Attorney Docket No.49755-0049WO1 TREATMENT OF B CELL LYMPHOMAS WITH NK CELLS AND A CD20 TARGETED ANTIBODY CLAIM OF PRIORITY [0001] This application claims the benefit of U.S. Provisional Application Serial No. 63/507,393, filed on June 9, 2023. The entire contents of the foregoing are incorporated herein by reference. BACKGROUND [0002] Targeted therapies, including antibody therapy, have revolutionized cancer treatment. One mechanism of action by which antibody therapy induces cytotoxicity is through antibody dependent cell-mediated cytotoxicity (ADCC). Many cancer patients are unable to mount a robust ADCC response. A reduced ADCC response may render any of the indicated monoclonal antibody therapeutics significantly less effective for these patients, which could prevent these patients from responding or lead to relapse. Thus, a reduced ADCC response could negatively impact their clinical outcomes. [0003] Despite recent discoveries and developments of several anti-cancer agents, there is still a need for improved methods and therapeutic agents due to poor prognosis for many types of cancers, including Non-Hodgkin Lymphomas. [0004] NHLs are a heterogeneous group of lymphoproliferative malignancies that usually originate in lymphoid tissues and can spread to other organs. Prognosis for NHL patients depends on histologic type, stage, and response to treatment. NHL can be divided into 2 prognostic groups: the indolent lymphomas and the aggressive lymphomas. Indolent NHLs offer a relatively good prognosis with a median survival of up to 20 years and are generally responsive to immunotherapy, radiation therapy, and chemotherapy. However, a continuous rate of relapse is seen in advanced stages of indolent NHLs. In contrast, aggressive NHLs present acutely and are more commonly resistant or refractory to frontline therapy. [0005] In general, patients with newly diagnosed NHL are treated with chemotherapy combined with rituximab that confers long-term remissions in most patients. NHL patients who are refractory to front-line treatment or those who relapse soon after completing front- line therapies, have poor outcomes. These patients are typically treated with a second line of chemotherapy (ICE or DHAP), often combined with an approved therapeutic monoclonal
Attorney Docket No.49755-0049WO1 antibody (mAb). Depending on their response to this therapy and the patient’s physical condition, autologous stem cell transplant (ASCT) or an approved chimeric antigen receptor T-cell therapy (CAR-T) may be offered. For patients who are ineligible for ASCT, treatment options are limited, and median overall survival is 3.3 months. For patients who have experienced disease progression after ASCT or CAR-T, treatment options and survival are poor (Van Den Neste 2016 Bone Marrow Transplantation 51:51-57). Relapsed and refractory NHL of B-cell origin is, therefore, an area of unmet medical need. [0006] NHL’s are a heterogeneous group of lymphoproliferative disorders originating in B-lymphocytes, T-lymphocytes or NK cells (NK/T cell lymphomas are very rare). In 2019 an estimated 74,200 people will be diagnosed with NHL, and there will be approximately 19,970 deaths due to the disease (ACS Cancer Facts & Figures, 2019). NHL is the seventh leading cause of new cancer cases among men and women, accounting for 4% to 5% of new cancers, and 3% to 4% of cancer related deaths (ACS Cancer Facts & Figures, 2018). In prospectively collected data from the National Cancer Database, diffuse, large B-cell lymphoma (DLBCL) was the major NHL subtype (32%) diagnosed in the United States between 1998 and 2011, followed by chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) at 19%. [0007] B and T lymphocytes are important members of the immune system that above all serve to protect against infectious agents. In general, B cells produce antibodies with antigen-binding capacity, whereas T cells recognize antigen presented by other cells. A variety of different secreted proteins, or cytokines, released by activated T cells (especially of the T helper cell, or CD4+, type) serve to alert and coordinate the local immune response. In light of the importance of the T cells in controlling B-cell as well as overall immune function, it is perhaps not surprising that the strongest and most well established risk factors for malignant lymphomas are characterized by dysregulation or suppression of T- cell function (e.g., HIV/AIDS, organ transplantation) that allow for Epstein-Barr virus (EBV) driven B- cell proliferation and transformation. [0008] As in cancer development in general, neoplastic transformation of T or B cells represents a multi-step process with progressive accumulation of genetic lesions that result in clonal expansion and establishment of a solid or leukemic tumor. Mechanisms may involve dysregulation of cell growth, cell signaling pathways and programmed cell death (apoptosis). The intricate rearrangements in B-cell immunoglobulin or T-cell receptor genes during the normal differentiation and adaptation of these cells represent genetically vulnerable stages.
Attorney Docket No.49755-0049WO1 During these processes, physiologically occurring DNA double-strand breaks pave the way for aberrant chromosomal translocations, which are typical of NHL tumors. [0009] In fact, chromosomal translocations have been observed in up to 90% of NHL cases (Offit K, Wong G, Filippa DA, Tao Y, Chaganti RS. Cytogenetic analysis of 434 consecutively ascertained specimens of non-Hodgkin’s lymphoma: Clinical correlations. Blood 1991;77:1508-1515, Ye BH. BCL-6 in the pathogenesis of non-Hodgkin’s lymphoma. Cancer Invest 2000;18:356 -365). These translocations, with or without additional genetic lesions, can precipitate the activation of oncogenes or inactivation of tumor suppressor genes. Oncogenic viruses provide other possible mechanisms for genetic lesions, as well as direct carcinogenesis by environmental factors. Although the importance of genetic factors in lymphoma development is evident, the geographically uniform rise in NHL incidence implicates a crucial role of one or several environmental agents in the etiology of NHL. [0010] Patients with newly diagnosed NHL are generally treated with at least 4 cycles of R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone) leading to long-term remissions in most patients. NHL patients who are refractory to R-CHOP treatment, however, or those who experience disease relapse soon after completing R-CHOP have poor outcomes. These patients are typically treated with a second line of chemotherapy (ICE or DHAP), often combined with an approved therapeutic mAb. Depending on their response to this therapy and the patient’s physical condition, autologous SCT or an approved CAR-T may be offered. For patients who are ineligible for ASCT, treatment options are limited, and median overall survival is 3.3 months. For patients who have experienced disease progression after ASCT or CAR-T, treatment options and survival are poor (Van Den Neste et al., Outcome of patients with relapsed diffuse large B-cell lymphoma who fail second-line salvage regimens in the International CORAL study. Bone Marrow Transplantation (2016) 51, 51–57). [0011] Although allogeneic NK cells have been used clinically since 2005, their utility has been limited by challenges with product sourcing, scalability, and dose-to-dose variability. [0012] The present invention addresses these and other deficiencies in the art. SUMMARY [0013] NK cells are immune cells that can engage tumor cells through a complex array of receptors on their cell surface, as well as through antibody-dependent cellular cytotoxicity
Attorney Docket No.49755-0049WO1 (ADCC). To initiate ADCC, NK cells engage with antibodies via the CD16 receptor on their surface. NK cells may have an advantage over other immune cells, such as the T cells used in CAR-T cell therapy and other cell therapies. In an exemplary advantage, NK cells can be used as allogeneic therapies, meaning that NK cells from one donor can be safely used in one or many patients without the requirement for HLA matching, gene editing, or other genetic manipulations. Allogeneic NK cells with anti-tumor activity can be administered safely to patients without many of the risks associated with T cell therapies, such as severe cytokine release syndrome (CRS), and neurological toxicities or graft versus host disease (GvHD). [0014] Allogeneic NK cells may provide an important treatment option for cancer patients. In one exemplary advantage, NK cells have been well tolerated without evidence of graft-versus-host disease, neurotoxicity or cytokine release syndrome associated with other cell-based therapies. In another exemplary advantage, NK cells do not require prior antigen exposure or expression of a specific antigen to identify and lyse tumor cells. In another exemplary advantage, NK cells have the inherent ability to bridge between innate immunity and engender a multi-clonal adaptive immune response resulting in long-term anticancer immune memory. All of these features contribute to the potential for NK cell efficacy as cancer treatment options. [0015] For example, NK cells can recruit and activate other components of the immune system. Activated NK cells secrete cytokines and chemokines, such as interferon gamma (IFNγ); tumor necrosis factor alpha (TNFα); and macrophage inflammatory protein 1 (MIP1) that signal and recruit T cells to tumors. Through direct killing of tumor cells, NK cells also expose tumor antigens for recognition by the adaptive immune system. [0016] Additionally, cords with preferred characteristics for enhanced clinical activity (e.g., high-affinity CD16 and Killer cell Immunoglobulin-like Receptor (KIR) B-haplotype) can be selected by utilizing a diverse umbilical cord blood bank as a source for NK cells. [0017] The administration of the allogenic NK cells, as described herein, can enhance patients’ ADCC responses, e.g., when undergoing monoclonal antibody therapy. [0018] Thus, described herein, are methods for treating a patient suffering from a CD20+ cancer selected from diffuse large B-cell lymphoma (DLBCL), high-grade B-cell lymphoma, or primary mediastinal B-cell lymphoma (PMBCL), comprising: administering 1) allogenic natural killer cells (NK cells), and 2) an antibody targeted to human CD20, optionally rituximab, to a patient suffering from a CD20+ cancer selected from diffuse large B-cell lymphoma (DLBCL), high-grade B-cell lymphoma, or primary mediastinal B-cell lymphoma
Attorney Docket No.49755-0049WO1 (PMBCL); wherein the NK cells are a population of expanded natural killer cells comprising a KIR-B haplotype and homozygous for a CD16158V polymorphism. [0019] In some embodiments, the cancer is diffuse large B-cell lymphoma (DLBCL). In some embodiments, the cancer is high-grade B-cell lymphoma. In some embodiments, the cancer is primary mediastinal B-cell lymphoma (PMBCL). In some embodiments, the patient has relapsed after treatment with a CD19-directed therapy. In some embodiments, the CD19- directed therapy is a CAR-T cell therapy. [0020] In some embodiments, administering comprises one or more treatment cycles comprising multiple doses of the antibody and/or NK cells. In some embodiments, the treatment cycle is from 11 to 29 days long starting at the first dose of NK cells. In some embodiments, the treatment cycle comprises four administrations of NK cells. In some embodiments, the NK cells are administered on days 1, 4, 8, and 11. In some embodiments, the NK cells are administered at or at about 4 x 10
9 cells on days 1 and 8. In some embodiments, the NK cells are administered at or at about 2 x 10
9 cells on days 4 and 11. In some embodiments, the NK cells are administered at or at about 4 x 10
9 cells on days 1 and 8 and 2 x 10
9 cells on days 4 and 11. In some embodiments, the antibody is administered on day 8. In some embodiments, the antibody is administered at or at about 500mg/m
2. In some embodiments, the treatment cycle comprises lymphodepletion prior to the first administration of NK cells. In some embodiments, the lymphodepleting comprises non-myeloablative chemotherapy. In some embodiments, the lymphodepleting chemotherapy comprises treatment with at least one of cyclophosphamide and fludarabine. In some embodiments, the lymphodepleting chemotherapy comprises treatment with cyclophosphamide and fludarabine. In some embodiments, the cyclophosphamide is administered between 100 and 500 mg/m
2/day. In some embodiments, the cyclophosphamide is administered at 250 mg/m
2/day. In some embodiments, the cyclophosphamide is administered at 500 mg/m
2/day. In some embodiments, the fludarabine is administered between 10 and 50 mg/m
2/day. In some embodiments, the fludarabine is administered 30 mg/m
2/day. In some embodiments, the lymphodepleting chemotherapy is administered at the beginning of the treatment cycle. In some embodiments, the lymphodepleting chemotherapy is administered on days -5 through -3 of the treatment cycle. In some embodiments, the antibody is administered during the lymphodepletion. In some embodiments, the antibody is administered on Day -4. In some embodiments, the method further comprises administering IL-2. In some embodiments, the method does not comprise administering IL-2. In some embodiments, administration comprises 1, 2, 3, 4, 5, or 6 treatment cycles, optionally 3 treatment cycles. In some
Attorney Docket No.49755-0049WO1 embodiments, the treatment cycles are spaced about 6-10 weeks apart, optionally about 6, 7, 8, 9, or 10 weeks apart. In some embodiments, cycles 2 and 3 are initiated 6–10 weeks after the first day of lymphodepletion in the prior cycle. [0021] In some embodiments, the NK cells are not genetically modified. In some embodiments, at least 70% of the NK cells are CD56+ and CD16+. In some embodiments, at least 85% of the NK cells are CD56+ and CD3-. In some embodiments, 1% or less of the NK cells are CD3+, 1% or less of the NK cells are CD19+ and 1% or less of the NK cells are CD14+. In some embodiments, the allogenic NK cells are expanded natural killer cells. In some embodiments, the expanded natural killer cells are expanded umbilical cord blood natural killer cells. In some embodiments, the expanded natural killer cells comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% CD16+ cells. In some embodiments, the expanded natural killer cells comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKG2D+ cells. In some embodiments, the expanded natural killer cells comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKp46+ cells. In some embodiments, the expanded natural killer cells comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKp30+ cells. In some embodiments, the expanded natural killer cells comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% DNAM-1+ cells. In some embodiments, the expanded natural killer cells comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKp44+ cells. In some embodiments, the expanded natural killer cells comprise less than 20%, e.g., 10% or less, 5% or less, 1% or less, 0.5% or less, or 0% CD3+ cells. In some embodiments, the expanded natural killer cells comprise less than 20% or less, e.g., 10% or less, 5% or less, 1% or less, 0.5% or less, or 0% CD14+ cells. In some embodiments, the expanded natural killer cells comprise less than 20% or less, e.g., 10% or less, 5% or less, 1% or less, 0.5% or less, or 0% CD19+ cells. In some embodiments, the expanded natural killer cells comprise less than 20% or less, e.g., 10% or less, 5% or less, 1% or less, 0.5% or less, or 0% CD38+ cells. In some embodiments, the expanded natural killer cells do not comprise a CD16 transgene. In some embodiments, the expanded natural killer cells do not express an exogenous CD16 protein. In some embodiments, the expanded natural killer cells are not genetically engineered. In some embodiments, the expanded natural killer cells are derived from the same umbilical cord blood donor.
Attorney Docket No.49755-0049WO1 [0022] In some embodiments, the expanded natural killer cells are a population of expanded natural killer cells produced by a method comprising: (a) obtaining seed cells comprising natural killer cells from umbilical cord blood; (b) depleting the seed cells of CD3+ cells; (c) expanding the natural killer cells by culturing the depleted seed cells with a first plurality of Hut78 cells engineered to express a membrane bound IL-21, a mutated TNFα, and a 4-1BBL gene to produce expanded natural killer cells, thereby producing the population of expanded natural killer cells. In some embodiments, the expanded natural killer cells are a population of expanded natural killer cells produced by a method comprising: (a) obtaining seed cells comprising natural killer cells from umbilical cord blood; (b) depleting the seed cells of CD3+ cells; (c) expanding the natural killer cells by culturing the depleted seed cells with a first plurality of Hut78 cells engineered to express a membrane bound IL-21, a mutated TNFα, and a 4-1BBL gene to produce a master cell bank population of expanded natural killer cells; and (d) expanding the master cell bank population of expanded natural killer cells by culturing with a second plurality of Hut78 cells engineered to express a membrane bound IL-21, a mutated TNFα, and a 4-1BBL gene to produce expanded natural killer cells; thereby producing the population of expanded natural killer cells. In some embodiments, the method further comprises, after step (c), (i) freezing the master cell bank population of expanded natural killer cells in a plurality of containers; and (ii) thawing a container comprising an aliquot of the master cell bank population of expanded natural killer cells, wherein expanding the master cell bank population of expanded natural killer cells in step (d) comprises expanding the aliquot of the master cell bank population of expanded natural killer cells. In some embodiments, the umbilical cord blood is from a donor with the KIR-B haplotype and homozygous for the CD16158V polymorphism. In some embodiments, the method comprises expanding the natural killer cells from umbilical cord blood at least 10,000 fold, e.g., 15,000 fold, 20,000 fold, 25,000 fold, 30,000 fold, 35,000 fold, 40,000 fold, 45,000 fold, 50,000 fold, 55,000 fold, 60,000 fold, 65,000 fold, or 70,000 fold. In some embodiments, the population of expanded natural killer cells is not enriched or sorted after expansion. [0023] In some embodiments, the percentage of NK cells expressing CD16 in the population of expanded natural killer cells is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. In some embodiments, the percentage of NK cells expressing NKG2D in the population of expanded natural killer cells is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. In some embodiments, the percentage of NK cells expressing NKp30
Attorney Docket No.49755-0049WO1 in the population of expanded natural killer cells is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. In some embodiments, the percentage of NK cells expressing NKp44 in the population of expanded natural killer cells is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. In some embodiments, the percentage of NK cells expressing NKp46 in the population of expanded natural killer cells is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. In some embodiments, the percentage of NK cells expressing DNAM-1 in the population of expanded natural killer cells is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. [0024] Other features and advantages of the invention will be apparent from the following detailed description and figures, and from the claims. INCORPORATION BY REFERENCE [0025] All publications, patents, and patent applications mentioned in this specification are herein incorporated by reference to the same extent as if each individual publication, patent, or patent application was specifically and individually indicated to be incorporated by reference. BRIEF DESCRIPTION OF THE DRAWINGS [0026] The novel features of the invention are set forth with particularity in the appended claims. A better understanding of the features and advantages of the present invention will be obtained by reference to the following detailed description that sets forth illustrative embodiments, in which the principles of the invention are utilized, and the accompanying drawings of which: [0027] FIG.1 is a patient diagram depicting an example treatment. DETAILED DESCRIPTION [0028] Provided herein are, amongst other things, Natural Killer (NK) cells, e.g., expanded and stimulated NK cells, methods for producing the NK cells, pharmaceutical compositions comprising the NK cells, and methods of treating patients suffering, e.g., from cancer, with the NK cells.
