aにより血管の加齢を評価することができる。駆出率は、各心拍で心室から送られる血液の割合であり、加速度脈波加齢指数に比例する。LVETは左心室駆出時間であり、大動脈弁解放後、左室内の血液が大動脈へ駆出される時間である。
心電図データには、呼吸数、心拍数、RR間隔、RR間隔の標準偏差、MxDMn比率、低周波帯のパワースペクトル、高周波帯のパワースペクトル、心拍数変動指標LF/HF、トータルパワーのいずれか、またはその組み合わせが含まれる。ここで、RR間隔とは、心電図のQRS波から次のQRS波までの間隔である。MxDMn比率とは、時間内の最も長いRR間隔と最も短いRR間隔の比であり、不規則な心拍の指数である。トータルパワーとは、2分間の分間測定における周波数0~0.4Hz(VLF,LF,HF)のパワースペクトルのトータルパワーの計算値である。この値は交感神経活動が主に占める自律神経系活動全体を反映する。心電図よりパワースペクトル密度を計算することで、高周波のパワースペクトル割合(0.1875~0.50Hz:HF)、低周波のパワースペクトル割合(0.05~0.1875Hz:LF)、LF/HF比、超低周波帯のパワースペクトル割合(0~0.05Hz:VLF)を計算することができる。
「1額左側-2左手/SCR A」は、「1額左側」がカソード、「2左手」がアノード方向となるように電気が流れた際に測定された経路のコンダクタンス(または伝導性)であり、「5左手-6左足/デルタSCR C-SCR A」は、「5左手」、「6左足」間でアノード-カソード、カソード-アノードとなるよう通電した際に測定されたコンダクタンスの差分である。
推定モデル記憶部36は、学習処理部35により生成したコレステロールリスクの推定モデルを記憶する。非侵襲な生体情報には、BMI、血圧、脈波データ、心電図データおよび生体インピーダンスのいずれか、またはその組み合わせが含まれる。さらに、必要に応じて酸素飽和度(SpO2)が含まれる。
図3は、コレステロールリスク推定装置30のハードウェア構成図である。図3に示すように、コレステロールリスク推定装置30は、一つまたは複数のプロセッサ301と、メモリ302と、ストレージ303と、入出力ポート304と、通信ポート305とを有するコンピュータ300により構成される。プロセッサ301は、プログラムを実行することにより本実施形態に係るコレステロール推定に関する処理を行う。メモリ302は、プログラム及びプログラムの演算結果を一時的に記憶する。ストレージ303は、コレステロールリスク推定装置30による処理を実行するプログラムを格納している。ストレージ303は、コンピュータにより読み取り可能であればどのようなものであっても良く、例えば、記録媒体(磁気ディスク、光ディスク等)、ランダムアクセスメモリー、フラシュタイプメモリー、リードオンリーメモリー等の種々の記録媒体を利用することができる。入出力ポート304は、端末装置10および生体情報測定装置20より情報を入力したり、表示装置39へコレステロール推定値の出力を行う。通信ポート305は、図示しない他のコンピュータ等の情報端末との間でデータの送受信を行う。通信の方法は、無線通信、有線通信を利用することができる。
なお、コレステロールリスク推定装置30は、市販のデスクトップPCまたはノートPCにより実装することが可能であり、推定モデルを用いたコレステロールリスクの推定値の算出に要する時間は数秒である。
なお、コレステロールリスク推定装置30のプロセッサ301においては、動作する際に、上述の第1取得部31、第2取得部32、学習処理部35、推定処理部37等が機能する。
また、下記に示すように、非侵襲生体データに含まれる各データの数を限定した場合であっても、コレステロールが正常か否かの判定を行うことも可能である。
図4は、機械学習によるLDLコレステロールリスク推定モデルの生成実行手順を示すフローチャートである。
ステップST101では、学習処理部35は、入力データ(例えば、上述の訓練データセット)の前処理を行う。具体的には、学習処理部35は、血液検査により得られたLDLコレステロールについて、LDLコレステロール120 mg/dl未満を0(リスク無し)、120 mg/dl以上を1(リスク有り)に変換する。また、学習処理部35は、0と分類された人数と1と分類された人数が乖離し不均衡な場合は、学習データに対してSMOTE (Chawla, NV. et al. 2002)を適用し、人工的にトレーニングサンプルを生成してもよい。すなわち、入力データ(訓練データセット)において、血液検査により得られたLDLコレステロールに基づいてLDLコレステロールリスクの有無を示すラベル(例えば、上述の0または1)を付加し、当該ラベルにおいて、LDLコレステロールリスク有り(ラベル:1)の数と、LDLコレステロールリスク無し(ラベル:0)の数との差が所定の値以上の場合は、この差を小さくするように訓練データセットにおけるサンプルデータを増加(生成)させてもよい。