Attorney Docket No.49755-0049WO1 I. EXPANSION AND STIMULATION OF NATURAL KILLER CELLS [0029] In some cases, the NK cells are expanded and stimulated, e.g., as described in WO2022216813, which is hereby incorporated by reference in its entirety. [0030] In some cases, e.g., after having been ex vivo expanded and stimulated, e.g., as described herein, the expanded and stimulated NK cell populations not only have a number/density (e.g., as described above) that could not occur naturally in the human body, but they also differ in their phenotypic characteristics, (e.g., gene expression and/or surface protein expression) with the starting source material or other naturally occurring populations of NK cells. [0031] In some cases, the starting NK cell source is a sample derived from a single individual, e.g., a single cord blood unit that has not been ex vivo expanded. Therefore, in some cases, the expanded and stimulated NK cells share a common lineage, i.e., they all result from expansion of the starting NK cell source, and, therefore, share a genotype via clonal expansion of a population of cells that are, themselves, from a single organism. Yet, they could not occur naturally at the density achieved with ex vivo expansion and also differ in phenotypic characteristics from the starting NK cell source. [0032] In some cases, the population of expanded and stimulated NK cells comprises at least 100 million expanded natural killer cells, e.g., 200 million, 250 million, 300 million, 400 million, 500 million, 600 million, 700 million, 750 million, 800 million, 900 million, 1 billion, 2 billion, 3 billion, 4 billion, 5 billion, 6 billion, 7 billion, 8 billion, 9 billion, 10 billion, 15 billion, 20 billion, 25 billion, 50 billion, 75 billion, 80 billion, 9- billion, 100 billion, 200 billion, 250 billion, 300 billion, 400 billion, 500 billion, 600 billion, 700 billion, 800 billion, 900 billion, 1 trillion, 2 trillion, 3 trillion, 4 trillion, 5 trillion, 6 trillion, 7 trillion, 8 trillion, 9 trillion, or 10 trillion expanded natural killer cells. [0033] In some embodiments, the expanded and stimulated NK cells comprise at least 80%, e.g., at least 90%, at least 95%, at least 99%, or 100% CD56+CD3- cells. [0034] In some embodiments, the expanded and stimulated NK cells do not comprise a CD16 transgene. [0035] In some embodiments, the expanded and stimulated NK cells do not express an exogenous CD16 protein. [0036] The expanded and stimulated NK cells can be characterized, for example, by surface expression, e.g., of one or more of CD16, CD56, CD3, CD38, CD14, CD19, NKG2D, NKp46, NKp30, DNAM-1, and NKp44.
Attorney Docket No.49755-0049WO1 [0037] The surface protein expression levels stated herein, in some cases are achieved without positive selection on the particular surface protein referenced. For example, in some cases, the NK cell source, e.g., a single cord unit, comprises both the KIR B allele of the KIR receptor family and the 158 V/V variant of CD16 and is + enriched and CD3(+) depleted, e.g., by gating on CD56+CD3- expression, but no other surface protein expression selection is carried out during expansion and stimulation. [0038] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKG2D+ cells. [0039] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKp46+ cells. [0040] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKp30+ cells. [0041] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% DNAM-1+ cells. [0042] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKp44+ cells. [0043] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprise at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% CD94+ (KLRD1) cells. [0044] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CD3+ cells.
Attorney Docket No.49755-0049WO1 [0045] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CD14+ cells. [0046] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CD19+ cells. [0047] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CXCR+ cells. [0048] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CD122+ (IL2RB) cells. [0049] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises 90% or more, e.g., 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 99%, or 100% CD3-CD14- CD19-CD16+CD56- cells. [0050] As described herein, the inventors have demonstrated that, surprisingly, the NK cells expanded and stimulated by the methods described herein express CD16 at high levels throughout the expansion and stimulation process, resulting in a cell population with high CD16 expression. The high expression of CD16 obviates the need for engineering the expanded cells to express CD16, which is important for initiating ADCC, and, therefore, a surprising and unexpected benefit of the expansion and stimulation methods described herein. Thus, in some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprise 50% or more, e.g., 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, or 95% CD16+ NK cells. [0051] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises both the KIR B allele of the KIR receptor family and the 158 V/V variant of CD16 and comprise 50% or more, e.g., 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, or 95% CD16+ NK cells.
Attorney Docket No.49755-0049WO1 [0052] In some embodiments, the percentage of expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, expressing CD16 is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. [0053] In some embodiments, the percentage of expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, expressing NKG2D is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. [0054] In some embodiments, the percentage of expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, expressing NKp30 is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. [0055] In some embodiments, the percentage of expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, expressing DNAM-1 is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. [0056] In some embodiments, the percentage of expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, expressing NKp44 is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. [0057] In some embodiments, the percentage of expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, expressing NKp46 is the same or higher than the percentage of natural killer cells in the seed cells from umbilical cord blood. [0058] As described herein, the inventors have also demonstrated that, surprisingly, the NK cells expanded and stimulated by the methods described herein express CD38 at low levels. CD38 is an effective target for certain cancer therapies (e.g., multiple myeloma and acute myeloid leukemia). See, e.g., Jiao et al., “CD38: Targeted Therapy in Multiple Myeloma and Therapeutic Potential for Solid Cancers,” Expert Opinion on Investigational Drugs 29(11):1295–1308 (2020). [0059] Thus, in some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprise less than or equal to 80% CD38+ cells, e.g., less than or equal to 75%, 70%, 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25%, or 20% CD38+ cells.
Attorney Docket No.49755-0049WO1 [0060] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises both the KIR B allele of the KIR receptor family and the 158 V/V variant of CD16 and comprise less than or equal to 80% CD38+ cells, e.g., less than or equal to 75%, 70%, 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25%, or 20% CD38+ cells. [0061] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises both the KIR B allele of the KIR receptor family and the 158 V/V variant of CD16 and comprise less than or equal to 80% CD38+ cells, e.g., less than or equal to 75%, 70%, 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25%, or 20% CD38+ cells, and 50% or more, e.g., 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, or 95% CD16+ NK cells. [0062] In some embodiments, the expanded and stimulated NK cells, e.g., from expansion and stimulation of a single cord blood unit, e.g., as described above, comprises both the KIR B allele of the KIR receptor family and the 158 V/V variant of CD16 and comprise: i) 50% or more, e.g., 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, or 95% CD16+ NK cells; and/or ii) less than or equal to 80% CD38+ cells, e.g., less than or equal to 75%, 70%, 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25%, or 20% CD38+ cells; and/or iii) at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKG2D+ cells; and/or iv) at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKp46+ cells; and/or v) at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKp30+ cells; and/or vi) at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% DNAM-1+ cells; and/or vii) at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% NKp44+ cells; and/or viii) at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% CD94+ (KLRD1) cells; and/or ix) less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CD3+ cells; and/or x) less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CD14+ cells; and/or xi) less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CD19+ cells; and/or xii) less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CXCR+ cells; and/or xiii) less than or equal to 20%, e.g., less than or equal to 10%, less than or equal to 5%, less than or equal to 1% or 0% CD122+ (IL2RB) cells.
Attorney Docket No.49755-0049WO1 [0063] In some embodiments, the NK cell is engineered to alter, e.g., reduce, expression of one or more inhibitor receptor genes. [0064] In some embodiments, the inhibitory receptor gene is a HLA-specific inhibitory receptor. In some embodiments, the inhibitory receptor gene is a non-HLA-specific inhibitory receptor. [0065] In some embodiments, the inhibitor receptor gene is selected from the group consisting of KIR, CD94/NKG2A, LILRB1, PD-1, Irp60, Siglec-7, LAIR-1, and combinations thereof. [0066] Also provided herein are pharmaceutical compositions comprising the natural killer cells described herein and dosage units of the pharmaceutical compositions described herein. [0067] In some cases, the dosage unit comprises between 100 million and 5 billion cells, e.g., 100 million, 200 million, 300 million, 400 million, 500 million, 600 million, 700 million, 800 million, 900 million, 1 billion, 1.1 billion, 1.2 billion, 1.3 billion, 1.4 billion, 1.5 billion, 2 billion, 3 billion, 4 billion, or 5 billion. [0068] Pharmaceutical compositions typically include a pharmaceutically acceptable carrier. As used herein the language “pharmaceutically acceptable carrier” includes saline, solvents, dispersion media, coatings, antibacterial and antifungal agents, isotonic and absorption delaying agents, and the like, compatible with pharmaceutical administration. [0069] In some embodiments, the pharmaceutical composition comprises: a) natural killer cell(s) described herein; and b) a cryopreservation composition. Suitable cryopreservation compositions are described herein. [0070] In some embodiments, the composition is frozen. In some embodiments, the composition has been frozen for at least three months, e.g., at least six months, at least nine months, at least 12 months, at least 15 months, at least 18 months, at least 24 months, or at least 36 months. [0071] In some embodiments, at least 60%, e.g., at least 70%, at least 80%, at least 90% at least 95%, at least 99%, or 100% of the natural killer cells are viable after being thawed. [0072] In some embodiments, the pharmaceutical composition comprises: a) a cryopreservation composition described herein; and b) therapeutic cell(s), e.g., the engineered NK cells described herein. [0073] In some embodiments, the pharmaceutical composition further comprises: c) a buffer solution. Suitable buffer solutions are described herein, e.g., as for cryopreservation compositions.
Attorney Docket No.49755-0049WO1 [0074] In some embodiments, the pharmaceutical composition comprises from or from about 1x10
7 to or to about 1x10
9 cells/mL. In some embodiments, the pharmaceutical composition comprises 1x10
8 cells/mL. In some embodiments, the pharmaceutical composition comprises about 1x10
8 cells/mL. [0075] In some embodiments, the pharmaceutical composition comprises from or from about 1x10
8 to or to about 1x10
10 cells/mL. [0076] In some embodiments, the pharmaceutical composition further comprises an antibody or antigen binding fragment thereof, e.g., an antibody described herein. [0077] Pharmaceutical compositions are typically formulated to be compatible with its intended route of administration. Examples of routes of administration include parenteral, e.g., intravenous, intradermal, subcutaneous, oral (e.g., inhalation), transdermal (topical), transmucosal, and rectal administration. [0078] Methods of formulating suitable pharmaceutical compositions are known in the art, see, e.g., Remington: The Science and Practice of Pharmacy, 21st ed., 2005; and the books in the series Drugs and the Pharmaceutical Sciences: a Series of Textbooks and Monographs (Dekker, NY). For example, solutions or suspensions used for parenteral, intradermal, or subcutaneous application can include the following components: a sterile diluent such as water for injection, saline solution, fixed oils, polyethylene glycols, glycerine, propylene glycol or other synthetic solvents; antibacterial agents such as benzyl alcohol or methyl parabens; antioxidants such as ascorbic acid or sodium bisulfite; chelating agents such as ethylenediaminetetraacetic acid; buffers such as acetates, citrates or phosphates and agents for the adjustment of tonicity such as sodium chloride or dextrose. pH can be adjusted with acids or bases, such as hydrochloric acid or sodium hydroxide. The parenteral preparation can be enclosed in ampoules, disposable syringes or multiple dose vials made of glass or plastic. [0079] Pharmaceutical compositions suitable for injectable use can include sterile aqueous solutions (where water soluble) or dispersions and sterile powders for the extemporaneous preparation of sterile injectable solutions or dispersion. For intravenous administration, suitable carriers include physiological saline, bacteriostatic water, Cremophor EL™ (BASF, Parsippany, NJ) or phosphate buffered saline (PBS). In all cases, the composition must be sterile and should be fluid to the extent that easy syringability exists. It should be stable under the conditions of manufacture and storage and must be preserved against the contaminating action of microorganisms such as bacteria and fungi. The carrier can be a solvent or dispersion medium containing, for example, water, ethanol, polyol (for
Attorney Docket No.49755-0049WO1 example, glycerol, propylene glycol, and liquid polyethylene glycol, and the like), and suitable mixtures thereof. The proper fluidity can be maintained, for example, by the use of a coating such as lecithin, by the maintenance of the required particle size in the case of dispersion and by the use of surfactants. Prevention of the action of microorganisms can be achieved by various antibacterial and antifungal agents, for example, parabens, chlorobutanol, phenol, ascorbic acid, thimerosal, and the like. In many cases, it will be preferable to include isotonic agents, for example, sugars, polyalcohols such as mannitol, sorbitol, sodium chloride in the composition. Prolonged absorption of the injectable compositions can be brought about by including in the composition an agent that delays absorption, for example, aluminum monostearate and gelatin. [0080] Sterile injectable solutions can be prepared by incorporating the active compound in the required amount in an appropriate solvent with one or a combination of ingredients enumerated above, as required, followed by filtered sterilization. Generally, dispersions are prepared by incorporating the active compound into a sterile vehicle, which contains a basic dispersion medium and the required other ingredients from those enumerated above. In the case of sterile powders for the preparation of sterile injectable solutions, the preferred methods of preparation are vacuum drying and freeze-drying, which yield a powder of the active ingredient plus any additional desired ingredient from a previously sterile-filtered solution thereof. [0081] Examples of suitable pharmaceutical compositions are described, for example, in WO2017/135631 and WO2022/0133061, each of which is hereby incorporated by reference in its entirety. II. ANTIBODIES [0082] The methods described herein comprise administering a CD20 targeted antibody. [0083] In some embodiments, the CD20 targeted antibody is rituximab or a biosimilar thereof. Rituximab (e.g., Rituxan®) is one example of a CD20 targeted antibody useful in the presently described methods. Rituximab is a chimeric monoclonal antibody against the protein CD20, which is primarily found on the surface of immune system B cells. It is used to treat diseases characterized by excessive numbers of B cells, overactive B cells, or dysfunctional B cells. This includes, e.g., disorders described herein, such as, for example, many lymphomas, leukemias, transplant rejection, and autoimmune disorders.
Attorney Docket No.49755-0049WO1 [0084] In some embodiments, the CD20 targeting antibody is a CD20 targeting antibody selected from Table 1, or a combination thereof. Table 1. CD20 Targeted Antibodies Name Internal Name Antigen Company Reference ofatumumab Arzerra, Kesimpta, CD20 Genmab, GSK, Sorensen et al., . 9 4 2

Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company Reference MT-3724 CD20 Molecular Huang et al., Blood 6 6 8 1 7 9 1 9- 7 st 9 5 5 k 5 6 8 2
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company Reference Reditux DRL_RI CD20 Dr. Reddy's Bhati et al., Clin 7 3 8 6 5 . 9 3 9 1

[0085] In some embodiments, the CD20 targeting antibody is selected from the group comprising rituximab (or a biosimilar thereof), obinutuzumab (or a biosimilar thereof), ofatumumab (or a biosimilar thereof), ocrelizumab (or a biosimilar thereof), ibritumomab (or a biosimilar thereof), veltuzumab (or a biosimilar thereof), tositumomab (or a biosimilar thereof), ublituximab (or a biosimilar thereof), and combinations thereof. In some embodiments, the CD20 targeting antibody is selected rituximab or a biosimilar thereof. In some embodiments, the CD20 targeting antibody is rituximab. III. PHARMACEUTICAL COMPOSITIONS [0086] Provided herein are pharmaceutical compositions comprising the natural killer cells described herein and dosage units of the pharmaceutical compositions described herein. [0087] In some cases, the dosage unit comprises between 100 million and 5 billion cells, e.g., 100 million, 200 million, 300 million, 400 million, 500 million, 600 million, 700 million, 800 million, 900 million, 1 billion, 1.1 billion, 1.2 billion, 1.3 billion, 1.4 billion, 1.5 billion, 2 billion, 2.5 billion, 3 billion, 3.5 billion, 4 billion, 4.5 billion, 5 billion, or thereabouts.
Attorney Docket No.49755-0049WO1 [0088] Pharmaceutical compositions typically include a pharmaceutically acceptable carrier. As used herein the language "pharmaceutically acceptable carrier" includes saline, solvents, dispersion media, coatings, antibacterial and antifungal agents, isotonic and absorption delaying agents, and the like, compatible with pharmaceutical administration. [0089] In some embodiments, the pharmaceutical composition comprises: a) natural killer cell(s) described herein; and b) a cryopreservation composition. [0090] Suitable cryopreservation compositions are described herein. Examples of suitable cryopreservation compositions are as follows: Table 2. Exemplary Cryopreservation Compositions Exemplary Range v/v% Excipient Concentration Range Exemplary Solution in Cryopreservation

Exemplary v/v% in Final Concentration in Excipient S
l ti n C m iti n Cr r r ti n Cr r r ti n 0
;
Attorney Docket No.49755-0049WO1 Table 4. Exemplary Cryopreservation Composition #2 Exemplary v/v% Final Concentration in Excipient S
olution Composition in Cryopreservation 0
;
Exemplary v/v% Final Concentration in Excipient in 0
;

[0091] In some embodiments, the pharmaceutical composition comprises: a) a cryopreservation composition described herein; and b) therapeutic cell(s). [0092] In some embodiments, the therapeutic cell(s) are animal cell(s). In some embodiments, the therapeutic cell(s) are human cell(s). [0093] In some embodiments, the therapeutic cell(s) are immune cell(s). In some embodiments, the immune cell(s) are selected from basophils, eosinophils, neutrophils, mast cells, monocytes, macrophages, neutrophils, dendritic cells, natural killer cells, B cells, T cells, and combinations thereof.
Attorney Docket No.49755-0049WO1 [0094] In some embodiments, the immune cell(s) are natural killer (NK) cells. In some embodiments, the natural killer cell(s) are expanded and stimulated by a method described herein. [0095] In some embodiments, the pharmaceutical composition further comprises: c) a buffer solution. Suitable buffer solutions are described herein, e.g., as for cryopreservation compositions. [0096] In some embodiments, the pharmaceutical composition comprises from or from about 1x10
7 to or to about 1x10
10 cells/mL. In some embodiments, the pharmaceutical composition comprises 1x10
8 cells/mL. In some embodiments, the pharmaceutical composition comprises about 1x10
8 cells/mL. [0097] In some embodiments, the pharmaceutical composition further comprises an antibody or antigen binding fragment thereof, e.g., an antibody described herein. [0098] Pharmaceutical compositions are typically formulated to be compatible with its intended route of administration. Examples of routes of administration include parenteral, e.g., intravenous, intradermal, subcutaneous, oral (e.g., inhalation), transdermal (topical), transmucosal, and rectal administration. [0099] Methods of formulating suitable pharmaceutical compositions are known in the art, see, e.g., Remington: The Science and Practice of Pharmacy, 21st ed., 2005; and the books in the series Drugs and the Pharmaceutical Sciences: a Series of Textbooks and Monographs (Dekker, NY). For example, solutions or suspensions used for parenteral, intradermal, or subcutaneous application can include the following components: a sterile diluent such as water for injection, saline solution, fixed oils, polyethylene glycols, glycerine, propylene glycol or other synthetic solvents; antibacterial agents such as benzyl alcohol or methyl parabens; antioxidants such as ascorbic acid or sodium bisulfite; chelating agents such as ethylenediaminetetraacetic acid; buffers such as acetates, citrates or phosphates and agents for the adjustment of tonicity such as sodium chloride or dextrose. pH can be adjusted with acids or bases, such as hydrochloric acid or sodium hydroxide. The parenteral preparation can be enclosed in ampoules, disposable syringes or multiple dose vials made of glass or plastic. [0100] Pharmaceutical compositions suitable for injectable use can include sterile aqueous solutions (where water soluble) or dispersions and sterile powders for the extemporaneous preparation of sterile injectable solutions or dispersion. For intravenous administration, suitable carriers include physiological saline, bacteriostatic water, Cremophor EL™ (BASF, Parsippany, NJ) or phosphate buffered saline (PBS). In all cases, the
Attorney Docket No.49755-0049WO1 composition must be sterile and should be fluid to the extent that easy syringability exists. It should be stable under the conditions of manufacture and storage and must be preserved against the contaminating action of microorganisms such as bacteria and fungi. The carrier can be a solvent or dispersion medium containing, for example, water, ethanol, polyol (for example, glycerol, propylene glycol, and liquid polyetheylene glycol, and the like), and suitable mixtures thereof. The proper fluidity can be maintained, for example, by the use of a coating such as lecithin, by the maintenance of the required particle size in the case of dispersion and by the use of surfactants. Prevention of the action of microorganisms can be achieved by various antibacterial and antifungal agents, for example, parabens, chlorobutanol, phenol, ascorbic acid, thimerosal, and the like. In many cases, it will be preferable to include isotonic agents, for example, sugars, polyalcohols such as mannitol, sorbitol, sodium chloride in the composition. Prolonged absorption of the injectable compositions can be brought about by including in the composition an agent that delays absorption, for example, aluminum monostearate and gelatin. [0101] Sterile injectable solutions can be prepared by incorporating the active compound in the required amount in an appropriate solvent with one or a combination of ingredients enumerated above, as required, followed by filtered sterilization. Generally, dispersions are prepared by incorporating the active compound into a sterile vehicle, which contains a basic dispersion medium and the required other ingredients from those enumerated above. In the case of sterile powders for the preparation of sterile injectable solutions, the preferred methods of preparation are vacuum drying and freeze-drying, which yield a powder of the active ingredient plus any additional desired ingredient from a previously sterile-filtered solution thereof. IV. METHODS OF TREATMENT [0102] The NK cells described herein find use for treating cancer or other proliferative disorders. [0103] Thus, also provided herein are methods of treating a patient suffering from a disorder, e.g., a disorder associated with a cancer, e.g., a NHL, e.g., diffuse large B cell lymphoma (DLBCL) comprising administering the NK cells, e.g., the NK cells described herein, and a CD20 targeting antibody, e.g., an antibody described herein, e.g., rituximab. [0104] Also provided herein are methods of preventing, reducing and/or inhibiting the recurrence, growth, proliferation, migration and/or metastasis of a cancer cell or population of cancer cells in a subject in need thereof, comprising administering the NK cells, e.g., the
Attorney Docket No.49755-0049WO1 NK cells described herein, and a CD20 targeting antibody, e.g., an antibody described herein, e.g., rituximab. [0105] Also provided herein are methods of enhancing, improving, and/or increasing the response to an anticancer therapy in a subject in need thereof, comprising administering the NK cells, e.g., the NK cells described herein, and a CD20 targeting antibody, e.g., an antibody described herein, e.g., rituximab. [0106] Also provided herein are methods for inducing the immune system in a subject in need thereof comprising administering the NK cells, e.g., the NK cells described herein, and a CD20 targeting antibody, e.g., an antibody described herein, e.g., rituximab. [0107] The methods described herein include methods for the treatment of disorders associated with abnormal apoptotic or differentiative processes, e.g., cellular proliferative disorders or cellular differentiative disorders, e.g., cancer, including both solid tumors and hematopoietic cancers. Generally, the methods include administering a therapeutically effective amount of a treatment as described herein, to a subject who is in need of, or who has been determined to be in need of, such treatment. In some embodiments, the methods include administering a therapeutically effective amount of a treatment comprising an NK cells, e.g., NK cells described herein, and a CD20 targeting antibody, e.g., an antibody described herein, e.g., rituximab. [0108] As used herein, the terms “treatment,” “treat,” and “treating” refer to reversing, alleviating, delaying the onset of, or inhibiting the progress of a disorder associated with abnormal apoptotic or differentiative processes. For example, a treatment can result in a reduction in tumor size or growth rate. Administration of a therapeutically effective amount of a compound described herein for the treatment of a condition associated with abnormal apoptotic or differentiative processes will result in a reduction in tumor size or decreased growth rate, a reduction in risk or frequency of reoccurrence, a delay in reoccurrence, a reduction in metastasis, increased survival, and/or decreased morbidity and mortality, among other things. In some embodiments, treatment may be administered after one or more symptoms have developed. In other embodiments, treatment may be administered in the absence of symptoms. For example, treatment may be administered to a susceptible individual prior to the onset of symptoms (e.g., in light of a history of symptoms and/or in light of genetic or other susceptibility factors). Treatment may also be continued after symptoms have resolved, for example to prevent or delay their recurrence. [0109] As used herein, the terms "inhibition”, as it relates to cancer and/or cancer cell proliferation, refer to the inhibition of the growth, division, maturation or viability of cancer
Attorney Docket No.49755-0049WO1 cells, and/or causing the death of cancer cells, individually or in aggregate with other cancer cells, by cytotoxicity, nutrient depletion, or the induction of apoptosis. [0110] As used herein, “delaying” development of a disease or disorder, or one or more symptoms thereof, means to defer, hinder, slow, retard, stabilize and/or postpone development of the disease, disorder, or symptom thereof. This delay can be of varying lengths of time, depending on the history of the disease and/or subject being treated. As is evident to one skilled in the art, a sufficient or significant delay can, in effect, encompass prevention, in that the subject does not develop the disease, disorder, or symptom thereof. For example, a method that “delays” development of cancer is a method that reduces the probability of disease development in a given time frame and/or reduces extent of the disease in a given time frame, when compared to not using the method. Such comparisons may be based on clinical studies, using a statistically significant number of subjects. [0111] As used herein, “prevention” or “preventing” refers to a regimen that protects against the onset of the disease or disorder such that the clinical symptoms of the disease do not develop. Thus, “prevention” relates to administration of a therapy (e.g., administration of a therapeutic substance) to a subject before signs of the disease are detectable in the subject and/or before a certain stage of the disease (e.g., administration of a therapeutic substance to a subject with a cancer that has not yet metastasized). The subject may be an individual at risk of developing the disease or disorder, or at risk of disease progression, e.g., cancer metastasis. Such as an individual who has one or more risk factors known to be associated with development or onset of the disease or disorder. For example, an individual may have mutations associated with the development or progression of a cancer. Further, it is understood that prevention may not result in complete protection against onset of the disease or disorder. In some instances, prevention includes reducing the risk of developing the disease or disorder. The reduction of the risk may not result in complete elimination of the risk of developing the disease or disorder. [0112] An “increased” or “enhanced” amount (e.g., with respect to antitumor response, cancer cell metastasis) refers to an increase that is 1.1, 1.2, 1.3, 1.4, 1.5, 1.6, 1.7, 1.8, 1.9, 2, 2.5, 3, 3.5, 4, 4.5, 5, 6, 7, 8, 9, 10, 15, 20, 30, 40, or 50 or more times (e.g., 100, 500, 1000 times) (including all integers and decimal points in between and above 1, e.g., 2.1, 2.2, 2.3, 2.4, etc.) an amount or level described herein. It may also include an increase of at least 10%, at least 20%, at least 30%, at least 40%, at least 50%, at least 60%, at least 70%, at least 80%, at least 90%, at least 100%, at least 150%, at least 200%, at least 500%, or at least 1000% of an amount or level described herein.
Attorney Docket No.49755-0049WO1 [0113] A “decreased” or “reduced” or “lesser” amount (e.g., with respect to tumor size, cancer cell proliferation or growth) refers to a decrease that is about 1.1, 1.2, 1.3, 1.4, 1.5, 1.6 1.7, 1.8, 1.9, 2, 2.5, 3, 3.5, 4, 4.5, 5, 6, 7, 8, 9, 10, 15, 20, 30, 40, or 50 or more times (e.g., 100, 500, 1000 times) (including all integers and decimal points in between and above 1, e.g., 1.5, 1.6, 1.7.1.8, etc.) an amount or level described herein. It may also include a decrease of at least 10%, at least 20%, at least 30%, at least 40%, at least 50%, at least 60%, at least 70%, at least 80%, or at least 90%, at least 100%, at least 150%, at least 200%, at least 500%, or at least 1000% of an amount or level described herein. A. Disorders [0114] Methods and manufactured compositions disclosed herein find use in targeting a number of disorders, such as cellular proliferative disorders. A benefit of the approaches herein is that allogenic cells are used in combination with exogenous antibody administration to target specific proliferating cells targeted by the exogenous antibody. Unlike previous therapies, such as chemo or radiotherapy, using the approaches and pharmaceutical compositions herein, one is able to specifically target cells exhibiting detrimental proliferative activity, potentially without administering a systemic drug or toxin that impacts proliferating cells indiscriminately. [0115] Examples of cellular proliferative and/or differentiative disorders include cancer, e.g., carcinoma, sarcoma, metastatic disorders or hematopoietic neoplastic disorders, e.g., leukemias. A metastatic tumor can arise from a multitude of primary tumor types, including but not limited to those of prostate, colon, lung, breast and liver origin. [0116] As used herein, the terms “cancer”, “hyperproliferative” and “neoplastic” refer to cells having the capacity for autonomous growth, i.e., an abnormal state or condition characterized by rapidly proliferating cell growth. Hyperproliferative and neoplastic disease states may be categorized as pathologic, i.e., characterizing or constituting a disease state, or may be categorized as non-pathologic, i.e., a deviation from normal but not associated with a disease state. The term is meant to include all types of cancerous growths or oncogenic processes, metastatic tissues or malignantly transformed cells, tissues, or organs, irrespective of histopathologic type or stage of invasiveness. “Pathologic hyperproliferative” cells occur in disease states characterized by malignant tumor growth. Examples of non-pathologic hyperproliferative cells include proliferation of cells associated with wound repair. [0117] The terms “cancer” or “neoplasms” include malignancies of the various organ systems, such as affecting lung, breast, thyroid, lymphoid, gastrointestinal, and genito-urinary
Attorney Docket No.49755-0049WO1 tract, as well as adenocarcinomas which include malignancies such as most colon cancers, renal-cell carcinoma, prostate cancer and/or testicular tumors, non-small cell carcinoma of the lung, cancer of the small intestine and cancer of the esophagus. [0118] The term “carcinoma” is art recognized and refers to malignancies of epithelial or endocrine tissues including respiratory system carcinomas, gastrointestinal system carcinomas, genitourinary system carcinomas, testicular carcinomas, breast carcinomas, prostatic carcinomas, endocrine system carcinomas, and melanomas. In some embodiments, the disease is renal carcinoma or melanoma. Exemplary carcinomas include those forming from tissue of the cervix, lung, prostate, breast, head and neck, colon and ovary. The term also includes carcinosarcomas, e.g., which include malignant tumors composed of carcinomatous and sarcomatous tissues. An “adenocarcinoma” refers to a carcinoma derived from glandular tissue or in which the tumor cells form recognizable glandular structures. [0119] The term “sarcoma” is art recognized and refers to malignant tumors of mesenchymal derivation. [0120] Additional examples of proliferative disorders include hematopoietic neoplastic disorders. As used herein, the term “hematopoietic neoplastic disorders” includes diseases involving hyperplastic/neoplastic cells of hematopoietic origin, e.g., arising from myeloid, lymphoid or erythroid lineages, or precursor cells thereof. In some cases, the diseases arise from poorly differentiated acute leukemias, e.g., erythroblastic leukemia and acute megakaryoblastic leukemia. Additional exemplary myeloid disorders include, but are not limited to, acute promyeloid leukemia (APML), acute myelogenous leukemia (AML) and chronic myelogenous leukemia (CML) (reviewed in Vaickus, L. (1991) Crit Rev. in Oncol./Hemotol.11:267-97); lymphoid malignancies include, but are not limited to acute lymphoblastic leukemia (ALL) which includes B-lineage ALL and T-lineage ALL, chronic lymphocytic leukemia (CLL), prolymphocytic leukemia (PLL), hairy cell leukemia (HLL) and Waldenstrom's macroglobulinemia (WM). Additional forms of malignant lymphomas include, but are not limited to non-Hodgkin lymphoma and variants thereof, peripheral T cell lymphomas, adult T cell leukemia/lymphoma (ATL), cutaneous T-cell lymphoma (CTCL), large granular lymphocytic leukemia (LGF), Hodgkin's disease and Reed-Sternberg disease. [0121] In some embodiments, the cancer is selected from the group consisting of: acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), adrenocortical carcinoma, Kaposi sarcoma, AIDS-related lymphoma, primary CNS lymphoma, anal cancer, appendix cancer, astrocytoma, typical teratoid/rhabdoid tumor, basal cell carcinoma, bile duct cancer,
Attorney Docket No.49755-0049WO1 bladder cancer, bone cancer, brain tumor, breast cancer, bronchial tumor, Burkitt lymphoma, carcinoid, cardiac tumors, medulloblastoma, germ cell tumor, primary CNS lymphoma, cervical cancer, cholangiocarcinoma, chordoma, chronic lymphocytic leukemia (CLL), chronic myelogenous leukemia (CML), chronic myeloproliferative neoplasms, colorectal cancer, craniopharyngioma, cutaneous T-cell lymphoma, ductal carcinoma in situ, embryonal tumors, endometrial cancer, ependymoma, esophageal cancer, esthesioneuroblastoma, Ewing sarcoma, extracranial germ cell tumor, extragonadal germ cell tumor, eye cancer (e.g., intraocular melanoma or retinoblastoma), fallopian tube cancer, fibrous histiocytoma of bone, osteosarcoma, gallbladder cancer, gastric cancer, gastrointestinal carcinoid tumor, gastrointestinal stromal tumors (GIST), germ cell tumors, gestational trophoblastic disease, hairy cell leukemia, head and neck cancer, heart tumor, hepatocellular cancer, histiocytosis, Hodgkin lymphomas, hypopharyngeal cancer, intraocular melanoma, islet cell tumors, pancreatic neuroendocrine tumors, kidney (renal cell) carcinoma, Langerhans cell histiocytosis, laryngeal cancer, leukemia, lip and oral cavity cancer, liver cancer, lung cancer (e.g., non-small cell lung cancer, small cell lung cancer, pleuropulmonary blastoma, and tracheobronchial tumor), lymphoma, male breast cancer, malignant fibrous histiocytoma of bone, melanoma, Merkel cell carcinoma, mesothelioma, metastatic cancer, metastatic squamous neck cancer, midline tract carcinoma, mouth cancer, multiple endocrine neoplasia syndromes, multiple myeloma/plasma cell neoplasms, mycosis fungoides, myelodysplastic syndromes, myelodysplastic/myeloproliferative neoplasms, myeloproliferative neoplasms, nasal cavity and paranasal sinus cancer, nasopharyngeal cancer, neuroblastoma, non-Hodgkin lymphoma, oral cancer, lip and oral cavity cancer, oropharyngeal cancer, osteosarcoma, malignant fibrous histiocytoma, ovarian cancer, pancreatic cancer, pancreatic neuroendocrine tumors, papillomatosis, paraganglioma, paranasal sinus and nasal cavity cancer, parathyroid cancer, penile cancer, pharyngeal cancer, pheochromocytomas, pituitary tumor, plasma cell neoplasm, multiple myeloma, pleuropulmonary blastoma, pregnancy and breast cancer, primary central nervous system lymphoma, primary peritoneal cancer, prostate cancer, rectal cancer, recurrent cancer, renal cell cancer, retinoblastoma, rhabdomyosarcoma, salivary gland cancer, sarcoma (e.g., childhood rhabdomyosarcoma, childhood vascular tumors, Ewing sarcoma, Kaposi sarcoma, osteosarcoma, soft tissue sarcoma, uterine sarcoma), Sezary syndrome, skin cancer, small intestine cancer, soft tissue sarcoma, squamous cell carcinoma, squamous neck cancer, stomach cancer, T-cell lymphomas, testicular cancer, throat cancer, nasopharyngeal cancer, oropharyngeal cancer, hypopharyngeal cancer, thryomoma and thymic carcinomas, thyroid cancer, tracheobronchial tumors, transitional cell cancer of the