ステップST102では、学習処理部35は、勾配ブースティング決定木による機械学習を行う。勾配ブースティング回帰木による機械学習では、XGBoost、CatBoost、LightBGM等のソフトウェアライブラリを用いることができる。
また、血液検査により得られたLDLコレステロール値を所定の閾値と比較することにより得られたリスク値(0:リスク無し、1:リスク有り)と機械学習により推定されたLDLコレステロールリスク値を比較し、f1スコアが最大となるようにXGBoostの各パラメータ(max_depth、subsample、colsample_bytree、learning_rate)を調整し、推定モデルを生成した。max_depthは決定木の深さであり、subsampleは各木においてランダムに抽出される標本の割合であり、colsample_bytreeは各木においてランダム抽出される列の割合であり、learning_rateは学習率を示す。ただし、max_depthは1~10、subsampleは0.1~1.0、colsample_bytreeは0.3~1.0、learning_rateは0.1~0.7の範囲で調整を行った。
学習処理部35は、上述の学習処理によって生成されたLDLコレステロールリスク推定モデルを、推定モデル記憶部36に記憶する。
なお、上述の機械学習アルゴリズムは一例であって、これらに限定されるものではない。
図5に示すように、ステップST201では、コレステロールリスク推定装置30の第1取得部31は、端末装置10よりユーザの属性情報を取得する。ステップST202では、コレステロールリスク推定装置30の第2取得部32は、ユーザの非侵襲な生体情報を取得する。そして、ユーザの属性情報と非侵襲な生体情報をユーザデータ記憶部33に記憶する。そして、ステップST203では、推定モデル記憶部36に格納されているLDLコレステロールリスク推定モデルを用いて、推定処理部37によりクラス0(リスク無し)またはクラス1(リスク有り)に属する確率、すなわちLDLコレステロールリスク推定値を算出する。ステップST204では、算出されたLDLコレステロールリスク推定値は推定データ記憶部38に記憶され、ステップST205では、LDLコレステロールリスク推定値を表示装置39等の外部端末へ出力し、表示させる。
図6は、機械学習によるHDLコレステロールリスク推定モデルの生成実行手順を示すフローチャートである。
ステップST301では、学習処理部35は、入力データの前処理を行う。具体的には、学習処理部35は、血液検査により得られたHDLコレステロールについて、HDLコレステロール40 mg/dl以上を0(リスク無し)、40 mg/dl未満を1(リスク有り)に変換する。また、学習処理部35は、0と分類された人数と1と分類された人数が乖離し不均衡な場合は、学習データに対してSMOTE (Chawla, NV. et al. 2002)を適用し、人工的にトレーニングサンプルを生成してもよい。すなわち、入力データ(訓練データセット)において、血液検査により得られたHDLコレステロールに基づいてHDLコレステロールリスクの有無を示すラベル(例えば、上述の0または1)を付加し、当該ラベルにおいて、HDLコレステロールリスク有り(ラベル:1)の数と、HDLコレステロールリスク無し(ラベル:0)の数との差が所定の値以上の場合は、この差を小さくするように訓練データセットにおけるサンプルデータを増加(生成)させてもよい。さらにデータの標準化および正規化を行う。
ステップST302では、学習処理部35は、ロジスティック回帰による機械学習を行う。ロジスティック回帰による機械学習には、例えばPythonのオープンソース機械学習ライブラリであるScikit-learnにて提供されているLogistic Regressionを用いることができる。また、必要に応じて、主成分分析により次元数を圧縮してもよい。
また、血液検査により得られたHDLコレステロール値を所定の閾値と比較することにより得られたリスク値(0:リスク無し、1:リスク有り)と機械学習により推定されたHDLコレステロールリスク値を比較し、f1スコアが最大となるようにLogistic Regressionの各パラメーター(C、正則化方法、max_iter、solber)を調整して、HDLコレステロールリスク推定モデルを生成した。ここで、Cとは正則化の強度を決定するトレードオフパラメータであり、値が大きいほど正則化強度は弱くなる。正則化方法とは、L1正則化またはL2正則化を意味し、これを選択する。max_iterは、学習を反復する最大回数である。solberでは交差エントロピー誤差を最小化する収束方法(例えば、L-BFGS法、ニュートンCG法、liblinear、sagおよびsaga)を選択する。なお、下記の実施例2、3ではliblinear法を選択した。
学習処理部35は、上述の学習処理によって生成されたHDLコレステロールリスク推定モデルを、推定モデル記憶部36に記憶する。
なお、上述の機械学習アルゴリズムは一例であって、これらに限定されるものではない。
図7に示すように、ステップST401では、コレステロールリスク推定装置30の第1取得部31は、端末装置10よりユーザの属性情報を取得する。ステップST402では、コレステロールリスク推定装置30の第2取得部32は、ユーザの非侵襲な生体情報を取得する。そして、ユーザの属性情報と非侵襲な生体情報をユーザデータ記憶部33に記憶する。そして、ステップST403では、推定モデル記憶部36に格納されているHDLコレステロールリスク推定モデルを用いて、推定処理部37によりクラス0(リスク無し)またはクラス1(リスク有り)に属する確率、すなわちHDLコレステロールリスク推定値を算出する。ステップST404では、算出されたHDLコレステロールリスク推定値は推定データ記憶部38に記憶され、ステップST405では、HDLコレステロールリスク推定値を表示装置39等の外部端末へ出力し、表示させる。
以下にLDLコレステロールリスク推定の実施例を記載する。但し、本発明におけるLDLコレステロールリスク推定の態様は、以下の実施例に限定されるものではない。
属性情報には、ID、氏名、年齢、性別のいずれか、またはこれらの組み合わせが含まれ、非侵襲な生体情報には、BMI、血圧、脈波データ、心電図データ、生体インピーダンス、および酸素飽和度(SpO2)のいずれか、またはこれらの組み合わせが含まれる。BMIの算出基準となる身長、体重については、それぞれ身長計および体重計により計測し、血圧については血圧計により測定した。また、脈波データ、心電図データ、生体インピーダンス、酸素飽和度(SpO2)については、エステックBC-3(両備システムズ)により測定した。なお、エステックBC-3に替えて、市販の脈波計、心電図計、インピーダンス測定装置、パルオキシメーターを組み合わせて使用してもよい。また、所定のウェアラブル端末を用いて、上述の非侵襲な生体情報を取得してもよい。
生体インピーダンス(コンダクタンス)の測定は、両足、両手、左右額の計6か所の電極のうち、2か所の間に微弱な電気を流すことで測定した。電圧と電流は1.28V, 200 μAとし、コンダクタンスは1秒につき32ミリ秒間測定した。6か所の電極中で2か所に電流を流し、(1)アノード/カソードコンダクタンス(μS)、(2)カソード/アノードのコンダクタンス(μS)、(3)上記(1)で測定されたコンダクタンスと上記(2)で測定されたコンダクタンスの差分(デルタSCRA-SCRC)、(4)電気伝導度(μS/m)を測定した。
また、筋量、体脂肪量、総水分量、位相角、および抵抗値を測定し、右手⇔左手間、右額⇔左額間で通電している際の誘電率(μSi)も測定した。
学習モデル1では、図4に示すように、勾配ブースティング決定木による機械学習を行わせた。
この際、属性情報、および非侵襲な生体データとして下記に示すデータを選択し、使用した。(A)属性情報・年齢(B)非侵襲な生体データ・血圧・・・拡張期血圧・脈波データ・・・弾性指数、・心電図データ・・・心拍数、RR間隔の標準偏差・生体インピーダンス・・・体脂肪量(kg)、筋量、総水分量(%)、心拍出量、5左手-6左足/SCRA、ESG2+4+15+17(μS/m)、ESG 9+10(μS/m)、ESG9+10(%)、R(Ω)
ここで、ESG9+10は図2に示す部位で測定されたインピーダンスの平均値である。[μS/m]は実測平均値の単位であり、[%]は通常計測され得る範囲内に実測平均値をスケール変換した値である。
また、非侵襲な生体データには、生体インピーダンスに含まれる心拍出量、および酸素飽和度(SpO2)より推定される酸素運搬量がさらに含まれる。
実施例1では、被験者712名の(1)属性情報、(2)身長体重計、血圧計、およびエステックBC-3により測定した非侵襲な生体情報、および(3)非侵襲な生体情報測定と同日に行われた血液検査により得られたLDLコレステロールの訓練データセットを用いて、上記学習モデル1の機械学習を通じて、LDLコレステロールリスク推定モデルを生成した。
そして、LDLコレステロールリスク推定モデルの推定精度について、推定結果をROC_AUC曲線により評価した。その結果、ROC_AUCは0.71を示し、良好な分類ができていることを示す0.7を超えた。実施例1の推定結果のROC_AUC曲線を図8に示す。
以下にHDLコレステロールリスク推定の実施例を記載する。但し、本発明におけるHDLコレステロールリスク推定の態様は、以下の実施例に限定されるものではない。