Attorney Docket No.49755-0049WO1 renal pelvis and ureter, urethral cancer, uterine cancer, uterine sarcoma, vaginal cancer, vascular tumors, vulvar cancer, and Wilms tumor. [0122] In some embodiments, the cancer is a solid tumor. [0123] In some embodiments, the cancer is metastatic. [0124] In some embodiments, the disorder is selected from the group consisting of chronic lymphocytic leukemia (CLL), diffuse large B-cell lymphoma, follicular lymphoma, granulomastosis with polyangiitis, microscopic polyangiitis, multiple sclerosis, non-Hodkin’s Lymphoma, Pemphigus Vulgaris, Rheumatoid Arthritis, and combinations thereof. [0125] In some embodiments, the cancer is a CD20+ cancer. [0126] In some embodiments, the CD20+ cancer is selected from the group consisting of non-Hodgkin's lymphoma (NHL) and chronic lymphocytic leukemia (CLL). [0127] In some embodiments, the CD20+ cancer is selected from the group consisting of indolent or aggressive non-Hodgkin’s lymphoma (NHL). In some embodiments, the CD20+ cancer is relapsed or refractory indolent or aggressive NHL of B-cell origin. Among the aggressive and indolent subtypes are those in Table 6. [0128] In some embodiments, the CD20+ cancer is diffuse large B-cell lymphoma (DLBCL). In some cases, the DLBCL is a double hit DLBCL. In some cases, the DLBCL is a triple hit DLBCL. In some cases, the DLBCL is transformed from an antecedent indolent lymphoma. IN some cases, the CD20+ cancer is high-grade B-cell lymphoma. In some cases, the CD20+ cancer is primary mediastinal B-cell lymphoma (PMBCL). [0129] In some cases, the CD20+ cancer is a histologically confirmed CD20+ cancer. In some cases, the CD20+ cancer is confirmed histologically within one year of treatment. Table 6. Exemplary Aggressive and Indolent NHL Aggressive Subtype Indolent Subtype Diff l B ll l h F lli l l h G d I II d IIIA) i
a

Attorney Docket No.49755-0049WO1 B. Patients [0130] Suitable patients for the compositions and methods herein include those who are suffering from, who have been diagnosed with, or who are suspected of having a cellular proliferative and/or differentiative disorder, e.g., a cancer. Patients subjected to technology of the disclosure herein generally respond better to the methods and compositions herein, in part because the pharmaceutical compositions are allogeneic and target cells identified by the antibodies, rather than targeting proliferating cells generally. As a result, there is less off- target impact and the patients are more likely to complete treatment regimens without substantial detrimental off-target effects. [0131] In some embodiments, the methods of treatment provided herein may be used to treat a subject (e.g., human, monkey, dog, cat, mouse) who has been diagnosed with or is suspected of having a cellular proliferative and/or differentiative disorder, e.g., a cancer. In some embodiments, the subject is a mammal. In some embodiments, the subject is a human. [0132] As used herein, a subject refers to a mammal, including, for example, a human. [0133] In some embodiments, the mammal is selected from the group consisting of an armadillo, an ass, a bat, a bear, a beaver, a cat, a chimpanzee, a cow, a coyote, a deer, a dog, a dolphin, an elephant, a fox, a panda, a gibbon, a giraffe, a goat, a gopher, a hedgehog, a hippopotamus, a horse, a humpback whale, a jaguar, a kangaroo, a koala, a leopard, a lion, a llama, a lynx, a mole, a monkey, a mouse, a narwhal, an orangutan, an orca, an otter, an ox, a pig, a polar bear, a porcupine, a puma, a rabbit, a raccoon, a rat, a rhinoceros, a sheep, a squirrel, a tiger, a walrus, a weasel, a wolf, a zebra, a goat, a horse, and combinations thereof. [0134] In some embodiments, the mammal is a human. [0135] The subject, e.g., the human subject, can be a child, e.g., from or from about 0 to or to about 14 years in age. The subject can be a youth, e.g., from or from about 15 to or to about 24 years in age. The subject can be an adult, e.g., from or from about 25 to or to about 64 years in age. The subject can be a senior, e.g, 65+ years in age. [0136] In some embodiments, the subject may be a human who exhibits one or more symptoms associated with a cellular proliferative and/or differentiative disorder, e.g., a cancer, e.g., a tumor. Any of the methods of treatment provided herein may be used to treat cancer at various stages. By way of example, the cancer stage includes but is not limited to early, advanced, locally advanced, remission, refractory, reoccurred after remission and progressive. In some embodiments, the subject is at an early stage of a cancer. In other embodiments, the subject is at an advanced stage of cancer. In various embodiments, the
Attorney Docket No.49755-0049WO1 subject has a stage I, stage II, stage III or stage IV cancer. The methods of treatment described herein can promote reduction or retraction of a tumor, decrease or inhibit tumor growth or cancer cell proliferation, and/or induce, increase or promote tumor cell killing. In some embodiments, the subject is in cancer remission. The methods of treatment described herein can prevent or delay metastasis or recurrence of cancer. [0137] In some embodiments, the subject suffers from low numbers of NK cells. Some subjects with low numbers of NK cells are unable to mount robust ADCC responses when treated with antibodies, including rituximab. Resistance to rituximab can result even without CD20 antigen loss. In some cases, low NK cell numbers can result in or contribute to resistance to rituximab. In some cases, low NK cell numbers are associated with relapsed or refractory NHL. Thus, these patients may benefit from the use of the compositions and methods described herein. [0138] In some embodiments, the subject is at risk, or genetically or otherwise predisposed (e.g., risk factor), to developing a cellular proliferative and/or differentiative disorder, e.g., a cancer, that has or has not been diagnosed. [0139] As used herein, an “at risk” individual is an individual who is at risk of developing a condition to be treated, e.g., a cellular proliferative and/or differentiative disorder, e.g., a cancer. Generally, an “at risk” subject may or may not have detectable disease, and may or may not have displayed detectable disease prior to the treatment methods described herein. “At risk” denotes that an individual has one or more so-called risk factors, which are measurable parameters that correlate with development of a disease or condition and are known in the art. For example, an at risk subject may have one or more risk factors, which are measurable parameters that correlate with development of cancer. A subject having one or more of these risk factors has a higher probability of developing cancer than an individual without these risk factor(s). In general, risk factors may include, for example, age, sex, race, diet, history of previous disease, presence of precursor disease, genetic (e.g., hereditary) considerations, and environmental exposure. In some embodiments, the subjects at risk for cancer include, for example, those having relatives who have experienced the disease, and those whose risk is determined by analysis of genetic or biochemical markers. [0140] In addition, the subject may be undergoing one or more standard therapies, such as chemotherapy, radiotherapy, immunotherapy, surgery, or combination thereof. Accordingly, one or more kinase inhibitors may be administered before, during, or after administration of chemotherapy, radiotherapy, immunotherapy, surgery or combination thereof.
Attorney Docket No.49755-0049WO1 [0141] In certain embodiments, the subject may be a human who is (i) substantially refractory to at least one chemotherapy treatment, or (ii) is in relapse after treatment with chemotherapy, or both (i) and (ii). In some of embodiments, the subject is refractory to at least two, at least three, or at least four chemotherapy treatments (including standard or experimental chemotherapies). In some embodiments, at least one of such therapies is or includes an anti-CD20 monoclonal antibody therapy. In some embodiments, the subject has previously undergone an autologous hematopoietic stem cell transplant. In some embodiments, the subject has previously been treated with a CAR-T therapy. In some embodiments, the subject has previously been administered an investigational drug or agent. [0142] In some cases, the patient is relapsed or progressed (e.g., progressed at least 4 months) from a prior CD19 directed therapy (e.g., a CD19-directed CAR-T therapy). [0143] In some embodiments, the patient is or has been diagnosed with a disorder selected from the group consisting of chronic lymphocytic leukemia (CLL), diffuse large B- cell lymphoma, follicular lymphoma, granulomastosis with polyangiitis, microscopic polyangiitis, multiple sclerosis, non-Hodkin's Lymphoma, Pemphigus Vulgaris, Rheumatoid Arthritis, and combinations thereof. [0144] In some embodiments, the patient is or has been diagnosed with a CD20+ cancer. [0145] In some embodiments, the patient is or has been diagnosed with a CD20+ cancer by immunohistochemical staining of a biopsy or surgical sample of the cancer. In some embodiments, the patient is or has been diagnosed with a CD20+ cancer by chromogenic in situ hybridization. In some embodiments, the patient is or has been diagnosed with a CD20+ cancer by fluorescent in situ hybridization of a biopsy or surgical sample of the cancer. [0146] In some embodiments, the patient is or has been diagnosed with a CD20+ cancer by genetic analysis, e.g., by identifying a CD20 mutated cancer, e.g., a somatic mutation, e.g., a somatic mutation in the CD20 (MS4A1) gene. [0147] In some embodiments, the patient has a cancer comprising one or more mutations set forth in Table 7, an insertion or deletion polymorphism in the CD20 gene, a copy number variation of the CD20 gene, a methylation mutation of the CD20 gene, or combinations thereof. [0148] In some embodiments, the patient has a chromosomal translocation associated with cancer, e.g., a CD20+ cancer. In some embodiments, the patient has a fusion gene associated with cancer, e.g., a CD20+ cancer.
Attorney Docket No.49755-0049WO1 Table 7. CD20 (MS4A1) Mutations (relative to Human Genome Assembly Reference Build GRCh38.p13 (ncbi.nlm.nih.gov/assembly/88331) Mutation (GRCh38) Protein Position Consequence 11:60463055:G>A 71 missense_variant

Attorney Docket No.49755-0049WO1 Mutation (GRCh38) Protein Position Consequence 11:60462530:G>A 52 synonymous_variant
Attorney Docket No.49755-0049WO1 Mutation (GRCh38) Protein Position Consequence 11:60466036:G>T 151 missense_variant 11:60466042:A>C 153 missense_variant
Attorney Docket No.49755-0049WO1 Mutation (GRCh38) Protein Position Consequence 11:60468394:G>A 274 missense_variant t
with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone), e.g., at least 4 cycles of R-CHOP, a second line of chemotherapy, e.g., ICE (ifosfamide, carboplatin, and etoposide) or DHAP (dexamethasone, high-dose Ara-C cytarabine, and platinol) with or without an approved therapeutic mAb (e.g., rituximab). C. Lymphodepletion [0150] In some embodiments, the patient is lymphodepleted before treatment or before each cycle of treatment. [0151] Illustrative lymphodepleting chemotherapy regimens, along with correlative beneficial biomarkers, are described in WO 2016/191756 and WO 2019/079564, hereby incorporated by reference in their entirety. In certain embodiments, the lymphodepleting chemotherapy regimen comprises administering to the patient doses of cyclophosphamide (between 200 mg/m
2/day and 2000 mg/m
2/day) and doses of fludarabine (between 20 mg/m
2/day and 900 mg/m
2/day). [0152] In some embodiments, lymphodepletion comprises administration of or of about 250 to about 500 mg/m
2 of cyclophosphamide, e.g., from or from about 250 to or to about 500, 250, 400, 500, about 250, about 400, or about 500 mg/m
2 of cyclophosphamide. [0153] In some embodiments, lymphodepletion comprises administration of or of about 20 mg/m
2/day to or to about 40 mg/m
2/day fludarabine, e.g., 30 or about 30 mg/m
2/day. [0154] In some embodiments, lymphodepletion comprises administration of both cyclophosmamide and fludarabine. [0155] In some embodiments, the patient is lymphodepleted by intravenous administration of cyclophosphamide (250 mg/m
2/day) and fludarabine (30 mg/m
2/day).
Attorney Docket No.49755-0049WO1 [0156] In some embodiments, the patient is lymphodepleted by intravenous administration of cyclophosphamide (500 mg/m
2/day) and fludarabine (30 mg/m
2/day). [0157] In some embodiments, the lymphodepletion occurs no more than 5 days prior to the first dose of NK cells. In some embodiments, the lymphodepletion occurs no more than 7 days prior to the first dose of NK cells. [0158] In some embodiments, lymphodepletion occurs daily for 3 consecutive days. In some embodiments, lymphodepletion occurs daily for 3 consecutive days, starting 5 days before the first dose of NK cells (i.e., from Day -5 through Day -3). [0159] In some embodiments, the lymphodepletion occurs on day -5, day -4 and day -3. D. Administration 1. NK Cells [0160] In some embodiments, the NK cells are administered as part of a pharmaceutical composition, e.g., a pharmaceutical composition described herein. Cells are administered after thawing, in some cases without any further manipulation in cases where their cryoprotectant is compatible for immediate administration. For a given individual, a treatment regimen often comprises administration over time of multiple aliquots or doses of NK cells drawn from a common batch or donor. [0161] In some embodiments, the NK cells, e.g., the NK cells described herein are administered at or at about 1 x 10
8 to or to about 8 x 10
10 NK cells per dose, including 1 x 10
8, 2 x 10
8, 3 x 10
8, 4 x 10
8, 5 x 10
8, 6 x 10
8, 7 x 10
8, 8 x 10
8, 9 x 10
8, 1 x 10
9, 2 x 10
9, 3 x 10
9, 4 x 10
9, 5 x 10
9, 6 x 10
9, 7 x 10
9, or 8 x 10
9 cells per dose. In some embodiments, the NK cells are administered at or at about 1 x 10
8, at or at about 1 x 10
9, at or at about 4 x 10
9, or at or at about 8 x 10
9 NK cells per dose. [0162] In some embodiments, the NK cells are administered weekly. In some embodiments, the NK cells are administered weekly for or for about four weeks. In some embodiments, the NK cells are administered weekly for or for about 8 weeks. In some embodiments, the NK cells are administered for a plurality of cycles, each cycle comprising administering weekly doses for 3, 4, 5, 6, 7, 8, 9, 10, 11, or 12 weeks. The number of cycles include 2, 3, 4, or 5 cycles. Each cycle can be preceded by lymphodepletion, a debulking or pretreatment dose of antibody, or both. In some embodiments, the NK cells are administered without a dose of antibody weekly for or for about four weeks followed by administration of NK cells with a dose of antibody, e.g., rituximab.
Attorney Docket No.49755-0049WO1 [0163] In some embodiments, the NK cells are administered for one or more treatment cycles (e.g., 1, 2, 3, 4, or 5 treatment cycles), each comprising administration on days 1, 8, 4, and 11. In some embodiments, the NK cells are administered at or at about 4 x 10
9 on days 1 and 8 and 2 x 10
9 on days 4 and 11 of the treatment cycle. In some embodiments, following the first treatment cycle, subsequent treatment cycles are administered 6-10 weeks apart (e.g., 6, 7, 8, 9, or 10 weeks apart, or thereabouts). [0164] In some cases, the plurality of cycles comprising weekly doses are followed by additional doses administered less frequently, including one dose every four weeks, every month, every other month, or every third month. Such doses can help the patient maintain a response to the therapy. [0165] In some embodiments, the NK cells are cryopreserved in an infusion-ready media, e.g., a cryopreservation composition suitable for intravenous administration, e.g., as described herein. [0166] In some embodiments, the NK cells are cryopreserved in vials containing from or from about 1 x 10
8 to or to about 8 x 10
10 cells per vial, including 1 x 10
8, 2 x 10
8, 3 x 10
8, 4 x 10
8, 5 x 10
8, 6 x 10
8, 7 x 10
8, 8 x 10
8, 9 x 10
8, 1 x 10
9, 2 x 10
9, 3 x 10
9, 4 x 10
9, 5 x 10
9, 6 x 10
9, 7 x 10
9, or 8 x 10
9 cells per vial. In some embodiments, the NK cells are cryopreserved in vials containing a single dose. In some embodiments, the NK cells are cryopreserved in vials containing less than a single dose. In some of such cases, multiple vials can be thawed simultaneously or separately, and can be combined prior to administration or administered separately. [0167] In some embodiments, the cells are thawed, e.g., in a 37°C water bath, prior to administration. [0168] In some embodiments, the thawed vial(s) of NK cells are aseptically transferred to a single administration vessel, e.g., administration bag using, e.g., a vial adapter and a sterile syringe. The NK cells can be administered to the patient from the vessel through a Y-type blood/solution set filter as an IV infusion, by gravity. [0169] In some embodiments, the NK cells are administered as soon as practical, preferably less than 90 minutes, e.g., less than 80, 70, 60, 50, 40, 30, 20, or 10 minutes after thawing. In some embodiments, the NK cells are administered within 30 minutes of thawing. [0170] In some embodiments, the pharmaceutical composition is administered intravenously via syringe or via gravity IV infusion. In some embodiments, the infusion is administered in or in about 1 minute, 2 minutes, 3, minutes, 4 minutes, 5 minutes, 6 minutes, 7 minutes, 8 minutes, 9 minutes, or 10 minutes. In some embodiments, the infusion is
Attorney Docket No.49755-0049WO1 administered over or over about 1 minute, 2 minutes, 3, minutes, 4 minutes, 5 minutes, 6 minutes, 7 minutes, 8 minutes, 9 minutes, or 10 minutes. [0171] In some embodiments, 1 mL, 4 mL, or 10 mL of drug product is administered to the patient intravenously via syringe. 2. Antibodies [0172] In some embodiments, the NK cell(s) described herein, e.g., the pharmaceutical compositions comprising NK cell(s) described herein, are administered in combination with an antibody, e.g., an antibody described herein, e.g., a CD20 targeting antibody, e.g., rituximab. In some embodiments, an antibody is administered together with the NK cells as part of a pharmaceutical composition. In some embodiments, an antibody is administered separately from the NK cells, e.g., as part of a separate pharmaceutical composition. Antibodies can be administered prior to, subsequent to, or simultaneously with administration of the NK cells. [0173] In some embodiments, the antibody is administered before the NK cells. In some embodiments, the antibody is administered after the NK cells. [0174] In some embodiments, the NK cells are administered or are administered at least 30 minutes, 60 minutes, 90 minutes, 120 minutes, 150 minutes, 180 minutes, 210 minutes, or 240 minutes after completing administration of the antibody. In some embodiments, the NK cells are administered within 30 minutes, 60 minutes, 90 minutes, 120 minutes, 150 minutes, 180 minutes, 210 minutes, or 240 minutes after completing administration of the antibody. [0175] In some embodiments, the NK cells are administered the day after the antibody is administered. [0176] In some embodiments, the NK cells are administered at each administration, while the antibody is administered at a subset of the administrations. For example, in some embodiments, the NK cells are administered once a week and the antibody is administered once a every other week, once every three weeks, once every four weeks, or once a month. [0177] In some embodiments, the antibody is administered weekly for 8 weeks. In some embodiments, the antibody is administered every two weeks for 8 weeks. In some embodiments, the antibody administered for a plurality of cycles, each cycle comprising administering weekly doses for 3, 4, 5, 6, 7, 8, 9, 10, 11, or 12 weeks. The number of cycles include 2, 3, 4, or 5 cycles. Each cycle can be preceded by lymphodepletion, a debulking or pretreatment dose of antibody, or both.