属性情報には、ID、氏名、年齢、性別のいずれか、またはこれらの組み合わせが含まれ、非侵襲な生体情報には、BMI、血圧、脈波データ、心電図データ、生体インピーダンス、および酸素飽和度(SpO2)のいずれか、またはこれらの組み合わせが含まれる。BMIの算出基準となる身長、体重については、それぞれ身長計および体重計により計測し、血圧については血圧計により測定した。また、脈波データ、心電図データ、生体インピーダンス、酸素飽和度(SpO2)については、エステックBC-3(両備システムズ)により測定した。なお、エステックBC-3に替えて、市販の脈波計、心電図計、インピーダンス測定装置、パルオキシメーターを組み合わせて使用してもよい。また、所定のウェアラブル端末を用いて、上述の非侵襲な生体情報を取得してもよい。
生体インピーダンス(コンダクタンス)の測定は、両足、両手、左右額の計6か所の電極のうち、2か所の間に微弱な電気を流すことで測定した。電圧と電流は1.28V, 200 μAとし、コンダクタンスは1秒につき32ミリ秒間測定した。6か所の電極中で2か所に電流を流し、(1)アノード/カソードコンダクタンス(μS)、(2)カソード/アノードのコンダクタンス(μS)、(3)上記(1)で測定されたコンダクタンスと上記(2)で測定されたコンダクタンスの差分(デルタSCRA-SCRC)、(4)電気伝導度(μS/m)を測定した。
また、筋量、体脂肪量、総水分量、位相角、および抵抗値を測定し、右手⇔左手間、右額⇔左額間で通電している際の誘電率(μSi)も測定した。
学習モデル2では、図6に示すように、ロジスティック回帰による機械学習を行わせた。
この際、属性情報、および非侵襲な生体データとして下記に示すデータを選択し、使用した。(A)属性情報・性別(B)非侵襲な生体データ・血圧・・・脈圧・脈波データ・・・末梢血管抵抗、脈拍、e/a、加速度脈波加齢指数・心電図データ・・・LF/HF・生体インピーダンス・・・除脂肪率(%)、15右手-16額左側/SCRC、ESG 9+10(μS/m)、額経路の誘電率・パルスオキシメーター・・・SpO2
また、非侵襲な生体データには、生体インピーダンスに含まれる心拍出量、および酸素飽和度(SpO2)より推定される酸素運搬量および脈拍と脈圧から計算される脈圧/脈拍がさらに含まれる。
学習モデル3では、図6に示すように、ロジスティック回帰による機械学習を行わせた。
この際、属性情報、および非侵襲な生体データとして下記に示すデータを選択し、使用した。(A)属性情報・性別(B)非侵襲な生体データ・BMI・心電図データ・・・RR間隔、・生体インピーダンス・・・心拍出量、13左足-14右足/SCRC、R(Ω)
実施例2では、被験者321名の(1)属性情報、(2)身長体重計、血圧計、およびエステックBC-3により測定した非侵襲な生体情報、および(3)非侵襲な生体情報測定と同日に行われた血液検査により得られたHDLコレステロールの訓練データセットを用いて、上記学習モデル2の機械学習を通じて、HDLコレステロールリスク推定モデルを生成した。
そして、HDLコレステロールリスク推定モデルの推定精度について、推定結果をROC_AUC曲線により評価した。その結果、ROC_AUCは0.78を示し、良好な分類ができていることを示す0.7を超えた。実施例2の推定結果のROC_AUC曲線を図9に示す。
実施例3では、のべ被験者712名の(1)属性情報、(2)身長体重計、血圧計、およびエステックBC-3により測定した非侵襲な生体情報、および(3)非侵襲な生体情報測定と同日に行われた血液検査により得られたHDLコレステロールの訓練データセットを用いて、上記学習モデル3の機械学習を通じて、HDLコレステロールリスク推定モデルを生成した。
そして、HDLコレステロールリスク推定モデルの推定精度について、推定結果をROC_AUC曲線によって評価した。その結果、ROC_AUCは0.87を示し、極めて良好な分類ができていることを示す0.8を超えた。実施例3の推定結果のROC_AUC曲線を図10に示す。
上述の実施形態では、学習モデル2または学習モデル3を用いてHDLコレステロールリスクを推定する例について説明したが、複数の学習モデルを用いて、HDLコレステロールリスクを推定してもよい。
これにより、1つの学習モデルを用いてHDLコレステロールリスクを推定するよりも、高精度に推定できる。
BMIは、一般に、ウェアラブル端末等で取得されず、ユーザの入力した身長や体重から求めているが、当該BMIを推定することで、生体情報のみを取得することにより、上述のコレステロールリスクを取得することができるため、ユーザにとって利便性が向上する。
BMIの推定方法は特に限定されないが、例えば、BMIは、ユーザの腹部の(所定の位置の)傾きと相関があることが知られている。そこで、例えば、ユーザの腹部に所定の加速度センサを設け(または加速度センサを備えるリストバンド型のウェアラブル端末等を腹部に当てて)、当該加速度センサから出力されるデータに基づいて、腹部の傾きを求め、BMIを推定してもよい。
なお、この場合、上述の第2取得部は、推定された生体情報を取得してもよい。