Attorney Docket No.49755-0049WO1 [0178] In some cases, the plurality of cycles comprising weekly doses are followed by additional doses administered less frequently, including one dose every four weeks, every month, every other month, or every third month. Such doses can help the patient maintain a response to the therapy. [0179] In some embodiments, a dose of antibody is given prior to the first dose of cells. In some embodiments, a debulking dose or a pretreatment dose of the antibody is given prior to the first dose of cells. [0180] Rituximab is preferably administered at 375 mg/m
2 or 500 mg/m
2 (e.g., 375 mg/m
2 or 500 mg/m
2 per day), preferably at least 1 hour prior to administration of NK cells, e.g., 2–24 hours before administration of NK cells. [0181] In some embodiments, the CD20 targeting antibody (e.g., rituximab) is administered (e.g., intravenously) during lymphodepletion. In some embodiments, the CD20 targ 3. Cytokines [0182] In some embodiments, a cytokine is administered to the patient. [0183] In some embodiments, the cytokine is administered together with the NK cells as part of a pharmaceutical composition. In some embodiments, the cytokine is administered separately from the NK cells, e.g., as part of a separate pharmaceutical composition. [0184] In some embodiments, the cytokine is IL-2. Some tumor microenvironments can become deprived of certain cytokines, including IL-2. In such cases, it can be advantageous to administer a cytokine, such as IL-2, to the patient as part of a treatment regimen involving NK cells. In some cases, the presence of the cytokine, such as IL-2, at the tumor site can increase, enhance, or support the cytotoxicity of the NK cells. In some cases, the cytokine, such as IL-2, can enhance the survival, persistence, or expansion of the NK cells in the patient’s body. [0185] In some embodiments, the IL-2 is administered subcutaneously. [0186] In some embodiments, the IL-2 is administered from between 1 to 4 or about 1 to about 4 hours following the conclusion of NK cell administration. In some embodiments, the IL-2 is administered at least 1 hour following the conclusion of NK cell administration. In some embodiments, the IL-2 is administered no more than 4 hours following the conclusion of NK cell administration. In some embodiments, the IL-2 is administered at least 1 hour after and no more than 4 hours following the conclusion of NK cell administration. Thus, in some embodiments, the IL-2 is administered weekly. In some embodiments, the IL-2 is
Attorney Docket No.49755-0049WO1 administered weekly for or for about four weeks. In some embodiments, the IL-2 is administered weekly for or for about 8 weeks. [0187] In some embodiments, the IL-2 is administered at up to 10 million IU/M
2, e.g., up to 1 million, 2 million, 3 million, 4 million, 5 million, 6 million, 7 million, 8 million, 9 million, or 10 million IU/m
2. [0188] In some embodiments, the IL-2 is administered at or at about 0.5 million, 1 million, at or at about 2 million, at or at about 3 million, at or at about 4 million, at or at about 5 million, at or at about 6 million, at or at about 7 million, at or at about 8 million, at or at about 9 million, at or at about 10 million IU/m
2 [0189] In some embodiments, the IL-2 is administered at or at about 1 x 10
6 IU/M
2. In some embodiments, the IL-2 is administered at or at about 2 x 10
6 IU/m
2. In some embodiments, the IL-2 is administered at or at about 6 x 10
6 IU/m
2. [0190] In some embodiments, less than 1 x 10
6 IU/m
2 IL-2 is administered to the patient. [0191] In some embodiments, a flat dose of IL-2 is administered to the patient. In some embodiments, a flat dose of 1 million IU or about 1 million IU is administered to the patient. In some embodiments, a flat dose of 2 million IU or about 2 million IU is administered to the patient. In some embodiments, a flat dose of 3 million IU or about 3 million IU is administered to the patient. In some embodiments, a flat dose of 4 million IU or about 4 million IU is administered to the patient. In some embodiments, a flat dose of 5 million IU or about 5 million IU is administered to the patient. In some embodiments, a flat dose of 6 million IU or about 6 million IU is administered to the patient. In some embodiments, a flat dose of 7 million IU or about 7 million IU is administered to the patient. In some embodiments, a flat dose of 8 million IU or about 8 million IU is administered to the patient. In some embodiments, a flat dose of 9 million IU or about 9 million IU is administered to the patient. [0192] In some embodiments, IL-2 is not administered to the patient. 4. Pre-Treatments [0193] In some cases, the patient is pre-treated, e.g., 30-60 minutes before NK cell administration. In some cases, the patient is pre-medicated with acetaminophen (e.g., 500 to 1,000 mg given orally); diphenhydramine (e.g., 12.5 to 25 mg given orally, e.g., when needed to treat hypersensitivity reactions); intravenous glucocorticoid (e.g., dexamethasome (e.g., 20 mg) and/or methylprednisone (e.g., 80 mg)). An example pre-medication regimen is shown in Table 8.
Attorney Docket No.49755-0049WO1 Table 8. Example Pre-Medication Regimen NK cell Optional NK i
nfusion Patients Premedication Administration cell dose n n

E. Dosing [0194] An “effective amount” is an amount sufficient to effect beneficial or desired results. For example, a therapeutic amount is one that achieves the desired therapeutic effect. This amount can be the same or different from a prophylactically effective amount, which is an amount necessary to prevent onset of disease or disease symptoms. An effective amount can be administered in one or more administrations, applications or dosages. A therapeutically effective amount of a therapeutic compound (i.e., an effective dosage)
Attorney Docket No.49755-0049WO1 depends on the therapeutic compounds selected. The compositions can be administered one from one or more times per day to one or more times per week; including once every other day. The skilled artisan will appreciate that certain factors may influence the dosage and timing required to effectively treat a subject, including but not limited to the severity of the disease or disorder, previous treatments, the general health and/or age of the subject, and other diseases present. Moreover, treatment of a subject with a therapeutically effective amount of the therapeutic compounds described herein can include a single treatment or a series of treatments. [0195] Dosage, toxicity and therapeutic efficacy of the therapeutic compounds can be determined by standard pharmaceutical procedures in cell cultures or experimental animals, e.g., for determining the LD50 (the dose lethal to 50% of the population) and the ED50 (the dose therapeutically effective in 50% of the population). The dose ratio between toxic and therapeutic effects is the therapeutic index and it can be expressed as the ratio LD50/ED50. Compounds which exhibit high therapeutic indices are preferred. While compounds that exhibit toxic side effects may be used, care should be taken to design a delivery system that targets such compounds to the site of affected tissue in order to minimize potential damage to uninfected cells and, thereby, reduce side effects. [0196] The data obtained from cell culture assays and animal studies can be used in formulating a range of dosage for use in humans. The dosage of such compounds may be within a range of circulating concentrations that include the ED50 with little or no toxicity. The dosage may vary within this range depending upon the dosage form employed and the route of administration utilized. For any compound used in the method of the invention, the therapeutically effective dose can be estimated initially from cell culture assays. A dose may be formulated in animal models to achieve a circulating plasma concentration range that includes the IC50 (i.e., the concentration of the test compound which achieves a half- maximal inhibition of symptoms) as determined in cell culture. Such information can be used to more accurately determine useful doses in humans. F. Combination Therapies [0197] In some embodiments, the method comprises administering the NK cells described herein and a CD20 targeted antibody in combination with another therapy, e.g., an additional antibody, an NK cell engager, an antibody drug conjugate (ADC), a chemotherapy drug, e.g., a small molecule drug, an immune checkpoint inhibitor, and combinations thereof.
Attorney Docket No.49755-0049WO1 1. Small Molecule / Chemotherapy Drugs [0198] In some embodiments, the additional therapy is a small molecule drug. In some embodiments, the additional therapy is a chemotherapy drug. In some embodiments, the additional therapy is a small molecule chemotherapy drug. Such small molecule drugs can include existing standard-of-care treatment regimens to which adoptive NK cell therapy is added. In some cases, the use of the NK cells described herein can enhance the effects of small molecule drugs, including by enhancing the efficacy, reducing the amount of small molecule drug necessary to achieve a desired effect, or reducing the toxicity of the small molecule drug. [0199] In some embodiments, the drug is [(1S,2S,3R,4S,7R,9S,10S,12R,15S)-4-acetyloxy- 1,9,12-trihydroxy-15-[(2R,3S)-2-hydroxy-3-[(2-methylpropan-2-yl)oxycarbonylamino]-3- phenylpropanoyl]oxy-10,14,17,17-tetramethyl-11-oxo-6- oxatetracyclo[11.3.1.0
3,10.0
4,7]heptadec-13-en-2-yl] benzoate (docetaxel) or a pharmaceutically acceptable salt thereof. [0200] In some embodiments, the drug is [(1S,2S,3R,4S,7R,9S,10S,12R,15S)-4,12- diacetyloxy-15-[(2R,3S)-3-benzamido-2-hydroxy-3-phenylpropanoyl]oxy-1,9-dihydroxy- 10,14,17,17-tetramethyl-11-oxo-6-oxatetracyclo[11.3.1.0
3,10.0
4,7]heptadec-13-en-2-yl] benzoate (paclitaxel) or a pharmaceutically acceptable salt thereof. [0201] In some embodiments, the drug is 6-N-(4,4-dimethyl-5H-1,3-oxazol-2-yl)-4-N-[3- methyl-4-([1,2,4]triazolo[1,5-a]pyridin-7-yloxy)phenyl]quinazoline-4,6-diamine (tucatinib) or a pharmaceutically acceptable salt thereof. [0202] In some embodiments, the drug is pentyl N-[1-[(2R,3R,4S,5R)-3,4-dihydroxy-5- methyloxolan-2-yl]-5-fluoro-2-oxopyrimidin-4-yl]carbamate (capecitabine) or a pharmaceutically acceptable salt thereof. [0203] In some embodiments, the drug is azanide;cyclobutane-1,1-dicarboxylic acid;platinum(2+) (carboplatin) or a pharmaceutically acceptable salt thereof. [0204] In some embodiments, the drug is methyl (1R,9R,10S,11R,12R,19R)-11- acetyloxy-12-ethyl-4-[(12S,14R)-16-ethyl-12-methoxycarbonyl-1,10- diazatetracyclo[12.3.1.0
3,11.0
4,9]octadeca-3(11),4,6,8,15-pentaen-12-yl]-10-hydroxy-5- methoxy-8-methyl-8,16-diazapentacyclo[10.6.1.0
1,9.0
2,7.0
16,19]nonadeca-2,4,6,13-tetraene-10- carboxylate (vinorelbine) or a pharmaceutically acceptable salt thereof.
Attorney Docket No.49755-0049WO1 [0205] In some embodiments, the drug is N-[3-chloro-4-[(3- fluorophenyl)methoxy]phenyl]-6-[5-[(2-methylsulfonylethylamino)methyl]furan-2- yl]quinazolin-4-amine (lapatinib) or a pharmaceutically acceptable salt thereof. [0206] In some embodiments, the drug is (E)-N-[4-[3-chloro-4-(pyridin-2- ylmethoxy)anilino]-3-cyano-7-ethoxyquinolin-6-yl]-4-(dimethylamino)but-2-enamide (neratinib) or a pharmaceutically acceptable salt thereof. [0207] In some embodiments, the drug is 6-acetyl-8-cyclopentyl-5-methyl-2-[(5- piperazin-1-ylpyridin-2-yl)amino]pyrido[2,3-d]pyrimidin-7-one (palbociclib) or a pharmaceutically acceptable salt thereof. [0208] In some embodiments, the drug is 7-cyclopentyl-N,N-dimethyl-2-[(5-piperazin-1- ylpyridin-2-yl)amino]pyrrolo[2,3-d]pyrimidine-6-carboxamide (ribociclib) or a pharmaceutically acceptable salt thereof. [0209] In some embodiments, the drug is N-[5-[(4-ethylpiperazin-1-yl)methyl]pyridin-2- yl]-5-fluoro-4-(7-fluoro-2-methyl-3-propan-2-ylbenzimidazol-5-yl)pyrimidin-2-amine (abemaciclib) or a pharmaceutically acceptable salt thereof. [0210] In some embodiments, the drug is (1R,9S,12S,15R,16E,18R,19R,21R,23S,24E,26E,28E,30S,32S,35R)-1,18-dihydroxy-12-[(2R)- 1-[(1S,3R,4R)-4-(2-hydroxyethoxy)-3-methoxycyclohexyl]propan-2-yl]-19,30-dimethoxy- 15,17,21,23,29,35-hexamethyl-11,36-dioxa-4-azatricyclo[30.3.1.0
4,9]hexatriaconta- 16,24,26,28-tetraene-2,3,10,14,20-pentone (everolimus) or a pharmaceutically acceptable salt thereof. [0211] In some embodiments, the drug is (2S)-1-N-[4-methyl-5-[2-(1,1,1-trifluoro-2- methylpropan-2-yl)pyridin-4-yl]-1,3-thiazol-2-yl]pyrrolidine-1,2-dicarboxamide (alpelisib) or a pharmaceutically acceptable salt thereof. [0212] In some embodiments, the drug is 4-[[3-[4-(cyclopropanecarbonyl)piperazine-1- carbonyl]-4-fluorophenyl]methyl]-2H-phthalazin-1-one (olaparib) or a pharmaceutically acceptable salt thereof. [0213] In some embodiments, the drug is (11S,12R)-7-fluoro-11-(4-fluorophenyl)-12-(2- methyl-1,2,4-triazol-3-yl)-2,3,10-triazatricyclo[7.3.1.0
5,13]trideca-1,5(13),6,8-tetraen-4-one (talazoparib) or a pharmaceutically acceptable salt thereof. [0214] In some embodiments, the drug is N-[2-[2-(dimethylamino)ethyl-methylamino]-4- methoxy-5-[[4-(1-methylindol-3-yl)pyrimidin-2-yl]amino]phenyl]prop-2-enamid (osimertinib) or a pharmaceutically acceptable salt thereof.
Attorney Docket No.49755-0049WO1 [0215] In some embodiments, the drug is N-(3-chloro-4-fluorophenyl)-7-methoxy-6-(3- morpholin-4-ylpropoxy)quinazolin-4-amine (gefitinib) or a pharmaceutically acceptable salt thereof. [0216] In some embodiments, the drug is N-(3-ethynylphenyl)-6,7-bis(2- methoxyethoxy)quinazolin-4-amine (erlotinib) or a pharmaceutically acceptable salt thereof. [0217] In some embodiments, the drug is (E)-N-[4-(3-chloro-4-fluoroanilino)-7-[(3S)- oxolan-3-yl]oxyquinazolin-6-yl]-4-(dimethylamino)but-2-enamide (afatinib) or a pharmaceutically acceptable salt thereof. [0218] In some embodiments, the drug is azane;dichloroplatinum (cisplatin, platinol) or a pharmaceutically acceptable salt thereof. [0219] In some embodiments, the drug is azanide;cyclobutane-1,1-dicarboxylic acid;platinum(2+) (carboplatin) or a pharmaceutically acceptable salt thereof [0220] In some embodiments, the drug is 4-amino-1-[(2R,4R,5R)-3,3-difluoro-4-hydroxy- 5-(hydroxymethyl)oxolan-2-yl]pyrimidin-2-one (gemcitabine) or a pharmaceutically acceptable salt thereof. [0221] In some embodiments, the drug is (2S)-2-[[4-[2-(2-amino-4-oxo-3,7- dihydropyrrolo[2,3-d]pyrimidin-5-yl)ethyl]benzoyl]amino]pentanedioic acid (pemetrexed) or a pharmaceutically acceptable salt thereof. [0222] In some embodiments, the drug is N,N-bis(2-chloroethyl)-2-oxo-1,3,2λ
5- oxazaphosphinan-2-amine (cyclophosphamide) or a pharmaceutically acceptable salt thereof. [0223] In some embodiments, the drug is (2R,3S,4S,5R)-2-(6-amino-2-fluoropurin-9-yl)- 5-(hydroxymethyl)oxolane-3,4-diol (fludarabine) or a pharmaceutically acceptable salt thereof. [0224] In some embodiments, the drug is (7S,9S)-7-[(2R,4S,5S,6S)-4-amino-5-hydroxy-6- methyloxan-2-yl]oxy-6,9,11-trihydroxy-9-(2-hydroxyacetyl)-4-methoxy-8,10-dihydro-7H- tetracene-5,12-dione (doxorubicin) or a pharmaceutically acceptable salt thereof. [0225] In some embodiments, the drug is methyl (1R,9R,10S,11R,12R,19R)-11- acetyloxy-12-ethyl-4-[(13S,15S,17S)-17-ethyl-17-hydroxy-13-methoxycarbonyl-1,11- diazatetracyclo[13.3.1.0
4,12.0
5,10]nonadeca-4(12),5,7,9-tetraen-13-yl]-8-formyl-10-hydroxy-5- methoxy-8,16-diazapentacyclo[10.6.1.0
1,9.0
2,7.0
16,19]nonadeca-2,4,6,13-tetraene-10- carboxylate (vincristine) or a pharmaceutically acceptable salt thereof. [0226] In some embodiments, the drug is (8S,9S,10R,13S,14S,17R)-17-hydroxy-17-(2- hydroxyacetyl)-10,13-dimethyl-6,7,8,9,12,14,15,16-octahydrocyclopenta[a]phenanthrene- 3,11-dione (prednisone) or a pharmaceutically acceptable salt thereof.