また例えば、上述した一連の処理は、ハードウェアにより実行させることもできるし、ソフトウェアにより実行させることもできる。換言すると、上述の機能的構成は例示に過ぎず、特に限定されない。即ち、上述した一連の処理を全体として実行できる機能が情報処理システムに備えられていれば足り、この機能を実現するためにどのような機能ブロックを用いるのかは特に上述の例に限定されない。また、機能ブロックの存在場所も、図1に特に限定されず、任意でよい。例えば、サーバの機能ブロックを他の端末や装置等に移譲させてもよい。逆に他の端末や装置の機能ブロックをサーバ等に移譲させてもよい。また、一つの機能ブロックは、ハードウェア単体で構成してもよいし、ソフトウェア単体で構成してもよいし、それらの組み合わせで構成してもよい。
10 端末装置
20 生体情報測定装置
30 コレステロールリスク推定装置
31 第1取得部
32 第2取得部
33 ユーザデータ記憶部
34 訓練データ記憶部
35 学習処理部
36 推定モデル記憶部
37 推定処理部
38 推定データ記憶部
39 表示装置
300 コンピュータ
301 プロセッサ
302 メモリ
303 ストレージ
304 入出力ポート
305 通信ポート
Claims (12)
- 所定のユーザの属性情報および非侵襲な生体情報を取得する情報取得部と、
コレステロールリスク推定モデルを記憶する推定モデル記憶部と、
前記コレステロールリスク推定モデルを用いて、前記所定のユーザの属性情報および/または非侵襲な生体情報に基づいて、前記所定のユーザのコレステロールリスク推定値を計算する推定処理部と、を備えることを特徴とするコレステロールリスク推定装置。 - 前記属性情報は、年齢、および性別のいずれか、またはこれらの組み合わせを含み、
前記非侵襲な生体情報は、BMI、血圧、脈波データ、心電図データ、および生体インピータンスのいずれか、またはこれらの組み合わせを含む、ことを特徴とする請求項1に記載のコレステロールリスク推定装置。 - 前記コレステロールリスク推定値の推定精度は、リスクの有無をROC_AUCが0.7以上で分類可能な精度である、ことを特徴とする請求項1または2に記載のコレステロールリスク推定装置。
- 訓練データセットを記憶する訓練データ記憶部と、
前記訓練データセットに基づいて、機械学習により前記コレステロールリスク推定モデルを生成する学習処理部と、をさらに備えることを特徴とする請求項1から3のいずれか一項に記載のコレステロールリスク推定装置。 - 前記訓練データセットは、被験者の属性情報、非侵襲な生体情報、および血液から測定されたコレステロール測定値を含む、ことを特徴とする請求項4に記載のコレステロールリスク推定装置。
- 前記非侵襲な生体情報は、酸素飽和度(SpO2)をさらに含む、ことを特徴とする請求項5に記載のコレステロールリスク推定装置。
- 前記学習処理部は、
前記訓練データセットにおいて、血液から測定されたコレステロール測定値に基づいて前記コレステロールリスクの有無を示すラベルを付加し、
前記ラベルにおいて、前記コレステロールリスク有りの数と、前記コレステロールリスク無しの数との差が所定の値以上の場合は、前記差を小さくするように前記訓練データセットにおけるサンプルデータを増加させる、ことを特徴とする請求項4から6のいずれか一項に記載のコレステロールリスク推定装置。 - 前記学習処理部は、異なる種類の訓練データセットに基づいて、それぞれ機械学習により第1コレステロールリスク推定モデルおよび第2コレステロールリスク推定モデルを生成し、
前記推定処理部は、前記第1コレステロールリスク推定モデルおよび前記第2コレステロールリスク推定モデルを用いて、前記所定のユーザのコレステロールリスク推定値を計算する、ことを特徴とする請求項4から7のいずれか一項に記載のコレステロールリスク推定装置。 - 前記生体情報に含まれるBMI、血圧、脈波データ、心電図データ、および生体インピーダンス、酸素飽和度のうち少なくとも1つ以上の生体情報を推定する生体情報推定部をさらに備え、
前記情報取得部は、前記生体情報推定部によって推定された生体情報を前記所定のユーザの生体情報として取得する、ことを特徴とする請求項1から8のいずれか一項に記載のコレステロールリスク推定装置。 - 請求項1から9のいずれか一項に記載の前記コレステロールリスク推定装置と、
非侵襲な生体情報を測定する生体情報測定装置と、を備えることを特徴とする非侵襲コレステロールリスク推定システム。 - 被験者の属性情報、非侵襲な生体情報、および血液から測定されたコレステロール測定値を含む訓練データセットを記憶するステップと、
前記訓練データセットに基づいて、機械学習によりコレステロールリスク推定モデルを生成するステップと、
前記コレステロールリスク推定モデルを用いて、所定のユーザの属性情報および/または非侵襲な生体情報に基づいて、前記所定のユーザのコレステロールリスク推定値を計算するステップと、を含む、コレステロールリスク推定方法。 - 被験者の属性情報、非侵襲な生体情報、および血液から測定されたコレステロールの測定値を含む訓練データセットを記憶するステップと、
前記訓練データセットに基づいて、機械学習によりコレステロールリスク推定モデルを生成するステップと、
前記コレステロールリスク推定モデルを用いて、所定のユーザの属性情報および/または非侵襲な生体情報に基づいて、前記所定のユーザのコレステロールリスク推定値を計算するステップと、をコンピュータに実行させるプログラム。
Priority Applications (3)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| CN202280005618.XA CN115884710A (zh) | 2021-06-22 | 2022-03-28 | 胆固醇风险估计设备、胆固醇风险估计方法以及程序 |
| EP22828018.6A EP4362045A4 (en) | 2021-06-22 | 2022-03-28 | Cholesterol risk estimation device, cholesterol risk estimation method, and program |
| US18/041,971 US20240266058A1 (en) | 2021-06-22 | 2022-03-28 | Cholesterol risk estimation device, cholesterol risk estimation method, and computer program |
Applications Claiming Priority (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2021-102923 | 2021-06-22 | ||
| JP2021102923 | 2021-06-22 | ||
| JP2022040635A JP2023002453A (ja) | 2021-06-22 | 2022-03-15 | コレステロールリスク推定装置、コレステロールリスク推定方法及びプログラム |
| JP2022-040635 | 2022-03-15 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2022270099A1 true WO2022270099A1 (ja) | 2022-12-29 |
Family
ID=84545389
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2022/015093 Ceased WO2022270099A1 (ja) | 2021-06-22 | 2022-03-28 | コレステロールリスク推定装置、コレステロールリスク推定方法及びプログラム |
Country Status (5)
| Country | Link |
|---|---|
| US (1) | US20240266058A1 (ja) |
| EP (1) | EP4362045A4 (ja) |
| CN (1) | CN115884710A (ja) |
| TW (1) | TWI907677B (ja) |
| WO (1) | WO2022270099A1 (ja) |
Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2007127424A (ja) * | 2005-10-31 | 2007-05-24 | Toray Ind Inc | 高脂血症またはその発症リスクの判定方法、総コレステロール測定方法およびキット |
| JP2013509588A (ja) * | 2009-10-29 | 2013-03-14 | テシス バイオサイエンス, インコーポレイテッド | 2型糖尿病の予防に対して一貫した改善をもたらすタンパク質バイオマーカーおよび脂質代謝物バイオマーカー |
| WO2014087825A1 (ja) | 2012-12-06 | 2014-06-12 | 国立大学法人北海道大学 | 非侵襲型生体脂質濃度計測器、非侵襲型生体脂質代謝機能計測器、非侵襲による生体脂質濃度計測方法および非侵襲による生体脂質代謝機能検査方法 |
| WO2017204233A1 (ja) * | 2016-05-23 | 2017-11-30 | Necソリューションイノベータ株式会社 | 健康状態予測装置、健康状態予測方法、及びコンピュータ読み取り可能な記録媒体 |
| JP2018088263A (ja) * | 2018-01-10 | 2018-06-07 | オムロンヘルスケア株式会社 | 血圧リスク分析装置及び血圧リスク分析方法 |