Attorney Docket No.49755-0049WO1 [0227] In some embodiments, the drug is N,3-bis(2-chloroethyl)-2-oxo-1,3,2λ
5- oxazaphosphinan-2-amine (ifosfamide) or a pharmaceutically acceptable salt thereof. [0228] In some embodiments, the drug is (5S,5aR,8aR,9R)-5-[[(2R,4aR,6R,7R,8R,8aS)- 7,8-dihydroxy-2-methyl-4,4a,6,7,8,8a-hexahydropyrano[3,2-d][1,3]dioxin-6-yl]oxy]-9-(4- hydroxy-3,5-dimethoxyphenyl)-5a,6,8a,9-tetrahydro-5H-[2]benzofuro[6,5- f][1,3]benzodioxol-8-one (etopside) or a pharmaceutically acceptable salt thereof. [0229] In some embodiments, the drug is (8S,9R,10S,11S,13S,14S,16R,17R)-9-fluoro- 11,17-dihydroxy-17-(2-hydroxyacetyl)-10,13,16-trimethyl-6,7,8,11,12,14,15,16- octahydrocyclopenta[a]phenanthren-3-one (dexamethasone) or a pharmaceutically acceptable salt thereof. [0230] In some embodiments, the drug is (8S,9R,10S,11S,13S,14S,16R,17R)-9-fluoro- 11,17-dihydroxy-17-(2-hydroxyacetyl)-10,13,16-trimethyl-6,7,8,11,12,14,15,16- octahydrocyclopenta[a]phenanthren-3-one (cytarabine) or a pharmaceutically acceptable salt thereof. 2. NK Cell Engagers [0231] In some embodiments, the additional therapy is an NK cell engager, e.g., a bispecific or trispecific antibody. [0232] In some embodiments, the NK cell engager is a bispecific antibody against CD16 and a disease-associated antigen, e.g., cancer-associated antigen, e.g., an antigen of cancers described herein. In some embodiments, the NK cell engager is a trispecific antibody against CD16 and two disease-associated antigens, e.g., cancer-associated antigens, e.g., antigens of cancers described herein. [0233] In some embodiments, the NK cells, e.g., the NK cells described herein, e.g., AB- 101 cells, are administered in combination with a CD20 targeting antibody as well as a therapy selected from the group consisting of cyclophosphamide, doxorubicin, vincristine, prednisone, dexamethasone, cytarabine, e.g., high-dose Ara-C cytarabine, platinol, and combinations thereof (e.g., R-CHOP, ICE, or DHAP). 3. Checkpoint Inhibitors [0234] In some embodiments, the additional therapy is an immune checkpoint inhibitor. [0235] In some embodiments, the immune checkpoint inhibitor is selected from the group consisting of a PD-1 inhibitor, a PD-L1 inhibitor, a CTLA-4 inhibitor, and combinations thereof.
Attorney Docket No.49755-0049WO1 [0236] In some embodiments, the immune checkpoint inhibitor is selected from the group consisting of a PD-1 inhibitor, a PD-L1 inhibitor, a CTLA-4 inhibitor, a VISTA inhibitor, a BTLA inhibitor, a TIM-3 inhibitor, a KIR inhibitor, a LAG-3 inhibitor, a TIGIT inhibitor, a CD-96 inhibitor, a SIRPα inhibitor, and combinations thereof. [0237] In some embodiments, the immune checkpoint inhibitor is selected from the group consisting of a PD-1 inhibitor, a PD-L1 inhibitor, a CTLA-4 inhibitor, a LAG-3 (CD223) inhibitor, a TIM-3 inhibitor, a B7-H3 inhibitor, a B7-H4 inhibitor, an A2aR inhibitor, a CD73 inhibitor, a NKG2A inhibitor, a PVRIG/PVRL2 inhibitor, a CEACAM1 inhibitor, a CEACAM 5 inhibitor, a CEACAM 6 inhibitor, a FAK inhibitor, a CCL2 inhibitor, a CCR2 inhibitor, a LIF inhibitor, a CD47 inhibitor, a SIRPα inhibitor, a CSF-1 inhibitor, an M-CSF inhibitor, a CSF-1R inhibitor, an IL-1 inhibitor, an IL-1R3 inhibitor, an IL-RAP inhibitor, an IL-8 inhibitor, a SEMA4D inhibitor, an Ang-2 inhibitor, a CELVER-1 inhibitor, an Axl inhibitor, a phsphatidylserine inhibitor, and combinations thereof. [0238] In some embodiments, the immune checkpoint inhibitor is selected from those shown in Table 9, or combinations thereof. Table 9. Exemplary Immune Checkpoint Inhibitors Target Inhibitor L
AG525 (IMP701), REGN3767 (R3767), BI 754,091, tebotelimab
Attorney Docket No.49755-0049WO1 [0239] In some embodiments, the immune checkpoint inhibitor is an antibody. [0240] In some embodiments, the PD-1 inhibitor is selected from the group consisting of pembrolizumab, nivolumab, toripalimab, cemiplimab-rwlc, sintilimab, and combinations thereof. [0241] In some embodiments, the PD-L1 inhibitor is selected from the group consisting of atezolizumab, durvalumab, avelumab, and combinations thereof. [0242] In some embodiments, the CTLA-4 inhibitor is ipilimumab. In some embodiments, the PD-1 inhibitor is selected from the group of inhibitors shown in Table 10. Table 10. Exemplary PD-1 Inhibitor Antibodies Name Internal Name Antigen Company nivolumab Opdivo, ONO-4538, PD-1 BMS, Medarex, Ono n
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company F520 PD-1 Shandong New Time e
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company camrelizumab SHR-1210 PD-1 Incyte, Jiangsu u
, ors shown in Table 11. Table 11. Exemplary PD-L1 Inhibitor Antibodies Name Internal Name Antigen Company I
mfinzi, MEDI-4736, AstraZeneca, Celgene, Me i
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company IBI322 IBI-322 CD47, PD-L1 Innovent a
i
[0244] In some embodiments, the CTLA-4 inhibitor is selected from the group of inhibitors shown in Table 12. Table 12. Exemplary CTLA4 Inhibitor Antibodies Name Internal Name Antigen Company
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company vudalimab XmAb20717 CTLA4, PD-1 Xencor n i

[0245] In some embodiments, the immune checkpoint inhibitor is a small molecule drug. Small molecule checkpoint inhibitors are described, e.g., in WO2015/034820A1, WO2015/160641A2, WO2018/009505 A1, WO2017/066227 A1, WO2018/044963 A1, WO2018/026971 A1, WO2018/045142 A1, WO2018/005374 A1, WO2017/202275 A1, WO2017/202273 A1, WO2017/202276 A1, WO2018/006795 A1, WO2016/142852 A1, WO2016/142894 A1, WO2015/033301 A1, WO2015/033299 A1, WO2016/142886 A2, WO2016/142833 A1, WO2018/051255 A1, WO2018/051254 A1, WO2017/205464 A1, US2017/0107216 A1, WO2017/070089A1, WO2017/106634A1, US2017/0174679 A1, US2018/0057486 A1, WO2018/013789 A1, US2017/0362253 A1, WO2017/192961 A1, WO2017/118762 A1, US2014/199334 A1, WO2015/036927 A1, US2014/0294898 A1, US2016/0340391 A1, WO2016/039749 A1, WO2017/176608 A1, WO2016/077518 A1, WO2016/100608 A1, US2017/0252432 A1, WO2016/126646 A1, WO2015/044900 A1,
Attorney Docket No.49755-0049WO1 US2015/0125491 A1, WO2015/033303 A1, WO2016/142835 A1, WO2019/008154 A1, WO2019/008152 A1, and WO2019023575A1. [0246] In some embodiments, the PD-1 inhibitor is 2-[[4-amino-1-[5-(1-amino-2- hydroxypropyl)-1,3,4-oxadiazol-2-yl]-4-oxobutyl]carbamoylamino]-3-hydroxypropanoic acid (CA-170). [0247] In some embodiments, the immune checkpoint inhibitor is (S)-1-(3-Bromo-4-((2- bromo-[1,1′-biphenyl]-3-yl)methoxy)benzyl)piperidine-2-carboxylic Acid. [0248] In some embodiments, the immune checkpoint inhibitor is a peptide. See, e.g., Sasikumar et al., “Peptide and Peptide-Inspired Checkpoint Inhibitors: Protein Fragments to Cancer Immunotherapy,” Medicine in Drug Discovery 8:100073 (2020). V. VARIANTS [0249] In some embodiments, the fusion protein(s) or components thereof described herein, or the NK cell genotypes described herein, are at least 80%, e.g., at least 85%, 90%, 95%, 98%, or 100% identical to the amino acid sequence of an exemplary sequence (e.g., as provided herein), e.g., have differences at up to 1%, 2%, 5%, 10%, 15%, or 20% of the residues of the exemplary sequence replaced, e.g., with conservative mutations, e.g., including or in addition to the mutations described herein. In preferred embodiments, the variant retains desired activity of the parent. [0250] To determine the percent identity of two nucleic acid sequences, the sequences are aligned for optimal comparison purposes (e.g., gaps can be introduced in one or both of a first and a second amino acid or nucleic acid sequence for optimal alignment and non-homologous sequences can be disregarded for comparison purposes). The length of a reference sequence aligned for comparison purposes is at least 80% of the length of the reference sequence, and in some embodiments is at least 90% or 100%. The nucleotides at corresponding amino acid positions or nucleotide positions are then compared. When a position in the first sequence is occupied by the same nucleotide as the corresponding position in the second sequence, then the molecules are identical at that position (as used herein nucleic acid "identity" is equivalent to nucleic acid "homology"). The percent identity between the two sequences is a function of the number of identical positions shared by the sequences, taking into account the number of gaps, and the length of each gap, which need to be introduced for optimal alignment of the two sequences. [0251] Percent identity between a subject polypeptide or nucleic acid sequence (i.e. a query) and a second polypeptide or nucleic acid sequence (i.e. target) is determined in various
Attorney Docket No.49755-0049WO1 ways that are within the skill in the art, for instance, using publicly available computer software such as Smith Waterman Alignment (Smith, T. F. and M. S. Waterman (1981) J Mol Biol 147:195-7); "BestFit" (Smith and Waterman, Advances in Applied Mathematics, 482- 489 (1981)) as incorporated into GeneMatcher PlusTM, Schwarz and Dayhof (1979) Atlas of Protein Sequence and Structure, Dayhof, M.O., Ed, pp 353-358; BLAST program (Basic Local Alignment Search Tool; (Altschul, S. F., W. Gish, et al. (1990) J Mol Biol 215: 403- 10), BLAST-2, BLAST-P, BLAST-N, BLAST-X, WU-BLAST-2, ALIGN, ALIGN-2, CLUSTAL, or Megalign (DNASTAR) software. In addition, those skilled in the art can determine appropriate parameters for measuring alignment, including any algorithms needed to achieve maximal alignment over the length of the sequences being compared. In general, for target proteins or nucleic acids, the length of comparison can be any length, up to and including full length of the target (e.g., 5%, 10%, 20%, 30%, 40%, 50%, 60%, 70%, 80%, 90%, 95%, or 100%). For the purposes of the present disclosure, percent identity is relative to the full length of the query sequence. [0252] For purposes of the present disclosure, the comparison of sequences and determination of percent identity between two sequences can be accomplished using a Blossum 62 scoring matrix with a gap penalty of 12, a gap extend penalty of 4, and a frameshift gap penalty of 5. [0253] Conservative substitutions typically include substitutions within the following groups: glycine, alanine; valine, isoleucine, leucine; aspartic acid, glutamic acid, asparagine, glutamine; serine, threonine; lysine, arginine; and phenylalanine, tyrosine. VI. DEFINITIONS [0254] Unless defined otherwise, all terms of art, notations and other technical and scientific terms or terminology used herein are intended to have the same meaning as is commonly understood by one of ordinary skill in the art to which the claimed subject matter pertains. In some cases, terms with commonly understood meanings are defined herein for clarity and/or for ready reference, and the inclusion of such definitions herein should not necessarily be construed to represent a substantial difference over what is generally understood in the art. [0255] Throughout this application, various embodiments may be presented in a range format. It should be understood that the description in range format is merely for convenience and brevity and should not be construed as an inflexible limitation on the scope of the disclosure. Accordingly, the description of a range should be considered to have specifically
Attorney Docket No.49755-0049WO1 disclosed all the possible subranges as well as individual numerical values within that range. For example, description of a range such as from 1 to 6 should be considered to have specifically disclosed subranges such as from 1 to 3, from 1 to 4, from 1 to 5, from 2 to 4, from 2 to 6, from 3 to 6 etc., as well as individual numbers within that range, for example, 1, 2, 3, 4, 5, and 6. This applies regardless of the breadth of the range. [0256] As used in the specification and claims, the singular forms “a”, “an” and “the” include plural references unless the context clearly dictates otherwise. For example, the term “a sample” includes a plurality of samples, including mixtures thereof. [0257] The terms “determining,” “measuring,” “evaluating,” “assessing,” “assaying,” and “analyzing” are often used interchangeably herein to refer to forms of measurement. The terms include determining if an element is present or not (for example, detection). These terms can include quantitative, qualitative or quantitative and qualitative determinations. Assessing can be relative or absolute. “Detecting the presence of” can include determining the amount of something present in addition to determining whether it is present or absent depending on the context. [0258] The terms “subject,” “individual,” or “patient” are often used interchangeably herein. [0259] The term “in vivo” is used to describe an event that takes place in a subject’s body. [0260] The term “ex vivo” is used to describe an event that takes place outside of a subject’s body. An ex vivo assay is not performed on a subject. Rather, it is performed upon a sample separate from a subject. An example of an ex vivo assay performed on a sample is an “in vitro” assay. [0261] The term “in vitro” is used to describe an event that takes places contained in a container for holding laboratory reagent such that it is separated from the biological source from which the material is obtained. In vitro assays can encompass cell-based assays in which living or dead cells are employed. In vitro assays can also encompass a cell-free assay in which no intact cells are employed. [0262] As used herein, the term “about” a number refers to that number plus or minus 10% of that number. The term “about” a range refers to that range minus 10% of its lowest value and plus 10% of its greatest value. [0263] As used herein, the term "buffer solution" refers to an aqueous solution consisting of a mixture of a weak acid and its conjugate base, or vice versa.
Attorney Docket No.49755-0049WO1 [0264] As used herein, the term "cell culture medium" refers to a mixture for growth and proliferation of cells in vitro, which contains essential elements for growth and proliferation of cells such as sugars, amino acids, various nutrients, inorganic substances, etc. [0265] A buffer solution, as used herein, is not a cell culture medium. [0266] As used herein, the term “bioreactor” refers to a culture apparatus capable of continuously controlling a series of conditions that affect cell culture, such as dissolved oxygen concentration, dissolved carbon dioxide concentration, pH, and temperature. [0267] The term “vector,” as used herein, refers to a nucleic acid molecule capable of propagating another nucleic acid to which it is linked. The term includes the vector as a self- replicating nucleic acid structure as well as the vector incorporated into the genome of a host cell into which it has been introduced. Some vectors are suitable for delivering the nucleic acid molecule(s) or polynucleotide(s) of the present application. Certain vectors are capable of directing the expression of nucleic acids to which they are operatively linked. Such vectors are referred to herein as expression vectors. [0268] The term “operably linked” refers to two or more nucleic acid sequence or polypeptide elements that are usually physically linked and are in a functional relationship with each other. For instance, a promoter is operably linked to a coding sequence if the promoter is able to initiate or regulate the transcription or expression of a coding sequence, in which case, the coding sequence should be understood as being “under the control of” the promoter. [0269] The terms “host cell,” “host cell line,” and “host cell culture” are used interchangeably and refer to cells into which exogenous nucleic acid has been introduced, including the progeny of such cells. Host cells include “engineered cells,” “transformants,” and “transformed cells,” which include the primary engineered (e.g., transformed) cell and progeny derived therefrom without regard to the number of passages. Progeny may not be completely identical in nucleic acid content to a parent cell, but may contain mutations. Mutant progeny that have the same function or biological activity as screened or selected for in the originally transformed cell are included herein. [0270] As appropriate, the host cells can be stably or transiently transfected with a polynucleotide encoding a fusion protein, as described herein. [0271] The section headings used herein are for organizational purposes only and are not to be construed as limiting the subject matter described.
Attorney Docket No.49755-0049WO1 VII. EXAMPLES [0272] The following examples are included for illustrative purposes only and are not intended to limit the scope of the invention. Example 1: AB-101 in Combination with Rituximab for Treatment of Diffuse Large B Cell Lymphoma (DLBCL) [0273] Patients with a histologically confirmed CD20+ cancer selected from diffuse large B-cell lymphoma (DLBCL) (including double hit or triple hit, or transformed from an antecedent indolent lymphoma), high-grade B-cell lymphoma, primary mediastinal B-cell lymphoma (PMBCL) are selected for treatment. [0274] Patients are administered 3 treatment cycles of AB-101 (described, e.g., in WO2022/133057) plus rituximab. Each treatment cycle is comprised of 4 doses of AB-101, administered by IV infusions on Day 1, 4, 8, and 11. AB-101 is administered at 4x10
9 cells on Day 1 and Day 8, and at 2x10
9 cells on days 4 and 11. [0275] Subsequent treatment cycles (Cyle 2 and cycle 3) are dosed 6-10 weeks apart in the absence of disease progression or a dose-limiting toxicity, or if none of the clinical trial discontinuation criteria is met. [0276] All cycles include 3 consecutive days of lymphodepleting chemotherapy, consisting of IV fludarabine (30mg/m
2) and IV cyclophosphamide (500mg/m
2) in preparation for treatment with AB-101. Two doses of rituximab (500mg/m
2) are administered in each cycle, on Day -4 and Day 8. [0277] IL-2 is not administered post AB-101 infusions. [0278] See FIG.1 for a patient flowchart. OTHER EMBODIMENTS It is to be understood that while the invention has been described in conjunction with the detailed description thereof, the foregoing description is intended to illustrate and not limit the scope of the invention, which is defined by the scope of the appended claims. Other aspects, advantages, and modifications are within the scope of the following claims.
 Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company Reference Reditux DRL_RI CD20 Dr. Reddy's Bhati et al., Clin 7 3 8 6 5 . 9 3 9 1
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company Reference Reditux DRL_RI CD20 Dr. Reddy's Bhati et al., Clin 7 3 8 6 5 . 9 3 9 1
 Attorney Docket No.49755-0049WO1 Table 4. Exemplary Cryopreservation Composition #2 Exemplary v/v% Final Concentration in Excipient Solution Composition in Cryopreservation 0;
Attorney Docket No.49755-0049WO1 Table 4. Exemplary Cryopreservation Composition #2 Exemplary v/v% Final Concentration in Excipient Solution Composition in Cryopreservation 0;
 Exemplary v/v% Final Concentration in Excipient in 0;
Exemplary v/v% Final Concentration in Excipient in 0;
 Attorney Docket No.49755-0049WO1 Mutation (GRCh38) Protein Position Consequence 11:60466036:G>T 151 missense_variant 11:60466042:A>C 153 missense_variant
Attorney Docket No.49755-0049WO1 Mutation (GRCh38) Protein Position Consequence 11:60466036:G>T 151 missense_variant 11:60466042:A>C 153 missense_variant
 Attorney Docket No.49755-0049WO1 Mutation (GRCh38) Protein Position Consequence 11:60468394:G>A 274 missense_variant t
Attorney Docket No.49755-0049WO1 Mutation (GRCh38) Protein Position Consequence 11:60468394:G>A 274 missense_variant t
 with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone), e.g., at least 4 cycles of R-CHOP, a second line of chemotherapy, e.g., ICE (ifosfamide, carboplatin, and etoposide) or DHAP (dexamethasone, high-dose Ara-C cytarabine, and platinol) with or without an approved therapeutic mAb (e.g., rituximab). C. Lymphodepletion [0150] In some embodiments, the patient is lymphodepleted before treatment or before each cycle of treatment. [0151] Illustrative lymphodepleting chemotherapy regimens, along with correlative beneficial biomarkers, are described in WO 2016/191756 and WO 2019/079564, hereby incorporated by reference in their entirety. In certain embodiments, the lymphodepleting chemotherapy regimen comprises administering to the patient doses of cyclophosphamide (between 200 mg/m2/day and 2000 mg/m2/day) and doses of fludarabine (between 20 mg/m2/day and 900 mg/m2/day). [0152] In some embodiments, lymphodepletion comprises administration of or of about 250 to about 500 mg/m2 of cyclophosphamide, e.g., from or from about 250 to or to about 500, 250, 400, 500, about 250, about 400, or about 500 mg/m2 of cyclophosphamide. [0153] In some embodiments, lymphodepletion comprises administration of or of about 20 mg/m2/day to or to about 40 mg/m2/day fludarabine, e.g., 30 or about 30 mg/m2/day. [0154] In some embodiments, lymphodepletion comprises administration of both cyclophosmamide and fludarabine. [0155] In some embodiments, the patient is lymphodepleted by intravenous administration of cyclophosphamide (250 mg/m2/day) and fludarabine (30 mg/m2/day).
Attorney Docket No.49755-0049WO1 [0156] In some embodiments, the patient is lymphodepleted by intravenous administration of cyclophosphamide (500 mg/m2/day) and fludarabine (30 mg/m2/day). [0157] In some embodiments, the lymphodepletion occurs no more than 5 days prior to the first dose of NK cells. In some embodiments, the lymphodepletion occurs no more than 7 days prior to the first dose of NK cells. [0158] In some embodiments, lymphodepletion occurs daily for 3 consecutive days. In some embodiments, lymphodepletion occurs daily for 3 consecutive days, starting 5 days before the first dose of NK cells (i.e., from Day -5 through Day -3). [0159] In some embodiments, the lymphodepletion occurs on day -5, day -4 and day -3. D. Administration 1. NK Cells [0160] In some embodiments, the NK cells are administered as part of a pharmaceutical composition, e.g., a pharmaceutical composition described herein. Cells are administered after thawing, in some cases without any further manipulation in cases where their cryoprotectant is compatible for immediate administration. For a given individual, a treatment regimen often comprises administration over time of multiple aliquots or doses of NK cells drawn from a common batch or donor. [0161] In some embodiments, the NK cells, e.g., the NK cells described herein are administered at or at about 1 x 108 to or to about 8 x 1010 NK cells per dose, including 1 x 108, 2 x 108, 3 x 108, 4 x 108, 5 x 108, 6 x 108, 7 x 108, 8 x 108, 9 x 108, 1 x 109, 2 x 109, 3 x 109, 4 x 109, 5 x 109, 6 x 109, 7 x 109, or 8 x 109 cells per dose. In some embodiments, the NK cells are administered at or at about 1 x 108, at or at about 1 x 109, at or at about 4 x 109, or at or at about 8 x 109 NK cells per dose. [0162] In some embodiments, the NK cells are administered weekly. In some embodiments, the NK cells are administered weekly for or for about four weeks. In some embodiments, the NK cells are administered weekly for or for about 8 weeks. In some embodiments, the NK cells are administered for a plurality of cycles, each cycle comprising administering weekly doses for 3, 4, 5, 6, 7, 8, 9, 10, 11, or 12 weeks. The number of cycles include 2, 3, 4, or 5 cycles. Each cycle can be preceded by lymphodepletion, a debulking or pretreatment dose of antibody, or both. In some embodiments, the NK cells are administered without a dose of antibody weekly for or for about four weeks followed by administration of NK cells with a dose of antibody, e.g., rituximab.
Attorney Docket No.49755-0049WO1 [0163] In some embodiments, the NK cells are administered for one or more treatment cycles (e.g., 1, 2, 3, 4, or 5 treatment cycles), each comprising administration on days 1, 8, 4, and 11. In some embodiments, the NK cells are administered at or at about 4 x 109 on days 1 and 8 and 2 x 109 on days 4 and 11 of the treatment cycle. In some embodiments, following the first treatment cycle, subsequent treatment cycles are administered 6-10 weeks apart (e.g., 6, 7, 8, 9, or 10 weeks apart, or thereabouts). [0164] In some cases, the plurality of cycles comprising weekly doses are followed by additional doses administered less frequently, including one dose every four weeks, every month, every other month, or every third month. Such doses can help the patient maintain a response to the therapy. [0165] In some embodiments, the NK cells are cryopreserved in an infusion-ready media, e.g., a cryopreservation composition suitable for intravenous administration, e.g., as described herein. [0166] In some embodiments, the NK cells are cryopreserved in vials containing from or from about 1 x 108 to or to about 8 x 1010 cells per vial, including 1 x 108, 2 x 108, 3 x 108, 4 x 108, 5 x 108, 6 x 108, 7 x 108, 8 x 108, 9 x 108, 1 x 109, 2 x 109, 3 x 109, 4 x 109, 5 x 109, 6 x 109, 7 x 109, or 8 x 109 cells per vial. In some embodiments, the NK cells are cryopreserved in vials containing a single dose. In some embodiments, the NK cells are cryopreserved in vials containing less than a single dose. In some of such cases, multiple vials can be thawed simultaneously or separately, and can be combined prior to administration or administered separately. [0167] In some embodiments, the cells are thawed, e.g., in a 37°C water bath, prior to administration. [0168] In some embodiments, the thawed vial(s) of NK cells are aseptically transferred to a single administration vessel, e.g., administration bag using, e.g., a vial adapter and a sterile syringe. The NK cells can be administered to the patient from the vessel through a Y-type blood/solution set filter as an IV infusion, by gravity. [0169] In some embodiments, the NK cells are administered as soon as practical, preferably less than 90 minutes, e.g., less than 80, 70, 60, 50, 40, 30, 20, or 10 minutes after thawing. In some embodiments, the NK cells are administered within 30 minutes of thawing. [0170] In some embodiments, the pharmaceutical composition is administered intravenously via syringe or via gravity IV infusion. In some embodiments, the infusion is administered in or in about 1 minute, 2 minutes, 3, minutes, 4 minutes, 5 minutes, 6 minutes, 7 minutes, 8 minutes, 9 minutes, or 10 minutes. In some embodiments, the infusion is
Attorney Docket No.49755-0049WO1 administered over or over about 1 minute, 2 minutes, 3, minutes, 4 minutes, 5 minutes, 6 minutes, 7 minutes, 8 minutes, 9 minutes, or 10 minutes. [0171] In some embodiments, 1 mL, 4 mL, or 10 mL of drug product is administered to the patient intravenously via syringe. 2. Antibodies [0172] In some embodiments, the NK cell(s) described herein, e.g., the pharmaceutical compositions comprising NK cell(s) described herein, are administered in combination with an antibody, e.g., an antibody described herein, e.g., a CD20 targeting antibody, e.g., rituximab. In some embodiments, an antibody is administered together with the NK cells as part of a pharmaceutical composition. In some embodiments, an antibody is administered separately from the NK cells, e.g., as part of a separate pharmaceutical composition. Antibodies can be administered prior to, subsequent to, or simultaneously with administration of the NK cells. [0173] In some embodiments, the antibody is administered before the NK cells. In some embodiments, the antibody is administered after the NK cells. [0174] In some embodiments, the NK cells are administered or are administered at least 30 minutes, 60 minutes, 90 minutes, 120 minutes, 150 minutes, 180 minutes, 210 minutes, or 240 minutes after completing administration of the antibody. In some embodiments, the NK cells are administered within 30 minutes, 60 minutes, 90 minutes, 120 minutes, 150 minutes, 180 minutes, 210 minutes, or 240 minutes after completing administration of the antibody. [0175] In some embodiments, the NK cells are administered the day after the antibody is administered. [0176] In some embodiments, the NK cells are administered at each administration, while the antibody is administered at a subset of the administrations. For example, in some embodiments, the NK cells are administered once a week and the antibody is administered once a every other week, once every three weeks, once every four weeks, or once a month. [0177] In some embodiments, the antibody is administered weekly for 8 weeks. In some embodiments, the antibody is administered every two weeks for 8 weeks. In some embodiments, the antibody administered for a plurality of cycles, each cycle comprising administering weekly doses for 3, 4, 5, 6, 7, 8, 9, 10, 11, or 12 weeks. The number of cycles include 2, 3, 4, or 5 cycles. Each cycle can be preceded by lymphodepletion, a debulking or pretreatment dose of antibody, or both.
Attorney Docket No.49755-0049WO1 [0178] In some cases, the plurality of cycles comprising weekly doses are followed by additional doses administered less frequently, including one dose every four weeks, every month, every other month, or every third month. Such doses can help the patient maintain a response to the therapy. [0179] In some embodiments, a dose of antibody is given prior to the first dose of cells. In some embodiments, a debulking dose or a pretreatment dose of the antibody is given prior to the first dose of cells. [0180] Rituximab is preferably administered at 375 mg/m2 or 500 mg/m2 (e.g., 375 mg/m2 or 500 mg/m2 per day), preferably at least 1 hour prior to administration of NK cells, e.g., 2–24 hours before administration of NK cells. [0181] In some embodiments, the CD20 targeting antibody (e.g., rituximab) is administered (e.g., intravenously) during lymphodepletion. In some embodiments, the CD20 targ 3. Cytokines [0182] In some embodiments, a cytokine is administered to the patient. [0183] In some embodiments, the cytokine is administered together with the NK cells as part of a pharmaceutical composition. In some embodiments, the cytokine is administered separately from the NK cells, e.g., as part of a separate pharmaceutical composition. [0184] In some embodiments, the cytokine is IL-2. Some tumor microenvironments can become deprived of certain cytokines, including IL-2. In such cases, it can be advantageous to administer a cytokine, such as IL-2, to the patient as part of a treatment regimen involving NK cells. In some cases, the presence of the cytokine, such as IL-2, at the tumor site can increase, enhance, or support the cytotoxicity of the NK cells. In some cases, the cytokine, such as IL-2, can enhance the survival, persistence, or expansion of the NK cells in the patient’s body. [0185] In some embodiments, the IL-2 is administered subcutaneously. [0186] In some embodiments, the IL-2 is administered from between 1 to 4 or about 1 to about 4 hours following the conclusion of NK cell administration. In some embodiments, the IL-2 is administered at least 1 hour following the conclusion of NK cell administration. In some embodiments, the IL-2 is administered no more than 4 hours following the conclusion of NK cell administration. In some embodiments, the IL-2 is administered at least 1 hour after and no more than 4 hours following the conclusion of NK cell administration. Thus, in some embodiments, the IL-2 is administered weekly. In some embodiments, the IL-2 is
Attorney Docket No.49755-0049WO1 administered weekly for or for about four weeks. In some embodiments, the IL-2 is administered weekly for or for about 8 weeks. [0187] In some embodiments, the IL-2 is administered at up to 10 million IU/M2, e.g., up to 1 million, 2 million, 3 million, 4 million, 5 million, 6 million, 7 million, 8 million, 9 million, or 10 million IU/m2. [0188] In some embodiments, the IL-2 is administered at or at about 0.5 million, 1 million, at or at about 2 million, at or at about 3 million, at or at about 4 million, at or at about 5 million, at or at about 6 million, at or at about 7 million, at or at about 8 million, at or at about 9 million, at or at about 10 million IU/m2 [0189] In some embodiments, the IL-2 is administered at or at about 1 x 106 IU/M2. In some embodiments, the IL-2 is administered at or at about 2 x 106 IU/m2. In some embodiments, the IL-2 is administered at or at about 6 x 106 IU/m2. [0190] In some embodiments, less than 1 x 106 IU/m2 IL-2 is administered to the patient. [0191] In some embodiments, a flat dose of IL-2 is administered to the patient. In some embodiments, a flat dose of 1 million IU or about 1 million IU is administered to the patient. In some embodiments, a flat dose of 2 million IU or about 2 million IU is administered to the patient. In some embodiments, a flat dose of 3 million IU or about 3 million IU is administered to the patient. In some embodiments, a flat dose of 4 million IU or about 4 million IU is administered to the patient. In some embodiments, a flat dose of 5 million IU or about 5 million IU is administered to the patient. In some embodiments, a flat dose of 6 million IU or about 6 million IU is administered to the patient. In some embodiments, a flat dose of 7 million IU or about 7 million IU is administered to the patient. In some embodiments, a flat dose of 8 million IU or about 8 million IU is administered to the patient. In some embodiments, a flat dose of 9 million IU or about 9 million IU is administered to the patient. [0192] In some embodiments, IL-2 is not administered to the patient. 4. Pre-Treatments [0193] In some cases, the patient is pre-treated, e.g., 30-60 minutes before NK cell administration. In some cases, the patient is pre-medicated with acetaminophen (e.g., 500 to 1,000 mg given orally); diphenhydramine (e.g., 12.5 to 25 mg given orally, e.g., when needed to treat hypersensitivity reactions); intravenous glucocorticoid (e.g., dexamethasome (e.g., 20 mg) and/or methylprednisone (e.g., 80 mg)). An example pre-medication regimen is shown in Table 8.
Attorney Docket No.49755-0049WO1 Table 8. Example Pre-Medication Regimen NK cell Optional NK infusion Patients Premedication Administration cell dose n n
with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone), e.g., at least 4 cycles of R-CHOP, a second line of chemotherapy, e.g., ICE (ifosfamide, carboplatin, and etoposide) or DHAP (dexamethasone, high-dose Ara-C cytarabine, and platinol) with or without an approved therapeutic mAb (e.g., rituximab). C. Lymphodepletion [0150] In some embodiments, the patient is lymphodepleted before treatment or before each cycle of treatment. [0151] Illustrative lymphodepleting chemotherapy regimens, along with correlative beneficial biomarkers, are described in WO 2016/191756 and WO 2019/079564, hereby incorporated by reference in their entirety. In certain embodiments, the lymphodepleting chemotherapy regimen comprises administering to the patient doses of cyclophosphamide (between 200 mg/m2/day and 2000 mg/m2/day) and doses of fludarabine (between 20 mg/m2/day and 900 mg/m2/day). [0152] In some embodiments, lymphodepletion comprises administration of or of about 250 to about 500 mg/m2 of cyclophosphamide, e.g., from or from about 250 to or to about 500, 250, 400, 500, about 250, about 400, or about 500 mg/m2 of cyclophosphamide. [0153] In some embodiments, lymphodepletion comprises administration of or of about 20 mg/m2/day to or to about 40 mg/m2/day fludarabine, e.g., 30 or about 30 mg/m2/day. [0154] In some embodiments, lymphodepletion comprises administration of both cyclophosmamide and fludarabine. [0155] In some embodiments, the patient is lymphodepleted by intravenous administration of cyclophosphamide (250 mg/m2/day) and fludarabine (30 mg/m2/day).