| JP2020162834A (ja) * | 2019-03-29 | 2020-10-08 | 株式会社タニタ | 健康情報提供システム及び健康情報提供プログラム |
Family Cites Families (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2021084375A1 (en) * | 2019-10-31 | 2021-05-06 | Aarca Research Inc. | Non-invasive non-contact system and method for measuring dyslipidemia condition using thermal imaging |
-
2022
- 2022-03-25 TW TW111111234A patent/TWI907677B/zh active
- 2022-03-28 US US18/041,971 patent/US20240266058A1/en active Pending
- 2022-03-28 WO PCT/JP2022/015093 patent/WO2022270099A1/ja not_active Ceased
- 2022-03-28 CN CN202280005618.XA patent/CN115884710A/zh active Pending
- 2022-03-28 EP EP22828018.6A patent/EP4362045A4/en active Pending
Patent Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2007127424A (ja) * | 2005-10-31 | 2007-05-24 | Toray Ind Inc | 高脂血症またはその発症リスクの判定方法、総コレステロール測定方法およびキット |
| JP2013509588A (ja) * | 2009-10-29 | 2013-03-14 | テシス バイオサイエンス, インコーポレイテッド | 2型糖尿病の予防に対して一貫した改善をもたらすタンパク質バイオマーカーおよび脂質代謝物バイオマーカー |
| WO2014087825A1 (ja) | 2012-12-06 | 2014-06-12 | 国立大学法人北海道大学 | 非侵襲型生体脂質濃度計測器、非侵襲型生体脂質代謝機能計測器、非侵襲による生体脂質濃度計測方法および非侵襲による生体脂質代謝機能検査方法 |
| WO2017204233A1 (ja) * | 2016-05-23 | 2017-11-30 | Necソリューションイノベータ株式会社 | 健康状態予測装置、健康状態予測方法、及びコンピュータ読み取り可能な記録媒体 |
| JP2018088263A (ja) * | 2018-01-10 | 2018-06-07 | オムロンヘルスケア株式会社 | 血圧リスク分析装置及び血圧リスク分析方法 |
| JP2020162834A (ja) * | 2019-03-29 | 2020-10-08 | 株式会社タニタ | 健康情報提供システム及び健康情報提供プログラム |
Non-Patent Citations (4)
| Title |
|---|
| "Summary of the clinical investigations E. S. Teck Complex", PSYCHOLOGY RESEARCH AND BEHAVIOR MANAGEMENT, vol. 4, 20 March 2010 (2010-03-20), pages 81 - 86 |
| MAAREK A.: "Electro interstitial scan system: assessment of 10 years of research and development", MED DEVICES (AUCKL)., vol. 5, 2012, pages 23 - 30 |
| R. N. CHUAY. W. HAUC. M. TIEWW. L. HAU: "Investigation of Attention Deficit/Hyperactivity Disorder Assessment Using Electro Interstitial Scan Based on Chronoamperometry Technique", IEEE ACCESS, vol. 7, 2019, pages 144679 - 144690, XP011750230, DOI: 10.1109/ACCESS.2019.2938095 |
| See also references of EP4362045A4 |
Also Published As
| Publication number | Publication date |
|---|---|
| EP4362045A1 (en) | 2024-05-01 |
| TWI907677B (zh) | 2025-12-11 |
| TW202301379A (zh) | 2023-01-01 |
| US20240266058A1 (en) | 2024-08-08 |
| EP4362045A4 (en) | 2025-04-16 |
| CN115884710A (zh) | 2023-03-31 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| JP2022153288A (ja) | 血糖値推定装置、血糖値推定方法及びプログラム | |
| WO2022210570A1 (ja) | 血糖値推定装置、血糖値推定方法及びプログラム | |
| WO2023013164A1 (ja) | HbA1cリスク推定装置、HbA1cリスク推定方法及びプログラム | |
| TWI907677B (zh) | 膽固醇風險推定裝置、膽固醇風險推定方法及程式 | |
| JP2023002453A (ja) | コレステロールリスク推定装置、コレステロールリスク推定方法及びプログラム | |
| WO2023013166A1 (ja) | 尿酸値推定装置、尿酸値推定方法及びプログラム | |
| EP4383264A1 (en) | yGT ESTIMATION DEVICE, yGT ESTIMATION METHOD, AND PROGRAM | |
| JP2023024258A (ja) | 尿酸値推定装置、尿酸値推定方法及びプログラム | |
| WO2023013167A1 (ja) | クレアチニンリスク推定装置、クレアチニンリスク推定方法及びプログラム | |
| JP2023024257A (ja) | γGT推定装置、γGT推定方法及びプログラム | |
| EP4362044A1 (en) | Blood neutral fat estimation device, blood neutral fat estimation method, and program | |
| JP2023024259A (ja) | クレアチニンリスク推定装置、クレアチニンリスク推定方法及びプログラム | |
| JP2023024256A (ja) | HbA1cリスク推定装置、HbA1cリスク推定方法及びプログラム | |
| JP2023002452A (ja) | 血中中性脂肪推定装置、血中中性脂肪推定方法及びプログラム | |
| HK40083288A (en) | Cholesterol risk estimation device, cholesterol risk estimation method, and program | |
| CN117678033A (zh) | 尿酸值推定装置、尿酸值推定方法以及程序 | |
| CN117678032A (zh) | γGT推定装置、γGT推定方法以及程序 | |
| HK40083296A (en) | Blood sugar level estimation device, blood sugar level estimation method and program | |
| CN117677849A (zh) | 肌酐风险推定装置、肌酐风险推定方法以及程序 | |
| HK40083287A (en) | Blood neutral fat estimation device, blood neutral fat estimation method, and program | |
| HK40102718A (zh) | 尿酸值推定装置、尿酸值推定方法以及程序 | |
| HK40102120A (zh) | γGT推定装置、γGT推定方法以及程序 | |
| CN117693313A (zh) | HbA1c风险推定装置、HbA1c风险推定方法以及程序 | |
| HK40102707A (zh) | Hba1c风险推定装置、hba1c风险推定方法以及程序 | |
| HK40102847A (zh) | 肌酐风险推定装置、肌酐风险推定方法以及程序 |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 22828018 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 202317010470 Country of ref document: IN |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2022828018 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2022828018 Country of ref document: EP Effective date: 20240122 |