Attorney Docket No.49755-0049WO1 [0156] In some embodiments, the patient is lymphodepleted by intravenous administration of cyclophosphamide (500 mg/m2/day) and fludarabine (30 mg/m2/day). [0157] In some embodiments, the lymphodepletion occurs no more than 5 days prior to the first dose of NK cells. In some embodiments, the lymphodepletion occurs no more than 7 days prior to the first dose of NK cells. [0158] In some embodiments, lymphodepletion occurs daily for 3 consecutive days. In some embodiments, lymphodepletion occurs daily for 3 consecutive days, starting 5 days before the first dose of NK cells (i.e., from Day -5 through Day -3). [0159] In some embodiments, the lymphodepletion occurs on day -5, day -4 and day -3. D. Administration 1. NK Cells [0160] In some embodiments, the NK cells are administered as part of a pharmaceutical composition, e.g., a pharmaceutical composition described herein. Cells are administered after thawing, in some cases without any further manipulation in cases where their cryoprotectant is compatible for immediate administration. For a given individual, a treatment regimen often comprises administration over time of multiple aliquots or doses of NK cells drawn from a common batch or donor. [0161] In some embodiments, the NK cells, e.g., the NK cells described herein are administered at or at about 1 x 108 to or to about 8 x 1010 NK cells per dose, including 1 x 108, 2 x 108, 3 x 108, 4 x 108, 5 x 108, 6 x 108, 7 x 108, 8 x 108, 9 x 108, 1 x 109, 2 x 109, 3 x 109, 4 x 109, 5 x 109, 6 x 109, 7 x 109, or 8 x 109 cells per dose. In some embodiments, the NK cells are administered at or at about 1 x 108, at or at about 1 x 109, at or at about 4 x 109, or at or at about 8 x 109 NK cells per dose. [0162] In some embodiments, the NK cells are administered weekly. In some embodiments, the NK cells are administered weekly for or for about four weeks. In some embodiments, the NK cells are administered weekly for or for about 8 weeks. In some embodiments, the NK cells are administered for a plurality of cycles, each cycle comprising administering weekly doses for 3, 4, 5, 6, 7, 8, 9, 10, 11, or 12 weeks. The number of cycles include 2, 3, 4, or 5 cycles. Each cycle can be preceded by lymphodepletion, a debulking or pretreatment dose of antibody, or both. In some embodiments, the NK cells are administered without a dose of antibody weekly for or for about four weeks followed by administration of NK cells with a dose of antibody, e.g., rituximab.
Attorney Docket No.49755-0049WO1 [0163] In some embodiments, the NK cells are administered for one or more treatment cycles (e.g., 1, 2, 3, 4, or 5 treatment cycles), each comprising administration on days 1, 8, 4, and 11. In some embodiments, the NK cells are administered at or at about 4 x 109 on days 1 and 8 and 2 x 109 on days 4 and 11 of the treatment cycle. In some embodiments, following the first treatment cycle, subsequent treatment cycles are administered 6-10 weeks apart (e.g., 6, 7, 8, 9, or 10 weeks apart, or thereabouts). [0164] In some cases, the plurality of cycles comprising weekly doses are followed by additional doses administered less frequently, including one dose every four weeks, every month, every other month, or every third month. Such doses can help the patient maintain a response to the therapy. [0165] In some embodiments, the NK cells are cryopreserved in an infusion-ready media, e.g., a cryopreservation composition suitable for intravenous administration, e.g., as described herein. [0166] In some embodiments, the NK cells are cryopreserved in vials containing from or from about 1 x 108 to or to about 8 x 1010 cells per vial, including 1 x 108, 2 x 108, 3 x 108, 4 x 108, 5 x 108, 6 x 108, 7 x 108, 8 x 108, 9 x 108, 1 x 109, 2 x 109, 3 x 109, 4 x 109, 5 x 109, 6 x 109, 7 x 109, or 8 x 109 cells per vial. In some embodiments, the NK cells are cryopreserved in vials containing a single dose. In some embodiments, the NK cells are cryopreserved in vials containing less than a single dose. In some of such cases, multiple vials can be thawed simultaneously or separately, and can be combined prior to administration or administered separately. [0167] In some embodiments, the cells are thawed, e.g., in a 37°C water bath, prior to administration. [0168] In some embodiments, the thawed vial(s) of NK cells are aseptically transferred to a single administration vessel, e.g., administration bag using, e.g., a vial adapter and a sterile syringe. The NK cells can be administered to the patient from the vessel through a Y-type blood/solution set filter as an IV infusion, by gravity. [0169] In some embodiments, the NK cells are administered as soon as practical, preferably less than 90 minutes, e.g., less than 80, 70, 60, 50, 40, 30, 20, or 10 minutes after thawing. In some embodiments, the NK cells are administered within 30 minutes of thawing. [0170] In some embodiments, the pharmaceutical composition is administered intravenously via syringe or via gravity IV infusion. In some embodiments, the infusion is administered in or in about 1 minute, 2 minutes, 3, minutes, 4 minutes, 5 minutes, 6 minutes, 7 minutes, 8 minutes, 9 minutes, or 10 minutes. In some embodiments, the infusion is
Attorney Docket No.49755-0049WO1 administered over or over about 1 minute, 2 minutes, 3, minutes, 4 minutes, 5 minutes, 6 minutes, 7 minutes, 8 minutes, 9 minutes, or 10 minutes. [0171] In some embodiments, 1 mL, 4 mL, or 10 mL of drug product is administered to the patient intravenously via syringe. 2. Antibodies [0172] In some embodiments, the NK cell(s) described herein, e.g., the pharmaceutical compositions comprising NK cell(s) described herein, are administered in combination with an antibody, e.g., an antibody described herein, e.g., a CD20 targeting antibody, e.g., rituximab. In some embodiments, an antibody is administered together with the NK cells as part of a pharmaceutical composition. In some embodiments, an antibody is administered separately from the NK cells, e.g., as part of a separate pharmaceutical composition. Antibodies can be administered prior to, subsequent to, or simultaneously with administration of the NK cells. [0173] In some embodiments, the antibody is administered before the NK cells. In some embodiments, the antibody is administered after the NK cells. [0174] In some embodiments, the NK cells are administered or are administered at least 30 minutes, 60 minutes, 90 minutes, 120 minutes, 150 minutes, 180 minutes, 210 minutes, or 240 minutes after completing administration of the antibody. In some embodiments, the NK cells are administered within 30 minutes, 60 minutes, 90 minutes, 120 minutes, 150 minutes, 180 minutes, 210 minutes, or 240 minutes after completing administration of the antibody. [0175] In some embodiments, the NK cells are administered the day after the antibody is administered. [0176] In some embodiments, the NK cells are administered at each administration, while the antibody is administered at a subset of the administrations. For example, in some embodiments, the NK cells are administered once a week and the antibody is administered once a every other week, once every three weeks, once every four weeks, or once a month. [0177] In some embodiments, the antibody is administered weekly for 8 weeks. In some embodiments, the antibody is administered every two weeks for 8 weeks. In some embodiments, the antibody administered for a plurality of cycles, each cycle comprising administering weekly doses for 3, 4, 5, 6, 7, 8, 9, 10, 11, or 12 weeks. The number of cycles include 2, 3, 4, or 5 cycles. Each cycle can be preceded by lymphodepletion, a debulking or pretreatment dose of antibody, or both.
Attorney Docket No.49755-0049WO1 [0178] In some cases, the plurality of cycles comprising weekly doses are followed by additional doses administered less frequently, including one dose every four weeks, every month, every other month, or every third month. Such doses can help the patient maintain a response to the therapy. [0179] In some embodiments, a dose of antibody is given prior to the first dose of cells. In some embodiments, a debulking dose or a pretreatment dose of the antibody is given prior to the first dose of cells. [0180] Rituximab is preferably administered at 375 mg/m2 or 500 mg/m2 (e.g., 375 mg/m2 or 500 mg/m2 per day), preferably at least 1 hour prior to administration of NK cells, e.g., 2–24 hours before administration of NK cells. [0181] In some embodiments, the CD20 targeting antibody (e.g., rituximab) is administered (e.g., intravenously) during lymphodepletion. In some embodiments, the CD20 targ 3. Cytokines [0182] In some embodiments, a cytokine is administered to the patient. [0183] In some embodiments, the cytokine is administered together with the NK cells as part of a pharmaceutical composition. In some embodiments, the cytokine is administered separately from the NK cells, e.g., as part of a separate pharmaceutical composition. [0184] In some embodiments, the cytokine is IL-2. Some tumor microenvironments can become deprived of certain cytokines, including IL-2. In such cases, it can be advantageous to administer a cytokine, such as IL-2, to the patient as part of a treatment regimen involving NK cells. In some cases, the presence of the cytokine, such as IL-2, at the tumor site can increase, enhance, or support the cytotoxicity of the NK cells. In some cases, the cytokine, such as IL-2, can enhance the survival, persistence, or expansion of the NK cells in the patient’s body. [0185] In some embodiments, the IL-2 is administered subcutaneously. [0186] In some embodiments, the IL-2 is administered from between 1 to 4 or about 1 to about 4 hours following the conclusion of NK cell administration. In some embodiments, the IL-2 is administered at least 1 hour following the conclusion of NK cell administration. In some embodiments, the IL-2 is administered no more than 4 hours following the conclusion of NK cell administration. In some embodiments, the IL-2 is administered at least 1 hour after and no more than 4 hours following the conclusion of NK cell administration. Thus, in some embodiments, the IL-2 is administered weekly. In some embodiments, the IL-2 is
Attorney Docket No.49755-0049WO1 administered weekly for or for about four weeks. In some embodiments, the IL-2 is administered weekly for or for about 8 weeks. [0187] In some embodiments, the IL-2 is administered at up to 10 million IU/M2, e.g., up to 1 million, 2 million, 3 million, 4 million, 5 million, 6 million, 7 million, 8 million, 9 million, or 10 million IU/m2. [0188] In some embodiments, the IL-2 is administered at or at about 0.5 million, 1 million, at or at about 2 million, at or at about 3 million, at or at about 4 million, at or at about 5 million, at or at about 6 million, at or at about 7 million, at or at about 8 million, at or at about 9 million, at or at about 10 million IU/m2 [0189] In some embodiments, the IL-2 is administered at or at about 1 x 106 IU/M2. In some embodiments, the IL-2 is administered at or at about 2 x 106 IU/m2. In some embodiments, the IL-2 is administered at or at about 6 x 106 IU/m2. [0190] In some embodiments, less than 1 x 106 IU/m2 IL-2 is administered to the patient. [0191] In some embodiments, a flat dose of IL-2 is administered to the patient. In some embodiments, a flat dose of 1 million IU or about 1 million IU is administered to the patient. In some embodiments, a flat dose of 2 million IU or about 2 million IU is administered to the patient. In some embodiments, a flat dose of 3 million IU or about 3 million IU is administered to the patient. In some embodiments, a flat dose of 4 million IU or about 4 million IU is administered to the patient. In some embodiments, a flat dose of 5 million IU or about 5 million IU is administered to the patient. In some embodiments, a flat dose of 6 million IU or about 6 million IU is administered to the patient. In some embodiments, a flat dose of 7 million IU or about 7 million IU is administered to the patient. In some embodiments, a flat dose of 8 million IU or about 8 million IU is administered to the patient. In some embodiments, a flat dose of 9 million IU or about 9 million IU is administered to the patient. [0192] In some embodiments, IL-2 is not administered to the patient. 4. Pre-Treatments [0193] In some cases, the patient is pre-treated, e.g., 30-60 minutes before NK cell administration. In some cases, the patient is pre-medicated with acetaminophen (e.g., 500 to 1,000 mg given orally); diphenhydramine (e.g., 12.5 to 25 mg given orally, e.g., when needed to treat hypersensitivity reactions); intravenous glucocorticoid (e.g., dexamethasome (e.g., 20 mg) and/or methylprednisone (e.g., 80 mg)). An example pre-medication regimen is shown in Table 8.
Attorney Docket No.49755-0049WO1 Table 8. Example Pre-Medication Regimen NK cell Optional NK infusion Patients Premedication Administration cell dose n n
 Attorney Docket No.49755-0049WO1 [0239] In some embodiments, the immune checkpoint inhibitor is an antibody. [0240] In some embodiments, the PD-1 inhibitor is selected from the group consisting of pembrolizumab, nivolumab, toripalimab, cemiplimab-rwlc, sintilimab, and combinations thereof. [0241] In some embodiments, the PD-L1 inhibitor is selected from the group consisting of atezolizumab, durvalumab, avelumab, and combinations thereof. [0242] In some embodiments, the CTLA-4 inhibitor is ipilimumab. In some embodiments, the PD-1 inhibitor is selected from the group of inhibitors shown in Table 10. Table 10. Exemplary PD-1 Inhibitor Antibodies Name Internal Name Antigen Company nivolumab Opdivo, ONO-4538, PD-1 BMS, Medarex, Ono n
Attorney Docket No.49755-0049WO1 [0239] In some embodiments, the immune checkpoint inhibitor is an antibody. [0240] In some embodiments, the PD-1 inhibitor is selected from the group consisting of pembrolizumab, nivolumab, toripalimab, cemiplimab-rwlc, sintilimab, and combinations thereof. [0241] In some embodiments, the PD-L1 inhibitor is selected from the group consisting of atezolizumab, durvalumab, avelumab, and combinations thereof. [0242] In some embodiments, the CTLA-4 inhibitor is ipilimumab. In some embodiments, the PD-1 inhibitor is selected from the group of inhibitors shown in Table 10. Table 10. Exemplary PD-1 Inhibitor Antibodies Name Internal Name Antigen Company nivolumab Opdivo, ONO-4538, PD-1 BMS, Medarex, Ono n
 Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company F520 PD-1 Shandong New Time e
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company F520 PD-1 Shandong New Time e
 Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company camrelizumab SHR-1210 PD-1 Incyte, Jiangsu u
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company camrelizumab SHR-1210 PD-1 Incyte, Jiangsu u
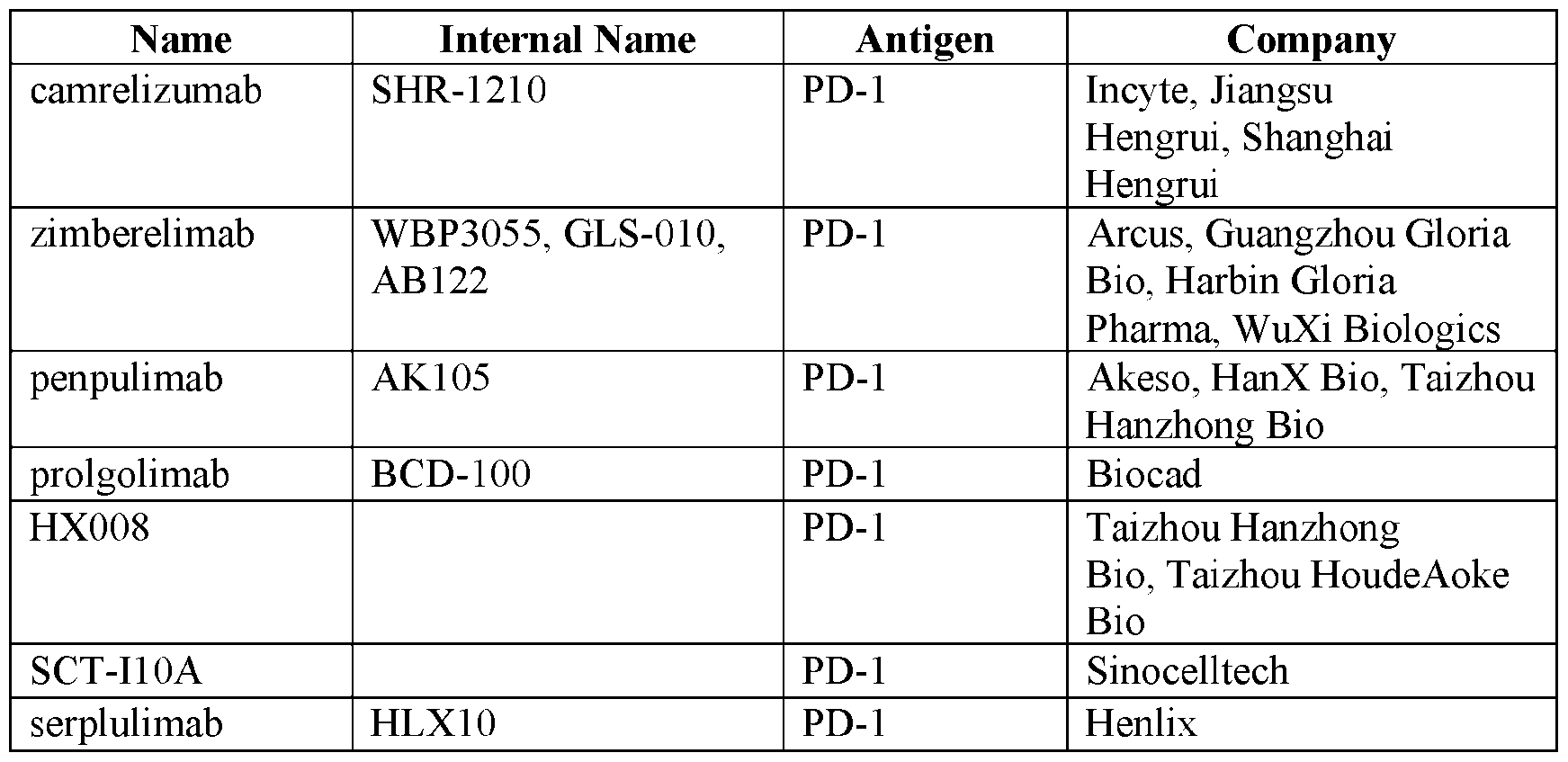 , ors shown in Table 11. Table 11. Exemplary PD-L1 Inhibitor Antibodies Name Internal Name Antigen Company Imfinzi, MEDI-4736, AstraZeneca, Celgene, Me i
, ors shown in Table 11. Table 11. Exemplary PD-L1 Inhibitor Antibodies Name Internal Name Antigen Company Imfinzi, MEDI-4736, AstraZeneca, Celgene, Me i
 Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company IBI322 IBI-322 CD47, PD-L1 Innovent ai
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company IBI322 IBI-322 CD47, PD-L1 Innovent ai
 [0244] In some embodiments, the CTLA-4 inhibitor is selected from the group of inhibitors shown in Table 12. Table 12. Exemplary CTLA4 Inhibitor Antibodies Name Internal Name Antigen Company
[0244] In some embodiments, the CTLA-4 inhibitor is selected from the group of inhibitors shown in Table 12. Table 12. Exemplary CTLA4 Inhibitor Antibodies Name Internal Name Antigen Company
 Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company vudalimab XmAb20717 CTLA4, PD-1 Xencor n i
Attorney Docket No.49755-0049WO1 Name Internal Name Antigen Company vudalimab XmAb20717 CTLA4, PD-1 Xencor n i